Abstract
Objective
To quantify the risk of suicidality and violence when selective serotonin and serotonin-norepinephrine reuptake inhibitors are given to adult healthy volunteers with no signs of a mental disorder.
Design
Systematic review and meta-analysis.
Main outcome measure
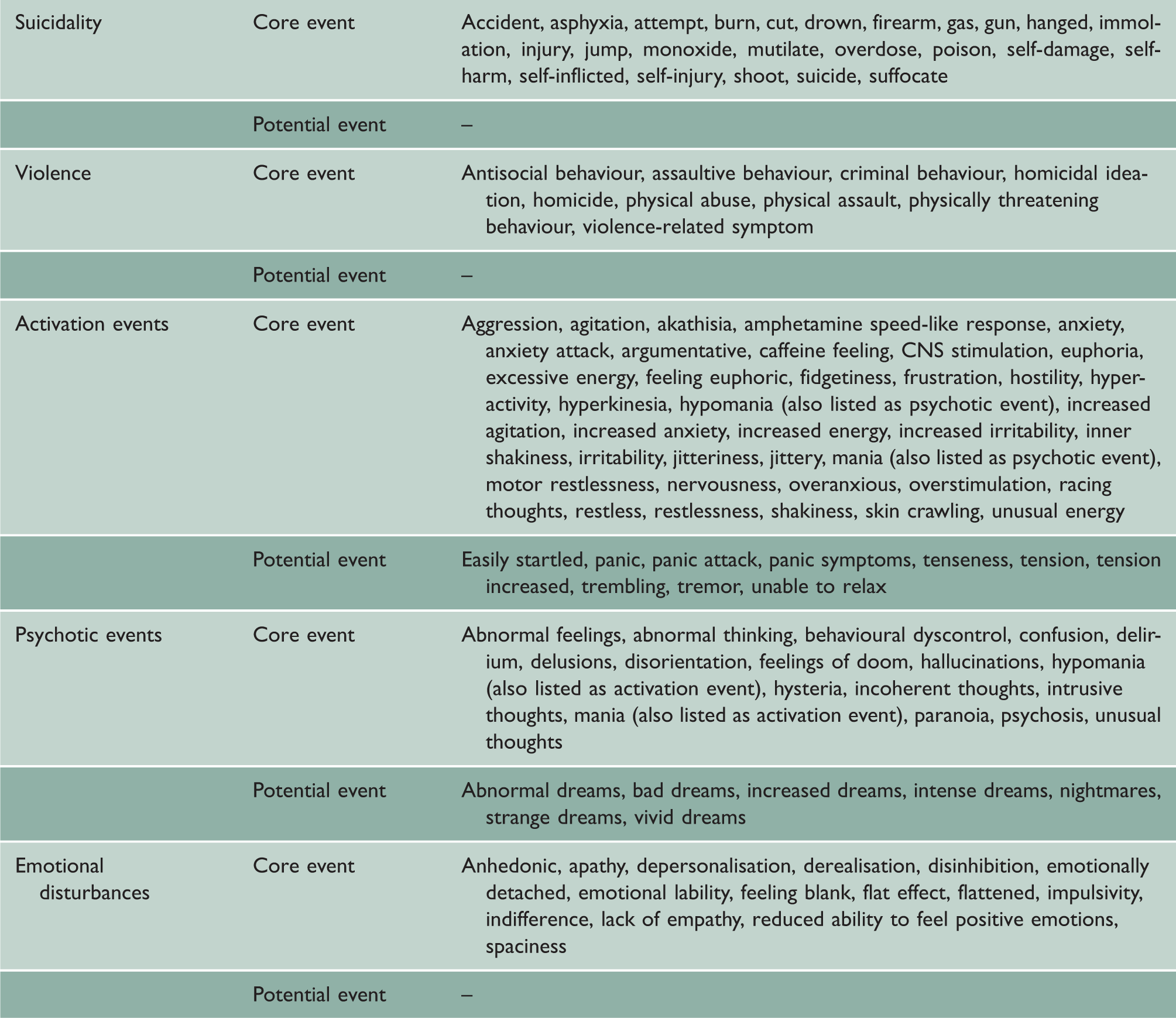
Harms related to suicidality, hostility, activation events, psychotic events and mood disturbances.
Setting
Published trials identified by searching PubMed and Embase and clinical study reports obtained from the European and UK drug regulators.
Participants
Double-blind, placebo-controlled trials in adult healthy volunteers that reported on suicidality or violence or precursor events to suicidality or violence.
Results
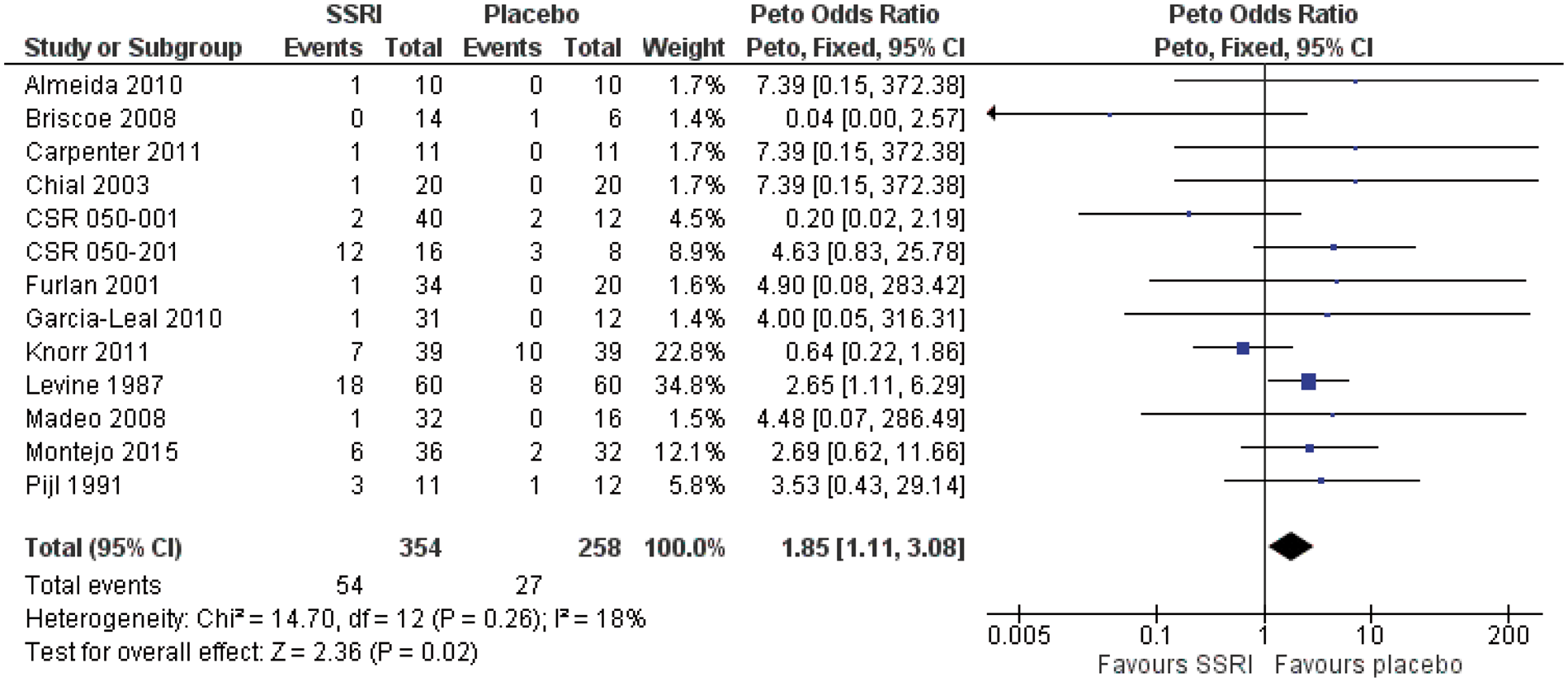
A total of 5787 publications were screened and 130 trials fulfilled our inclusion criteria. The trials were generally uninformative; 97 trials did not report the randomisation method, 75 trials did not report any discontinuations and 63 trials did not report any adverse events or lack thereof. Eleven of the 130 published trials and two of 29 clinical study reports we received from the regulatory agencies presented data for our meta-analysis. Treatment of adult healthy volunteers with antidepressants doubled their risk of harms related to suicidality and violence, odds ratio 1.85 (95% confidence interval 1.11 to 3.08, p = 0.02, I2 = 18%). The number needed to treat to harm one healthy person was 16 (95% confidence interval 8 to 100; Mantel-Haenszel risk difference 0.06). There can be little doubt that we underestimated the harms of antidepressants, as we only had access to the published articles for 11 of our 13 trials.
Conclusions
Antidepressants double the occurrence of events in adult healthy volunteers that can lead to suicide and violence.
Introduction
The reporting of harms in drug trials is generally poor, with inadequate explanation of how they were collected, and often harms are missing altogether.1,2 From 2011 to 2012, the Nordic Cochrane Centre received unredacted clinical study reports on antidepressants filed for regulatory approval at the European Medicines Agency and the UK Medicines and Healthcare products Regulatory Agency. We demonstrated selective reporting of major harms in the published articles of duloxetine and inconsistencies between the protocols and the clinical study reports. 3 Furthermore, we noticed that the adverse events tables in clinical study reports had hidden suicidal events due to the medical dictionaries and coding conventions used. 4 Based on the 70 clinical study reports we received, we found that antidepressants more than doubled the risk of suicidal and aggressive behaviour in children and adolescents. 5
A 2012 systematic review of 33 trials in healthy volunteers documented various effects of selective serotonin reuptake inhibitors but only mentioned the adverse events in a few words. 6 The review was based on published articles and none of these lived fully up to the CONSORT guideline for good reporting.
Since their introduction in the late 1980s, the benefits and harms of selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors have been the subject of huge debate. Because their harms – in particular suicidality – have often been explained away as if they were disease symptoms or only a problem in children,7–10 we wished to quantify the risk of suicidality and violence when these drugs are given to adult healthy volunteers.
Methods
According to our prespecified protocol (available from the authors), we included double-blind, randomised placebo-controlled trials of selective serotonin reuptake inhibitors or serotonin-norepinephrine reuptake inhibitors (called antidepressants throughout this paper) in adult healthy volunteers with no signs of a mental disorder. There were no language restrictions. We excluded trials in abusers of tobacco, drugs or alcohol and also imaging studies, as these have another objective and furthermore are of poor methodological quality. 11
Search strings for PubMed and Embase.
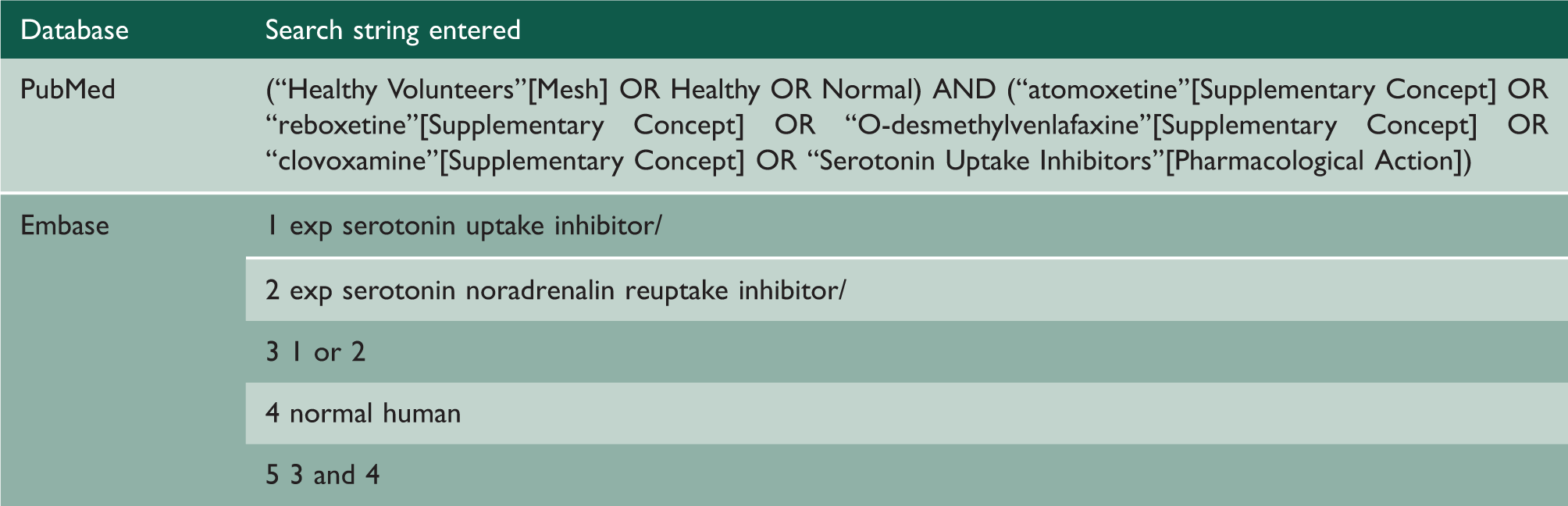
We also included relevant clinical study reports on antidepressant drugs we received from regulatory agencies for our projects in this area.3–5 We checked whether the clinical study reports had been published by searching for investigator names and drugs on PubMed and Embase.
Types of harms looked for when reading the reports.
Uncertainties during data extraction were resolved by discussion between the authors. If the reporting of harms was unclear, we contacted the authors of the trials for clarification. We assessed the risk of bias in the trials focusing on randomisation and blinding.
We performed a meta-analysis calculating Peto’s odds ratio for dichotomous outcomes with Review Manager. Because of the considerable risk of carryover effects in crossover trials, we only used trials that reported on periods separately.19,20
Results
We identified 5787 publications in PubMed and Embase, removed 569 duplicate entries, and screened the titles and abstracts of the remaining 5218 records, which left 316 articles for full-text reading (Figure 1).
PRISMA flow diagram of included studies based on the literature searches.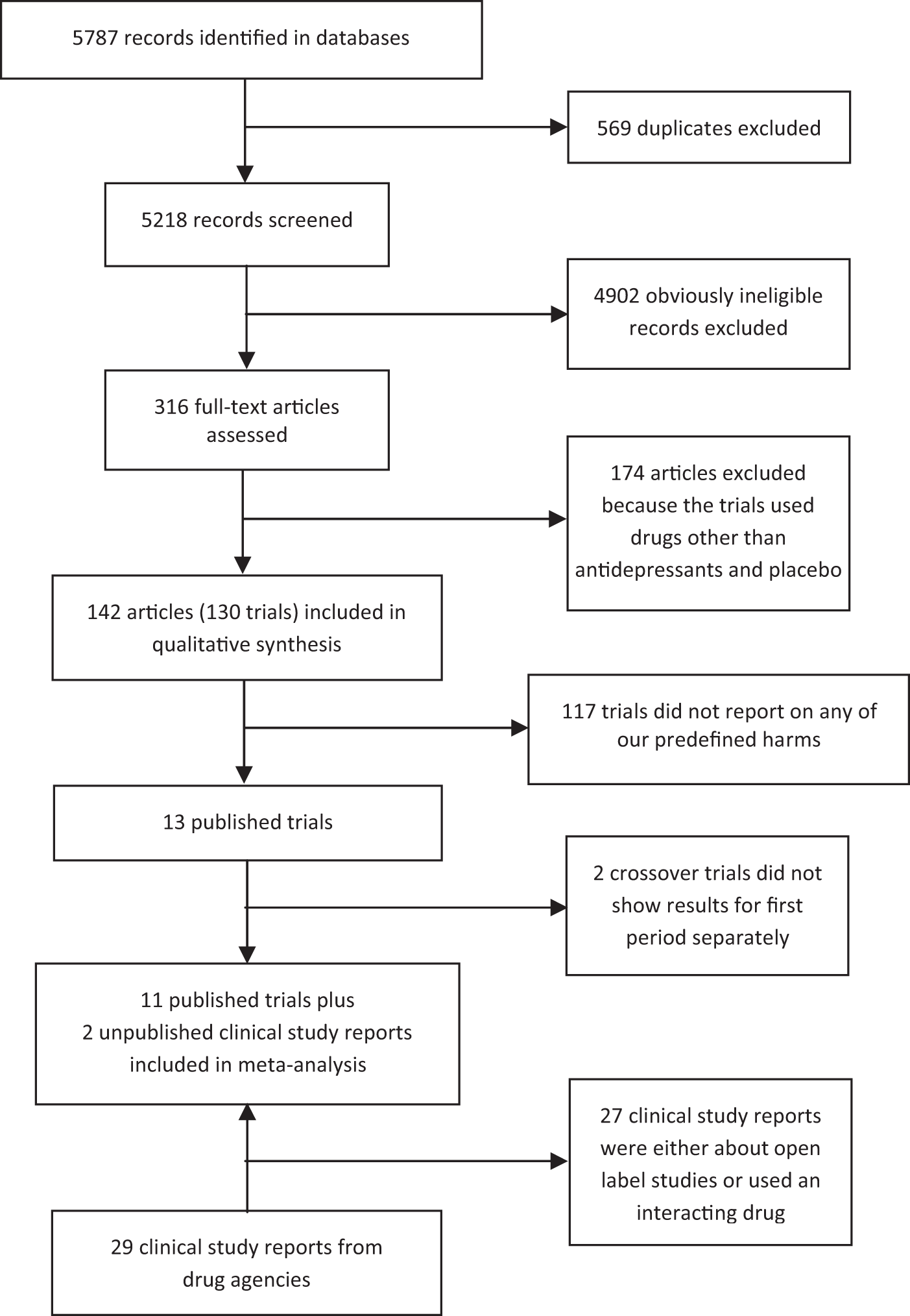
We excluded 174 of these articles because the studies were crossover trials using antidepressant inhibitor, a placebo and a third drug, or because the studies were parallel trials that used a drug other than an antidepressant as an interaction drug. This left 142 articles on a total of 130 trials that fulfilled our inclusion criteria, 52 of which were two-period crossover trials. Ten different antidepressants were tested in the trials; citalopram (n = 33) and paroxetine (n = 27) were most commonly used.
The trials did not report much about their methodology. All 130 trials were allegedly randomised, but 97 (75%) did not describe the method and 75 (58%) did not report any discontinuations or lack thereof.
Reporting of adverse events was generally inadequate; 63 trials (48%) did not report any adverse events or stated that there were none; 43 trials (33%) reported at least one adverse event; while 24 trials (18%) reported only the most frequently occurring adverse events or those leading to discontinuation. The source of funding was industry in 29 trials (22%), non-industrial sources in 47 trials (36%), mixed in 17 trials (13%) and not reported in 37 trials (28%).
Thirteen of the 130 trials reported on at least one of our predefined harms, 10 of which were parallel group trials and three crossover trials. We could not include two of the crossover trials, as there were no data for each period separately. We included the first period of the third crossover trial, which ended prematurely due to carryover effects despite a four-week washout period.A1
We received 29 clinical study reports from the regulatory agencies, two of which fulfilled our inclusion criteria for the meta-analysis. None of them had been published. Most of the remaining clinical study reports described non-blinded bioavailability studies or drug interaction studies.
Harms in the meta-analysed trials. Some trials included arms with drugs that were not antidepressants; these data are not shown.

CSR: clinical study report.
Risk of bias in the included trials
Adequate methods for sequence generation and concealment of treatment allocation were described for six trialsA3–A6,A8,A11 and for concealment of allocation for two trials.A7,A12 The methods were not specified in five trials.A1,A2,A9,A10,A13 Adequate blinding methods were mentioned for seven trialsA5–A8,A10–A12 and not specified in six trials.A1–A4,A9,A13 We did not look at attrition because the subject of our research was side effects, not beneficial effects.
Meta-analysis
Treatment of adult healthy volunteers with antidepressants doubled their risk of harms related to suicidality and violence, odds ratio 1.85 (95% confidence interval 1.11 to 3.08, p = 0.02, I2 = 18%) (Figure 2). The number needed to treat to harm one healthy person was 16 (95% confidence interval 8 to 100; Mantel-Haenszel risk difference 0.06). Two clinical study reports and one published trial reported the severity of the harms.
Discussion
The century-old belief that patients with depression are at heightened risk of suicide as they begin to recover and their energy and motivation return 21 is being propagated everywhere, e.g. in the 2003 practice guideline from the American Psychiatric Association, which states that ‘clinical observations suggest that there may be an early increase in suicide risk as depressive symptoms begin to lift but before they are fully resolved’. 22
Because of this deeply ingrained idea, many psychiatrists believe that when patients become suicidal on an antidepressant drug, it is not an adverse effect of the drug but a positive sign that the drug starts working.7,10 However, a systematic review from 2009 showed that the research that has been carried out contradicts this belief, 21 and our review also suggests that it is wrong. We found that antidepressants double the risk of suicidality and violence, and it is particularly interesting that the volunteers in the studies we reviewed were healthy adults with no signs of a mental disorder. Our results agree closely with a review of paroxetine trials in both adults and children with mental disorders using regulatory data released after a court case. It included events both during treatment and in the subsequent withdrawal phase and found a doubling in hostility events (odds ratio 2.10, 95% confidence interval 1.27 to 3.48). 23
While it is now generally accepted that antidepressants increase the risk of suicide and violence in children and adolescents5,12 (although many psychiatrists still deny this 10 ), most people believe that these drugs are not dangerous for adults. This is a potentially lethal misconception.7,10,15,24
As far as we know, our review is the first of the risk of suicide and violence in healthy volunteers. It was inspired by David Healy’s work. 7 In 2000, Healy published a study he had carried out with 20 healthy volunteers – all with no history of depression or other mental illness – and to his big surprise, two of them became suicidal when they received sertraline. 25 One was on her way out the door to kill herself in front of a train or a car when a phone call saved her. Both volunteers remained disturbed several months later and seriously questioned the stability of their personalities.
In one of the two crossover trials we excluded because we did not have data on the first period separately, a healthy volunteer committed suicide, which was mentioned in both published articles.A14,A15 She had received duloxetine in increasing doses for 16 days, tapered off the maximum dose of 400 mg daily very quickly (in just four days according to the design of the study) and killed herself four days later while on placebo. The authors, several of whom were employees of Eli Lilly or owned stock in the company, judged her suicide ‘to be unrelated to study drug treatment’,A15 although it is well known that the suicide risk is high when an antidepressant is stopped abruptly.10,23 There was no more information about the suicide in the articles, and it was not included in the listing of adverse events we acquired from Eli Lilly, which only mentioned a woman who reported suicidal ideation twice while on placebo. As we do not know if this was the same patient, we asked Eli Lilly for access to anonymised data for the volunteer who committed suicide and the detailed person narrative, as we also wanted to know how it could be possible to state that the suicide was not related to duloxetine, but the company refused to give us the data.
In another of Eli Lilly’s studies, a healthy 19-year-old student who had taken duloxetine in order to help pay her college tuition hanged herself in a laboratory run by Lilly. 26 It turned out that missing in the FDA’s files was any record of the college student and at least four other volunteers known to have committed suicide, and Lilly admitted that it had never made public at least two of those deaths. 26
In the other crossover trial we had to exclude, an unknown number of volunteers discontinued paroxetine due to restlessness, tremor and other adverse events.A16 We contacted the corresponding author of the study who referred us to the first author, but despite several attempts of making contact via two different email addresses and phone (to the doctor’s assistant), this author never responded.
Exploratory analyses of the clinical study reports
Although only two of the 29 clinical study reports were eligible for our meta-analysis, e.g. as the studies needed to be double-blind, two researchers (AØB and PBD) read them all (2224 pages) and extracted data independently, as we wanted to explore possible selective reporting of harms in the published articles. Nineteen clinical study reports reported on the harms we investigated and nine of these were published, but less than half of the harms were reported in the articles (21 of 50 events on antidepressants and two of four events on placebo).
One of these studiesA17 was mentioned by David Healy 7 who had spoken with the study investigator, Ian Hindmarch. It was a crossover trial of the interaction between sertraline and diazepam that was terminated due to unexpected adverse events after only four days, before the first phase had been completed and before any of the volunteers had received diazepam. All five volunteers in the sertraline group became agitated and four of them anxious, while one of seven volunteers in the placebo group became aggressive, agitated and anxious. The study was never published.
Limitations
There can be little doubt that we underestimated the harms of antidepressants. For 11 of our 13 trials, we only had access to the published article, and it well documented that the drug companies underreport seriously the harms of antidepressants related to suicide and violence, either by simply omitting them from the reports, by calling them something else or by committing scientific misconduct.2–5,7,10,27 In trials of duloxetine and sertraline, for example, only 33 of 45 cases of suicidal ideation, attempt or injury listed in a trial register were also mentioned in the published reports. 2
Psychiatrists believe that the suicide risk with antidepressants is only increased till age 24, but this misconception builds on seriously flawed trial data that the FDA has published. 12 Several meta-analysts have pointed out just how unreliable the trials are.5,10,28,29 A 2005 meta-analysis conducted by independent researchers of the published trials included 87,650 patients of all ages and found twice as many suicide attempts on drug than on placebo (odds ratio 2.28, 95% CI 1.14 to 4.55). 28 They also found out that many suicide attempts must have been missing; some of the investigators responded that there were suicide attempts they had not reported in their trials, while others replied that they did not even look for them. Further, events occurring shortly after active treatment was stopped were not counted. Another 2005 meta-analysis conducted by independent researchers used UK drug regulator data and included 40,826 patients; they found a non-significant doubling in suicides or self-harm events when events occurring later than 24 hours after the randomised phase was over were included (relative risk 2.14, 95% confidence interval 0.96 to 4.75, our calculation). 29 These researchers also noted that the companies had underreported the suicide risk in their trials, and they found that non-fatal self-harm and suicidality were seriously underreported compared to the reported suicides.
Even the FDA’s 2006 meta-analysis of 100,000 patients in 372 placebo-controlled trials12,30 is seriously flawed. Based on trials that were included in FDA’s analysis, one of us has estimated that there are likely to have been 15 times more suicides on antidepressant drugs than reported by the FDA. 10 Two important reasons for the underreporting of suicides are that the FDA trusted the data the companies sent to them and that they only included events up to 24 hours after the randomised phase was over. 10
We did not plan for any sensitivity analyses related to whether the randomisation and blinding methods were adequately described, as we were very well aware before we started our review that in the sort of trials we would find, there would likely be very little or no information about this. We reviewed trials in healthy volunteers, which have a completely different purpose than standard treatment trials, and the drug companies do not have any particular incentive to provide details about how they blinded the drug and the placebo and how they randomised the volunteers in such trials. Furthermore, we studied harms, not clinical beneficial effects, as we included healthy people. It would therefore be inappropriate to assume that trials that did not describe blinding and randomisation methods are less reliable than other trials.
Conclusions
Antidepressants double the occurrence of events in adult healthy volunteers that can lead to suicide and violence. We consider it likely that antidepressants increase suicides at all ages.
Meta-analysis of suicidal or violent events or precursors to such events.