
Abstract

This is the VIIth article in a series on population healthcare.
The distinction between leadership and management is reasonably well agreed. The leadership of an organisation creates the culture and the management works within that culture. If, for example, the leadership speaks with disrespect of people working in other organisations, then this will permeate the whole organisation. The Toyota Motor Corporation has taught us much about systems, but from the earliest days of studying the Japanese miracle, there was at least as much interest in the culture of the successful Japanese companies as there was in their systems and an appreciation that culture and systems were interwoven. In their study of The Toyota Product Development System, Morgan and Liker
1
emphasised that ‘leadership … and a company’s culture are inextricably intertwined’. Edgar Schein emphasised the importance of this when he said that: … if one wishes to distinguish leadership from management or administration one can argue that leadership creates and changes culture while management and administration act within a culture.
2
The culture of a group can now be defined as a pattern of shared basic assumptions that was learned by a group as it solved its problems of external adaptation and internal integration, that has worked well enough to be considered valid and, therefore, to be taught to new members as the correct way to perceive, think, and feel in relation to those problems.
2
Difference between the old culture and the new culture.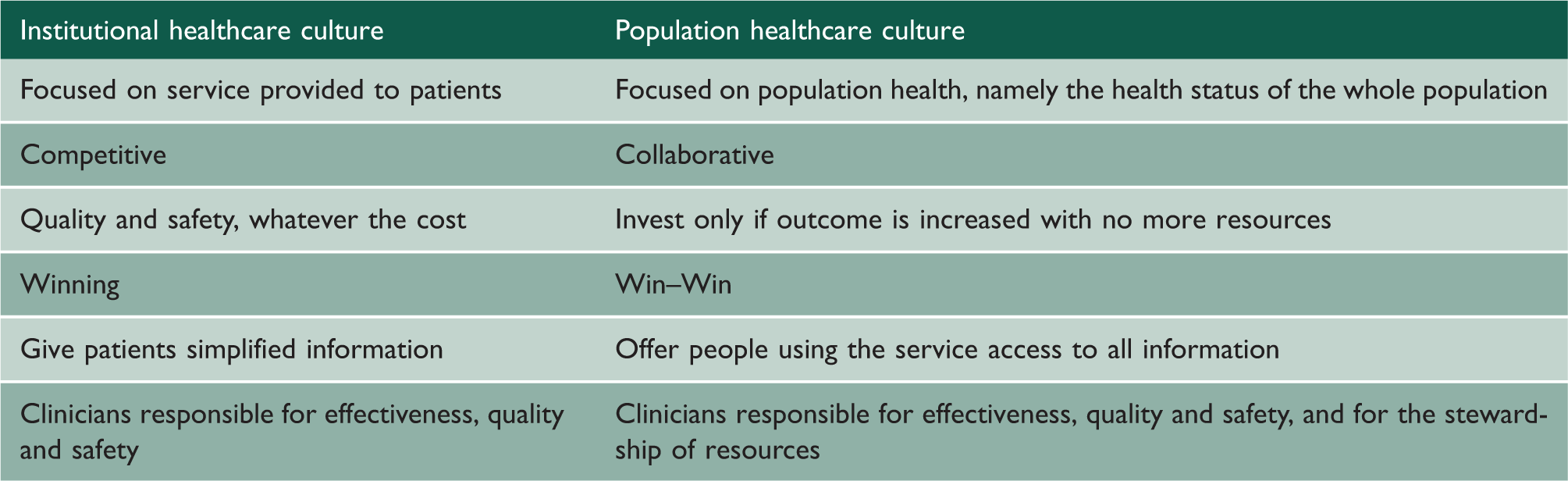
There are different ways in which culture can be created or changed. One way, obviously, is the actual behaviour of key people in the organisation, for example in what they say and do in relating to the people who work within that organisation. The leadership of a collaborative culture must ensure that people in their own sector do not speak with disrespect of people in another sector. General practitioners complaining about ‘over-investigation’ by hospital doctors, and hospital doctors complaining about general practitioners ‘missing’ what appear to them to be easy diagnoses, with both parties failing to understand the importance of the predictive value of a test, as distinct from its sensitivity, does not create the right collaborative culture. There are, however, a number of culture change activities that are more cognitive and which can be delivered through training or by influencing the environment in which people think and work:
Exposing unwarranted variation; Creating a common language; Using Programme Budgeting to create the culture of stewardship.
Exposing unwarranted variation
One of the drawbacks of focusing solely on quality and safety is that it overlooks the fact that there may be big differences in the rate of high-quality, safe services. The first work on this was done by Jack Wennberg 3 when he published the Dartmouth Atlas of Health Care. This had a huge impact in the United States. It challenged the cultural assumption that by focusing on evidence-based decision-making, reinforced by the production of evidence-based guidelines, care would become uniform. Even allowing for the size and diversity of the United States, what was revealed by his work was surprising, shocking and culture changing. The Atlas and the specialist reports that followed it demonstrated that there were variations in care that could not be explained by variations in need. Quite simply, interventions for conditions for which medical judgement played little part, repair of fractures of the neck of the femur, for example, showed little variation, whereas in the large part of medicine in which clinician choice plays a part in deciding who should have treatment and who should not, there were huge variations.
The Dartmouth Atlas of Health Care and the NHS Atlases of Variation which were based on the methods of Professor Jack Wennberg showed variation in investment, access, quality, safety and outcome – variation in everything. Some of this variation could be explained by variation in need, for example treatment of children with thalassemia takes place at a higher rate in London than Edinburgh, but much of the variation is unwarranted, an adjective defined by Jack Wennberg 3 in his intellectual autobiography as ‘variation in the utilisation of healthcare services that cannot be explained by variation in patient illness or patient preferences’.
Furthermore, Wennberg went on to talk about supply sensitive care which is not about a specific treatment per se; rather, it is about the frequency with which every miracle care is used in treating acute and chronic illnesses. Remedying variation and supply sensitive care requires coming to terms with the more care is better assumption.
3
that more care is always better; that clinical practice is now standardised because of evidence-based guidelines and evidence-based clinical practice; that additional resources are always needed to improve access to, or quality of, care.
Furthermore, Jack Wennberg et al. at Dartmouth and in Boston, notably Al Mulley et al., emphasised that some of the variation was due to the fact that a patient’s preferences were not being taken into account, leading to the concept of preference sensitive care with: “preference-sensitive” care, interventions for which there is more than one option and where the outcomes will differ according to the option used because patients delegate decision making to doctors, physician opinion rather than patient preference often determines which treatment patients receive. I argue that this can result in a serious but commonly overlooked medical error: operating on the wrong patients – on those who, were they fully informed, would not have wanted the operation they received.
4
Thus, the publication of unwarranted variation, either between populations contributes to culture change. So too does the development of a new language.
Creating a common language
The military culture, so often condemned as command and control, does in fact pay great attention to language or doctrine as they call it. In a rapidly changing world, particularly when working with people from a number of different organisations, it is essential to be clear about the meaning of the terms being used. As emphasised in the previous article, there is a new technical language about population healthcare, namely healthcare that focuses primarily on populations defined by a common need which may be a symptom such as breathlessness, a condition such as arthritis or a common characteristic such as frailty in old age, not on institutions, or specialties or technologies. Its aim is to maximise value for those populations and the individuals within them. For example, the language of systems, networks and pathways is helpful in changing culture, and here are ten key terms that need to be used with the same meaning by everyone.
^ A system is a set of activities with a common set of objectives with an annual report. ^ The network is the set of organisations and individuals that deliver the systems. ^ The pathway is the route most patients travel through the network. ^ Personalised value, determined by how well the outcome relates to the values of each individual. ^ Allocative, determined by how well the assets are distributed to different subgroups in the population
^ Between programme ^ Between system ^ Within system Technical, determined by how well resources are used for outcomes for all the people in need in the population.
There is another language which is unhelpful and counterproductive because it reinforces the old culture. The term ‘manager’, for example, sets management as a separate activity not done by clinicians, and it is more effective to talk about ‘people who manage’.
Sometimes a completely new term with which people are completely unfamiliar is helpful in changing culture. For example, the National Association of Primary Care launched the concept of the Primary Care Home, not as a new bureaucratic structure but as a new concept. They provide a clear description of the characteristics of the new approach which involves everyone working together ‘to meet the needs of a registered population’ but the concept is broad and new. The new term helped create a collaborative culture and is an excellent example of leadership. Another new term is the term stewardship.
Creating the culture of stewardship
Every culture has subcultures which are both shaped by and influence the principal culture of the organisation. In the leadership of services delivering care to individuals, it is essential to create not only a quality culture but also a safety culture and a culture of compassion. However, when creating a culture in population healthcare, another dimension has to be considered with subcultures relating the features of the new culture set out in Table 1, for example the collaborative subculture and the subculture of patient centredness but perhaps the most important is to develop a culture of stewardship.
Public reporting of CCG expenditure.
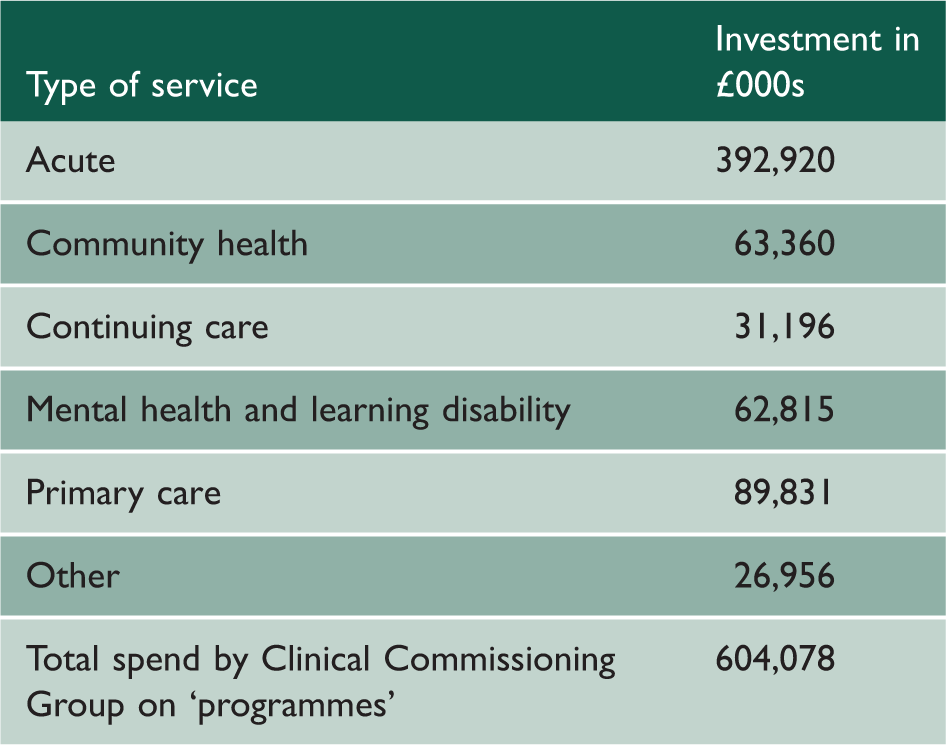
Large amounts of money go into ‘acute’ and ‘primary’ care but there is no indication of how much is going into musculoskeletal disease or respiratory disease. In England, the NHS has had programme budgeting for over a decade and the expenditure by programme varies from one part of the country to another, usually between 1.5- and 2-fold. However, the influence of programme budgeting is not only to reinforce the messages of variation but also to change the culture of clinicians so that they see themselves as the stewards of the resource. As stewards, they are responsible not only for spending the resource on effective high-quality, safe interventions day by day but also feeling responsible for ensuring that both individual patients and the population as a whole get good value from the resources available.
The term ‘stewardship’ is an old-fashioned term not easy to translate to other languages than English. In England, the steward looked after the land of the lord, who actually owned the land, but the good steward did not simply take as much wealth from the land as he could. He tried to leave the farms in a better condition than he found them. The same concept is highly relevant to the stewardship of healthcare. If clinicians do not make good use of the resources, there may not be a health service of the type they value for the generations to come. The concept of intergenerational equity was one that was developed in the environmental world but it is highly relevant to healthcare. The stewardship concept demands that we constantly ask the question: Will the resource be in better shape after my stewardship?
5
this is not simply about costs. It is about supporting doctors and other clinicians to ensure that the resources of the NHS are used in the most effective way possible to provide the best possible quality and quantity of care for patients … This process creates a higher value health care system where resources: cash, carbon and staff time, are released from some parts of the system to develop a new services or support struggling services. Reducing waste in today’s climate of constrained resource is really about creating the health care system that we want to have. It is not just about cutting corners or reducing spending. As responsible stewards, doctors can provide a more effective use of constrained economic and environmental resources. A cultural shift is required which calls upon doctors and other clinicians to ask, not if a treatment or procedure is possible, but whether it provides real value to the patient and genuinely improves the quality of their life or their prospects for recovery … Doctors should embrace the values of resource stewardship in their clinical practice
Leadership of population healthcare means taking a longer view than a view limited by the annual accounts or even a three-year plan. ‘Stewardship is to hold something in trust for another’ 7 and stewardship of a health service is to hold a health service in trust for the next generation.