
Abstract

Introduction
Despite having enacted an Immigration Act less than two years previously, in 2016 the UK government proposes going even further, with even more restrictive measures set out in a consultation document entitled Making a Fair Contribution. 1 The earlier Act introduced major restrictions on access to the NHS in England by overseas visitors and migrants that were heavily criticised, on three main grounds. 2 First, they imposed a high administrative burden on hard-pressed NHS staff. Second, they threatened the sustainability of the NHS workforce, already facing severe shortages in many areas, and in which 26% of all doctors qualified outside the European Economic Area (EEA). Third, they increased risks to the health of both migrants and the established population through late detection and inadequate treatment of both communicable and non-communicable diseases.
Proposed changes for non-EEA residents who have not paid the health surcharge.
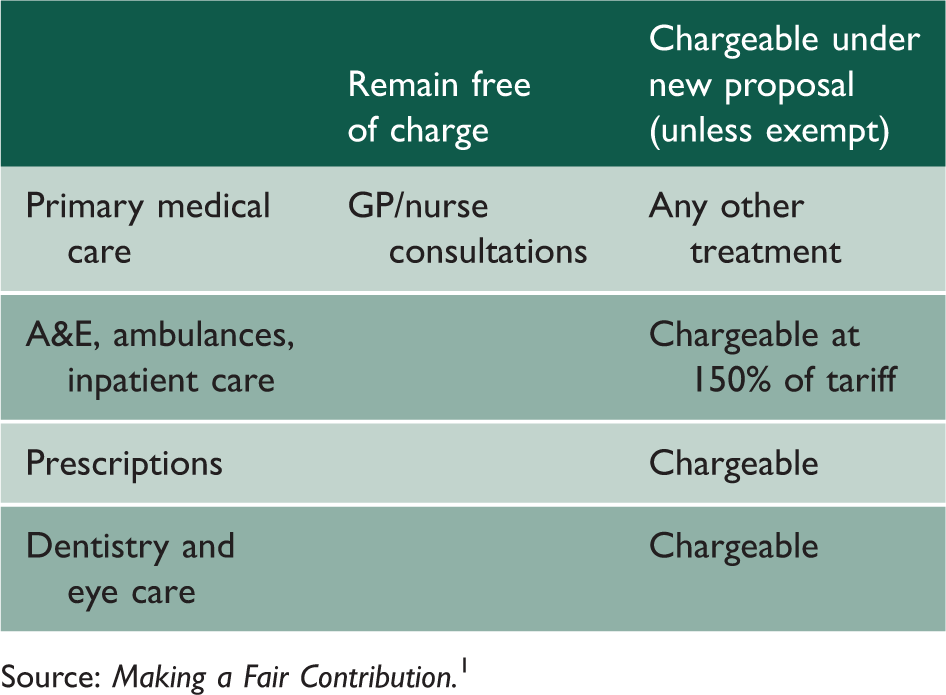
Source: Making a Fair Contribution. 1
Methods
The four overarching principles of the NHS.
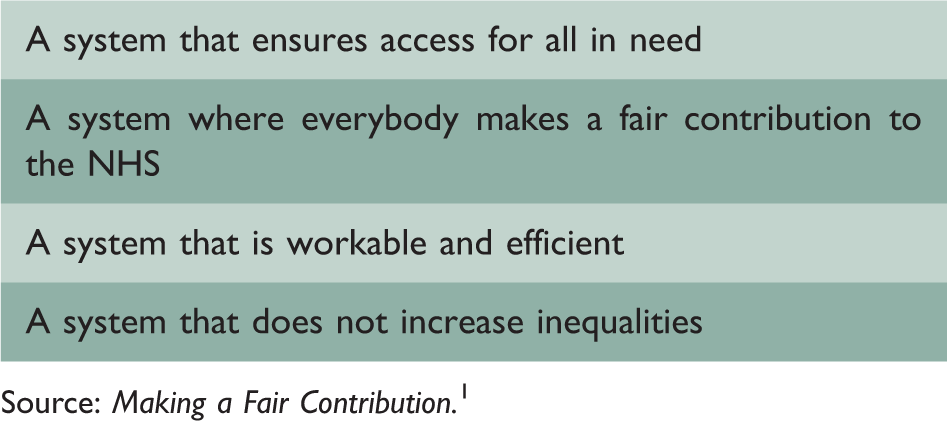
Source: Making a Fair Contribution. 1
We perform a conceptual analysis by examining each principle in turn; testing the proposals for charging non-EEA migrants against them, to assess if these changes are consistent with the philosophy claimed for the NHS.
Results and discussion
A system that ensures access for all in need
The imposition of charges for ambulance and emergency services for those in need is difficult to reconcile with the principle that no one should be denied timely, necessary treatment and with the position of the UN High Commission on Refugees that refugees in Europe should ‘have access to health services at equal levels to that of nationals’. 6
Evidence from the US shows that people lacking health insurance are significantly more likely to present late in emergencies. 7 In addition, it is easy to envisage major practical challenges, ranging from the challenge of extracting payment from those who, by virtue of their immigration status, are prevented from working, to a situation in which someone collapses in a public place but is deterred from getting into an ambulance by the risk of what could be, for them, catastrophic payment. This would seriously test the altruism of passers-by who stopped to help.
There are some exemptions, such as those suffering from contagious diseases, but many of the most vulnerable migrants already find the system extremely complex, 8 reducing their likelihood of seeking timely and effective care. Although, in general, migrants are at low risk of infectious disease, 9 experiences in Spain 10 and Greece, 11 where access to care by migrants has also been cut, show how undiagnosed or inadequately treated infections and children without access to routine immunisations can pose a risk to the existing population. Non-communicable diseases, such as diabetes, left untreated could also result in preventable serious complications, which, as German researchers have shown, 12 ultimately carries a greater long-term cost to the health system, as well as potentially reducing the ability of migrants to contribute to future economic growth in the UK.
A system where everybody makes a fair contribution to the NHS
The imposition of charges sends an implicit message that migrants do not already contribute to the NHS. Yet, between 2001 and 2011 non-EEA migrants contributed 2% more in taxes than they took out, amounting to a net fiscal contribution of £2.9 billion. 13 Furthermore, most arrive having completed their education abroad allowing the UK to reap the benefits without having contributed to the cost. 13 Consequently, the assertion that these individuals are not ‘making a contribution’ is unfounded; yet, this message appears frequently in the British tabloid press. Examples of this are plentiful, including headlines from the Daily Mail ‘… NHS is chasing £65 million from foreign patients … with one alone owing £467,000’ 14 and The Sun claiming that the ‘NHS “too good to migrants”’. 15
A linked message from the consultation, and again in some parts of the media, is that ‘our system is an outlier compared to the majority of other countries’1 in terms of providing care free at the point of delivery. This is both wrong and irrelevant. Almost all health systems in industrialised countries do so and many are, as in the UK, funded by general taxation. The NHS is consistently ranked as one of the most cost-effective healthcare systems, outperforming other high-income countries in many areas, despite spending less. 16 The Migration Integration Policy Index ranks the UK at number 7 in the responsiveness of healthcare policy to the needs of migrants, behind countries such as Norway, Italy and New Zealand. 17 The UK should be striving to improve this ranking; not taking measures that would almost certainly worsen it.
A system that is workable and efficient
Distinguishing those who should be charged is complex and difficult in practice. The administrative burden placed upon NHS staff, especially now that there is extensive evidence of staff shortages, would simply add to a workload that many consider already to be unmanageable. Staff would be required to ‘act as immigration officials’ in addition to their primary jobs. 2 The resources required to police patient attendances and ensure invoices are raised appropriately would be extensive and costly. Moreover, it is inevitable that errors would be made, potentially leading to costly legal implications.
The threat posed to health protection by charges is cited as the reason why GP consultations will remain free, noting the need to ‘lessen the risk of potential outbreaks’. 1 Consequently, as noted above, treatments for certain infectious diseases, such as tuberculosis, measles and HIV, are exempt from charging. However, the diagnosis may not be obvious and it may be difficult to divide the process of care between those elements that are chargeable and those not. There is also a risk of increasing referrals for ‘tuberculosis’ by well-meaning GPs seeking free care for impoverished migrants, skewing public health data collection and putting GPs in an impossible position when arranging potentially chargeable investigations.
With GP and nurse consultations in primary care, the only remaining free NHS service, there is also a real danger that their workload could become completely unsustainable, given the pressures on an already overstretched primary care system.
Another potential conflict lies in the differing care of migrants in immigration removal centres to those outside of them. The care in these centres is currently meant to be ‘NHS equivalent’, and would remain free of charge, but a significant proportion of those detained would not be eligible for free healthcare if released. This creates a serious risk of discontinuity of care. It could potentially lead to migrants wanting to be detained or remain in an immigration removal centre to gain free healthcare. Additionally, such discontinuities are well recognised to be a risk factor for the development of multi-drug resistant tuberculosis.18,19
A system that does not increase inequalities
It is difficult to reconcile a measure that disadvantages some of the most vulnerable in society with a commitment to reducing inequalities, and it is noteworthy that the proposal is not accompanied by any inequality impact assessment, but with the promise of one in the government’s response to the consultation.
Introducing these charges could set a dangerous precedent for those disadvantaged in other ways. One reason given for the 150% tariff is a need for translators. Would the next step be that non-English speakers, or those who have visual or hearing impairment, should pay towards their healthcare? Or those with a disability who are unable to make a ‘fair contribution’? What about children born with a life-limiting illness that will likely never be able to contribute? The notion of a ‘fair contribution’ is ultimately flawed and against the founding principles of the NHS which strives to protect the most vulnerable.
Conclusion
We contend that the proposed changes do not abide by any of the four overarching principles in Making a Fair Contribution, that they are ideologically driven and unlikely to result in substantial savings. We also believe that most NHS staff will find these proposals offensive and unworkable, creating further tension in an environment already suffering from low morale. The criteria for charging are confusing and assessment would be time-consuming, imposing a huge administrative burden. Primary care is unlikely to be able to cope with the surge of attendances due to charging for A&E, eye care and dentistry.
These proposals are inherently at odds with the founding ethos of the NHS. As the founder of the NHS, Aneurin Bevan, noted, ‘Illness is neither an indulgence for which people have to pay, nor an offence for which they should be penalised, but a misfortune, the costs of which should be shared by the community’. 20