
Abstract
The Declaration of Helsinki, adopted by the World Medical Association’s General Assembly in 1964, is the most important set of guidelines about research on human participants. It both reflects and shapes the ethos of international research ethics. It is a living instrument and is reviewed and revised regularly. Its latest revision was in 2013. There are four substantial changes, reflected in the new Paragraph 15 (which deals with compensation for trial related injuries), Paragraph 33 (relating to placebos), Paragraph 20 (relating to vulnerable groups) and the new Paragraph 34 (relating to post-trial provisions). This article analyses these changes, and asks whether they indicate any shift in the overall philosophy of the Declaration. We conclude that these changes, though significant, are not tectonic. They accord with the spirit that has motivated the Declaration through all its iterations, and indicate a steady, incremental evolution towards a holistic code of research ethics for research on human participants. Patient autonomy, though crucial, is no longer the only concern of the Declaration; distributive justice and beneficence are motivating forces too. While the Declaration is aware of the need to facilitate research, it is equally aware of the need to protect the vulnerable, and of the practical difficulties involved in that protection.
The Declaration of Helsinki was adopted by the World Medical Association in 1964 at its 18th General Assembly. It is a set of ethical guidelines relating to research on human subjects and is widely regarded as authoritative. 1 It is reviewed and revised regularly. 2
The latest revision of the Declaration was in 2013. New paragraphs have been added and it has been rearranged, with the paragraphs organised into specific sections. There are four substantial changes, reflected in Paragraph 15 (which deals with compensation for trial-related injuries), Paragraph 33 (relating to placebos), Paragraph 20 (relating to vulnerable groups) and Paragraph 34 (relating to post-trial provisions). This article analyses these changes, and asks whether they indicate any shift in the overall philosophy of the Declaration.
The new Paragraph 15: Compensation for harm
Paragraph 15 reads:
‘Appropriate compensation and treatment for subjects who are harmed as a result of participating in research must be ensured’. 3
This is wholly new. It had, surprisingly, no counterpart in previous versions, though the 2008 version required that information regarding compensation be stated in the research protocol – implying that participants were (morally) entitled to compensation, but did nothing to ensure that they got it.
While earlier iterations focused on ensuring that the autonomy interests of participants were respected, this new clause is an acknowledgment that bodily integrity and financial interests are important too.
Paragraph 33: Use of placebos
The period between 1996 and 2000 saw a debate over the paragraphs concerning the use of inert placebos for patients in control groups. The debate became particularly heated in relation to short regimen Azidothymidine trials to prevent mother to child transmission of HIV/AIDS in sub-Saharan Africa. The issue was whether the control group should be given the ‘best proven’ or the ‘best available’ treatment, or where there was no available treatment, as is often the case in developing countries (due to financial constraints), whether the control group should be given the placebo.
Where for compelling and scientifically sound methodological reasons the use of any intervention less effective than the best proven one, the use of placebo, or no intervention is necessary to determine the efficacy or safety of an intervention and the patients who receive any intervention less effective than the best proven one, placebo or no intervention will not be subject to additional risks of serious or irreversible harm as a result of not receiving the best proven intervention. [3, para. 33, emphasis added]
Changes relating to the use of placebo in the Declaration of Helsinki (1989–2013).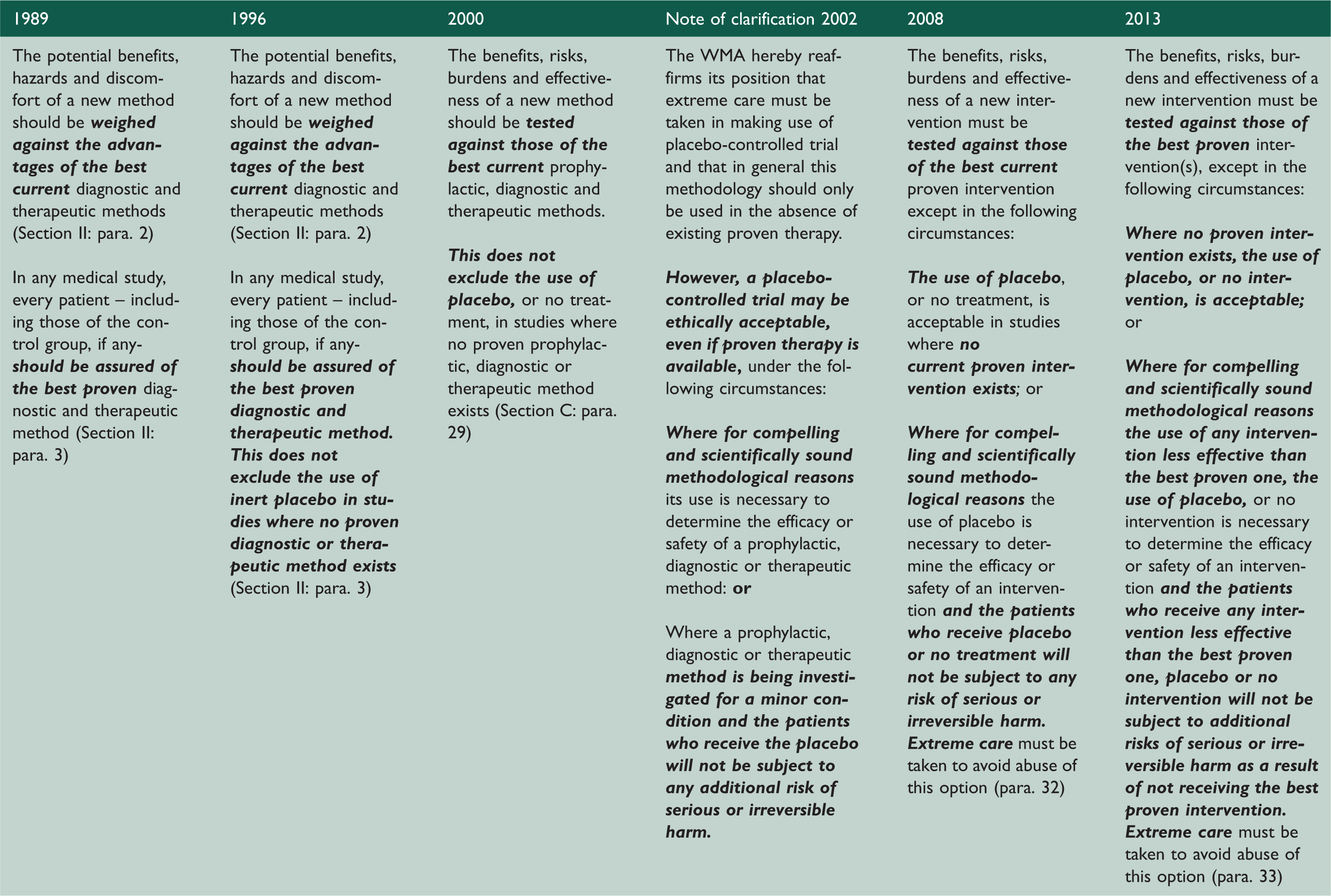
Was it right to add: ‘the use of any intervention less effective than the best proven one’? There are two main concerns: First: the vast majority of subjects in outsourced clinical trials (typically in developing countries) – will not have the best proven intervention available. Here, instead of encouraging efforts to make the best treatment options available, new but sub-optimal interventions may become the standard – so exacerbating disparities, within and between countries. Second: in locations where the best proven intervention may be available, giving the control group the less effective intervention is ethically dubious. Patients may be harmed by not having the best available treatment. In these circumstances, the research ethics committee is likely to refuse to approve the trial. If the trial did go ahead, patients suffering ‘additional’ harm may invoke their right to compensation under Paragraph 15 of the Declaration.
The trend is obvious enough: though there is much opposition by the proponents of placebo-controlled trials, 5 the Declaration is opposed to the use of placebos.
Paragraph 20 and 34: The general philosophy of justice and beneficence
Justice, applied to research, entails fair distribution of risks and benefits and equal access to the fruits of research. Beneficence means to do good, to make efforts to maximise possible benefits and minimise harms. It is said that the Declaration has moved from being a purely ethical document to one that is increasingly concerned with social justice. 5 This is a curious observation: social justice is an essential element of ethics.
Paragraph 20: Vulnerable groups and individuals
The exploitation of vulnerable populations, whether in the developing countries or developed countries, is a real danger in medical research.6–9 The problem is compounded by the fact that much research is conducted by commercial organisations motivated by profit.9,10 One way of reducing the chance of exploitation is to insist, as all versions of the Declaration have done, on informed consent. Although the Declaration allows for consultation with the family or community leaders in some contexts, thus respecting local cultural norms, 7 it emphasises that the decision to enroll must be made freely by the participant herself/himself [3, para.25].
Distributive justice is the basis for other anti-exploitation mechanisms. The 2013 version states, at Paragraph 20: Medical research with a vulnerable group is only justified if the research is responsive to the health needs or priorities of this group and the research cannot be carried out in a non-vulnerable group. In addition, this group should stand to benefit from the knowledge, practices or interventions that result from the research. [3, emphasis added]
Responsiveness and the Declaration of Helsinki 2000–2013.
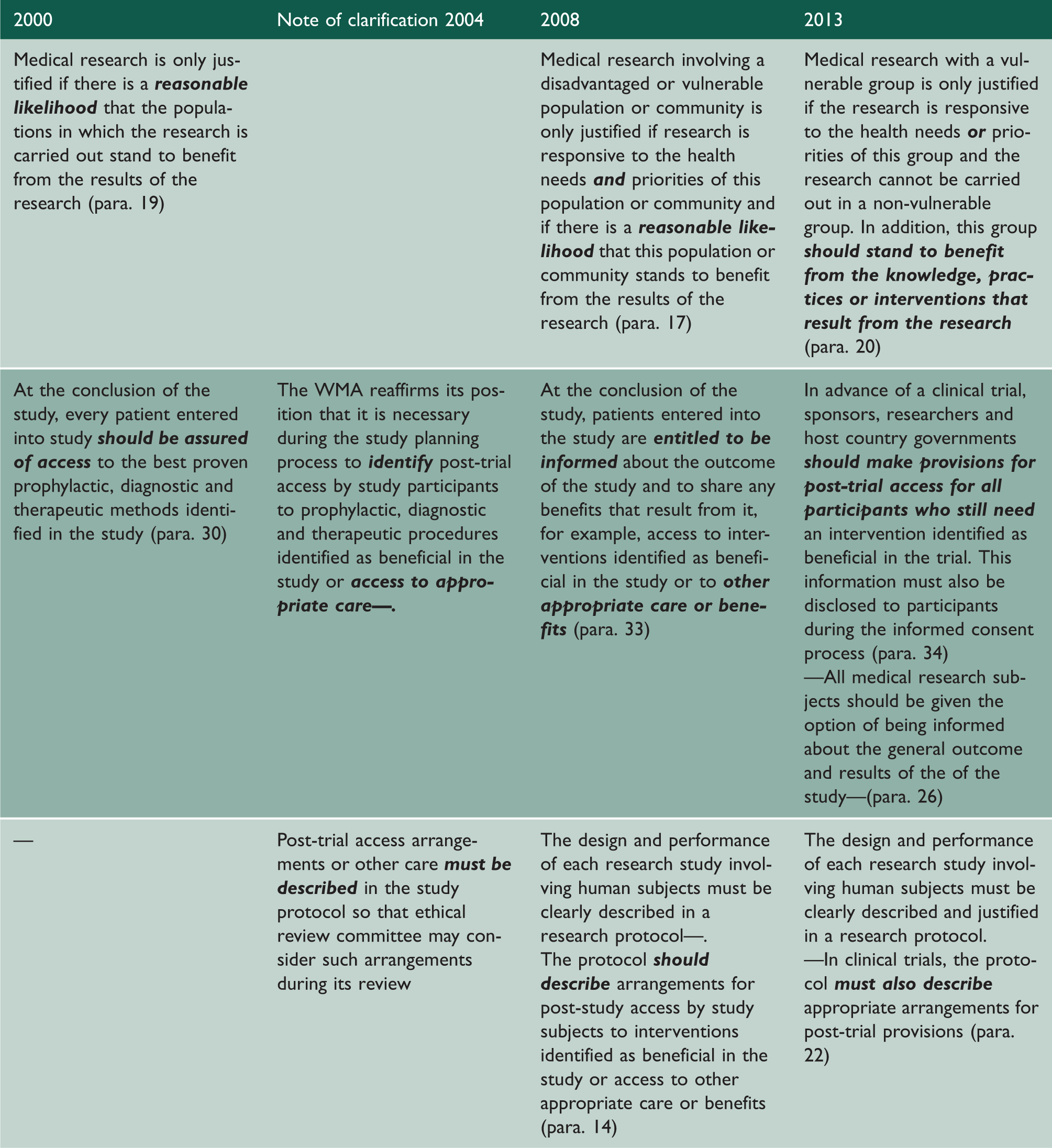
A key principle, embodied increasingly in successive iterations, is the ‘Responsiveness principle’ (Table 2). This demands that the trial should be relevant to the health needs of the local population (and participants should be selected fairly on the basis of their appropriateness to the research aims) and that the local population should benefit from the research. Whereas a narrow interpretation of benefits may be that the proven intervention is provided, a broader interpretation is that research benefits communities in other ways too, i.e. that post-trial benefits should not be limited to the provision of the proven intervention. 8 Benefits might include collateral health services not related to the research study, improvements in health and healthcare, employment and economic activity, long-term research collaboration, capacity building, and the sharing of financial rewards from research results. 11
Although the 2013 version endorses a broad conception of ‘benefits’, it will give rise to much discussion as to what ‘priorities’ may legitimately be considered. Power differentials between local physician-researchers and patient-participants, to the degree that the former may have unquestioned authority,12–14 make it challenging to ascertain ‘fair benefits’ from patient-participants’ perspective. Priorities considered important by the physician-researchers should not trump health needs of patient-participants. This means that patients enrolled in the trial must be represented in the process of developing the plan for the allocation of ‘fair benefits’.
The requirement to be responsive to the ‘health needs or priorities’ rather than ‘health needs and priorities’ – that was present in the 2008 version (Table 2) – may compromise the responsiveness principle.
The new Paragraph 34: Post-trial provisions
Paragraph 34 of the 2013 version requires that: In advance of a clinical trial, sponsors, researchers and host country governments should make provisions for post-trial access for all participants who still need an intervention identified as beneficial in the trial. [3, emphasis added]
This indicates a change from 2008 – where enrolled patients were ‘entitled’ to be informed, as opposed to the 2000 version where enrolled patients were ‘assured of access’ (Table 2). The new, sternly imperative ‘should’ is a significant endorsement of the responsiveness principle.
However, the phrase ‘access —to other appropriate care or benefits’, present in the 2008 version, is conspicuous by its absence from the new Paragraph 34 (Table 2). This is likely to lead to restrictive application of this requirement and may weaken the protection for participants, especially in low and middle income countries. 15 Having said this, reading the new Paragraph 34 and Paragraph 20 together ought to effectively meet the requirement of ‘access— to other appropriate care or benefits’ through fulfilling the requirement: ‘this group should stand to benefit from the knowledge, practices or interventions that result from the research’ (para. 20). It is plainly important that participants are aware of their rights. Hence, the Declaration emphasises in Paragraphs 26 and 34 that information regarding post-trial provisions must be disclosed to participants during the consent process. 3
The ethical principles underpinning the demands of Paragraphs 20 and 34 are justice and beneficence. In clinical trials, researchers gain a benefit by the acceptance of risk by patient-participants. Justice demands that, as a rule, there is compensation for the assumption of this risk, in the form of access to the proven intervention,16,17 and there is empirical evidence that patient-participants consider ensuring post-trial access to the trial drug a moral obligation.18,19
It is not enough to make a normative claim: the normative demands will be frustrated unless there is a viable pre-trial plan to ensure access to proven interventions. Tough contract negotiations are crucial. Collaboration is essential for a sustainable flow of the intervention. 20 Ad hoc approaches are ineffective.
Conclusion
The motivating spirit of the Declaration is clear from Paragraphs 15 (about compensation), 33 (which frowns on placebos) and 20 (which enshrines the principle of distributive justice and evinces the concern, evident from the birth of the Declaration, with the protection of the vulnerable). Paragraph 34 is more problematic. We do not doubt its intentions: it intends to ensure ethical post-trial provision of benefits, and in deciding on the ruling ethics it relies on the principles of beneficence and distributive justice that have consistently motivated it. But Paragraph 34 is drafted rather strangely: it may be that its eccentricities will frustrate some of its good intentions.
The changes are real: they indicate a steady, incremental evolution towards a holistic code for the regulation of research on human participants. Patient autonomy, crucial though that is, is no longer the sole concern of the Declaration. There is now much more than a nod to distributive justice: the principle is, increasingly, a motivating force. The draftsmen have learned, and will no doubt continue to learn, about the practical problems of implementing philosophical abstracts in hot and poor places. The new version of Paragraph 33 indicates an awareness of those realities. While the Declaration is aware of the need to facilitate research, where that facilitation clashes with the need to protect the vulnerable, the vulnerable win. That has, often to the frustration of sponsors/researchers, been (with a few faltering moments) the case throughout the life of the Declaration. The new version seems to have even more resolve than its forebears.