
Abstract
Renal and cardiac diseases are both prevalent and carry significant morbidity and mortality. They share common vascular risk factors and are physiologically interlinked. Dysfunction in one organ affects the other. Concurrent renal and cardiac disease is associated with a poor prognosis. This close relationship is reflected through cardiorenal syndrome. A classification system has been proposed; however, the underlying process is complex and multifactorial. Management of this syndrome focuses on improving heart function, reducing volume overload, and managing heart failure and chronic kidney disease. This, however, is challenging, limited by paucity of evidence and may lead to suboptimal therapy. Increased recognition of this syndrome should raise awareness in providing early therapy and avoiding adverse outcomes due to under-treatment. In this article, we provide an overview of our current understanding of cardiorenal syndrome, as well as its pathophysiology and treatment options.
Introduction
Within the human body, interactions between various organs are tightly controlled. The heart is responsible for ensuring that blood is circulated within the body, including to the kidneys, while the kidneys are responsible for filtering the circulating blood and managing electrolyte homeostasis. Both organs are undoubtedly crucial to our survival, tightly linked and inevitably inter-reliant. The maintenance of cardiovascular haemostasis is therefore dependent upon fine interactions between the heart and kidneys. It is thus not surprising that dysfunction in one organ will affect the other.
Indeed, cardiac disease and renal disease share common vascular risk factors (hypertension and diabetes to name but a few). Both renal disease and heart failure (HF) are independently associated with a poor prognosis. Concurrent renal disease and HF, given their close bi-directional relationship, are as a consequence associated with a worse prognosis 1 and hence a greater burden on our healthcare system and patient quality of life. The existence of this dual dysfunction has been recently termed as ‘cardiorenal syndrome’.
Cardiorenal syndrome has been difficult to define because it encompasses complex multifactorial facets including physiological, biochemical and hormonal. Following a consensus conference in 2008, 2 the report defines cardiorenal syndrome as ‘disorders of the heart and kidneys whereby acute or chronic dysfunction in one organ may induce acute or chronic dysfunction of the other’.
The purpose of this article is to provide an overview of our current understanding of cardiorenal syndrome as well as its pathophysiology and treatment options.
Methods
Within this review, we aimed to summarise the results of a MEDLINE, PubMed, Cochrane Library, Google and Google Scholar search (from January 1931 to September 2014) on the current understanding of the epidemiology, pathophysiology and treatment of cardiorenal syndrome. Databases were searched using the term ‘cardiorenal syndrome’, and articles were selected and analysed according to their relevance.
Epidemiology
Renal dysfunction frequently coexists with HF. The Acute Decompensated Heart Failure National Registry demonstrated that 30% of patients admitted with acute decompensated HF had chronic kidney disease (CKD) and 21% had a creatinine of >2 mg/dL. 3 In a study by Forman et al., 4 irrespective of HF, with or without preserved ejection fraction, raised serum creatinine on admission to hospital and worsening renal impairment during admission were both associated with prolonged inpatient stay and increased mortality.
Worse baseline renal function is a powerful independent risk factor for adverse cardiovascular outcomes. 5 However, not all studies show an adverse association with declining glomerular filtration rate (GFR). The Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterisation Effectiveness trail did not show statistical significance or increased mortality with a 25% decline in GFR. 6 This reflects that a decline in kidney function due to adequate diuresis or blockade of the renin–angiotensin–aldosterone system (RAAS) may be associated with improved outcomes.
Classification
Classification of cardiorenal syndrome based on a system proposed by Ronco and McCullough. 2
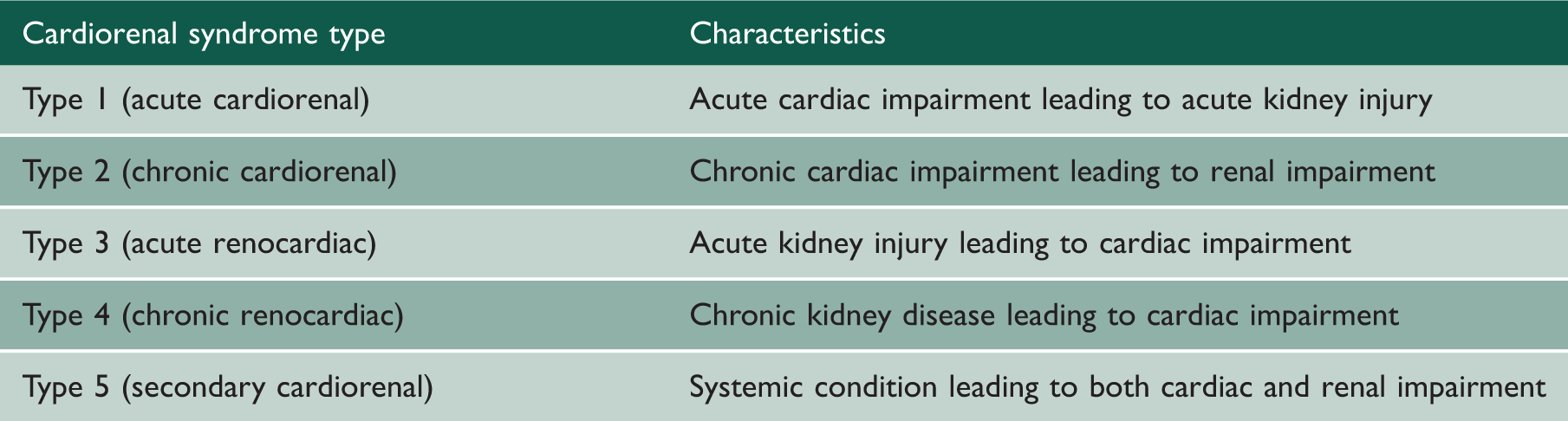
Acute cardiorenal syndrome (type 1)
Cardiorenal syndrome type 1 is characterised by acute worsening of cardiac function (pulmonary oedema, cardiogenic shock, acute HF) leading to an acute kidney injury (AKI). Approximately 27% of patients admitted with acute decompensated HF develop AKI. 4 The challenge in this subtype is the early identification of an AKI as creatinine will increase once AKI is established and early biomarkers such as neutrophil gelatinase-associated lipocalin have been studied as early predictors of AKI. 7
Chronic cardiorenal syndrome (type 2)
Cardiorenal syndrome type 2 is characterised by chronic cardiac dysfunction leading to renal dysfunction and can be used to describe chronic HF leading to renal failure. This syndrome is the most common and has been reported in 63% of patients admitted with congestive HF.2,8 The mechanism underlying this process is likely to be due to chronic renal hypoperfusion although there is limited evidence as of yet to suggest how left ventricular function correlates to GFR levels. 7
Acute renocardiac syndrome (type 3)
Cardiorenal syndrome type 3 is characterised by acute cardiac dysfunction (uraemic cardiomyopathy, arrhythmias due to hyperkalaemia) as a result of acute renal impairment. Defining the epidemiology in this subtype has proven a challenge due to different methods for defining AKI, different baseline risks for developing acute cardiac dysfunction and limited reporting by studies of AKI on the incidence of acute cardiac dysfunction as an outcome measure. 2
Chronic renocardiac syndrome (type 4)
Cardiorenal syndrome type 4 describes CKD leading to cardiac dysfunction (left ventricular failure or diastolic HF). Cardiac disease in patients with CKD is common, and adverse cardiac outcomes correlate well with severity of CKD. 2
Secondary cardiorenal syndromes (type 5)
Cardiorenal syndrome type 5 is characterised by simultaneous cardiac and renal dysfunction as a part of a systemic condition whether that may be acute or chronic. This most commonly includes systemic conditions such as sepsis and less so others such as amyloid or vasculitis.
Pathophysiology
A number of mechanisms have been identified as having a role in the development of cardiorenal syndrome. The pathogenesis is complex involving multiple pathways which have not yet been fully elucidated; however, a number of mechanisms have been proposed. Detailed descriptions of these are beyond the scope of this article; however, chronic over-activation of the neurohormonal systems and increased venous pressure are thought to be important factors.
Neurohormonal system
Initial triggering of the neurohormonal systems such as the RAAS, the sympathetic nervous system (SNS), the arginine-vasopressin system and the endothelin system is thought to be protective and aims to maintain homeostasis. The chronic activation, however, of all these mechanisms can have deleterious effects on both the cardiac and renal system.
Activation of the RAAS in the kidney leads to sodium and water retention, systemic vasoconstriction and further reduced glomerular filtration. The RAAS activation increases oxidative stress and further downstream profibrotic neurohormonal enhancement resulting in ventricular remodelling. 9 Chronic SNS over-activation results in reduced cardiac β-adrenoceptor density and sensitivity, 10 cardiomyocyte hypertrophy 11 and, through the enhancement of neuropeptide Y, vascular neointimal formation. 12 Impaired left ventricular function further contributes to decreased forward flow.
Increased venous pressure
HF is marked by an increase in central venous pressure which leads to a reduction in the perfusion gradient across the glomerular capillary bed and decline in renal function. The result of increased back pressure and its effects on urine formation was first studied around a century ago. In an experiment by Winton, 13 it was noted that urine formation was reduced with rising pressure. Right ventricular dilatation and dysfunction from elevated venous pressure further impairs left ventricular filling.
Management
The management of cardiorenal syndrome can be challenging. Treatment for HF may worsen renal function, and thus patients may receive suboptimal therapy impacting on their prognosis. Primary prevention cannot be overemphasised for both renal and cardiac disease as they share common risk factors. This includes blood pressure, cholesterol and glucose management as well as physical activity and smoking cessation. Although established guidelines exist for the management of HF and CKD separately, there is as of yet no consensus on the management of each cardiorenal syndrome individually. Instead, treatment strategies focus on managing the predominant underlying condition, whether that is cardiac or renal. As our understanding of the pathophysiology improves, we can look forward to more targeted therapies.
In this article, the management of cardiorenal syndrome has not been divided by subtype. This reflects the close interrelations between the different subtypes and in particular how therapies targeted to one subtype can also have a beneficial effect for other subtypes, such as the use of RAAS blockade in type 2 and 4. In general, however, within subtypes 1 and 2, therapy predominantly focuses on managing acute and chronic HF. For subtype 3, management of the underlying cause of AKI is most appropriate, while in type 4, management is challenging due to the multifactorial nature of HF secondary to CKD. Therapies for type 5 focus primarily on treating underlying pathology such as sepsis, amyloid or vasculitis.
We have subdivided treatment options therefore into the three following areas:
Improving cardiac function:
Inotropes The use of inotropic drugs is relevant in the treatment of cardiogenic shock. However, the hypothesis that use of intravenous milrinone in patients with HF in order to permit more effective diuresis has been refuted.
14
Similarly, no clinical benefit has been demonstrated with low-dose dopamine when used for the treatment or prevention of AKI.
15
Vasodilators Vasodilators such as nitrates form part of the treatment for HF. The effects of nesiritide (a recombinant human brain natriuretic peptide) on renal function in the treatment of acute decompensated HF are conflicting. The Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure trial found no change in risk of worsening renal function with nesiritide therapy, but it was associated with higher rates of hypotension.
16
Cardiac resynchronisation In a study by Van Bommel et al.,
17
patients with HF who had a GFR of <60 ml/min/1.73 m2 demonstrated a reduced response to cardiac resynchronisation therapy (CRT), defined as a decrease in left ventricular end-systolic volume >15% at six-month follow-up, compared to those with normal renal function. Worse renal function was also associated with worse long-term prognosis after CRT. Despite this, a systematic review by Garg et al.
18
demonstrated that CRT in patients with CKD led to an improvement in left ventricular ejection as well as GFR. More studies are required to evaluate this further; however, this suggests a degree of reversibility in cardiorenal syndromes 1 and 2. Beta-blockers Beta-blockers are avoided in acute HF but used in the management of chronic HF. In a systematic review by Badve et al.,
19
of patients with HF and CKD, the use of β-blockers reduced the risk of all-cause and cardiovascular mortality. However, it was associated with an increase in bradycardia and hypotension. Caution is to be exercised in their use in acute decompensated HF as they may further reduce forward flow and exacerbate renal dysfunction. Adenosine-receptor antagonists These drugs increase GFR by causing vasodilatation and increased renal perfusion. However, data from the PROTECT trial
20
suggests no difference in cardiovascular outcomes compared to placebo in the treatment of acute HF with renal dysfunction. Decreasing volume overload:
Diuretics First, low sodium intake needs to be reinforced. Diuretics are the mainstay of management in fluid overload in both HF and renal failure. Aggressive diuresis improves survival despite worsening renal function.
21
Intravenous diuretics, high dose loop diuretics and adding thiazides to loop diuretics are needed to try to overcome diuretic resistance where necessary. Diuretics are particularly useful in the management of type 1, 2 and 4 cardiorenal syndrome. Vasopressin receptor antagonists Tolvaptan is a selective vasopressin 2 receptor antagonist whose effect on cardiovascular actions was described in the Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan-Outcomes trial.
22
The study showed no effect on long-term mortality or HF-related morbidity. However, there was an increase in urine output resulting in improved dyspnoea as it increased free water clearance. Currently in the UK, tolvaptan is licensed for the treatment of hyponatraemia secondary to the syndrome of inappropriate antidiuretic hormone secretion. Ultrafiltration In recent years, ultrafiltration has had an increasing role in patients with decompensated HF and renal dysfunction, particularly affecting cardiorenal syndrome subtype 2. Three randomised trials (Ultrafiltration versus Intravenous Diuretics for Patients Hospitalised for Acute Decompensated Congestive Heart Failure [UNLOAD], Relief for Acutely Fluid-Overloaded Patients With Decompensated Congestive Heart Failure [RAPID-CHF], Cardiorenal Rescue Study in Acute Decompensated Heart Failure [CARESS-HF]) have compared diuretic therapy in patients with acute decompensated HF.23–25 In UNLOAD and RAPID-CHF, ultrafiltration was associated with greater fluid loss than diuretic therapy but no difference in serum creatinine, while in CARESS-HF weight loss was similar, but there was an increase in serum creatinine and greater adverse events. The 2013 American College of Cardiology Foundation/American Heart Association guidelines for the management of HF stated that “ultrafiltration may be considered for patients with refractory congestion not responding to medical therapy.”
26
Peritoneal dialysis has been trialled for the symptomatic management of refractory dyspnoea in end-stage HF with paucity of data from large randomised controlled trials.
27
Additional trials are ongoing to see the benefit of ultrafiltration. Drugs for reduced ejection fraction and CKD:
Renin–angiotensin–aldosterone system antagonism
RAAS antagonism is an integral part of therapy for acute and chronic HF and renal failure. Subgroup analyses of clinical trials of RAAS antagonism in HF have demonstrated that the beneficial effects on morbidity are not reduced by concurrent CKD. 28 The risk of hyperkalaemia and worsening renal function is higher in patients with CKD 28 and therefore requires regular monitoring.
Similarly, aldosterone antagonists showed a benefit in cardiovascular outcome despite a fall in GFR 29 with the same problem of hyperkalaemia.
Key points.
Conclusion
There is a high prevalence of cardiorenal syndrome where patients with HF have concurrent renal dysfunction. Reduced renal function is associated with increased morbidity and mortality in this population. It is a bi-directional relationship where dysfunction in either the heart or kidneys worsens the function of the other. Cardiorenal syndrome is difficult to define because it has multiple contributing factors; however, potential mechanisms include neurohormonal system activation leading to reduced forward flow and renal perfusion and increased venous pressure. Medical treatment options are primarily focused on improving cardiac function, reducing volume overload and managing HF and CKD. Although management of cardiorenal syndrome remains a challenge, increased recognition of this syndrome should raise our awareness in providing early therapy to improve patient care and avoid adverse outcomes due to under-treatment (Table 2).