
Abstract
Long-term use of statin therapy is essential to obtain clinical benefits, but adherence is often suboptimal and some patients are also reported to fail because of ‘statin resistance'. The identification of PCSK9 as a key factor in the LDL clearance pathway has led to the development of new monoclonal antibodies. Here we critically review the economic evaluations published in Europe and focused on statins. We searched the PubMed database to select the studies published from July 2006 to June 2016 and finally selected 19 articles. Overall, the majority of studies were conducted from a third-party payer's viewpoint and recurred to modelling. Most studies were sponsored by industry and funding seemed to play a pivotal role in the study design. Patients resistant to LDL-C level reduction were considered only in a few studies. The place in therapy of the new class of biologic should be considered a kind of ‘third line' for cholesterol-lowering, after patients have failed with restricted dietary regimens and then with current drug therapies. Otherwise they could result in hardly sustainable expenses even for developed countries.
Introduction
Cardiovascular disease is the main cause of death in Europe and worldwide.1,2 The relationship between low-density lipoprotein cholesterol levels and cardiovascular disease is well recognised and understood.3,4 In view of the key role of low-density lipoprotein cholesterol in the atherosclerotic process, cholesterol-lowering therapy represents one of the established tools for reducing cardiovascular risk in both primary and secondary prevention. 5
The current cholesterol-lowering drugs include statins, bile acid sequestrants and selective cholesterol absorption inhibitors. 6 Since their introduction, statins have become a cornerstone for cardiovascular disease prevention, with demonstrated efficacy in reducing cardiovascular morbidity and mortality in both primary and secondary prevention, particularly in high-risk patients.7–9
Long-term use is essential to obtain clinical benefits but adherence to statin therapy is often suboptimal, for various reasons (e.g. patient’s age, sex and polypharmacy) besides adverse effects,10,11 which can all contribute to failure in low-density lipoprotein cholesterol levels. 12 Yet, some patients are reported to fail in achieving low-density lipoprotein cholesterol targets because of ‘statin resistance’, 13 a condition associated with both genetic and environmental factors (such as gene polymorphisms and smoking) as well as pathological states (e.g. inflammation, hypertension and HIV infection).
The identification of proprotein convertase subtilisin/kexin type 9 (PCSK9), 14 a key factor in the LDL clearance pathway, and the finding that individuals with loss-of-function mutations in PCSK9 have low plasma levels of low-density lipoprotein cholesterol 15 and are protected from coronary heart disease 16 have led to the development of new therapeutic options aimed at PCSK9 inhibition. Evolocumab and alirocumab (both monoclonal antibodies against PCSK9)17,18 have now been approved for patients with mixed dyslipidaemia, heterozygous (familial and non-familial) and homozygous familial hypercholesterolaemia. Both biologics should be prescribed: (i) in combination with a statin only or a statin with other lipid-lowering therapies in patients unable to reach low-density lipoprotein cholesterol goals with the maximum tolerated dose of a statin; and (ii) alone or in combination with other lipid-lowering therapies in patients who are statin-intolerant (or for whom a statin is contraindicated). A third antibody (bococizumab) is currently in phase III trials for similar indications, 19 with likely to gain market approval in late 2016. All antibodies are injected subcutaneously once/twice per month.
Here, we critically review the full economic evaluations published in Europe and focused on statins and assess whether and how these studies included in their analyses the patients resistant to low-density lipoprotein cholesterol level reduction despite statin treatment, who are ideally the main therapeutic target for the new anticholesterol monoclonal antibodies. Finally, we discuss the potential future scenarios for the ‘market’ of these new drugs from a third-party payer’s perspective.
Methods
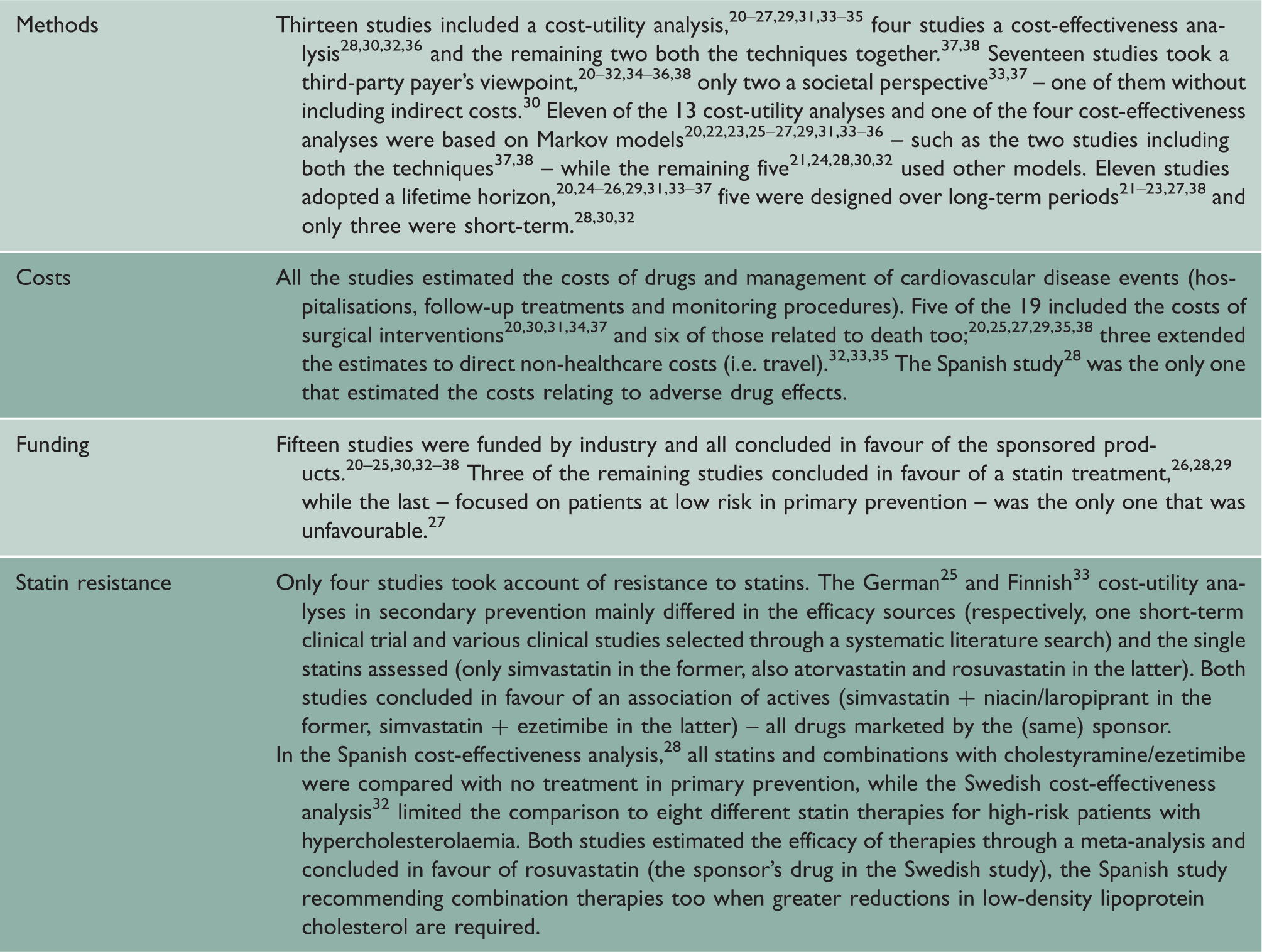
Main characteristics of the selected studies.

Main results of the review on statins.
Results
The studies came from 11 European Union countries, more than half of them from Sweden (4) and the UK (6). Six studies focused on primary prevention,21–24,27,28 five on secondary,20,25,33,34,37 one on both 35 and the remaining seven on other therapeutic targets – three on subjects with hypercholesterolaemia31,32,36 and four on patients affected by severe cardiovascular diseases.26,29,30,38 Fifteen studies analysed therapies with statins alone,20–27,30–32,34–38 four in combination with other active agents.25,28,29,33 Only six of the 19 studies took account of statin therapy adherence,20,24,26,27,30,38 five of the remaining 13 assumed that all patients were fully compliant,25,29,32–34 while three did not mention adherence as an issue.21,28,36
Only four studies selected took into account the question of resistance to statins in their analyses.25,28,32,33 One study focused on primary prevention, 28 two on secondary25,33 and the remainder on high-risk patients for hypercholesterolaemia. 32 The two studies in secondary prevention,25,33 based on lifetime Markov models, focused only on patients who failed to meet their low-density lipoprotein cholesterol target level with statin alone and analysed the additional benefit of combination therapies; the two others conducted a subgroup analysis over a one-year period in patients who did not achieve the low-density lipoprotein cholesterol therapeutic target.28,32
Overall, the majority of European full economic evaluations on statins were conducted from a third-party payer’s viewpoint on therapeutic targets of demonstrated efficacy for these drugs, using modelling to estimate the cost-effectiveness of single statins, mostly over a long-term time horizon. Many studies included costs related to death, and some even direct non-healthcare costs in their estimates, but adherence to statin therapies was hardly considered, even though long-term therapy is essential to obtain clinical benefits. The majority of studies were sponsored by industry and funding seemed to play a pivotal role in the study design, with results aimed at supporting the cost-effectiveness of the sponsored drug, as is often the case in pharmaco-economic literature. 39
Patients resistant to low-density lipoprotein cholesterol level reduction, i.e. the major therapeutic target of the new anticholesterol biologics, were considered only in a few studies. Yet, they were all conducted after the patent expiry of the first statins launched, and most analyses were extended to associations with other (in-patent) actives as alternatives, concluding in favour of either high-intensity statins or combination therapies.
With this background, we tend to conclude that statin resistance was not considered a relevant ‘unmet need’ in the European economic evaluations conducted before the launch of the new human antibodies.
Policy implications
At this stage, we wonder whether and how the forthcoming launch of this new class of biologics will affect the present market situation in the near future. In principle, these drugs should be prescribed for very specific patient targets, which represent ‘market niches’. Although these new products are expected to be very costly (as is typical for new human antibodies), the whole ‘budget impact’ of this therapeutic class on pharmaceutical expenditure should be limited, as for any rare disease, even though they might be prescribed as add-on therapy, with consequent extra cost for third-party payers. Moreover, the subcutaneous injection of human antibodies can hardly be considered an advantage for patients’ quality of life compared to a daily statin pill, although their marketers may well claim that the (bi)monthly schedules should facilitate patient adherence to cholesterol lowering therapy.
Following a rational strategy, the place in therapy of these new products could be considered a kind of ‘third line’ for cholesterol-lowering, after patients have failed with restricted dietary regimens first and then with current drug therapies (starting from statins) second.
However, experience in various other pathologies can lead us to predict very different scenarios, in which the role of the new antibodies may grow substantially depending on the marketing support that companies provide to promote them – as is typical in the (non) pharmaceutical market, where supply can often induce demand. 40 This is even more likely when the new products challenge off-patent drugs at the end of their ‘life cycle’, as happens in this competitive arena. A substantial ‘switch’ of prescribing patterns might lead to a massive budget impact for third-party payers, in line with the growth of the symptom in developed countries 41 and the increasing restrictions recommended in clinical guidelines. 6
According to a rough estimate based on the first official prices issued in the UK, a year’s treatment with the new human antibodies would cost around £4000 – at least 100 times more than that with a generic statin and 10 times the most expensive branded statin. 42 This would result in hardly sustainable expenses even for developed countries in case of substantial prescriptions of the new products.
In conclusion, to militate this sort of disruptive scenario for European third-party payers, we would warmly recommend the adoption of a ‘price-volume’-like contract43,44 for these products from the very beginning, in which drastic price reduction should be envisaged in case of prescriptions exceeding the appropriate therapeutic targets estimated ex ante.
Subsequently, systematic control of prescription patterns will be the only means of enhancing rational consumption in clinical practice, although its effectiveness is expected to vary a lot in different countries, depending on the type and management of healthcare systems, and on medical deontology too.
Footnotes
Declarations
Acknowledgements
None