
Abstract

Introduction
The most important context in which a medical doctor works is in the consultation or doctor–patient encounter, in which a complex blend of cognitive, psychomotor and interpersonal skills are deployed. Many of these are well established, such as the skills required to elicit findings on physical examination. Others, such as establishing and maintaining a relationship with the patient, are more recently recognised but an emerging evidence base supports their learning. 1
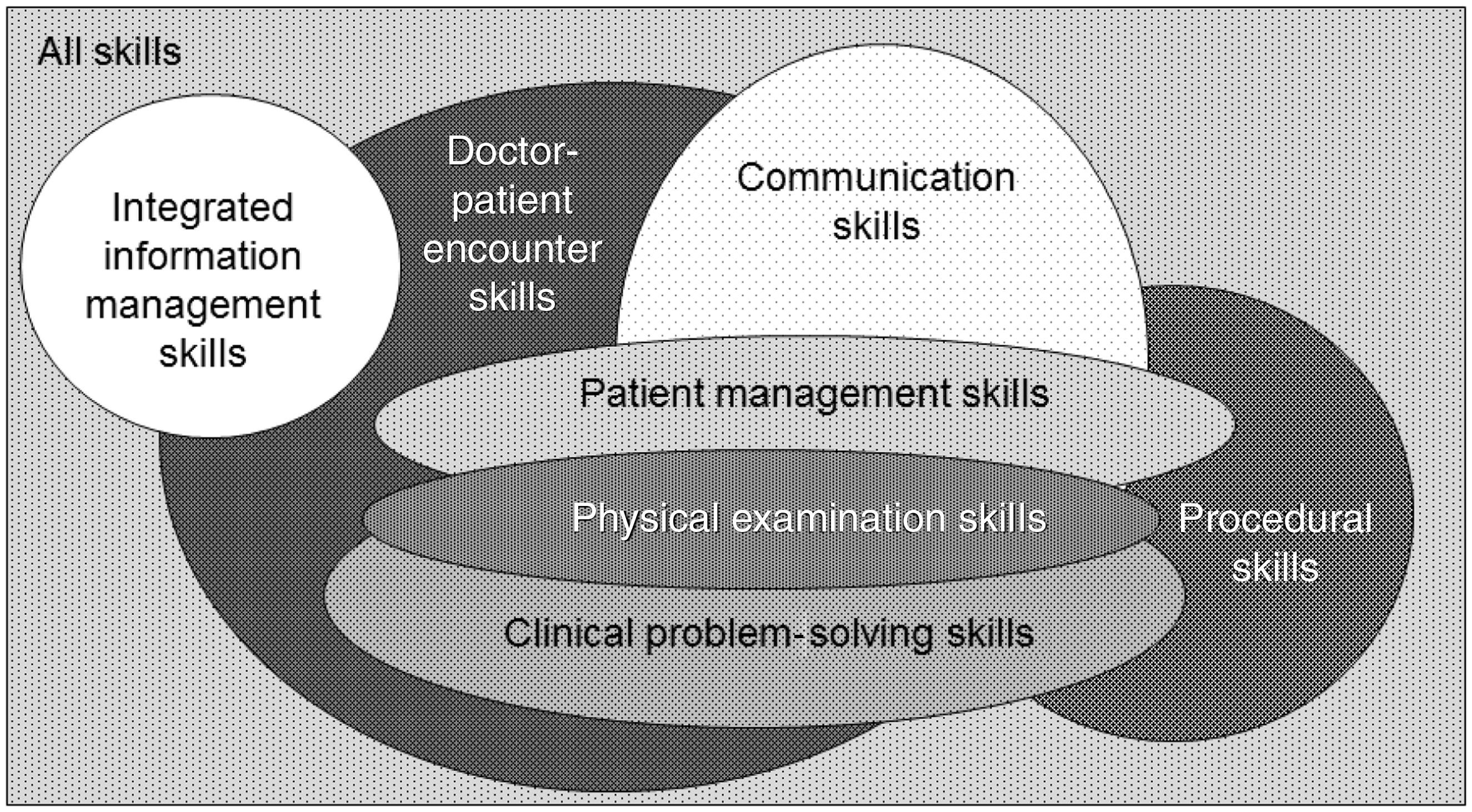
Good clinical outcomes require good clinical care, which in turn requires good clinical skills. Clinical skills are interdependent and context dependent. Those required to gather information, build relationships, structure the encounter and give information are formally integrated in the Calgary Cambridge Framework 1 ; the skills required to elicit the history, elicit appropriate findings on physical examination and clinical reasoning skills are intimately related and have been formally integrated in newer doctor–patient encounter models. 2 Even competent performance of clinical procedures requires interpersonal and team skills 3 as well as ‘pure’ psychomotor skills.
We use a unified skills model to support clinical skills tuition, which recognises this interdependence of clinical skills (Figure 1).
2
This blend of overlapping skills also includes integrated information management as a component doctor–patient encounter skill. This stance is supported by Outcomes for Graduates
4
which requires medical students to ‘use information effectively in a medical context’.
The relationship between skills required for the doctor–patient encounter.
2
This paper describes how we conceptualise integrated information management skills, why and how we teach them.
What is integrated information management within the doctor–patient encounter?
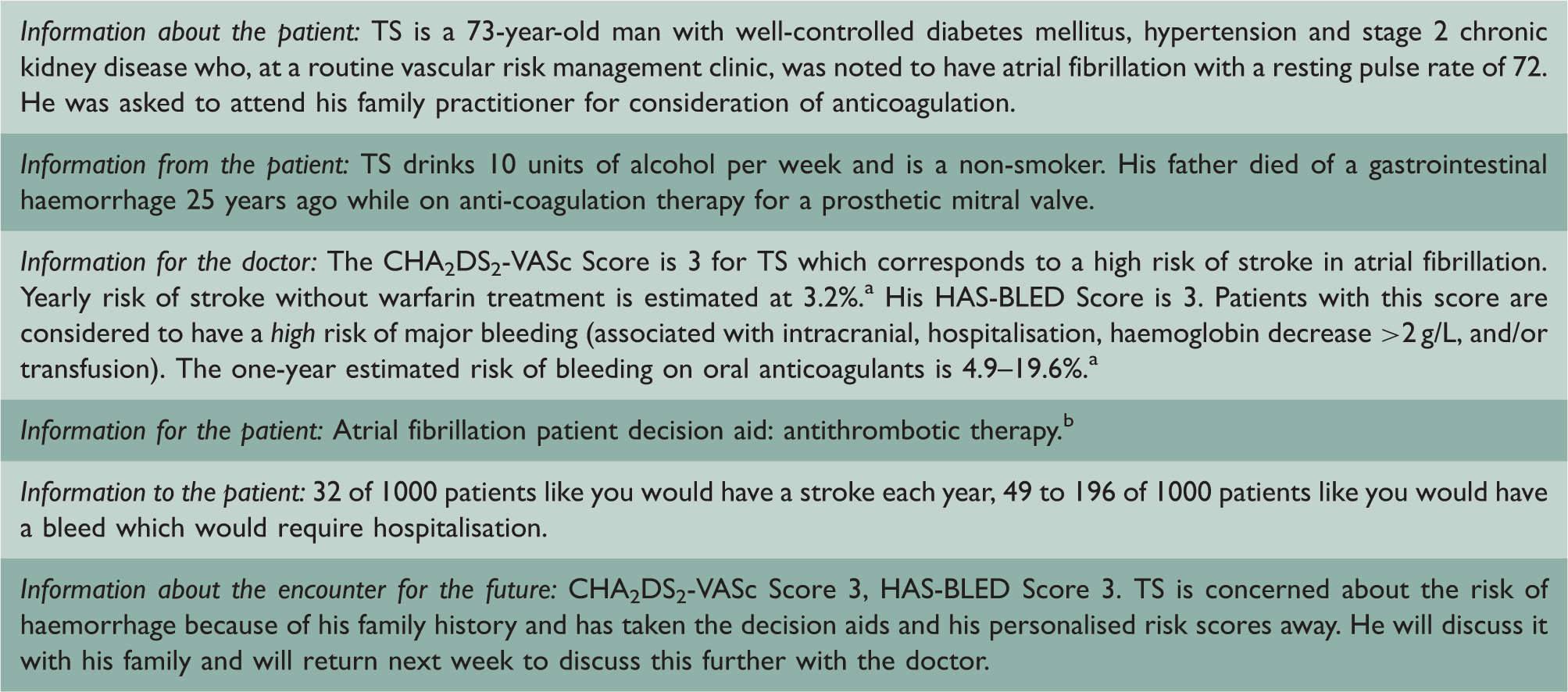
In the doctor–patient encounter, doctors manage six major information streams in an information-dense environment; four inputs and two outputs (Figure 2). Consider them in order of maximal flow:
Information streams in the doctor–patient encounter.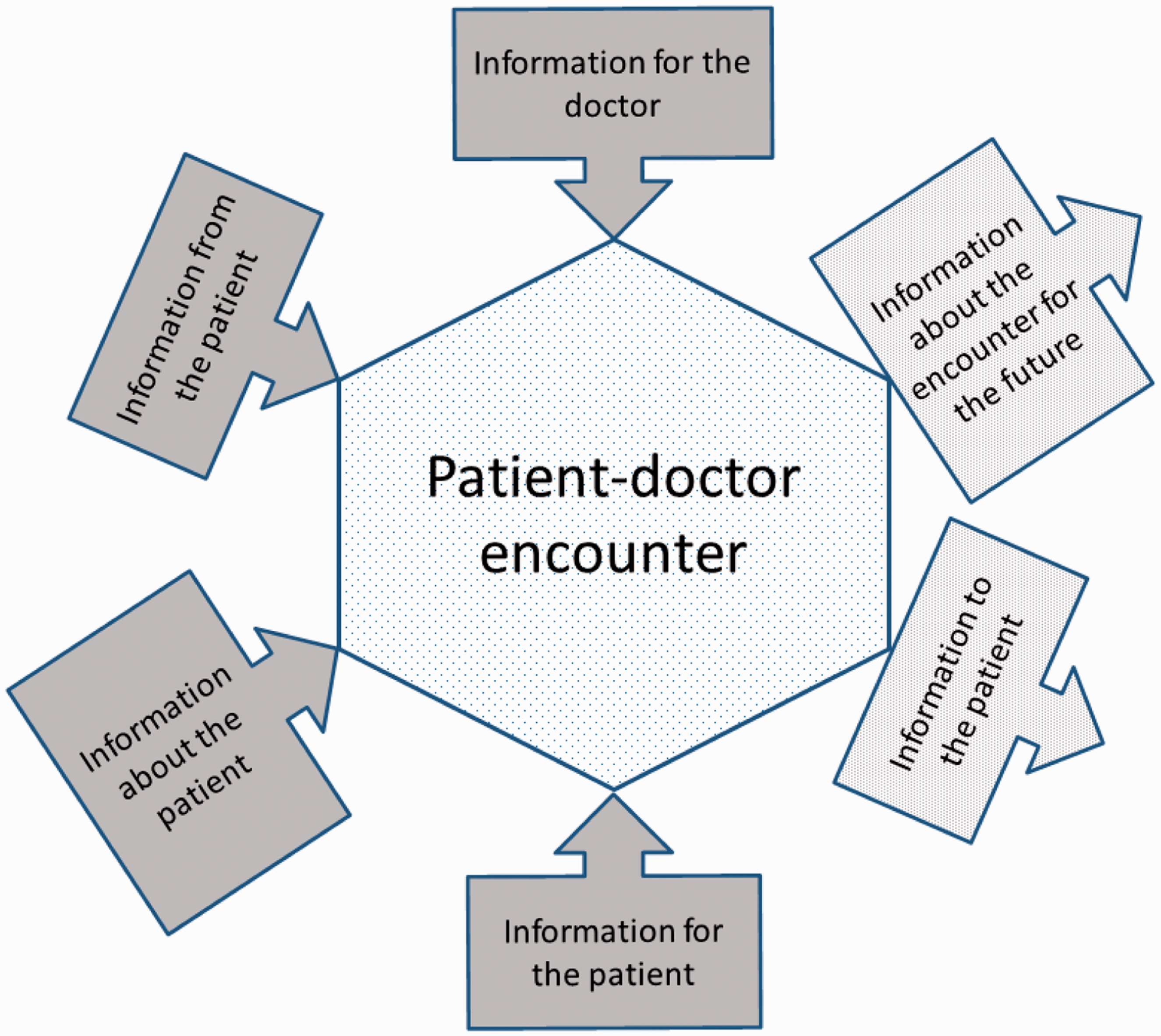
Information about the patient
The doctor has this information before the encounter starts. It may be in the patient’s clinical record, referral letters, letters from professionals to whom the patient has been referred, or in the doctor’s memory. Classically, this information is accessed before seeing the patient but alternative strategies have been proposed such as waiting until the patient has described why she has attended then reviewing her record. 5
Information from the patient
This is the information the patient brings to the encounter. It usually encapsulates the reason for attendance. However, patients sometimes bring other information with them: in the past, these were often newspaper or magazine cuttings; it now includes printouts from, or links to, websites of varying quality.
Information for the doctor
Information the doctor uses to assist decision-making. Historically, this has been printed material available in the office: drug formularies, clinical guidelines or protocols and textbooks. This is now delivered electronically through local intranets or the global internet and is disparate in quality and content. When just a few printed sources, the doctor could be familiar with the content and have some confidence in the quality. Now she is unfamiliar with much of what is available and is uncertain of its quality. This requires that the doctor has the skills to rapidly evaluate this information within the encounter.
Information for the patient
Historically, information available for the patient in the encounter was usually limited to a restricted range of printed patient information leaflets with which the doctor was familiar and had pre-appraised. The doctor’s decision-making was restricted to what and how much information to give the patient and to what end. 6 Now that the doctor can source patient information from the internet, this challenge is compounded by the need to evaluate the information found because the doctor retains responsibility for the quality of information given to a patient.6,7
Information to the patient
The four outputs of the doctor–patient encounter are management of the presented problem, modification of health-seeking behaviour, management of continuing problems and health promotion. 8 Each task is critically dependent on patient engagement with healthcare. While many patients actively engage with their healthcare, many don’t. 9 Information is key 9 and can be used to support biomedical compliance or an exchange of understanding thus achieving concordance. 6 We adopt no particular stance in this debate but invoke it to illustrate the complexity of information use.
Information for the future
Illustration of the six information streams in a doctor–patient encounter.
Is integrated information management part of the clinical skill set?
Clinical skills are critical to good clinical care and outcomes. While this is dependent on the traditional clinical skills described above, on their own they are insufficient without integrating the various information flows within the consultation. To ignore what is already known about the patient is self-evidently foolhardy. UK doctors are charged to ‘make good use of the resources’, which include information, to ‘keep clear, accurate and legible records’, to ‘encourage patients … to take an interest in their health and to take action to improve and maintain it’. 7 The ‘informed patient’ rhetoric is complex and contested6,9 but ultimately few doctors would advocate withholding information from our patients. Furthermore, doctors’ frequency of information needs are between ‘four times a half day’ and ‘five times per patient’ and are likely to affect the care of 40% of patients from whose care the information needs arose. 10 Sackett et al. 11 described evidence-based medicine as ‘the integration of best (current) research evidence with clinical expertise and patient values’, a definition which imbeds evidence-based medicine and its attendant information management skills in the doctor–patient encounter. Therefore, provision of good clinical care requires doctors to manage information while consulting with their patient: information management is self-evidently a clinical skill.
Isn’t promoting integrated information management as a clinical skill glorifying the trivial?
Integrated information management in a consultation is difficult for a number of reasons:
Patient record volume
Patient care and patient records are becoming increasingly complex and multiprofessional as medical knowledge advances. While the electronic patient record facilitates the ‘multiuser record’, it is harder for the practitioner to identify her last entry and all other entries relevant to today’s attendance.
Information paradox
Doctors are ‘overwhelmed with information but unable to find the knowledge they need when they need it’, 12 largely because of the growth in medical literature. Nevertheless, tools exist to support doctor access to quality-assured biomedical information, for example the McMaster Health Knowledge Refinery (http://hiru.mcmaster.ca/hiru/HIRU_McMaster_HKR.aspx). However, there are no equivalent tools to sift information resources for patients. This highlights the third problem.
Information quality
Not all information sources are equally trustworthy. While the issues are complex, reflecting differing perspectives of the functions of patient leaflets, 6 they are not trivial and need consideration.
Information purpose
Information is not neutral but is deployed strategically by healthcare systems, the medical profession, 6 interest groups and industry to achieve desired outcomes, manage demand or enhance uptake of goods and services. Nevertheless, there is increasing evidence of how information can be presented in ways which enable genuine patient choices. 13
We already know how to do it?
At the individual doctor level, this is patently not the case. Doctors still make choices contrary to best evidence, advice and practice. 14 Routine clinical practice generates many questions, yet most are never answered and, when they are, the sources consulted and information gained are often poor or outdated. 15 Knowledge of available information sources is patchy, skills required to efficiently use information found within the doctor–patient encounter are weak, teaching of these skills is still in its infancy and, until recently, the technology available inadequate. We need to nurture these skills for doctors of all ages and experiences and a good place to start is with medical students.
How can we support development of integrated information management skills?
Curriculum
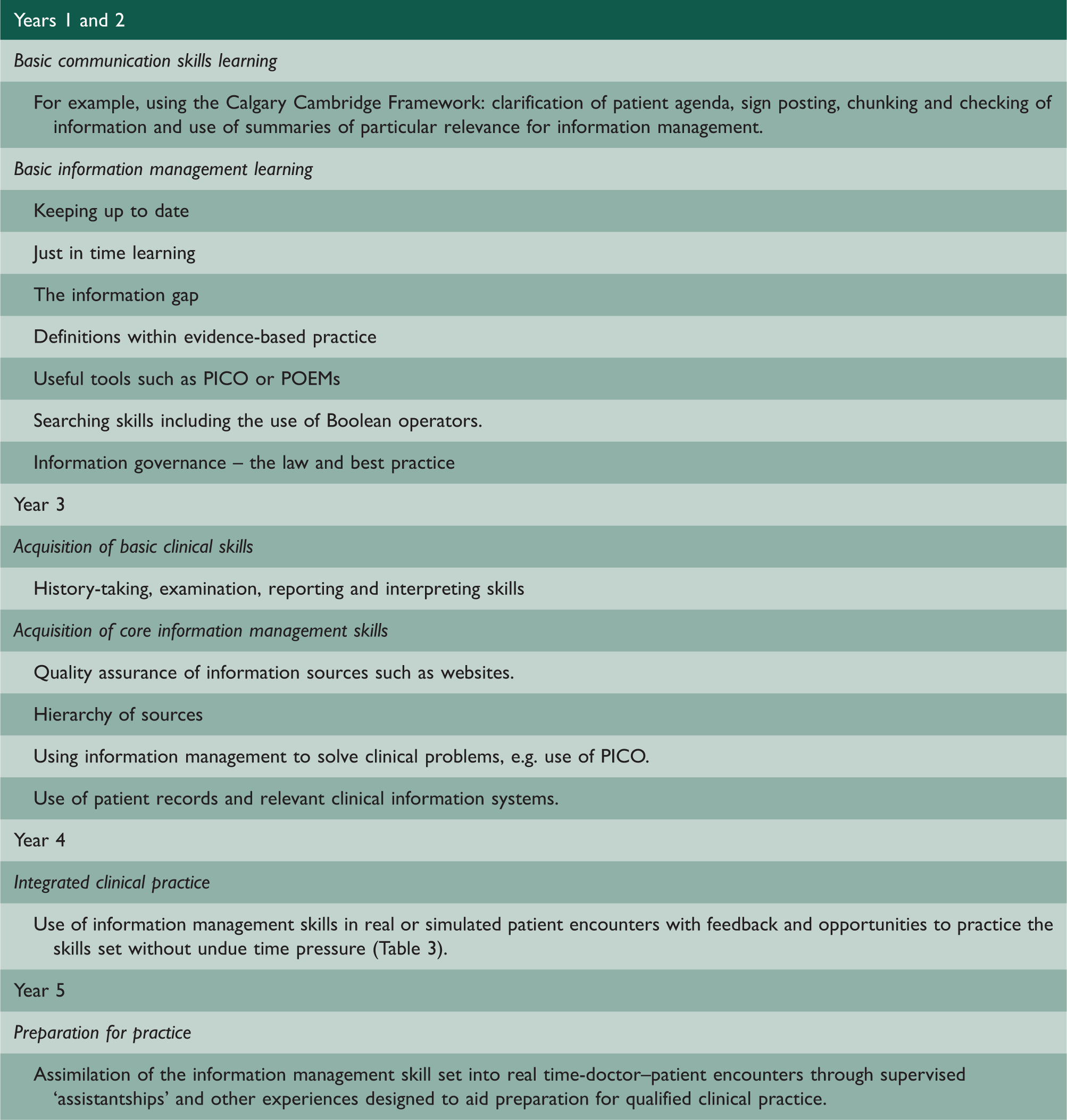
Curriculum architecture is beyond the scope of this paper but some suggestions are included in Table 2 and the following issues are relevant:
Components: Identify and develop key attitudes and skills first. These might include generation of awareness of need, opportunity, value and consequence among learners, critical appraisal of evidence skills, use of information sources and concepts such as ‘patient-oriented evidence that matters’ (POEMs).
16
Much of this is already part of many curricula. Integration into real-time patient encounters: Having developed key attitudes and skills, the learner then integrates them and rehearses them in real time alongside conventional skills (Table 3). Suggestions for an information management educational programme. POEM: patient-oriented evidence that matter. Integration of the information management skill set into the simulated or real doctor–patient encounter.
Culture change
Much of the required IT infrastructure is in place: virtually all UK family practitioners have used sophisticated electronic patient records since 2004. High-speed internet access has been commonplace for over 10 years. Adoption of electronic patient records has been slower in hospitals and only recently has medical student access been raised and addressed. 17 What is now needed is a cultural change so that IT policies, strategies and training better enable practitioners to implement evidence-based practice. 18
Assessment
Many medical schools assess components of an information management skills curriculum, but they are assessed individually. Critical appraisal of publications, for example, has been a core activity for many years. Clinical reasoning skills are now also attracting assessment. 18 Why should integrated information management be any different?
Discussion
We have argued that integrated information management is essential to modern doctor–patient encounters and good patient care. Effective integration of information management during the doctor–patient encounter is demanding and the demands are increasing. We assert that it is not currently conceptualised or taught as a clinical skill set and propose an approach to doing so.
Although we believe we are the first to assemble this argument, we are building on the ideas of others. Sackett et al.’s conceptualisation of evidence-based medicine is an important precursor, although information systems then available could not fully support evidence-based practice. Information systems have now matured to the point where Sackett’s vision can be realised in real-time. Clinical information systems and electronic patient records are now starting to deliver better care but are not uniformly safe and reliable in the work place. 19 Although further refinement of clinical information systems is needed, further development of doctors’ information management skills and their teaching is also required. We build on Slawson and Shaughnessy’s innovation of the POEM 16 by setting information for the doctor in the broader context of all information streams in the encounter.
We also contend that undergraduate medical education and postgraduate training must evolve from a ‘knowledge economy’, in which the doctor’s role is rooted in privileged professional knowledge, to a ‘cognitive skills economy’. With the increasing democratisation of information, powerful search engines which enable anyone with some IT skill to find information pertinent to their needs, and the internet as the delivery mechanism, the doctor’s role as an information source will be increasingly challenged. However, the doctors’ role in helping patients to make judgements about complex, contradictory and contextually dependent information will continue. This role is rooted in cognitive skills, one of which will be integrated information management. Integrated information management skills will accentuate the clinician’s capability and enhance patient experience.
This presents a radical change for medical education from curriculum, instructional and assessment design to IT infrastructure available in medical schools and the clinical environment and the culture of using IT. It will have enormous impacts on doctor–patient relationships, doctor–patient encounters and healthcare. Patients will move from being passive consumers of information to active explorers of the information mountain. Integration of information management skills into doctor–patient encounters will improve the encounter, its efficacy, patient safety, and patient and doctor satisfaction, as well as drive continuing lifetime professional development of doctors through learning tailored to practice context and patient needs.
If the centrality of integrated information management skills is accepted, our profession will need to ensure that they are represented in curricula and learners will need support to acquire them. This is not a trivial change for medical education and training, but it will be necessary to ensure that healthcare practitioners can respond to the potential of the ever-growing medical information mountain.