
Abstract
Objective
In Britain, consent for surgery is documented using a Department of Health form signed by the surgeon and the patient. In contrast, anaesthetic procedures have no formalised consent process. Evidence on the process of consent for regional anaesthesia, and patient perceptions of this, is scarce outside obstetric practice. We aimed to determine patient recall and perceptions of consent for interscalene brachial plexus block and compared this to surgical consent for shoulder arthroplasty.
Design
Prospective observational survey.
Setting
A specialist musculoskeletal centre, UK.
Participants
Forty-six patients (female:male 30:16, mean age 61 years) undergoing shoulder arthroplasty with interscalene brachial plexus block.
Main outcome measures
Recall and understanding of consent for regional anaesthesia and surgery was examined using a semi-structured questionnaire 1–2 days after arthroplasty. Surgical consent forms and discussions recorded by the anaesthetist were examined in participants’ medical notes to compare against the level of recall. Analysis to determine statistical significance was conducted using McNemar’s test.
Results
Recall of surgical risks was overall significantly better than recall of brachial plexus block risks. Compared to their recollections of surgical risk, patients remembered fewer specific risks for brachial plexus block (p < 0.001). There were more patients unable to recall any risks when questioned about brachial plexus block than about their surgery (p < 0.05). One-third of patients did not regard the consent discussion about regional anaesthesia as important as consent for surgery and over one-quarter had not recognised the preoperative discussion about the brachial plexus block as a consent process similar to that conducted for surgery.
Conclusions
Fundamental misunderstandings about the consent process are prevalent. Future work in this area should seek to investigate how documentation of the consent process and patients’ understanding of consent for regional anaesthesia can be improved.
Introduction
Informed consent to medical investigation or treatment is the process of obtaining permission from the patient for conducting a healthcare intervention. To be valid, consent must be voluntary, informed and given by a person with capacity. In its fullness, a consent discussion comprises an explanation of the nature and the aims of a procedure, the associated risks and the alternatives to the intervention as well as the consequences of not intervening. During the consent process, the healthcare professional should make every effort to ensure capacity, answer the patient’s questions and tailor the information provided to the patient's needs, wishes and priorities. 1
To date, consent for anaesthesia has not received as much attention as consent for surgery in the medical literature, and there is a relative paucity of data about patient understanding and recall of consent for anaesthetic procedures. This includes consent for regional anaesthesia outside obstetric practice. Interscalene brachial plexus block is a regional anaesthetic technique which enables perioperative analgesia of the upper arm for shoulder surgery. In skilled hands, it is possible to achieve optimal pain control for shoulder replacement without reliance on systemically administered analgesics. Interscalene brachial plexus block is, however, associated with recognised rare but serious risks which can lead to permanent sequelae.2,3 We set out to evaluate the conduct of consent for interscalene block through its documentation on anaesthetic charts. To help understand the factors that determine patients’ perceptions and recall of consent for regional anaesthesia, we decided to compare this with consent sought for surgery. The study was conducted in a specialist musculoskeletal centre in the UK, where specific written consent forms are not used for anaesthetic interventions; a practice in line with guidelines produced by the UK Department of Health and the Association of Anaesthetists of Great Britain and Northern Ireland.4–6
Methods
An observational evaluation was conducted in a specialist orthopaedic and musculoskeletal centre where up to six anaesthetists are routinely involved in shoulder surgery lists. Approval as service evaluation was obtained through the local Research and Development Committee.
Adult English-speaking patients who had undergone primary or revision shoulder replacement under general anaesthesia combined with interscalene brachial plexus block were approached on the ward by a researcher 1–2 days after surgery and provided with information about the study verbally and in writing. The researcher returned 1–2 h later to enquire whether the patient was willing to participate and signed consent was obtained prior to proceeding. Patients were judged to be cognitively intact if they could recall their personal details (full name and date of birth), the date and name of their operation. Potential participants were excluded if they had not signed the consent form themselves, were unable to understand the questions or were medically unwell postoperatively.
Calculation of optimal sample size is difficult for an observational investigation on a subject that has not been specifically studied in the past. A recent review of patient understanding of the informed consent process for surgery included studies on cognitively intact adults in peer-reviewed journals published in English. 7 The study sample sizes were highly variable. Although one had a sample size of 732, all other studies of surgical consent that met the inclusion criteria had much smaller sample sizes (range, 18–164) with a median of 45. For this study, we considered a sample size of 45–50 acceptable for drawing meaningful conclusions.
Participants were interviewed using a structured questionnaire with 18 questions designed to examine their recall and understanding of consent for both interscalene brachial plexus block and shoulder arthroplasty. Following completion of the questionnaire, the investigator reviewed the participant’s medical notes and recorded the information on the surgical consent form and the anaesthetic chart on a standardised pro forma. Analysis to determine statistical significance was conducted using McNemar’s test in separate contingency tables. Data were managed using a Microsoft Excel™ 2010 spreadsheet.
Results
A total of 46 participants (29 women and 17 men) were approached. All met the inclusion criteria and all agreed to take part. The mean age of participants was 61 years (range, 29–84 years). Thirty-one (65%) had had primary shoulder arthroplasty and 16 (35%) revision shoulder replacement. On average, 1.7 days had elapsed between surgery being performed and interviews being completed.
There was good recall of meeting the surgeon (46, 100% recall) and the anaesthetist (45, 98% recall) in the immediate preoperative period. The majority of patients felt satisfied that they knew what they had agreed to undergo both in terms of the surgery (46 satisfied) and the interscalene brachial plexus block (42 satisfied); the difference between these was not significant (p = 0.11).
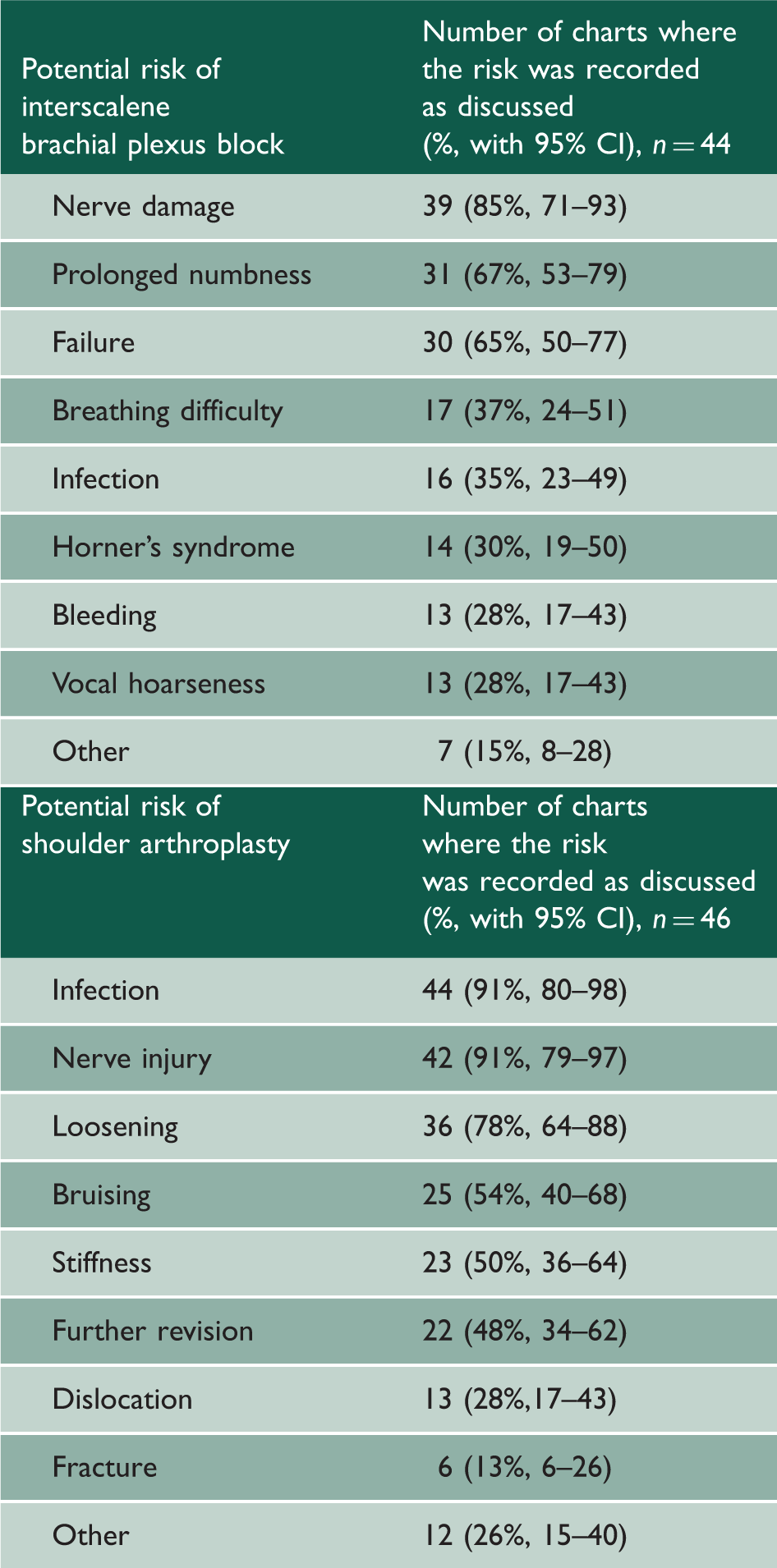
Documentation of consent
Risks recorded as discussed on anaesthetic charts or surgical consent forms.
Recollection of the consent process
Patient recall of risk discussions (n = 44).
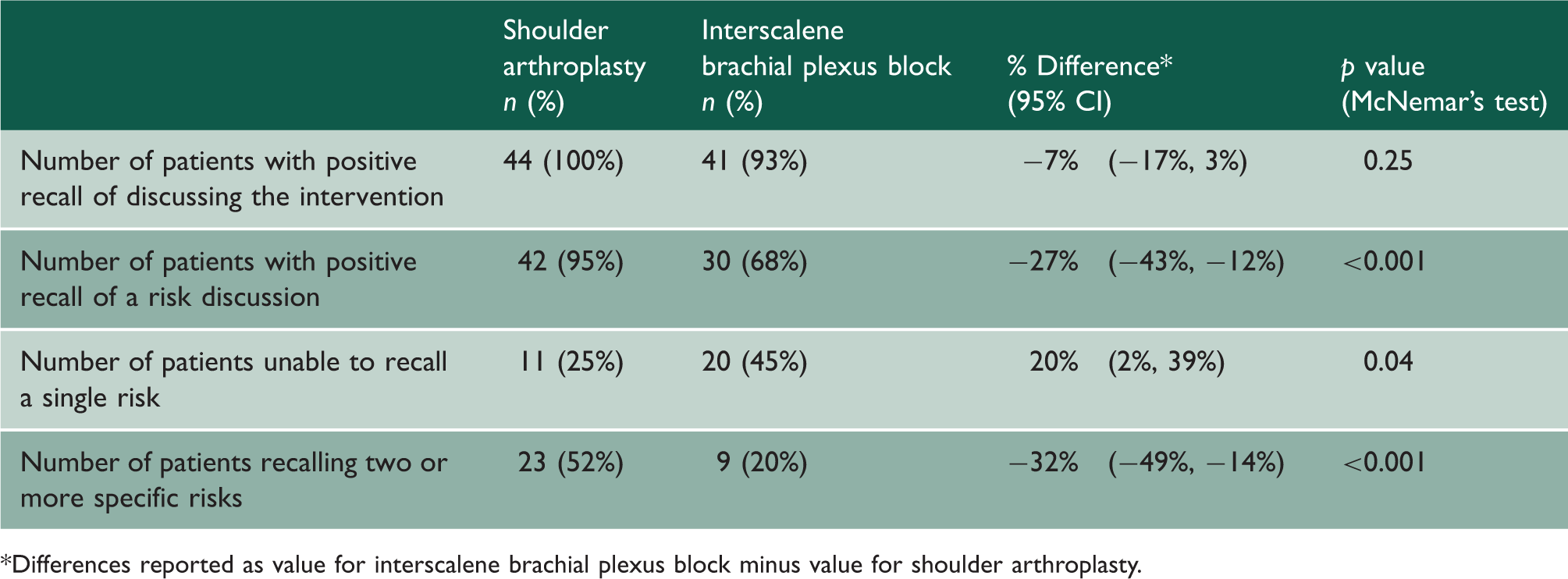
Differences reported as value for interscalene brachial plexus block minus value for shoulder arthroplasty.
Recall of the surgical risk discussions was overall significantly better than recall of interscalene block risk discussions. When asked whether they remembered being told about the risks and complications, fewer patients responded affirmatively to the question in relation to interscalene block (p < 0.001). We asked patients to try and recall as many risks as they could. Fewer patients could recall two or more risks of interscalene block than risks of surgery (p < 0.001), and there were more patients who could not recall any of the risks when they were asked about interscalene block (p = 0.04).
Understanding of the role of written consent
The majority of patients (34, 74%) believed written consent carries more legal weight than verbal consent. Sixty percent (28/46) of participants believed that once the consent form has been signed, they are bound by the decision and cannot withdraw their consent. Despite this, almost the same number (30) stated that they did not read the surgical consent form before signing it. When asked what they thought was the purpose of signing a consent form, over 50% (24/46) viewed it as a means by which the medical establishment protects itself against complaints or litigation.
Perceptions of consent for interscalene brachial plexus block
One-third of patients did not regard the consent discussion for interscalene brachial plexus block with their anaesthetist as being as important as the consent discussion for surgery. In the cases where there was documented evidence of consent, although most (42/44, 95%) patients stated that they understood why they had been offered interscalene block, 27% (12) of patients did not recognise the preoperative discussion about it as being a consent process similar to that conducted for surgery.
Despite the relatively poor recollection of the risks associated with interscalene brachial plexus block, only 20 (43%) participants felt that they would have liked to have been given more information, for example in the form of a leaflet or a website to visit about interscalene block.
Discussion
Documentation of consent for procedures related to anaesthesia has undoubtedly improved in the last two decades. However, there is evidence to show that there is still much room for improvement, and the deficiencies that we have observed in this single centre study are by no means an isolated finding. 8 As well as disseminating our findings locally, we have introduced measures to improve local practice (e.g. addition of a section on regional anaesthesia to a new patient information booklet on shoulder surgery).
Our findings concur with studies that have examined consent for surgery7,9,10 in that patient recollection of the consent discussion is often poor and that fundamental misconceptions about the consent process remain prevalent.7,11,12 Recall of consent discussions for anaesthesia has also been shown to be poor in the few studies that have examined this. A recent single-centre study of parental recall of information given at the time of consent discussions demonstrated that recollection of anaesthesia-related information was generally poor but improved when consent was obtained by an anaesthesia care provider. 12 In another study in which 159 patients had been given written information about anaesthesia, 64% had little or no recall of it. 13
We found significantly poorer recall and understanding of consent for regional anaesthesia compared to consent for surgery. An uncomfortable proportion of patients in this survey thought that consent for surgery is more important and over one-quarter of patients had not recognised the anaesthetist’s discussions with them about regional anaesthesia as part of a consent process even when they did recall it. The reasons for these findings are inevitably multi-factorial. In anaesthetic practice, patient contact is frequently limited to a single encounter, over a short period of time, in the immediate preoperative period. The Association of Anaesthetists’ 2006 5 guidance states that the ultimate responsibility for ensuring patient understanding lies with the anaesthetist and sufficient time should be allowed for this in the preoperative visit. However, to replicate the level of contact that characterises and ultimately facilitates the surgeon–patient interaction is inevitably difficult for anaesthetists on the day of surgery and this raises the question of whether consent discussions should always begin in anaesthesia preasessment clinics.
Another factor that affects patient’s perceptions of the consent process may be the use of a consent form. A consent form signed by the patient and surgeon is the norm in most surgical care settings in developed countries. In contrast, for anaesthetic procedures, there is great variation in the practice of obtaining consent particularly in relation to the use of a specific written form.14,15 Although there is evidence that surgeons and anaesthetists hold broadly similar views on consent, 16 the difference in practice between the specialties regarding the use of a written signed form has been enduring for decades and debate about it continues.15,17–19 Many have rightly argued that signatures on forms neither prove that consent has been correctly obtained nor protect against litigation. On a more critical note, the resistance to the notion of written signed consent may relate, at least in part, to uncertainties within the profession of how to disclose risks and the amount of information that should be given. 20
In this study, the variation in practice in terms of the risks discussed during consent for interscalene brachial plexus block in a single centre is striking; not one risk is consistently mentioned in all cases. Similar wide variations in risk disclosure for anaesthesia have been found in other studies and the reasons for this remain unclear.21,22 We agree with previous authors that there is a need for stronger consensus on what risks should be disclosed. Furthermore training in regional anaesthesia should incorporate this consensus.
The provision of accessible information to patients regarding their anaesthetic and related procedures may go some way towards achieving greater uniformity in practice and is recommended in the guidelines of several learned organisations.5,23,24 The findings of this evaluation suggest that the use of specific consent forms for anaesthesia could improve patient understanding of the consent process and may even elevate its status. It may also improve anaesthetists’ documentation of their discussions. The use of consent forms and written material does, however, bring with it other unresolved problems. This study and many others show that a significant number of patients do not read consent forms or written information given to them about surgery or anaesthesia.13,25,26 More innovative means of information provision, such as audiovisual materials that are readily accessible with commonly used electronic devices should be explored. A recent comprehensive review of this topic has outlined a number of effective strategies to improve the consent process for anaesthesia. 27
There are greater inherent complexities in understanding consent for anaesthetic procedures because they may reasonably be viewed by the patient as an essential part of the surgical process. Patients may therefore perceive all the discussion with the anaesthetist as merely an explanation of inevitable forthcoming events. The traditional view of consent for anaesthesia is that it should be given alongside consent for the procedure itself. 4 Taking this viewpoint, consent for anaesthesia is not a separate process but an integral part of consent for surgical intervention. However, this is at discord with what occurs in practice; the consent discussion for anaesthesia is undertaken by a different person and at a different time to consent for surgery. Further, most guidance on this subject assumes that all anaesthetic interventions are essential to the surgical procedure to the same degree.4,5 Arguably for regional anaesthesia interventions for postoperative pain, where there is true choice, a more systematic approach to consent is advised with an emphasis on the purpose of this intervention and full discussion of the alternatives.
Strengths and limitations
This study is one of few evaluations of consent for anaesthetic procedures. Many of the findings have been consistent with those of other studies of consent which gives external validity to the methodology. It is unique in comparing patient perceptions and recall of consent for an anaesthetic procedure in parallel with consent for a surgical intervention. Although the weaknesses in the process of consent for anaesthetic procedures have been pointed out by others, this is the first paper that explores whether the differences in the conduct of the consent process between surgeons and anaesthetists impede patients’ recollection and understanding of the risks of anaesthesia.
Considering we set out to examine recall of the consent process, our methodology could have included formal testing of patients’ memory. Previous studies of consent have also not included this and we recommend that it is part of future work that seeks to assess how understanding of consent may be improved. A limitation of this survey is that it has examined patients undergoing a specific operation in a single institution. This limitation has permitted meaningful comparison of the surgical and anaesthetic consent processes. It also allowed us to examine variation of practice in a highly specialist setting. Nevertheless, we acknowledge that the single-centre nature of this study may affect the extent to which its findings may be generalised.
Conclusions
This study has demonstrated that patients’ recall and perception of consent discussions for regional anaesthesia is significantly different to the same for surgery. The reasons for these differences is a subject for debate. This work emphasises the importance of adopting effective strategies to enhance patient understanding of consent for anaesthetic procedures. The findings make a significant contribution to the debate on the ethical and legal aspects of how consent for anaesthetic procedures should be discussed and documented in a way that is useful for both patients and anaesthetists.