
Abstract
Objective
There is evidence of substantial ethnic variations in asthma morbidity and the risk of hospitalisation, but the picture in relation to lower respiratory tract infections is unclear. We carried out an observational study to identify ethnic group differences for lower respiratory tract infections.
Design
A retrospective, cohort study.
Setting
Scotland.
Participants
4.65 million people on whom information was available from the 2001 census, followed from May 2001 to April 2010.
Main outcome measures
Hospitalisations and deaths (any time following first hospitalisation) from lower respiratory tract infections, adjusted risk ratios and hazard ratios by ethnicity and sex were calculated. We multiplied ratios and confidence intervals by 100, so the reference Scottish White population’s risk ratio and hazard ratio was 100.
Results
Among men, adjusted risk ratios for lower respiratory tract infection hospitalisation were lower in Other White British (80, 95% confidence interval 73–86) and Chinese (69, 95% confidence interval 56–84) populations and higher in Pakistani groups (152, 95% confidence interval 136–169). In women, results were mostly similar to those in men (e.g. Chinese 68, 95% confidence interval 56–82), although higher adjusted risk ratios were found among women of the Other South Asians group (145, 95% confidence interval 120–175). Survival (adjusted hazard ratio) following lower respiratory tract infection for Pakistani men (54, 95% confidence interval 39–74) and women (31, 95% confidence interval 18–53) was better than the reference population.
Conclusions
Substantial differences in the rates of lower respiratory tract infections amongst different ethnic groups in Scotland were found. Pakistani men and women had particularly high rates of lower respiratory tract infection hospitalisation. The reasons behind the high rates of lower respiratory tract infection in the Pakistani community are now required.
Keywords
Introduction
Acute lower respiratory infections are associated with significant morbidity and mortality and are one of the leading causes of years of life lost due to premature mortality. 1 Lower respiratory tract infection is an umbrella term and includes (among other diseases) influenza and pneumonia. In the UK, disease rates (in particular pneumonia and influenza) usually peak during the winter and spring months (i.e. September to February and March to May). 2 Risk factors that increase the likelihood of acute lower respiratory tract infections include chronic respiratory diseases (e.g. asthma and chronic obstructive pulmonary disease), tobacco smoking and immune suppression. 3 Of the lower respiratory tract infections, pneumonia causes the most deaths, with four million each year worldwide. Pneumonia is particularly prevalent in children and the elderly.4–6 For lower respiratory tract infections, reduction in modifiable risk factors, e.g. smoking and increased uptake of vaccination,7–9 represents an important approach to reduce illness and death.
Variations in lower respiratory tract infections by ethnic group have been noted previously in the United States (US), New Zealand and Australia.10–15 These studies found disparities in the incidence of lower respiratory tract infections among American Indian and Alaska native children and pneumonia among Black US adults and Māori in New Zealand. Some of these studies, however, did not adjust for confounding socioeconomic factors.11,13,14 National studies are needed to explore heterogeneity within broad ethnic groups, to maintain valid surveillance of trends and inequalities in diseases such as pneumonia, to set priorities (e.g. vaccination strategies and smoking cessation) and to ensure equitable service delivery. 16 Furthermore, ethnic variations in infectious respiratory diseases need periodic documentation. This is because disease patterns are altering over time as a result of changing environments and risk factor patterns (e.g. pollutants, housing, diet and smoking), particularly following migration. 17 Also lower respiratory tract infection rates may relate to travel, specifically religious travel such as the Hajj in which many people congregate at the same site and outbreaks of airborne/droplet borne infections (e.g. influenza, Middle East Respiratory Syndrome and meningitis) can occur. 18 Thus far, there have been few studies investigating ethnic variations in hospitalisations and deaths resulting from lower respiratory tract infections. Building on related work, 19 we undertook a national observational study, adjusting for socioeconomic confounding to identify ethnic group differences for lower respiratory tract infections.
Methods
We linked records from Scotland’s routinely collected hospital discharge records (SMR01) and the 2001 Census using probabilistic linkage methods (using information from multiple variables to maximise the chances of correctly linking disparate information on individuals) creating a retrospective cohort study of 4.65 million individuals; this represented over 90% of the Scottish population in 2001 (Figure 1). All personal identifiers including the encrypted Community Health Index identifier were removed from the data before analysis began. Over 80% linkage was achieved for each ethnic group.
19
Overview of Record Linkage Process (CHI and census numbers were encrypted).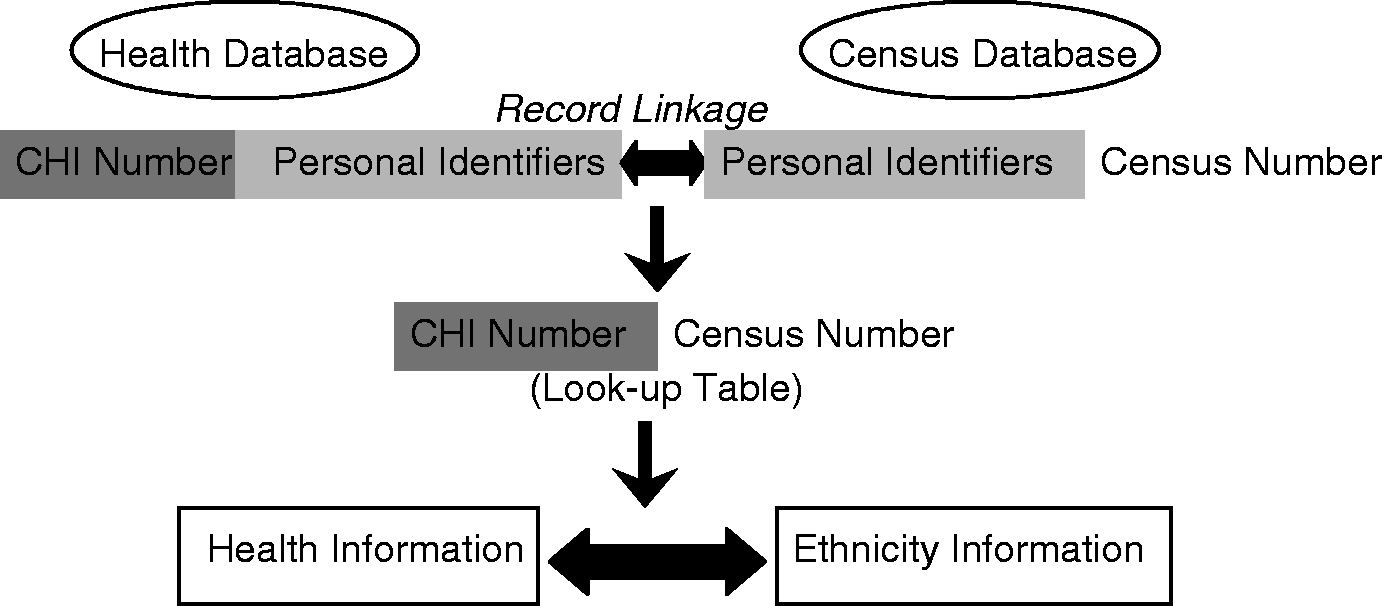
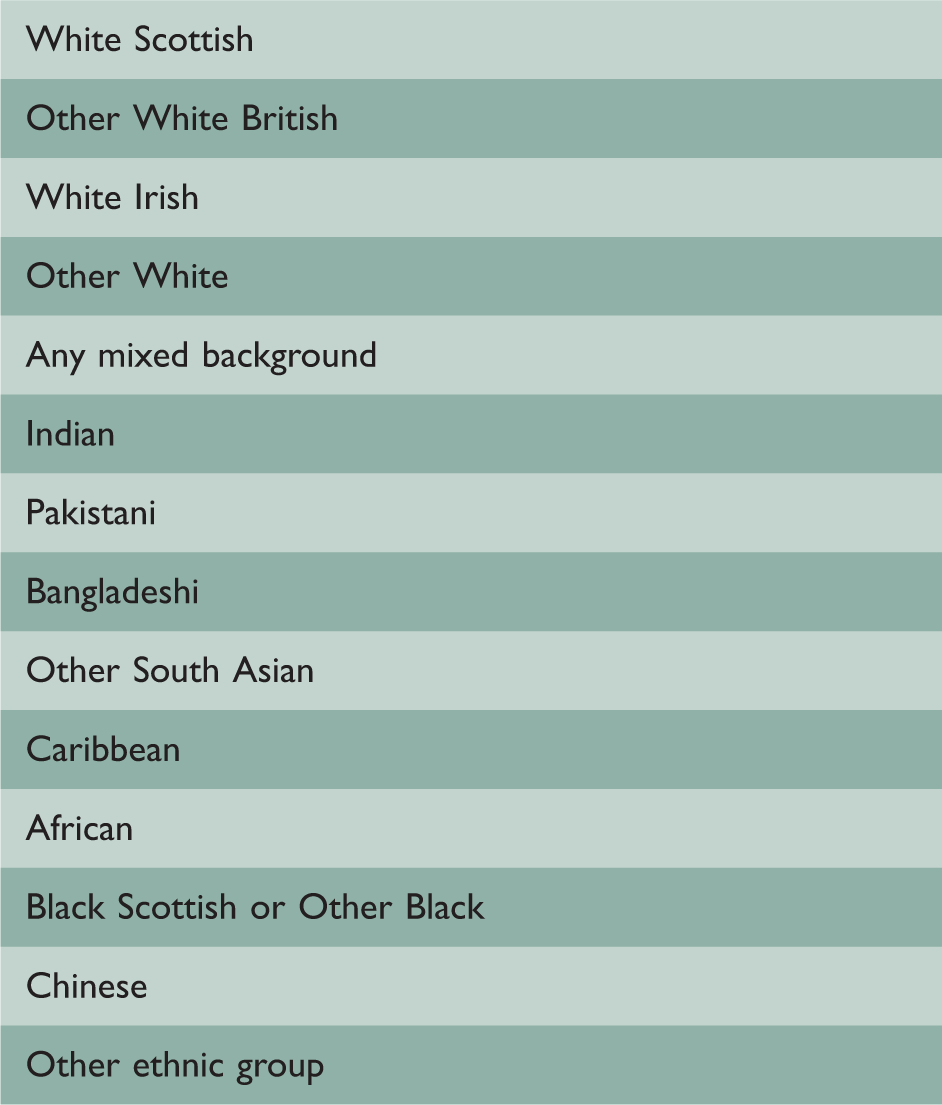
Ethnic groups
Scotland 2001 Census – self-reported ethnic groups.
Demographic and socioeconomic factors
In addition to age and sex, sociodemographic factors extracted from census data included: highest educational qualification of the individual (and separately the household), occupation, household tenure and quintile of Scottish Index of Multiple Deprivation. 20 The Scottish Index of Multiple Deprivation is the Scottish Government’s official measure of area-based multiple deprivation. It is based on 31 indicators in six individual domains of current income, employment, housing (although not household crowding), health, education, skills and training and geographic access to services and telecommunications.
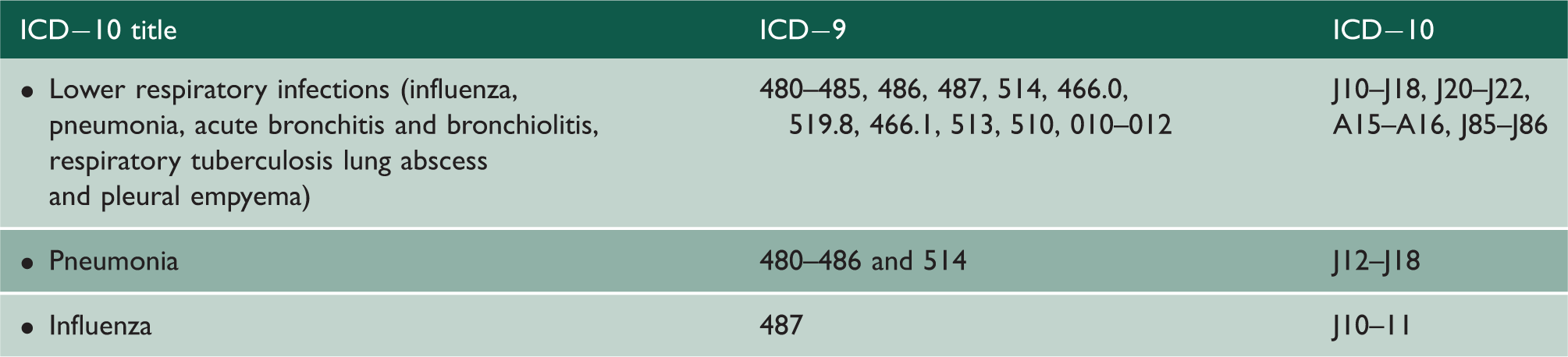
Outcomes of interest
International Classification of Disease (ICD)-9 and ICD-10 codes for respiratory conditions of interest.
Statistical analysis
We calculated age-adjusted rates and risk ratios (adjusted risk ratio) per 100,000/year with a person-years-at-risk denominator, using Poisson regression models with robust variance. As differences between sexes were found in previous analyses,16,19 an a priori decision was taken to stratify our analysis by sex. The White Scottish population was used as the reference population (risk ratio = 100) and all comparisons relate to the reference as stated or implied. We identified first events over a nine-year period: i.e. May 2001 to April 2010. No test for interaction was carried out because of the lack of statistical power, so observations on potential effect modification are interpreted as hypothesis generating and preliminary. We further adjusted risk ratios for country of birth (born in the UK or born outside the UK) and Scottish Index of Multiple Deprivation quintile as a proxy for socioeconomic status. We report overall age-adjusted survival to a cause-specific death following a first hospital admission for the same disease, for outcomes where there were sufficient numbers to allow analyses and satisfy disclosure control protocols. Survival analysis was carried out using Cox regression to calculate hazard ratios adjusted for age (adjusted hazard ratio) using the White Scottish population as reference. Survival to death and to readmission covered the nine-year follow-up period. Proportional hazards assumption was tested with the graphical method using log-log (-ln{-ln(survival)}) plots. Analyses were undertaken using the statistical analysis package SAS v9.3 (SAS Institute Inc., Cary, NC, USA).
Ethical approval
Ethical approval was granted by the Scotland A Research Ethics Committee. Permissions for data linkage and access to the Community Health Index were obtained from the Privacy Advisory Committee of the NHS Information Services Division, the General Register Office for Scotland (now National Records Scotland) and the Community Health Index Advisory Group. Access to data, analyses and release of outputs followed a prespecified protocol to ensure confidentiality and to prevent disclosure of any potentially identifying data.
Results
All lower respiratory tract infection hospitalisations and deaths for men.
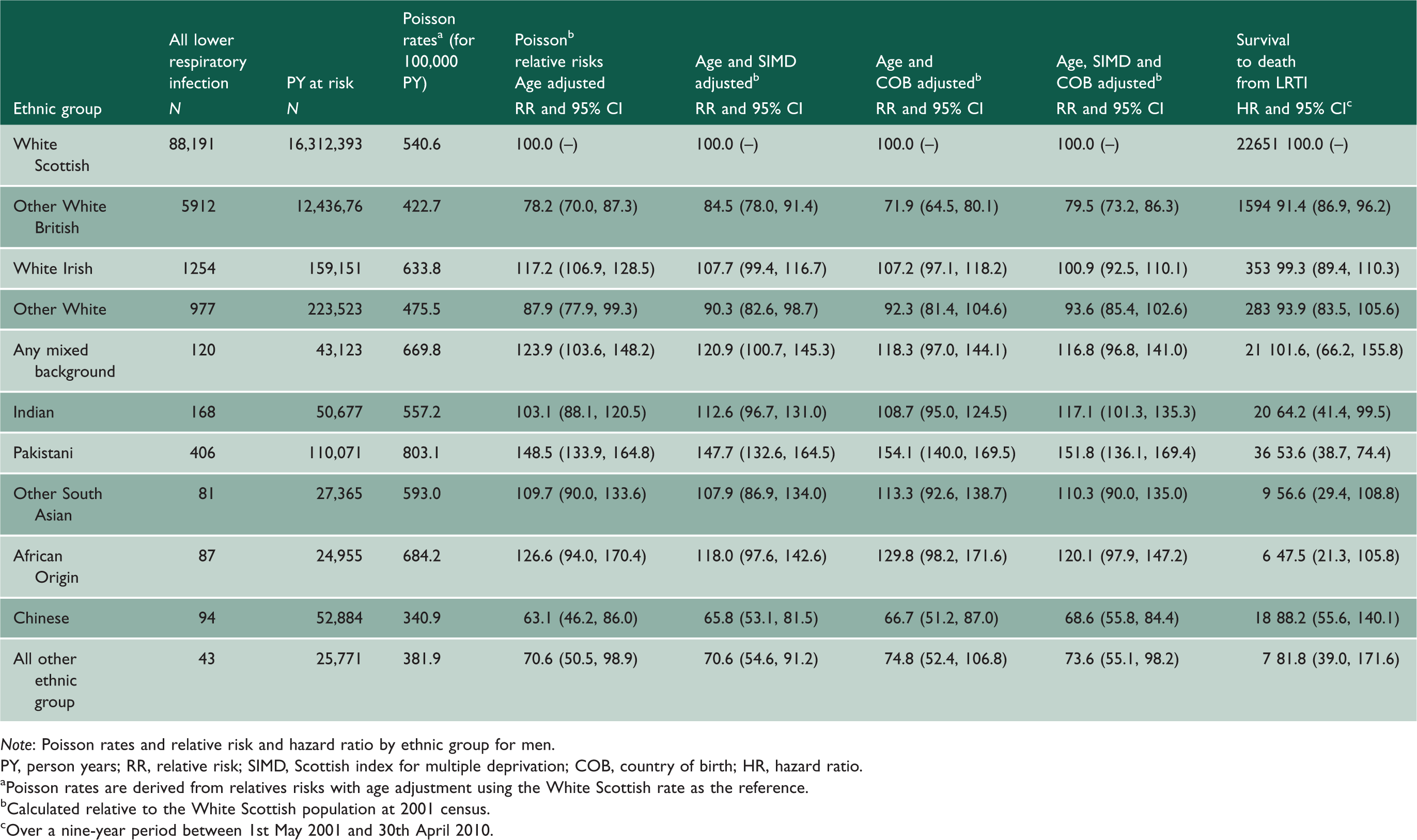
Note: Poisson rates and relative risk and hazard ratio by ethnic group for men.
PY, person years; RR, relative risk; SIMD, Scottish index for multiple deprivation; COB, country of birth; HR, hazard ratio.
aPoisson rates are derived from relatives risks with age adjustment using the White Scottish rate as the reference. bCalculated relative to the White Scottish population at 2001 census. cOver a nine-year period between 1st May 2001 and 30th April 2010.
Lower respiratory tract infection
All lower respiratory tract infection hospitalisations and deaths for women.
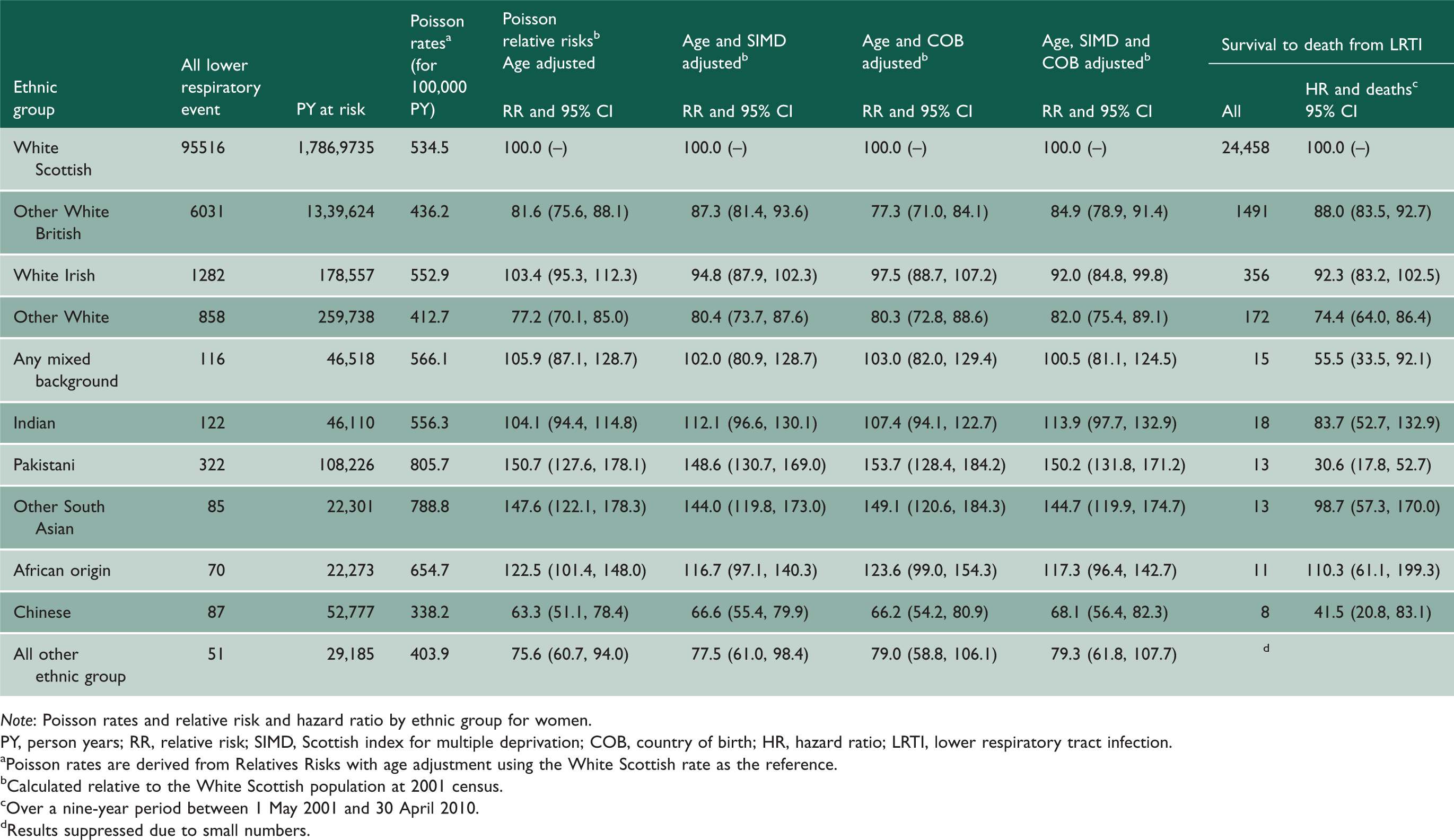
Note: Poisson rates and relative risk and hazard ratio by ethnic group for women.
PY, person years; RR, relative risk; SIMD, Scottish index for multiple deprivation; COB, country of birth; HR, hazard ratio; LRTI, lower respiratory tract infection.
aPoisson rates are derived from Relatives Risks with age adjustment using the White Scottish rate as the reference. bCalculated relative to the White Scottish population at 2001 census. cOver a nine-year period between 1 May 2001 and 30 April 2010. dResults suppressed due to small numbers.
Risk of readmission for any diagnosis following first hospital admission for LRTI and pneumonia.
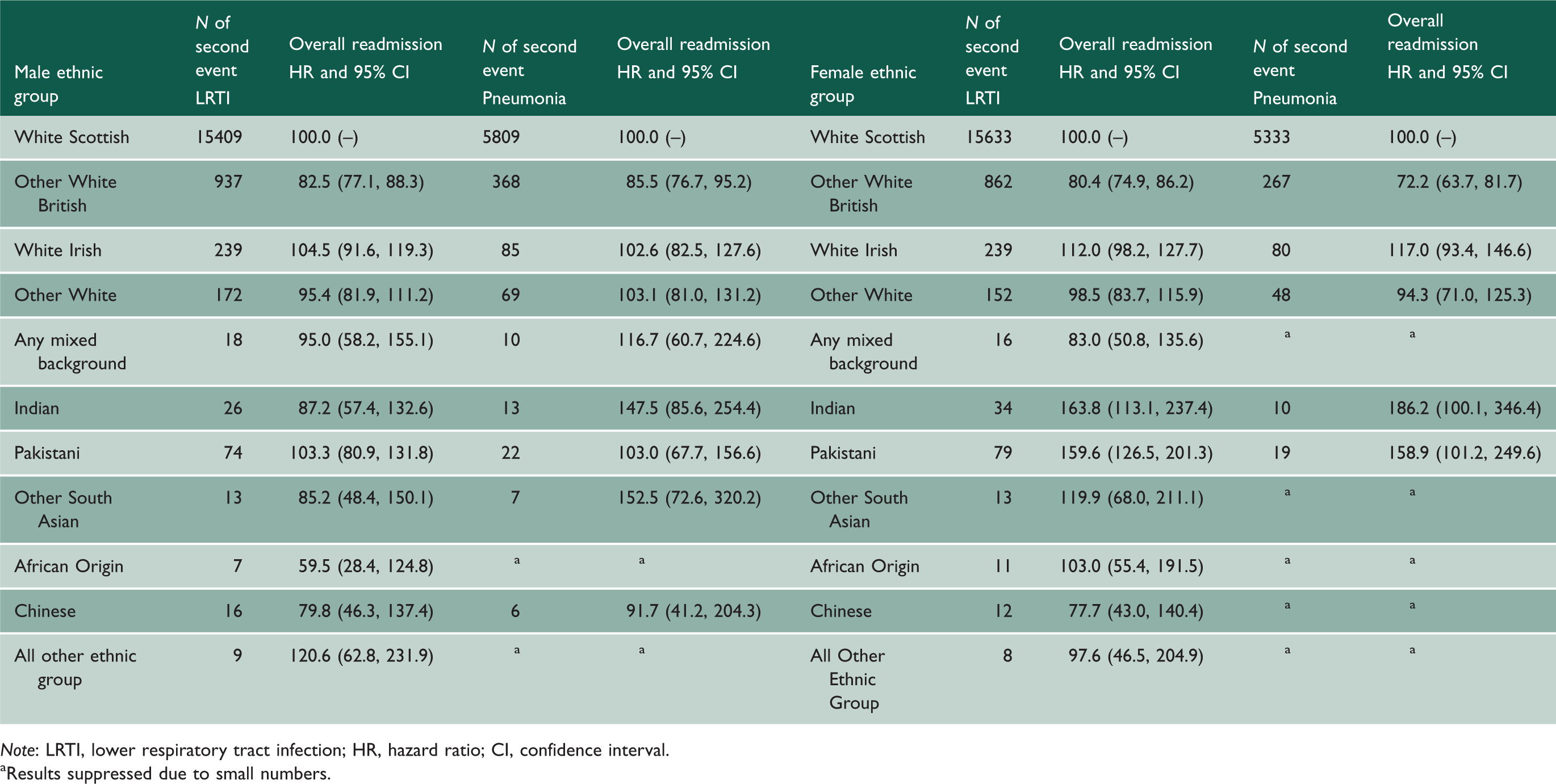
Note: LRTI, lower respiratory tract infection; HR, hazard ratio; CI, confidence interval.
aResults suppressed due to small numbers.
Pneumonia
Pneumonia hospitalisations and deaths for men.
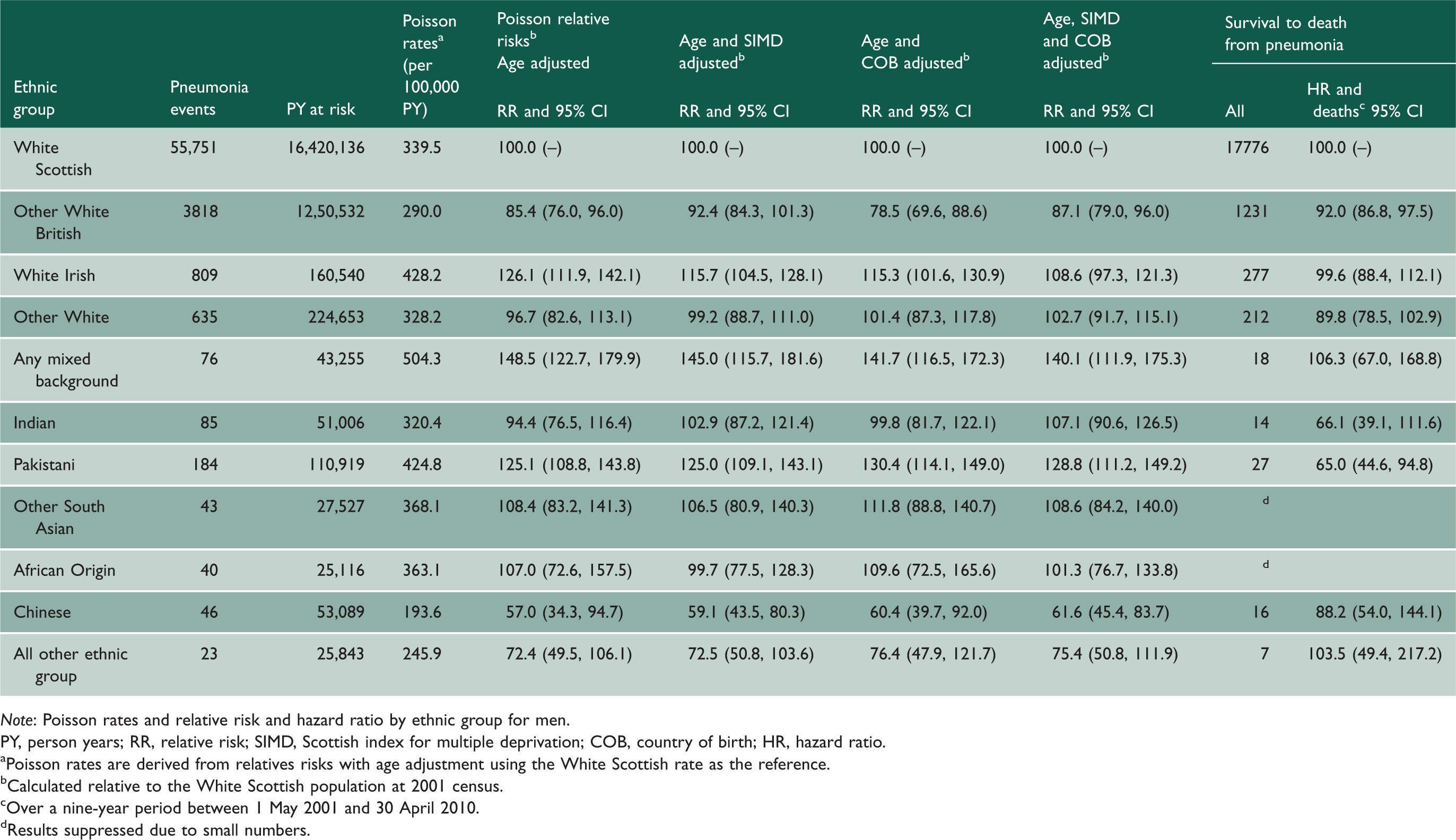
Note: Poisson rates and relative risk and hazard ratio by ethnic group for men.
PY, person years; RR, relative risk; SIMD, Scottish index for multiple deprivation; COB, country of birth; HR, hazard ratio.
aPoisson rates are derived from relatives risks with age adjustment using the White Scottish rate as the reference. bCalculated relative to the White Scottish population at 2001 census. cOver a nine-year period between 1 May 2001 and 30 April 2010. dResults suppressed due to small numbers.
Pneumonia hospitalisations and deaths for women.
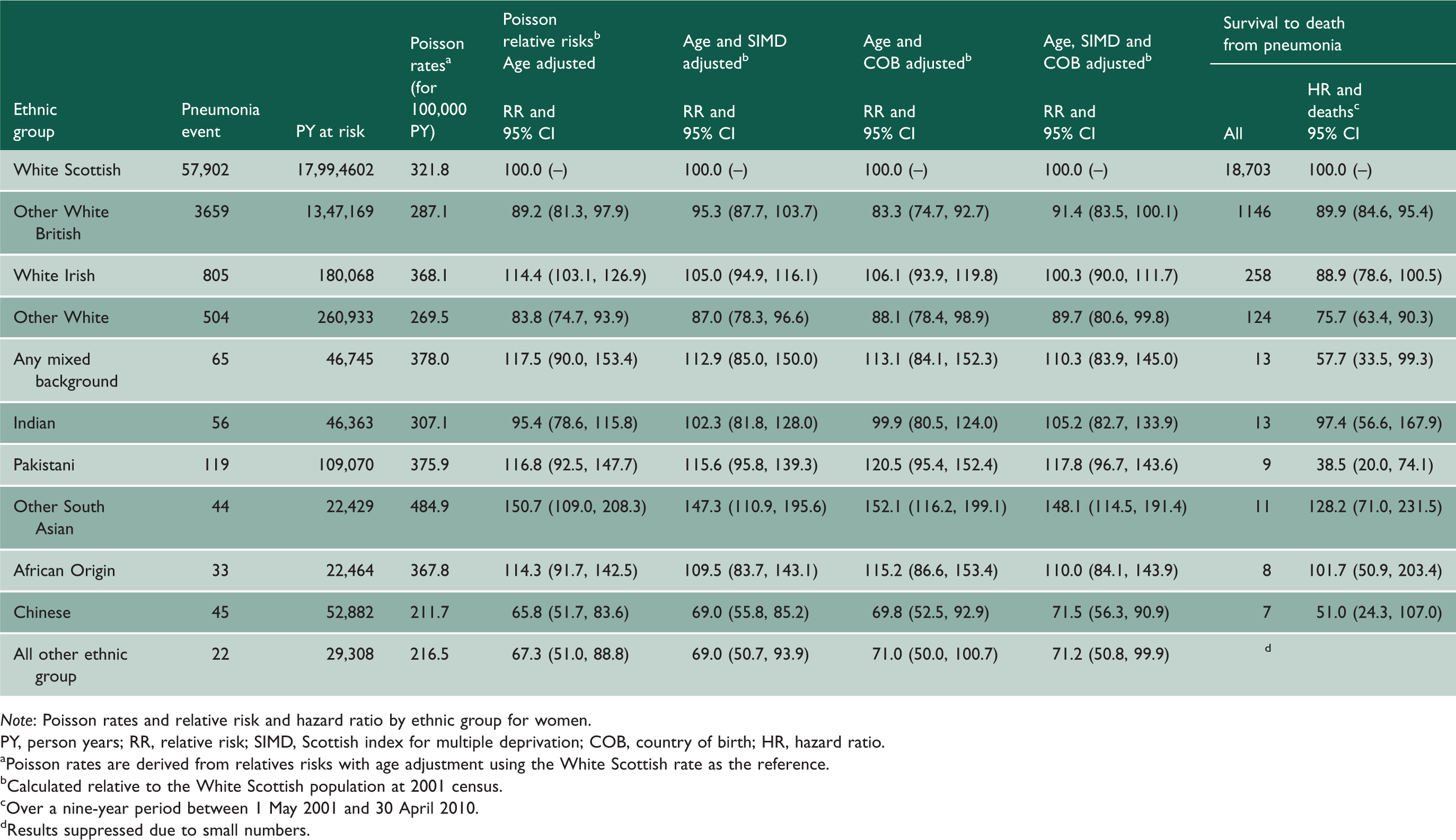
Note: Poisson rates and relative risk and hazard ratio by ethnic group for women.
PY, person years; RR, relative risk; SIMD, Scottish index for multiple deprivation; COB, country of birth; HR, hazard ratio.
aPoisson rates are derived from relatives risks with age adjustment using the White Scottish rate as the reference. bCalculated relative to the White Scottish population at 2001 census. cOver a nine-year period between 1 May 2001 and 30 April 2010. dResults suppressed due to small numbers.
Influenza
Influenza hospitalisation adjusted risk ratios were found to be higher in Pakistani men (235; 95% confidence interval 134, 412) than the reference group. This was the only significant group difference (in men and women) for influenza (Supplemental Table 1).
Discussion
Differences in the risks of hospital admission were found for lower respiratory tract infections including pneumonia and influenza, in particular with higher risks for Pakistani men and substantially lower risks in Chinese populations. Risks of readmission were higher for Indian and Pakistani women.
Comparison of findings with other published work
The literature on ethnicity and lower respiratory tract infections, particularly among European populations, is sparse – however, risks were found to be higher in indigenous Aboriginal children in Australia 10 and Native Americans in the US. 11 Comparatively higher rates of community-acquired pneumonia have been found among Black adults in the US 12 and among Maori in New Zealand. 13 For influenza, indigenous peoples also have high rates of disease and poorer outcomes. 14 The differences, however, in categorisation of race/ethnicity and system of healthcare in the US, Australia and New Zealand prevent meaningful comparisons with our data. In the UK, no difference in the rate of influenza between ethnic groups has been previously noted. However, a study by Nyland et al. set out to determine whether care pathway differences existed between non-White and White patients admitted with laboratory-confirmed pandemic influenza A (H1N1). They found that the non-White group was less likely to receive preadmission antibiotics. 15 However, there were no significant differences in delayed admission, severity at presentation for admission or likelihood of severe outcome.
Main strengths and limitations of this work
The strengths of Scottish Health and Ethnicity Linkage Study include the analysis at national level, the cohort design, the availability of ethnic group and sociodemographic data (including socioeconomic status) and the analyses of many ethnic groups. 23 We used Scottish Index of Multiple Deprivation because hospitalisation/death from respiratory diseases is commonest in older populations and Scottish Index of Multiple Deprivation data from the Census were available for all ages. Unlike Scottish Index of Multiple Deprivation, other alternative measures such as educational and economic status are only collected from 18 to 74 years of age. We used all diagnostic data on the hospitalisation and on mortality records (so-called multi-cause coding) and not just first hospital diagnosis and underlying cause of death. Both approaches have merits and limitations. Since we used the data primarily to compare ethnic groups, we think our approach is appropriate, especially as it maximises the number of events. Limitations include: incomplete linkage, few events in some groups (particularly for influenza) reflected in wide confidence intervals, lack of community and primary care data (where the majority of less severe lower respiratory tract infections are likely to present) and lack of linkable risk factor data, e.g. smoking (although a feasibility study to link primary care data to the Scottish Health and Ethnicity Linkage Study database is underway). There are other important missing data including key factors along the causal pathway of disease, e.g. social and genetic determinants, disease prevention, healthcare-seeking behaviour and healthcare access (e.g. higher risks could reflect an underestimated denominator or high levels of referral to hospital in some ethnic groups), potential differential treatment of people from different ethnic backgrounds by healthcare institutions (including related to sociocultural issues or difficulties with communication) and differences between use of alternative medicine and home care in different groups (including the care of people who are dying at home). Changing disease patterns (i.e. the 2009 H1N1 pandemic influenza outbreak) and specific co-morbidities such as diabetes, tuberculosis and immunosuppression, which may be high in specific ethnic groups and contribute to lower respiratory tract infection risk, were also missing. We did not have access to data to determine changing migration over time (although we had access to country of birth from the census); we were therefore unable to adjust for the length of residence in Scotland. This is likely to have an impact, as those living for longer periods in Scotland are likely to have markedly different health and socioeconomic status than more recent migrants who had being living in Scotland for a shorter period of time. Furthermore, lower risks could reflect unrecorded emigration whereby the numerator is underestimated and the denominator overestimated. As linkage was to the 2001 census, we were unable to link data to those born in Scotland after 2001. The number of children was therefore too small to allow a separate analysis. As causative lower respiratory tract infection and pneumonia organisms are different in adults and children (requiring different control measures), a stratified analysis by age should be a priority for future research. Bias may have been introduced as some groups with complex health needs, e.g. asylum seekers and the homeless, were under-represented in the 2001 census. Linkage rates were slightly lower among ethnic minorities than among the White Scottish population, increasing the risk of bias. However, there was no appreciable variation between groups in linkage rates. The 80% linkage target achieved for all ethnic groups was determined by the investigators to be both a realistic and yet valid and searching target.
Meaning of the study results: possible mechanisms and implications for clinicians and policy makers
We have shown substantial differences between ethnic groups, with low risks in Chinese and surprisingly high risks of hospitalisation (but better rates of survival) among Pakistani men. This finding of higher rates of a lower respiratory tract infection hospitalisation in Pakistani men is surprising. The reference White Scottish population, with a higher prevalence of smoking when compared with other ethnic groups, should be at a higher risk of respiratory diseases. 24
Vaccination, in particular with the pneumococcal polysaccharide and conjugate vaccines, haemophilus influenzae (Hib) vaccine and inactivated and live attenuated influenza vaccine, is a key preventative measure for reducing the burden of pneumonia. Although few data on specific vaccine uptake among different ethnic groups living in the UK exist, it is known that areas where more non-White groups live have lower uptake of pneumococcal polysaccharide vaccine vaccination (areas with population 99–100% White: 7.8% vs. areas with population <90% White: 4.2%). 25 Lower rates of pandemic H1N1 influenza vaccination have also been found among Blacks when compared to Whites in the US (13.8% vs. 20.4%). 26 The greater risk of hospital readmissions for Indian and Pakistani women following an lower respiratory tract infection episode also warrants further investigation. It should also be noted that Chinese origin populations had particularly low rates of lower respiratory tract infections; focusing on reasons for this phenomenon may identify potentially transferable lessons for other ethnic groups.
Conclusions and future research
Possible explanations for the disparities among ethnic groups – and in particular the Pakistani community – in hospitalisation and death from lower respiratory tract infections (including pneumonia and influenza) now need to be fully explored. Furthermore, it is important to investigate any variations in risk factors, such as vaccine uptake, smoking, presence of chronic respiratory conditions such as asthma and immunosuppression among different ethnic groups. However, as modifiable factors such as vaccination are likely to have an impact on the burden of disease and significant variations are known to exist, it is likely that strategies to increase vaccine uptake and improve chronic disease management among Pakistani and Other South Asian groups will reduce the burden of lower respiratory tract infections and pneumonia. Furthermore, future work should aim to replicate these analyses elsewhere in the UK and also continue monitoring any differences in lower respiratory tract infection and pneumonia rates and risk factors such as vaccination and chronic disease management between ethnic groups in Scotland.
Footnotes
Declarations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.