
Abstract
This is the eighth article in our series on population healthcare
The key distinction between leadership and management is that leadership creates the organisation of the culture and managers work within it. As we have emphasised, what is needed for population healthcare is a collaborative culture and a culture of stewardship but once this culture has been developed people still have to deliver within it and that is the job of management.
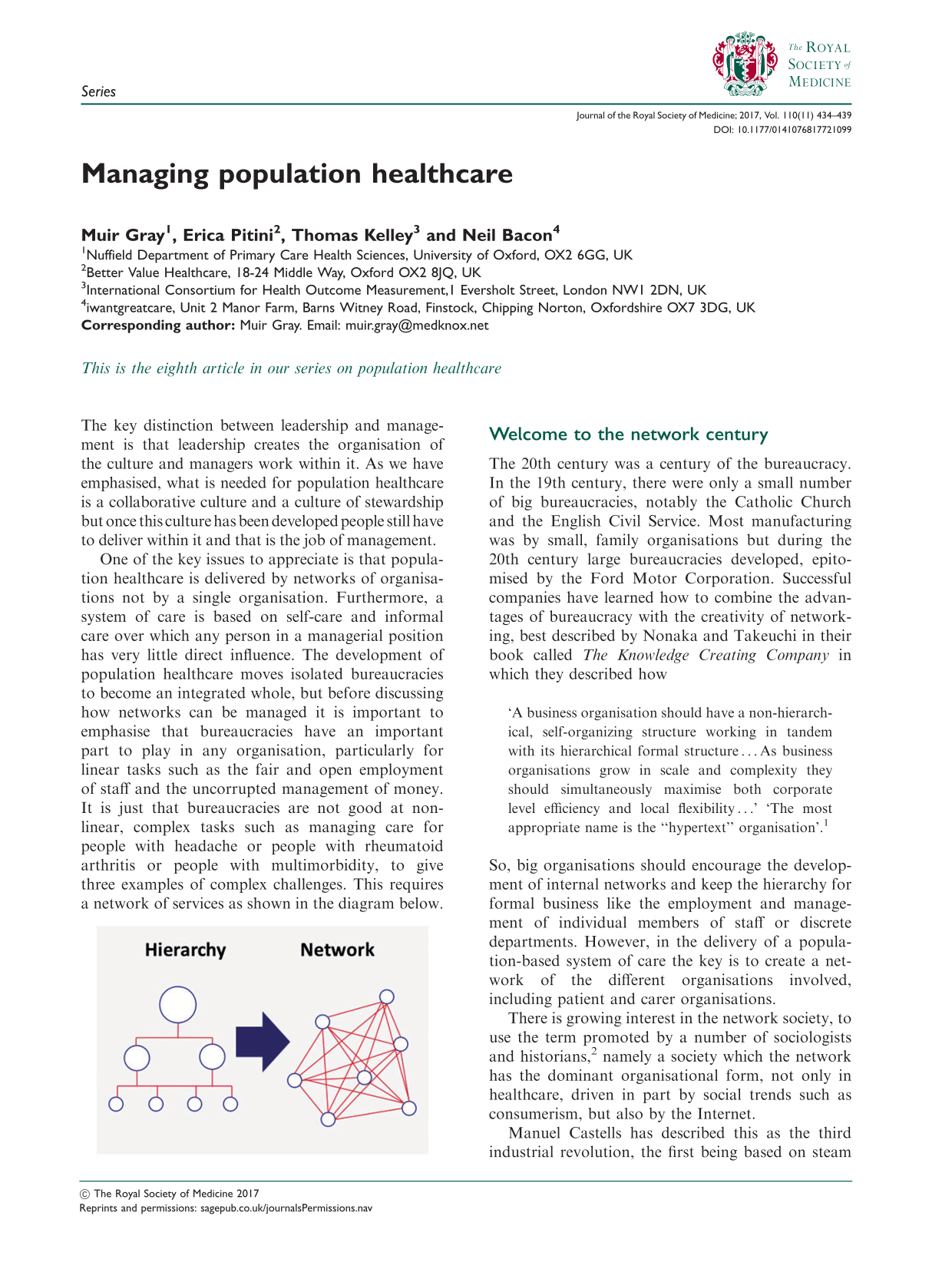
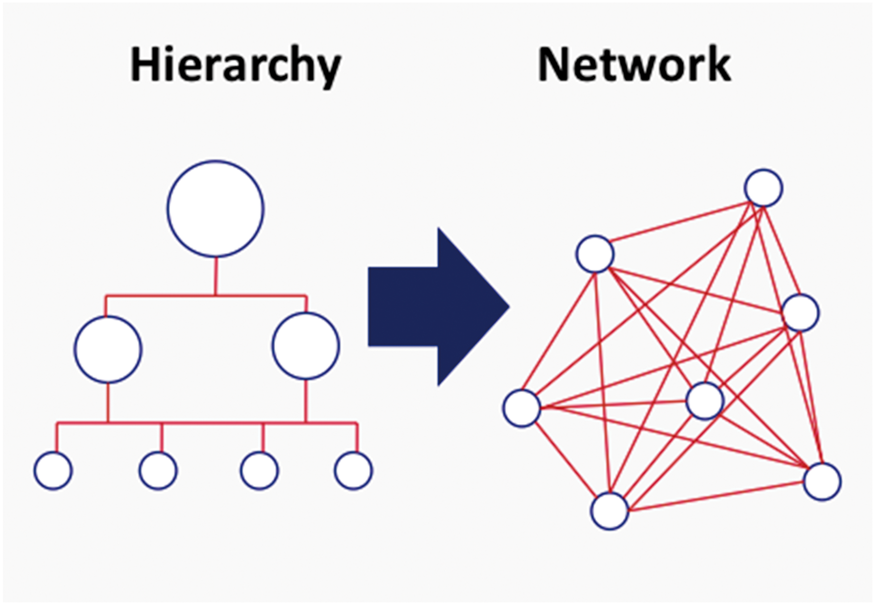
One of the key issues to appreciate is that population healthcare is delivered by networks of organisations not by a single organisation. Furthermore, a system of care is based on self-care and informal care over which any person in a managerial position has very little direct influence. The development of population healthcare moves isolated bureaucracies to become an integrated whole, but before discussing how networks can be managed it is important to emphasise that bureaucracies have an important part to play in any organisation, particularly for linear tasks such as the fair and open employment of staff and the uncorrupted management of money. It is just that bureaucracies are not good at non-linear, complex tasks such as managing care for people with headache or people with rheumatoid arthritis or people with multimorbidity, to give three examples of complex challenges. This requires a network of services as shown in the diagram below.
Welcome to the network century
The 20th century was a century of the bureaucracy. In the 19th century, there were only a small number of big bureaucracies, notably the Catholic Church and the English Civil Service. Most manufacturing was by small, family organisations but during the 20th century large bureaucracies developed, epitomised by the Ford Motor Corporation. Successful companies have learned how to combine the advantages of bureaucracy with the creativity of networking, best described by Nonaka and Takeuchi in their book called The Knowledge Creating Company in which they described how ‘A business organisation should have a non-hierarchical, self-organizing structure working in tandem with its hierarchical formal structure … As business organisations grow in scale and complexity they should simultaneously maximise both corporate level efficiency and local flexibility …’ ‘The most appropriate name is the “hypertext” organisation’.
1
There is growing interest in the network society, to use the term promoted by a number of sociologists and historians, 2 namely a society which the network has the dominant organisational form, not only in healthcare, driven in part by social trends such as consumerism, but also by the Internet.
Manuel Castells has described this as the third industrial revolution, the first being based on steam and coal, the second on high tech such as computers but with the third being based on three forces: citizens, knowledge and the Internet. This applies to healthcare with the first health revolution, public health revolution, being based on simple empirical decision-making; the second, the high tech medical revolution being based on science; and the third healthcare revolution being driven by three forces: citizens, many of whom are patients or carers, knowledge and the smartphone.
Good leadership creates the collaborative culture in which networking can flourish, but how is a network managed in the absence of the management skills of direct lines of reporting, rewards and sanctions that are thought to be necessary in a bureaucracy although they have a part to play?
A network delivering population healthcare is an organisation. As such, the rules of good general management apply and will not be rehearsed here. However, there are a number of specific skills involved in managing a network and the first step is that the definition of ‘network' needs to be agreed and there are several different uses of the term, as can be expected in a world that is evolving rapidly. Some of the key examples of the term ‘network’ are set out below. A network … emerges from the bottom up; individuals function as autonomous nodes, negotiating their own relationships, forging ties, coalescing into clusters. There is no ‘top’ in a network; each node is equal and self-directed. Democracy is a kind of network; so is a flock of birds, or the World Wide Web.
3
The [managed clinical] network … has a formal management structure with defined governance arrangements and specific objectives linked to a published strategy [are] linked groups of health professionals and organisations from primary, secondary and tertiary care working in a coordinated manner, unconstrained by existing professional and existing [organisational] boundaries to ensure equitable provision of high quality clinically effective services.
4
These are enterprises in which people exchange things with one another.
5
Networking is a broad concept referring to a form of organized transacting that offers an alternative to either markets or hierarchies. It refers to transactions across an organization’s boundaries that are recurrent and involve continuing relationships with a set of partners. The transactions are coordinated and controlled on a mutually agreed basis that is likely to require common protocols and systems, but do not necessarily require direct supervision by the organization’s own staff.
6
There are a number of specific approaches particular to the management of networks that need to be considered and these are not usually taught in general management courses. The key principles include:
Be clear about the population to be served Set clear objectives Agree the outcome measures Get feedback form service users Identify comparison populations to create a community of practice Become a learning organisation Be accountable to the population served as well as to the funding agency
Be clear about the population to be served
There are different ways of defining populations and when a geographic term is used it usually refers to a jurisdiction, namely a politically defined population where the organisation that is responsible has politically delegated authority to manage money. Populations have names like Derbyshire, Cardiff, Lothian, Leeds or Wandsworth. These are indeed populations but in healthcare the populations that are the focus of clinical networks and systems are rarely exactly coterminous with the populations of jurisdictions. Often healthcare networks have evolved over the years by referral patterns to a particular hospital and these in turn evolved reflecting public transport flows before the era of the motor car.
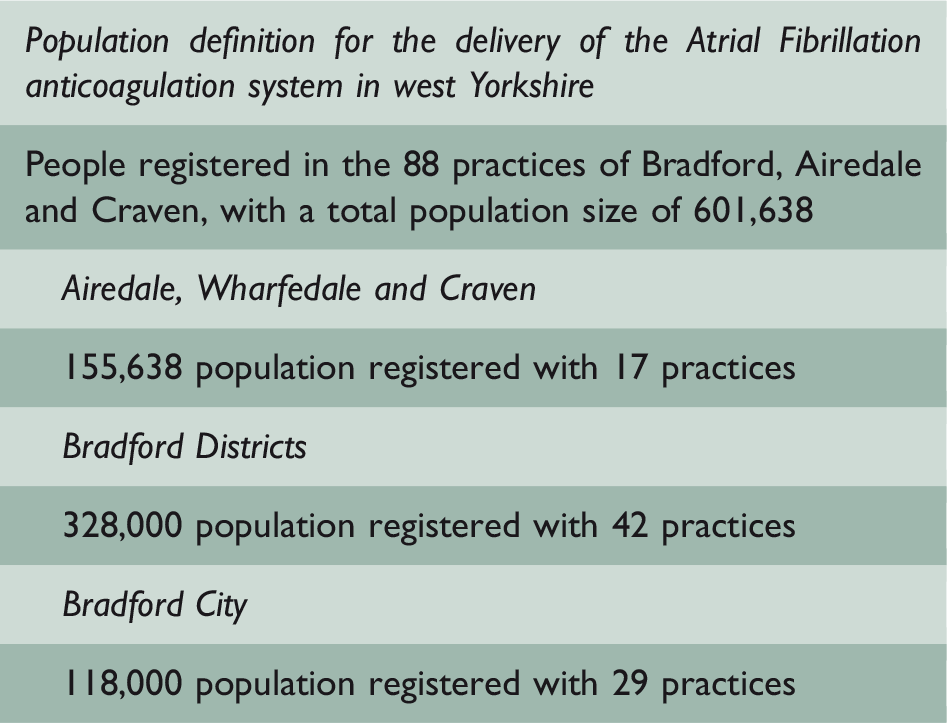
It is therefore essential to be clear about the population served and the population served by a system providing for relatively common condition without super specialist interventions may be anything from 200,000 to 500,000. Where super specialist services are involved, for example neurosurgery, then the population may be bigger so one hospital may be involved in a number of different networks serving different populations.
Set clear objectives
In the military there is a clear distinction between strategic and operational command. The aim of strategic command is to define the objectives of the mission. Operational commanders then have to achieve those objectives and the military is very good at letting people who are operational commanders decide precisely how they will achieve their objective taking into account local history and geography. Too often in health services the people at the top of the bureaucracy try to lay down detailed guidelines for operational commanders to follow instead of setting the strategic objectives. An example of a set of strategic objectives designed to reduce the incidence of stroke among people with atrial fibrillation is set out below:
To identify people with atrial fibrillation To assess risk accurately in all people known to have atrial fibrillation To treat people safely and effectively To phase out ineffective treatment with aspirin To ensure people with atrial fibrillation make a well-informed decision that takes their values into account To make the best use of resources To promote and support research To create a powerful community of practice and develop staff, both as individuals and teams To produce an annual report for the population served and to support quality improvement
The objectives give direction but what is needed also is a clear set of outcomes so that people would know if the objective was being attained or not.
Agree the outcome measures
For 20 years health services have been obsessed with quality and safety, and rightly so. Based on concern about poor quality and safety, highlighted in a number of reports about the turn of the century and inspired by the record of quality in Japanese industry and safety in the airline industry, health services focused on quality and safety, but although necessary this is not sufficient. Low quality care is certainly of low value but high quality care is not necessarily high value. For example, there has been a 10% increase in imaging in many countries in the last five years, all the images of high quality but what has been their value. The need to focus on quality was accepted, but in both the UK and the USA the need to focus on value was clearly stated. The NHS in England introduced commissioning in 2006 and published its first Annual Population Value Review which emphasised that: The aim of the commissioner is to maximise value for the population they serve from the resources they invest on their behalf. They can do this in two ways, directly and indirectly. Firstly, the Commissioner can maximise value by allocating the resources they control among the patient and population groups within that patient to best effect. Value is maximised when it is impossible to reallocate resources from one patient or population group to another to achieve more benefit or less harm. This is sometimes termed allocative efficiency. Secondly, the Commissioners can use their contracting power to help providers of health care improve the quality and safety of the care they provide, while minimising its cost. This is sometimes termed technical efficiency. Value in any field must be defined around the customer, not the supplier. Value must also be measured by outputs, not inputs. Hence it is patient health results that matter, not the volume of services delivered. But results are achieved at some cost. Therefore, the proper objective is the value of health care delivery, or the patient health outcomes relative to the total cost (inputs) of attaining those outcomes. Efficiency, then, is subsumed in the concept of value. So are other objectives like safety, which is one aspect of outcomes.
Evidence shows that using information from PROMs improves communication and decision-making between doctors and patients as well as patient satisfaction with care.9,10 Beyond clinical care, collection of PROMs is potentially useful for benchmarking and research regarding patient-centred care.
PROMs collection has been implemented in several countries, particularly for patients with chronic conditions. For example, the UK NHS routinely collects PROMs for selected elective surgeries such as hip and knee replacements, groin hernia and varicose veins. 11 In the USA, the Patient-Reported Outcomes Measurement Information System collects person-centred measures of physical, mental and social health. 12
Nevertheless, to make collection of PROMs part of routine care, some barriers have to be overcome. The first barrier is technological. PROMs need to be collected and recorded through dedicated electronic platforms and patients should be able to access them over the Internet or on a smart device. The second barrier relates to clinicians. They fear that using PROMs may increase their workload without adding additional information than those achievable simply talking to patients. Third, consensus on which specific outcome to collect and standardisation of the related clinical and office procedures is needed.
13
Emerging information and communication technologies are spurring the development of new systems designed to capture and use the patient voice. However, the extent to which these systems can improve care will depend on how effectively clinicians respond to the patient voice.
14
Burden of care to the patients
Hospital visits Treatment side effects Complications
Functioning and disease control
Symptom control Activities of daily living Independence Psychosocial health
Survival and disease control
Mortality
Focusing on outcomes is a very good management technique in any type of healthcare, particularly population healthcare.
Get feedback from service users
For learning to occur, it is essential for the system to have feedback. One type of feedback that is being collected is feedback from patients about their experience of care. Outcome can be measured objectively, for example by using the Oxford Knee Score, but it is also very important to record the patients’ subjective experience. The company called IWantGreatCare does this, and although there was great concern among some parts of the medical profession when they started their service the general feedback has been very positive and has actually improved the morale of the clinicians. Thomas Lee, a Harvard academic and medical director of Press Ganey, an American company with a particular expertise in consumer, analysed experience and related it to key outcome measures. Here is his conclusion: My colleagues and I have analysed data on patient experience as well as publicly reported data on patient safety and business performance. We have found that these performance ‘outcomes’ are correlated — that is, the organizations with better patient experience also has better safety records and report better financial margins.
15
Identifying and working with similar populations
In England, the NHS Rightcare Programme not only gave information about the performance of services for a population but also they told that population about the ten other populations in England most like them in sociodemographic terms. Often the populations that surround the population served by a particular network are unlike them, for example they may be in rural areas surrounding a city, and it is important for like to be compared with like. This can be done using data but a better approach is to develop a community of practice described by Etienne Wenger 16 who wrote that ‘For communities, it means that learning is an issue of refining their practice and ensuring new generations of members learn from experience’.
It is good to meet and share experiences, learning from both the successes and the failures of the others, with failure often being more useful for learning. This type of openness with others encourages people within each network to appreciate that learning is not only done in the workshop or conference but in the course of work, provided that the organisation in which they work is committed to being a learning organisation.
Become a learning organisation
A learning organisation has been defined the following way by Peter Senge in his book The Fifth Discipline: an organisation in which people see learning as part of working. The person managing the network needs to be encouraging learning. When something has gone well it is important not just to celebrate what has happened but why it has happened and what steps could be taken to include the probability of success in other projects. This was the subject of a special Harvard Business Review which emphasised that Peter Senge, 17 who popularised learning organisations in his book The Fifth Discipline, described them as places ‘where people continually expand their capacity to create the results they truly desire, where new and expansive patterns of thinking are nurtured, where collective aspiration is set free, and where people are continually learning how to learn together’.
Ikujiro Nonaka
1
defined knowledge-creating companies as places where inventing new knowledge is not a specialized activity … it is a way of behaving, indeed a way of being, in which everyone is a knowledge worker. A learning organization is an organization skilled at creating, acquiring and transferring knowledge, and at modifying its behaviour to reflect new knowledge and insights. When did this project start and, if complete, when was it completed? What was the setting and population covered? What were you seeking to achieve? Why did you decide to take action? What did you do? Why did you choose this approach? What was the outcome? What did you learn? What is the single most important line of advice which you can give to others starting a similar project? Where can people find out more?
Learning organisations do not just offer education and training, they do action learning defined by two of the leading writers as ‘a continuous process of learning and reflection that happens with the support of a group of “set” of colleagues, working on real issues, with the intention of getting things done’. 18 Part of this process of learning of course is the production of an annual report for the population served.
Be accountable to the population served
The accountability is usually thought of in bureaucratic terms in the one part of a health service that is accountable to another part of the health service in a higher part of the bureaucratic hierarchy. However, Mark Friedman, writing about education in the United States, has developed the concept of population accountability, namely that we should be accountable to the people served as well as to our political masters: ‘Accountability is a relationship between persons or groups, where one is responsible to another for something important’. 19
The application of this principle to health service accountability has been defined in the following way: We see accountability as a relationship based on the provision of information about performance from those who have it to those who have a right to it, either because they have the power to reward or sanction, or because they have a ‘right to know’.
20
In managing population healthcare, therefore, the concept of population accountability is of central importance.