
Abstract
Summary
Objectives
The independent impact of individual surgical experience and team familiarity on surgical performance has been widely studied; however, the interplay of these factors and their relative, quantified, contributions to performance is poorly understood. We determined the impact of team familiarity and surgeon, and cumulative team experience on operative efficiency in total knee replacement.
Design
Retrospective analysis of all total knee replacements conducted at the host institution in 1996–2009. Multivariate generalised-estimating-equation regression models were used to adjust for patient risk and clustering.
Setting
Tertiary care academic hospital.
Participants
All patients undergoing TKR at the host institution in 1996–2009.
Main outcome measure
Operative efficiency.
Results
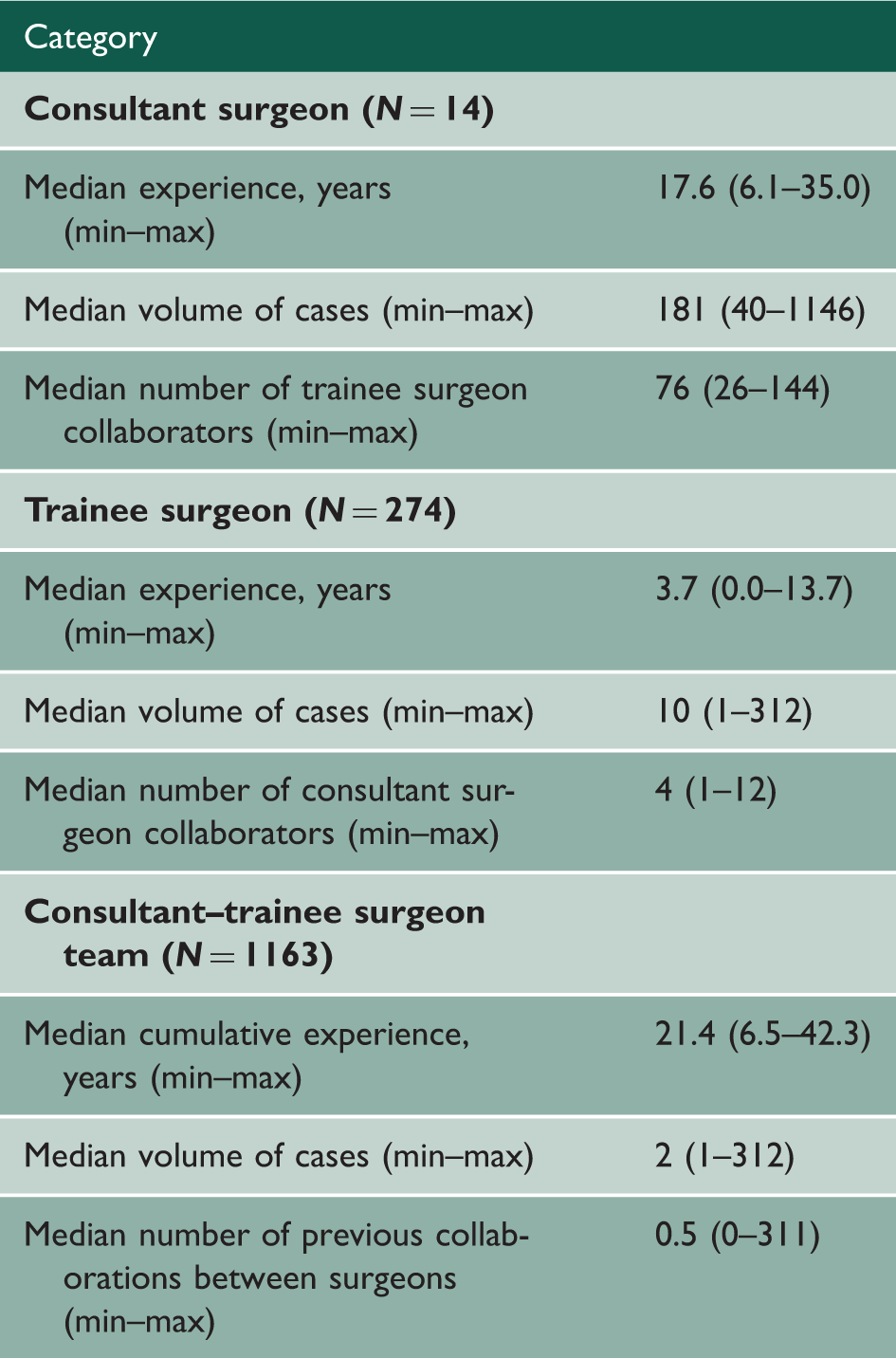
A total of 4276 total knee replacements were completed by 1163 different surgical teams. The median experience level was 17.6 years for consultant surgeons and 3.7 years for trainee surgeons. After patient-risk adjustment, consultant surgical experience (p < 0.0001), trainee surgical experience (p < 0.05), cumulative team operative experience (p < 0.0001) and team familiarity (p < 0.0001) were associated with significant reductions in operative time. Surgical experience and team familiarity demonstrated concave and linear relationships with operative time, respectively. For a consultant surgeon, the expected reduction in operative time after 25 years in practice was 51 min, compared to a 21-min reduction over the span of 40 collaborations with the same team members.
Conclusions
Surgical experience and team familiarity display important and distinct relationships with operative time in total knee replacement. Appreciation of this interplay may serve to guide implementation and allocation of procedure-specific quality improvement strategies in surgery.
Keywords
Introduction
With the increasing availability of high-resolution clinical data in the surgical sphere has come a markedly improved ability to investigate core drivers of surgical outcomes. 1 Stated plainly, the advent of the so-called Age of Big Data has enabled investigators to elucidate key forces that influence surgical efficiency, safety and quality to a degree that was not possible in the past. 2
Among the drivers that have been described to determine surgical performance is experience.3–6 While experience has traditionally referred to the maturity of the attending surgeon performing a given procedure, recent investigations have also provided the opportunity to broaden this definition to include the collective experience of the attending-resident dyad, as well as their level of familiarity (within the National Health Service, this is directly analogous to the consultant-surgical trainee dyad).7,8 While the independent influence of these factors on surgical performance has been demonstrated, their interplay and relative, quantified, contributions to performance is poorly understood.
In response to this investigative opportunity, we here present the results of a study in which we employed a prospectively collected, high-volume dataset with simple, reliable and quantifiable measures to assess the impact of different aspects of experience and team familiarity on operative efficiency in total knee replacement.
Methods
Design and population
Data for all total knee replacement procedures performed at a single academic tertiary care centre from 1996 to 2009 were culled from a combination of electronic medical records, an electronic operative time-tracking application and physician employee databases. The dataset was filtered to exclude erroneously coded procedures including partial knee replacements, combined procedures, bilateral procedures, and incomplete or incorrect data entries.
Operative time was defined as the time elapsed from skin incision to skin closure. The operative experience of the consultant surgeon was calculated as the difference between the date of the procedure and that of the surgeon’s completion of training. The operative experience of the trainee surgeon was calculated as the difference between the date of procedure and that of the surgeon’s training program start date. Cumulative team experience was defined as the sum of the consultant surgeon’s experience and the trainee’s experience. Familiarity was defined as the number of collaborations between a specific consultant surgeon and a specific trainee; it was calculated by measuring the cumulative number of total knee replacements performed previously by the same two surgeons. This study was performed under Institutional Review Board approval (protocol 2006p000586).
Statistical analysis
The characteristics of patients and surgeons were described using absolute frequencies with percentages for categorical variables. The mean values with standard deviations and median values with minimum–maximum intervals were calculated for continuous variables. Variables associated with prior collaborations between the consultant surgeons and surgical trainees were identified. To compare dichotomous and continuous variables across levels of previous collaborations (0 collaborations, 1–5 collaborations, 6–10 collaborations and >10 collaborations), we used a Rao-Scott Chi-Square test 9 and a generalised estimating equations Wilcoxon rank-sum type test, 10 respectively, which accounted for clustering of patients by surgeon.
In addition, the expected performance curve of surgical teams over time was generated based on a multivariate generalised estimating equations regression model. Operative time was the outcome of interest, while the number of previous collaborations was the predictor. Previous collaboration was entered as a linear and a quadratic term. Consultant and trainee experience levels (each entered both as a linear and a quadratic term) as well as patient case-mix (patient age and co-morbidities including coronary artery disease, chronic obstructive pulmonary disease, type II diabetes mellitus, hypertension, obesity and smoking) were also considered as covariates in these models, taking into consideration the clustering of patients by consultant surgeon. 11 Model estimates were obtained using the GENMOD procedures in SASTM 9.2 (SAS Institute Inc., Cary, NC, USA). According to model estimates, the expected mean operative time with corresponding minimum and maximum values was displayed as a function of the number of prior collaborations. The expected reductions in operative time independently associated with the cumulative team experience or the number of prior collaborations within the surgical team were plotted. All tests were two-tailed, and p < 0.05 were considered significant.
Results
Overview of study participants.
Demographics and outcomes by number of prior collaborations.
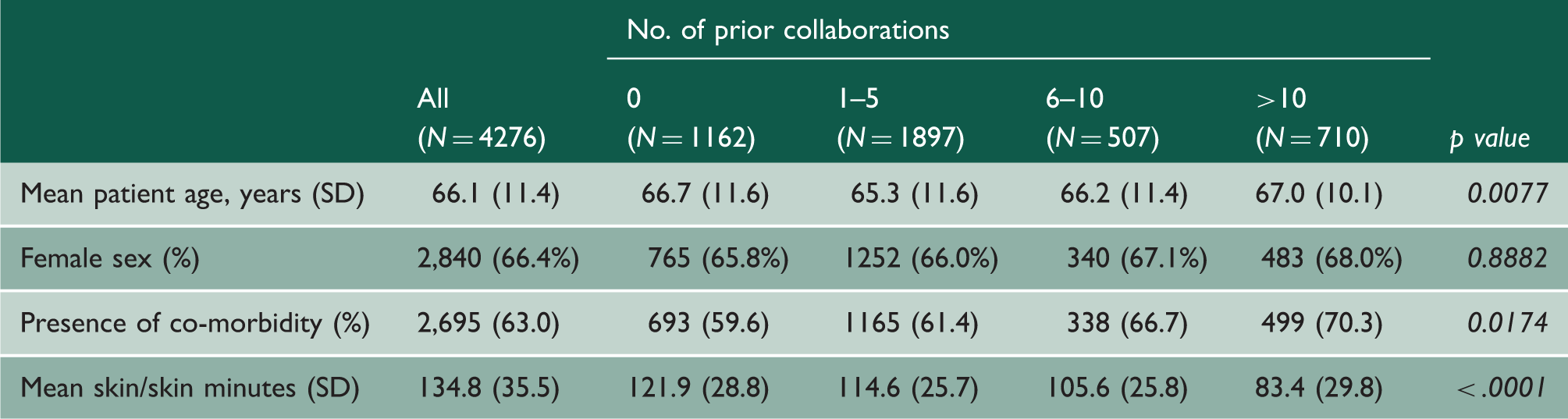
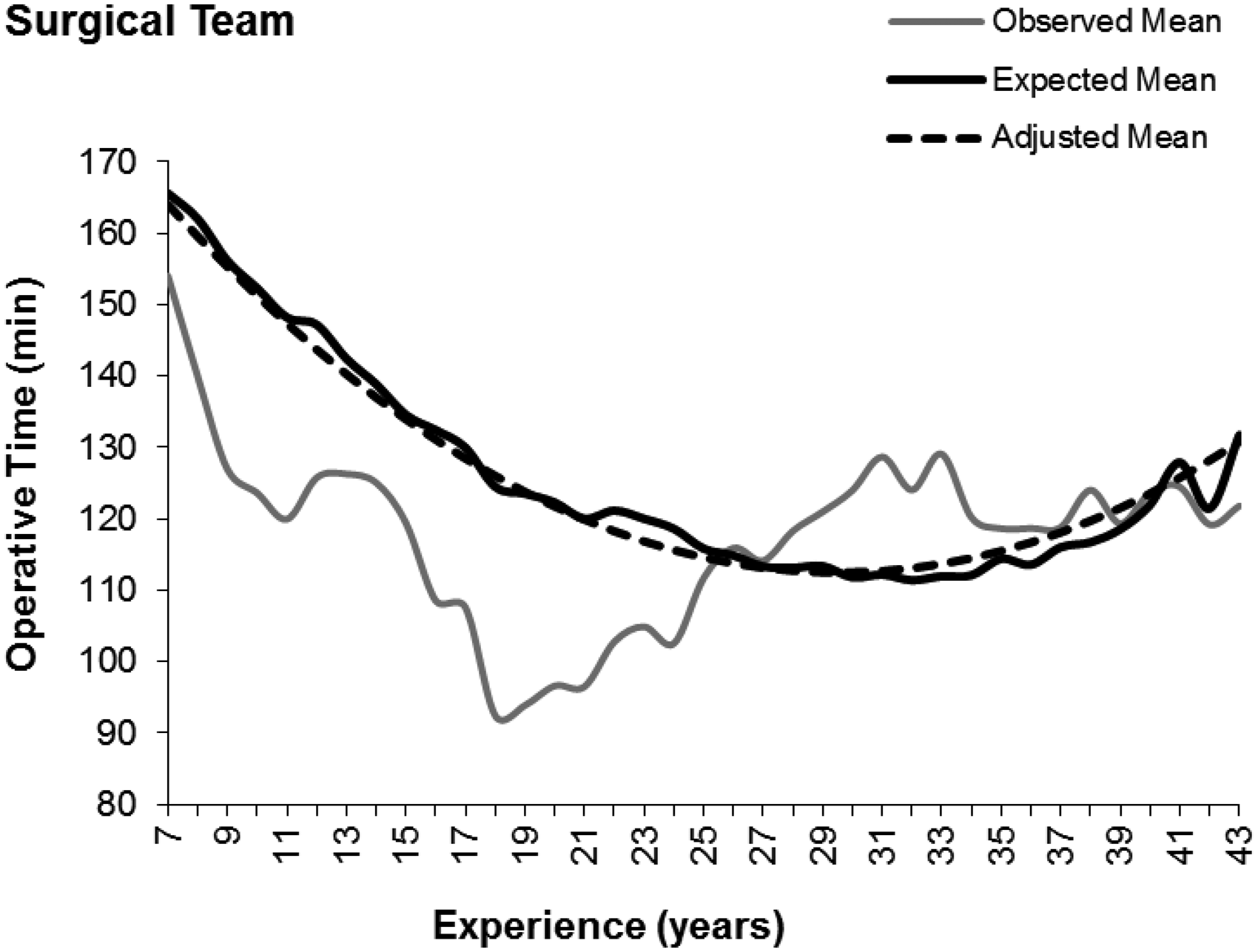
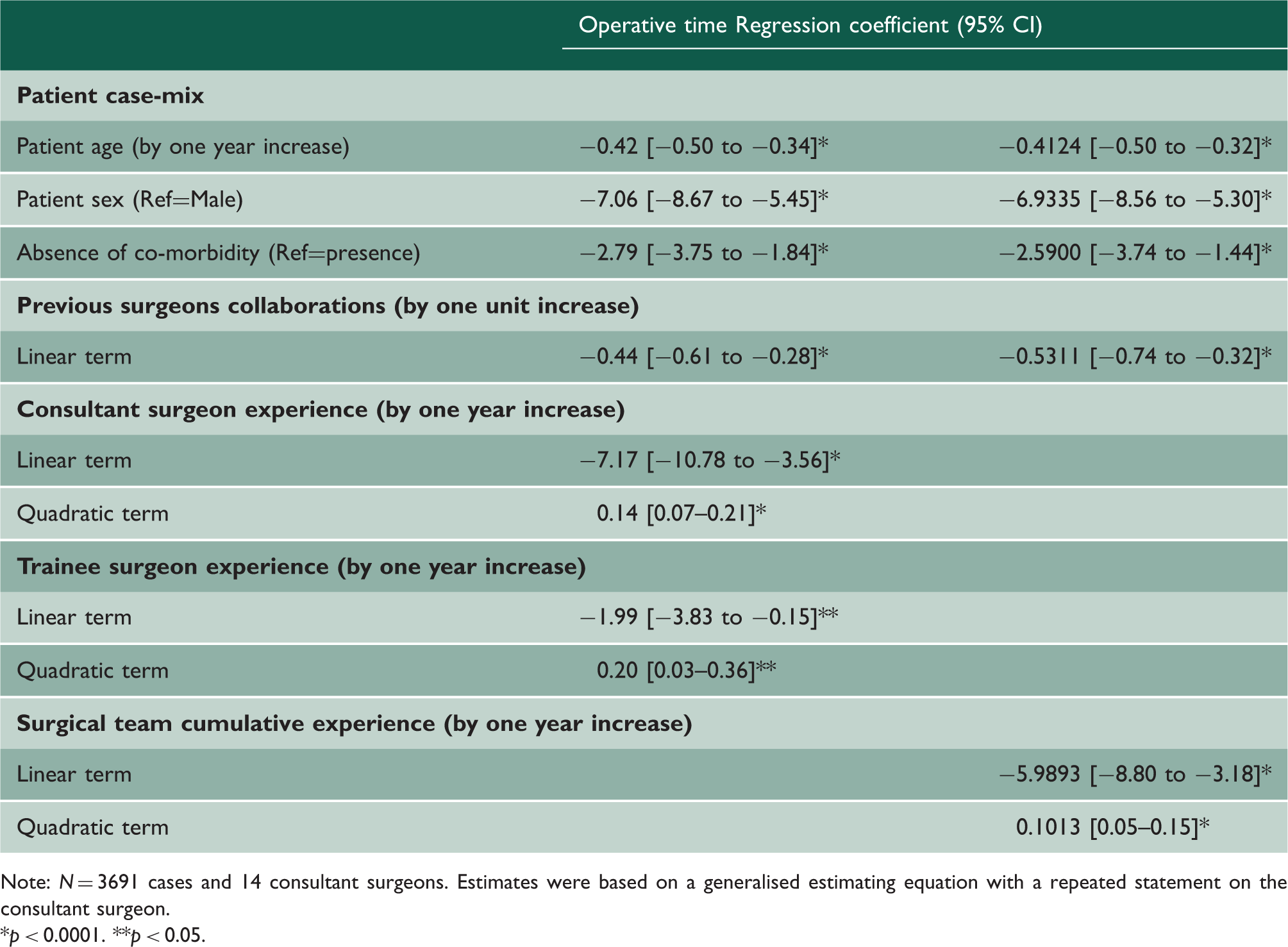
After adjusting for patient characteristics, we found a significant association between operative time and previous surgeon collaborations (p < 0.0001), as well as consultant surgeon experience (p < 0.0001), trainee experience (p < 0.05) and cumulative team experience (p < 0.0001) (Table 3). After adjustment of the raw observed data for case-mix variability (patient age and co-morbidities including coronary artery disease, chronic obstructive pulmonary disease, type II diabetes mellitus, hypertension, obesity and smoking), mapping of the consultant surgeon total knee replacement learning curve (Figure 1) revealed a concave relationship, with operative time declining by 51 min after 25 years of consultant surgical experience. Similarly, after case-mix adjustment, the surgical team total knee replacement learning curve (Figure 2) revealed a concave relationship, with operative time declining by 56 min after 30 years of cumulative team operative experience. On the other hand, mapping of operative time against team familiarity revealed a linear relationship (Figure 3(a) and (b)), declining by 21 min from teams with no prior collaborations to teams with over 40 prior collaborations.
Total knee replacement consultant surgeon learning curve. Raw observed data are shown in grey. Adjustment for patient case-mix (dashed black line) reveals that consultant surgeons’ growing operative experience was associated with reductions in operative time over the course of the procedural learning curve, reaching a plateau at approximately 26 years. Reductions in expected operative time as a function of cumulative team experience. Raw observed data are shown in grey. After adjustment for patient case-mix, cumulative team experience versus operative time demonstrated similar improvements in operative efficiency through 31 years of combined consultant/trainee experience (dashed black line). (a) Expected operative time as a function of team familiarity. Increasing team familiarity between discrete consultant–trainee surgeon pairs was independently associated with a reduction in both operative time and operative time variance. (b) Risk-adjusted operative time as a function of team familiarity. Operative time displayed a linear relationship with team familiarity. Multivariate analysis of patient and surgical team characteristics. Note: N = 3691 cases and 14 consultant surgeons. Estimates were based on a generalised estimating equation with a repeated statement on the consultant surgeon. p < 0.0001. **p < 0.05.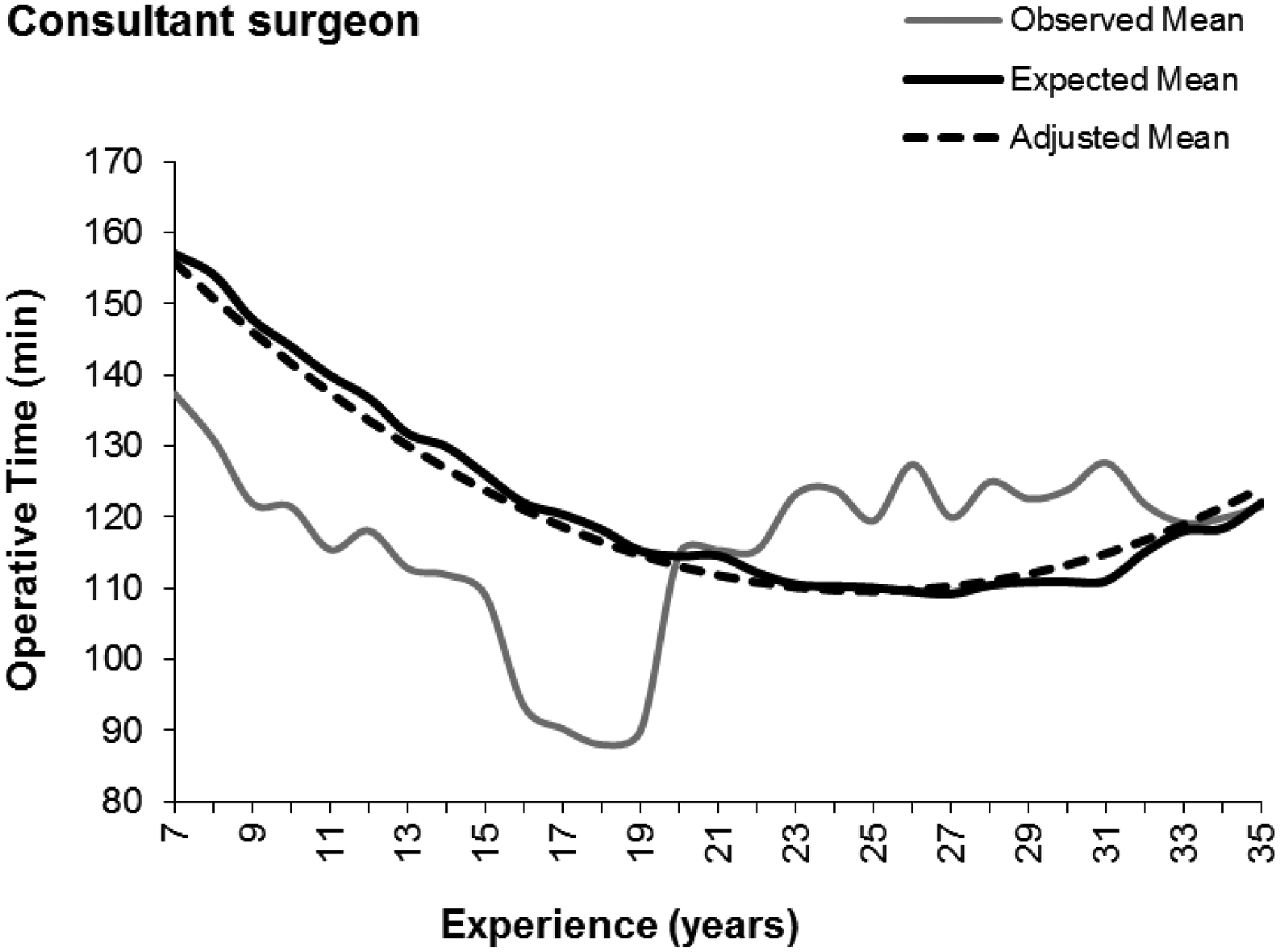
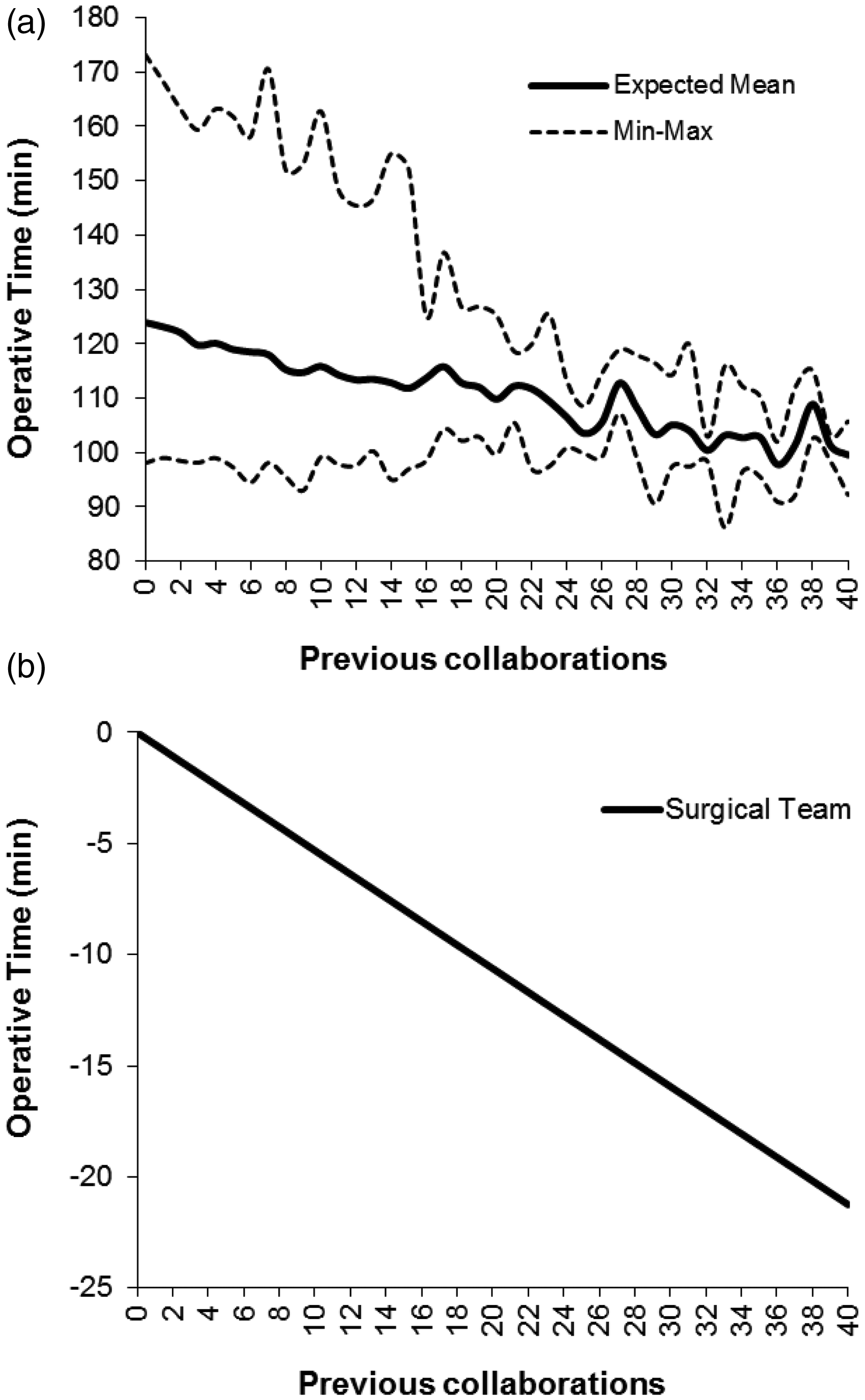
In addition to mean operative time, the operative time variability across teams gradually decreased as the number of prior collaborations increased (Figure 3(a)). Among teams with no prior collaborations, the range (min, max) of operative times was 75 (98–173) min, declining to 50 (98–148) min after 10 collaborations, 25 (100–125) min after 20 collaborations, 17 (97–114) min after 30 collaborations, and finally 13 (92–105) min after 40 collaborations.
Discussion
Our study demonstrates that operative efficiency is independently influenced by both consultant and consultant–trainee cumulative experience, as well as by the degree of familiarity of the consultant–trainee team. While these results are in keeping with intuition: that both increasing experience and familiarity should lead to improvements in operative efficiency, it is important to note that the characteristics of improvement in each case were distinct. In the cases of consultant and consultant–trainee cumulative experience, for example, both appear to exhibit a concave relationship with operative time that plateaus at approximately 25 years and 29 years, respectively, after which efficiency decayed with increasing experience – findings consistent with similar learning curve studies performed for other procedures in the past.3,12 Alternatively, increasing team collaboration was associated with a linear decrease in operative time and improved operative time variance – one that does not appear to extinguish even after 40 collaborative total knee replacements between a given consultant and trainee.
These findings, however, must be considered in the context of this study’s limitations, which include the following:
This retrospective investigation was performed at a single academic medical centre. Of note, however, the retrospective nature of this approach removed any Hawthorne effect with regard to performance assessment, and therefore may have provided a more rigorous depiction of procedural dynamics than could have been obtained prospectively. Our focus on operative efficiency as an outcome did not implicitly incorporate considerations related to surgical safety such as complication rates. Studies, however, have indicated that faster completion of the total knee replacement procedure is associated with better outcomes.
13
Indeed, in a variety of work both within surgery and outside, the time of task completion has been used as a robust indicator of learning and outcome.3,14–18 Our investigation utilised years of training and/or practice as a proxy for surgical experience, rather than number of cases performed. This limitation is due to our inability to capture procedures performed at other institutions by surgeons in our study cohort. However, years of training and/or practice have been utilised as an acceptable substitute for surgical experience in prior published studies in the surgical literature, with similar caveats.3,7,8,19 We focused on the familiarity and cumulative experience of the consultant–trainee dyad only. However, it is important to note that other team members, such as the scrub-nurse, and familiarity with the equipment/technologies used will also play an important role in team dynamics and performance.
The distinct nature of these observed relationships has specific implications that warrant thoughtful consideration. Increasing operative experience, either at the individual consultant level or at the level of the consultant–trainee pair, is highly correlated with improved efficiency in a manner that effectively reaches a saturation point at the end of the third decade. This suggests that surgical teams performing total knee replacements later in their careers, regardless of prior collaboration, are likely to operate more efficiently.20,21 While these findings are in keeping with intuition, our study provides evidence as to the magnitude of the improvement witnessed with increasing experience, as well as the diminishing importance of such experience past the 30-year end point. Such data may be helpful in efforts to reduce operative times and lower costs22,23 by enabling more accurate operating room scheduling and utilisation. 24 In addition, our graphical depiction of the influence of experience on operative efficiency also appears to indicate a decay in operative time past the 30 year mark; further investigation of the latter phenomenon is warranted. This post-plateau decay has been described in a number of other studies although no underlying cause has been clearly demonstrated. However, several potential hypotheses have been proposed, including a propensity towards increased mental fatigue, reduced compliance with evidence-based medicine and reduced stress tolerance among older surgeons. 25 It has also been suggested that the increasing administrative, research and leadership responsibility associated with seniority may also contribute.
In contrast, the linear influence of collaboration on operative efficiency in our study population suggests a positive relationship that does not appear to extinguish within the window we investigated, although it is likely that beyond the examined number of collaborations, a saturation point would be reached. This finding is distinct from the familiarity–efficiency relationship for reduction mammoplasty, identified by our group, which instead displayed a curvilinear relationship, demonstrating the procedure-specific nature of these dynamics. 7 Importantly, this may suggest that familiarity-based interventions could serve as less-saturating and consequently higher-yielding strategies than those focusing on performance at the individual level. Practically, it is conceivable that re-ordering staff rotations to make allowance for this level of team collaboration could be significantly more cost-effective than interventions aiming to accelerate surgical experience. This also highlights the importance of team training in the surgical curriculum, which may play an almost equal role to individual factors such as technical proficiency in a surgeon’s development.
Importantly, the development of experience- and collaboration-based learning curves like those elucidated in this study has the potential to inform efforts to prospectively monitor individual and team surgical performance on an ongoing basis. Through the application of iterative quality improvement systems such as statistical process control, the depicted learning curves could be utilised as a baseline against which to chart the progress of surgical personnel – whether to meet administrative or educational goals. Such methodologies are designed to first identify and then address unwarranted variation in clinical processes, which generally leads to substantial coincident improvements in efficiency, safety and quality; while initially conceived for the manufacturing industry, they have recently been recognised as having increasing relevance to the healthcare sphere. 3 Compared to more traditional approaches to quality control, they offer a more accurate means of assessing performance and guiding improvement initiatives, particularly when they are, as in the case of the data presented here, tailored to a specific operative procedure.19,26 The application of statistical process control methodology to the data presented here is explored in greater detail in a separate report. 27
Team familiarity and surgical experience are established drivers of surgical performance. This study quantitatively characterised the relative influences of familiarity and consultant, trainee and cumulative team surgical experience on operative time. Appreciation of this interplay serves to guide implementation and allocation of procedure-specific quality improvement strategies in surgery. Future research should aim to characterise the relationship shared by these factors with performance for other types of surgery, additional members of the operative team and alternative patient-centred outcomes.