
Abstract
Objective
To study whether cognitive behavioural therapy decreases suicide attempts in people with previous suicide attempts.
Design
Systematic review and meta-analysis.
Setting
Randomised trials that compare cognitive behavioural therapy with treatment as usual.
Participants
Patients who had engaged in any type of suicide attempt in the six months prior to trial entry resulting in presentation to clinical services.
Main outcome measure
Suicide attempt.
Results
We included ten trials, eight from Cochrane reviews and two from our updated searches (1241 patients, 219 of whom had at least one new suicide attempt). Cognitive behavioural therapy compared to treatment as usual reduced the risk of a new suicide attempt; risk ratio 0.47; 95% confidence interval 0.30–0.73; p = 0.0009; I2 = 57%. Only seven suicides were reported (3 versus 4). One trial had an unusually large effect; if this trial is excluded, the risk ratio becomes 0.61 (0.46–0.80) and the heterogeneity in the results disappears (I2 = 0%).
Conclusions
Cognitive behavioural therapy reduces not only repeated self-harm but also repeated suicide attempts. It should be the preferred treatment for all patients with depression.
Introduction
Suicide prevention is what matters the most when health professionals see patients with mental disorders. Getting people back to work and helping them improve their social relationships and quality of life are also important but these aims are secondary to keeping the patients alive.
Psychological therapies seem to work for suicide prevention. A Cochrane review of the randomised trials of psychosocial interventions in adults from 2016 showed that cognitive behavioural therapy reduced the occurrence of repeated self-harm compared to treatment as usual (odds ratio 0.70, 95% confidence interval 0.55–0.88; 17 trials and 2665 patients). 1 This is a remarkable result, not least because the patients in the control groups also received psychological support.
Deliberate self-harm is one of the strongest predictors of suicide, 2 but the suicidal intent varies and, most often, self-harm is not a suicidal attempt but a cry for help or a reaction to unbearable life circumstances. In the Cochrane review, the term ‘self-harm’ was used to describe all intentional acts of self-poisoning or self-injury, irrespective of degree of suicidal intent or other types of motivation. Accordingly, the 17 trials in the meta-analysis of cognitive behavioural therapy included some that had studied self-harm, some that had studied suicide attempts and some that had included both types of patients.
We decided to find out whether or not cognitive behavioural therapy reduces repeated suicide attempts, which is a more important outcome than repeated self-harm without suicidal intention.
Methods
Searches and selection of trials
We used the same methods as those described in the Cochrane review 1 but included all age groups and therefore also consulted a similar Cochrane review in children. 3
We included those randomised trials from the two Cochrane reviews that had compared cognitive behavioural therapy or problem-based learning, which is an integral part of this therapy, 1 with treatment as usual in patients who had engaged in any type of suicide attempt in the six months before trial entry resulting in presentation to clinical services. We updated the searches in the Cochrane reviews by searching PubMed using the keywords random* AND suicide attempt* (October 2013 to 17 February 2017). We also wrote to the primary investigators for the trials described as ongoing in the two Cochrane reviews and asked whether they had been published.
We included trials where the patients had attempted suicide previously. We did not contact the study authors to obtain unreported data for the trials included in the Cochrane reviews, as the Cochrane authors had already done this and we did not need to contact the authors for the additional trials we included.
Outcome
Suicide attempt.
Data extraction and synthesis
The two authors judged independently whether a trial was eligible and extracted data on a number of patients and events. Disagreements were resolved by discussion.
We calculated the pooled risk ratio and its accompanying 95% confidence interval, which we prefer to use when events are not rare. In order to compare our results with the results in the Cochrane reviews, we also calculated the odds ratio. We used the Mantel–Haenszel method for dichotomous data and a random effects model. The meta-analyses were performed using ReviewManager, version 5.
Results
The two Cochrane reviews had included 17 trials in adults and one in children of cognitive behavioural therapy, eight of which addressed suicide attempts only (all in adults). These eight trials were included in our review.4–11
Our PubMed search yielded 263 records, of which 249 were clearly irrelevant and two described the protocols for planned trials. We assessed the remaining 12 records for eligibility. In nine trials, the intervention was not cognitive behavioural therapy,12–20 and one trial was not about previous suicide attempts although it had ‘suicide survivors’ in the title; it included relatives to people who had committed suicide. 21 The two remaining trials were included in our review. Our contacts to the investigators for ongoing trials did not yield additional trial results.
Patient characteristics and trial quality.
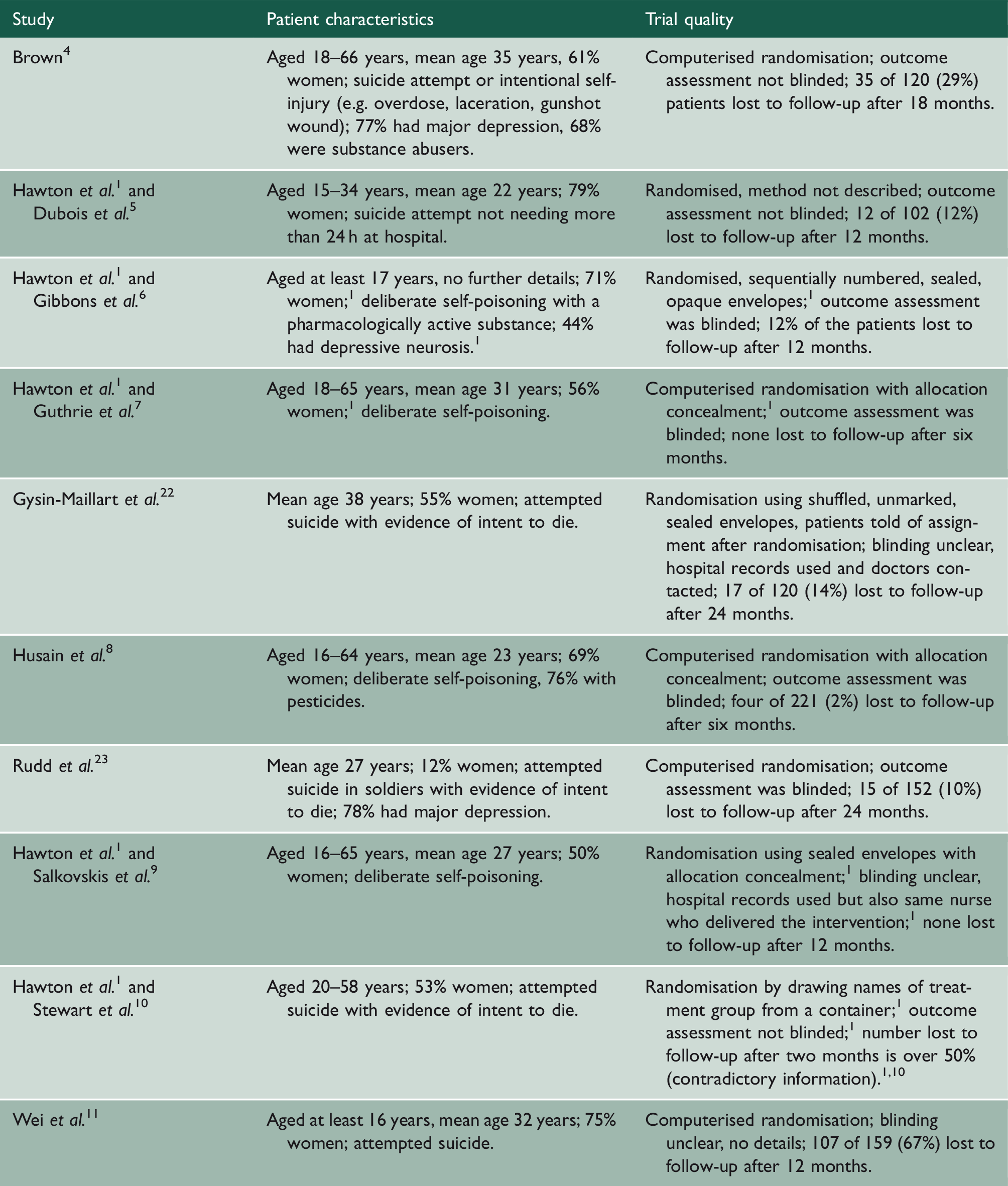
What constituted a previous suicide attempt was not explicitly defined in three trials.5,11,23 In four trials, it was deliberate self-poisoning;6–9 in one trial, most patients had self-poisoned; 4 one trial required a reported suicidal intent; 10 and one trial required such an intent either implicitly or explicitly. 22
Interventions.
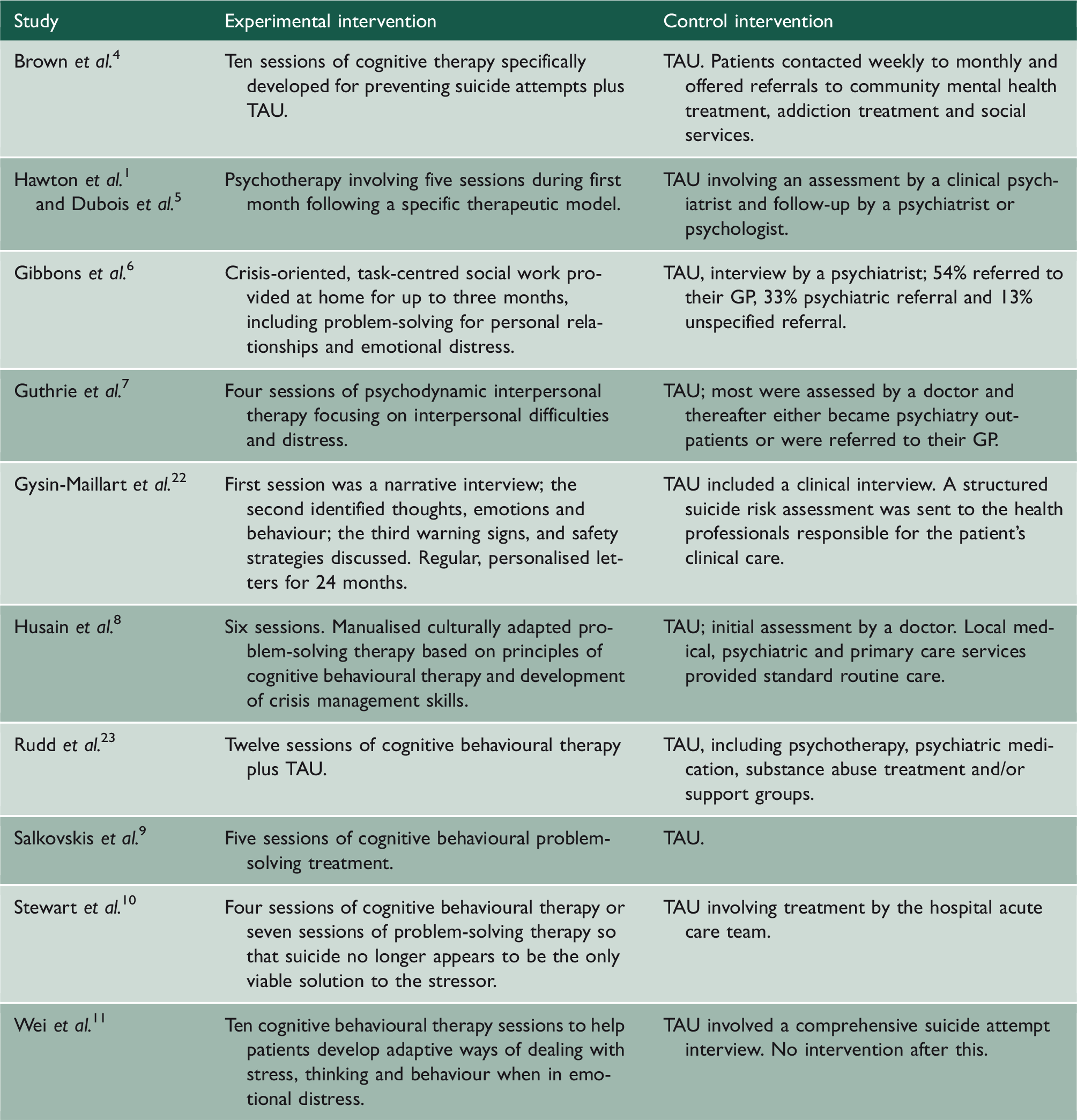
TAU: treatment as usual.
When we compared our data with those in the Cochrane review, we confirmed the number of suicide attempts apart from one trial 10 where we both found four versus two attempts in the cognitive behavioural therapy group and the control group, respectively, whereas the Cochrane review reported three versus two. 1 We used four versus two in our analyses.
In seven trials, the patients were randomised immediately after the suicide attempt; in two trials within 48 h, and in one trial, within seven days. The results were reported after a median follow-up of one year after randomisation. Cognitive behavioural therapy compared to treatment as usual reduced the risk of a new suicide attempt (Figure 1; risk ratio 0.47; 95% confidence interval 0.30–0.73; p = 0.0009; I2 = 57%; ten trials, 1241 patients and 219 events). One trial was an outlier with an unusually large effect;
22
if this trial is excluded, the risk ratio becomes 0.61 (0.46–0.80) and the heterogeneity in the results disappears (I2 = 0%).
Meta-analysis of suicide attempts. CBT: cognitive behavioural therapy; TAU: treatment as usual.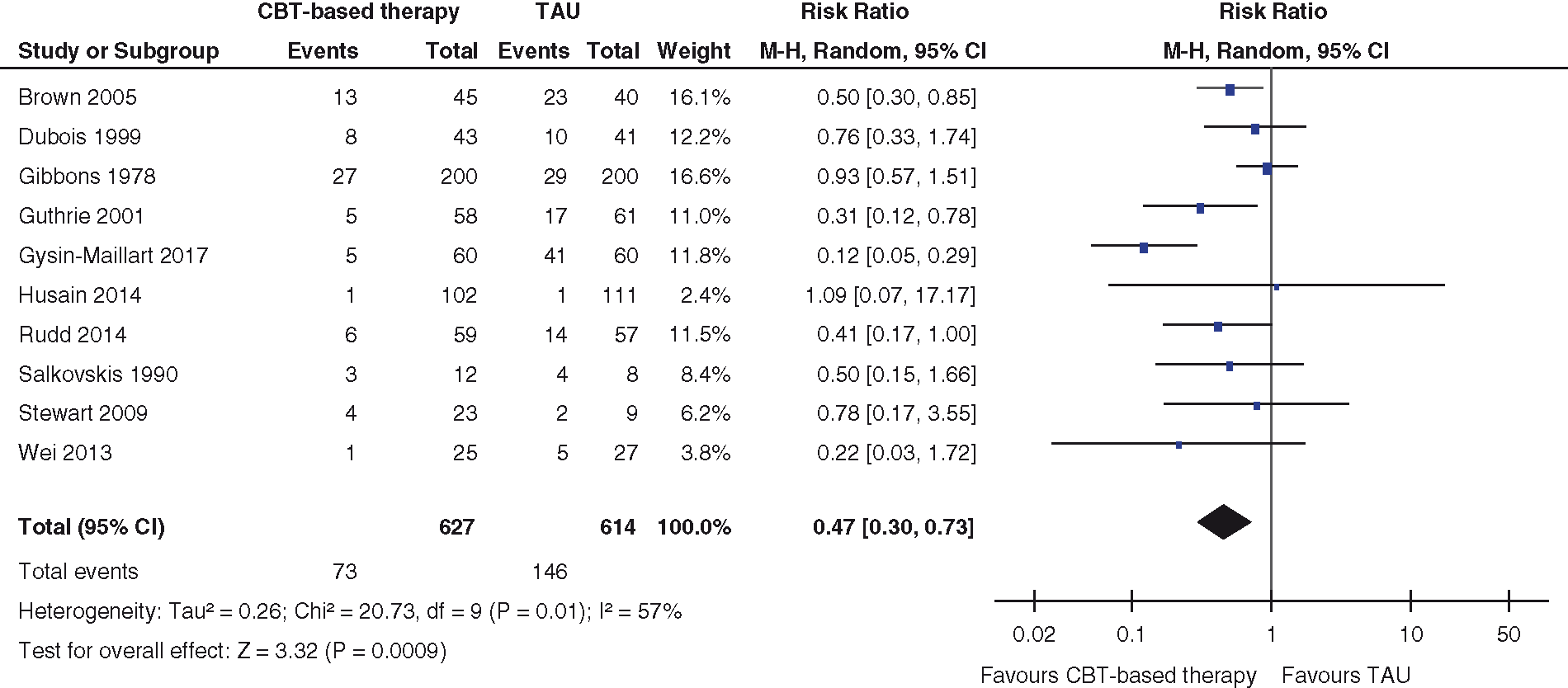
If we include only the eight trials also included in the Cochrane review, the odds ratio is 0.51 (0.32–0.83; I2 = 21%) for repeated suicide attempts, which is similar to the odds ratio in the Cochrane review for repeated self-harm, including suicide attempts, odds ratio 0.70 (0.55–0.88; I2 = 14%).
Only seven suicides were reported in the ten trials we included, three versus four.1,4,8,23
Discussion
We found that cognitive behavioural therapy compared to treatment as usual in patients with a previous recent suicide attempt halved the risk of a new suicide attempt. This is a very large effect. If the control group had received no treatment at all, the effect might have been even greater. 24
It is rarely possible to blind participants to psychological therapy, and the authors of the Cochrane review classified most of trials as having high risk of bias for blinding of participants. 1 However, we do not agree that this is an important problem with the trials we reviewed. First, our outcome, a new suicide attempt, is pretty objective. Second, any bias related to this outcome would be expected to be small compared with the size of the effect we found. Third, it is not clear why any bias would be expected to exaggerate the effect of cognitive behavioural therapy compared to the psychological support or therapies that were given to control group patients.
There were dropouts in the trials, and the Cochrane authors dealt with this by including only suicide attempts on those participants whose results were known, using as the denominator the total number of participants with data on the absence or presence of suicide attempts. We agree with this approach. Dropouts are concerning if there are differential reasons for dropout in the two groups but we found no data or plausible reasons suggesting that this was the case.
It was not an inclusion criterion in the trials that the patients were depressed and it could have been difficult to find out, since the trials were based on patients admitted to an emergency ward, some of whom were unconscious. However, it is likely that most patients attempting suicide will fulfil the criteria for a depression diagnosis, which the trial with the most events confirmed: the Beck depression inventory showed that most patients were depressed. 6 In agreement with this, the trial with the third-most events reported that, ‘At baseline, 77% had a major depressive disorder’. 4
In clinical guidelines all over the world, the standard treatment for severe depression is not psychotherapy but antidepressant drugs. This is not evidence-based medicine, as this recommendation goes directly against the most reliable evidence we have. For more than a decade, drug regulators have warned against using antidepressant drugs in children and adolescents because they increase the risk of suicide, aggression and violence.25,26 Until recently, it was difficult to know whether the suicide risk was also increased in adults, as there has been massive under-reporting and even fraud in the reporting of suicides, suicide attempts and suicidal thoughts in the placebo-controlled trials.25,27 However, a 2016 systematic review of the randomised trials showed that antidepressants double the occurrence of events that can lead to suicide and violence in adult healthy volunteers. 28 Another recent systematic review, which was based on clinical study reports obtained from the European Medicines Agency, showed that FDA defined precursor events for suicide and violence were 4–5 times more common with duloxetine than with placebo in randomised trials in middle-aged women with stress urinary incontinence. 29 It would have been impossible to demonstrate this based on the published trial reports.
It is therefore now clear that antidepressants increase the suicide risk at all ages while cognitive behavioural therapy decreases the suicide risk substantially. Cognitive behavioural therapy should therefore be the preferred treatment of depression of all severities. In our view, antidepressants should not be used at all, as they are unlikely to have a true effect on depression outcomes that matter to patients. 25 It is even unlikely that they have a true effect as measured with the Hamilton depression scale. 25 An arbitrary threshold for clinical significance once recommended by the National Institute for Clinical Excellence in England is 3 on this scale, but this is far too little, as the smallest effect that can be perceived on the scale is 5–7.30,31
Several meta-analyses have found that the effect of antidepressants is larger if the patients are severely depressed,32–34 and antidepressants are generally recommended for severe and sometimes moderate, but not mild depression. However, the reported effects are small for all severities of depression, e.g. in the most recent meta-analysis, it was 2.7 for patients with a baseline Hamilton score above 23, which is considered very severe depression, 33 and 1.3 for milder degrees of depression. 34 Moreover, it is likely just a mathematical artefact that the effect seems to be slightly larger in severe depression. Due to the conspicuous side effects of antidepressants, the placebo-controlled trials have not been adequately blinded, and this introduces a bias favouring the drugs when subjective outcomes like those on the Hamilton scale are being evaluated. 25 This bias can be large, and it was 68% on average when the observers had not been blinded compared to blinded observers in the same trials in a review that included all diseases, 35 but it need not be large in order to explain the results in the meta-analyses of antidepressant drugs. Since the baseline scores for severe depression are larger than for mild depression, any bias – whether or not related to insufficient blinding – will influence the measured result more in patients with severe depression than in those with mild depression.
It is very simple, really. It is therefore surprising that this bias, as far as we know, has not been described before in any paper about antidepressant drugs. If we assume, for example, that the unblinding bias is 10% when estimating the effect in the antidepressant group, and that for the simplicity of the example there is no bias in the placebo group and nothing happens between baseline and the final visit, then a Hamilton baseline score of 25 would still be 25 after treatment, but because of the bias, there would be a 2.5-point difference between drug and placebo. If the baseline is 15, the difference would only be 1.5.
Conclusions
Cognitive behavioural therapy halves the risk of a new suicide attempt in patients who have previously attempted suicide and it should therefore be the preferred treatment for all patients with depression. The clinical guidelines for treating depression need to be changed to reflect this. We believe antidepressant drugs should be avoided. They increase the risk of suicide; they have many other important harms; and their clinical effect on depression is doubtful.