
Abstract
Summary
Objectives
Health system reforms in England are opening broad areas of clinical practice to new providers of care. As part of these reforms, new entrants – including private companies – have been allowed into the primary care market under ‘alternative provider of medical services’ contracting mechanisms since 2004. The characteristics and performance of general practices working under new alternative provider contracts are not well described. We sought to compare the quality of care provided by new entrant providers to that provided by the traditional model of general practice.
Design
Open cohort study of English general practices. We used linear regression in cross-sectional and time series analyses, adjusting for practice and population characteristics, to compare quality in practices using alternative provider contracts to traditional practices. We created regression models using practice fixed effects to estimate the impact of practices changing to the new contract type.
Setting
The English National Health Service.
Participants
All general practices open from 2008/2009 to 2012/2013.
Main outcome measures
Seventeen established quality indicators – covering clinical effectiveness, efficiency, access and patient experience.
Results
In total, 4.1% (347 of 8300) of general practices in England were run by alternative contract providers. These practices tended to be smaller, and serve younger, more diverse and more deprived populations than traditional providers. Practices run by alternative providers performed worse than traditional providers on 15 of 17 indicators after adjusting for practice and population characteristics (p < 0.01 for all). Switching to a new alternative provider contract did not result in improved performance.
Conclusions
The introduction of new alternative providers to deliver primary care services in England has not led to improvements in quality and may have resulted in worse care. Regulators should ensure that new entrants to clinical provider markets are performing to adequate standards and at least as well as traditional providers.
Introduction
Health systems with a strong focus on delivery through primary care are more effective, equitable and efficient. 1 However, like other parts of the health system, primary care providers throughout the world need to show that they can provide high-quality care and efficiently use the resources allocated to them. Ongoing debate about how best to achieve efficient and high-quality primary care has led policy-makers to encourage more diverse or plural models of primary care delivery in some settings. This has included the entry of new commercial providers into primary care systems. 2
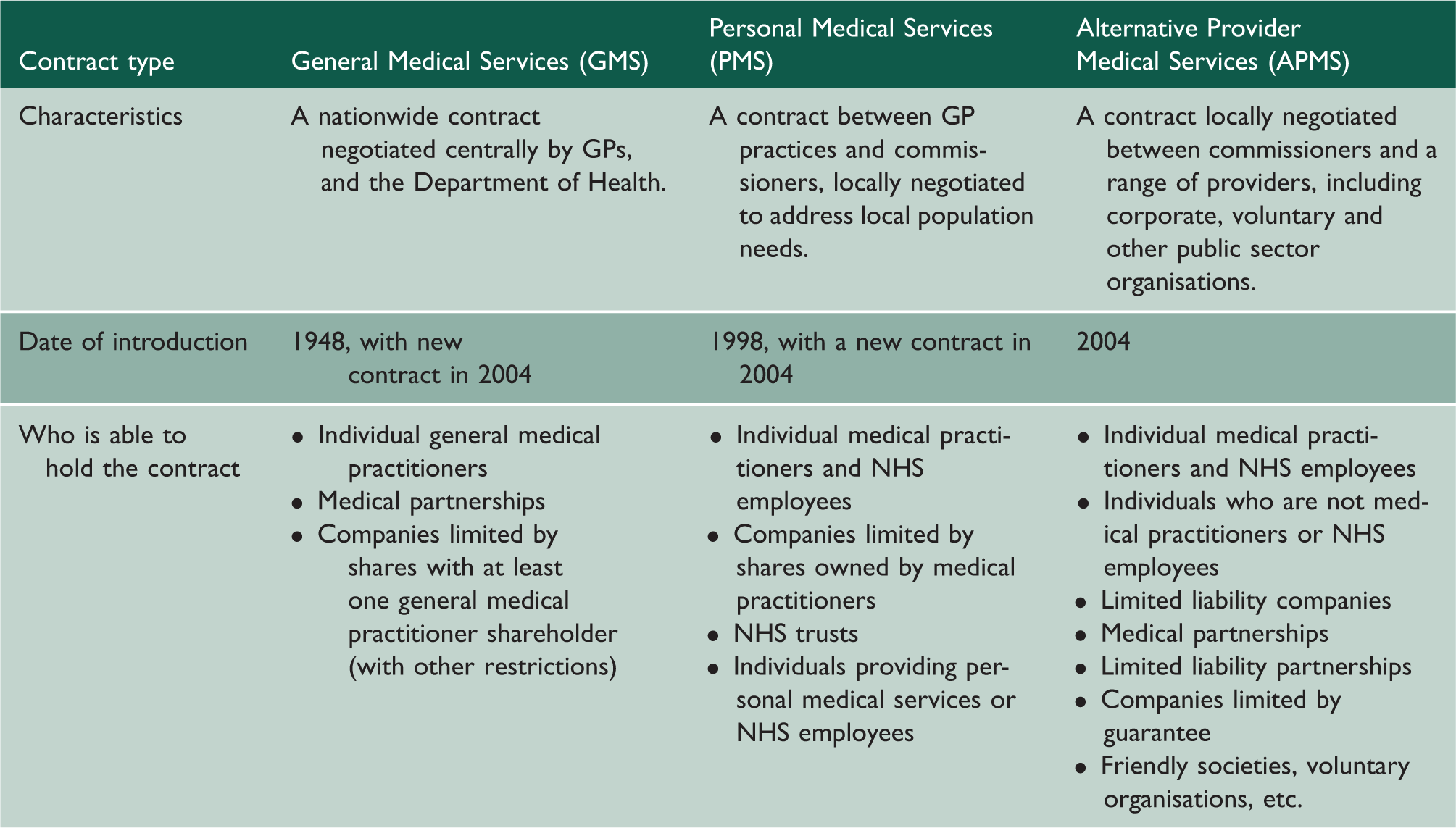
Increasing the role of non-traditional providers, including those from the private sector, in health-care delivery has been a key policy theme in England over the past decade. For the first five decades of the National Health Service (NHS), primary care was provided by general practitioners as independent businesses, contracted to the Department of Health. Practices would typically comprise a single or a small group of practitioners delivering care from common premises through a single core contract. Under a Labour government in 2004, corporate or voluntary organisations were allowed to provide general practice services for the first time through a competitive tendering process.
Main contract types for provision of NHS Primary Care Services in England.
Method
The study used an open cohort of all general practices operating in England between 2008/2009 and 2012/2013. We compared performance of general practices by contract type within each study year and examined the effect on quality of a practice being Alternative Provider of Medical Services over time. We compared the performance of Alternative Provider of Medical Services practices to those holding either GMS or PMS contracts combined, as these two groups represent the traditional model of GP-owned and -led general practice.
Selecting measures of quality
Selection of quality indicators was guided by the Institute of Medicine framework, 4 which divides quality into six components: clinical effectiveness; safety; patient experience; timeliness/access; efficiency; and equity. We selected a broad spectrum of established and commonly reported indicators, some general and some specific to conditions usually managed in primary care, where there is known variation in performance.
The measures chosen were percentage of total Quality and Outcomes Framework (QOF) points achieved, percentage of clinical QOF points achieved, percentage of hypertensive patients with controlled blood pressure (less than 150/90 mmHg), percentage of diabetes patients with controlled HbA1C (less than 7.5% in 2008/2009, less than 8% in other years), percentage of eligible patients receiving cervical screening, admission rate for ambulatory care sensitive conditions (ACSC) per 1000 people, 5 percentage of low-cost statin prescribing (not measured in 2012/2013), tonsillectomy rate per 1000 people, percentage satisfied with opening hours at their practice, percentage able to get an appointment at their practice (within 48 h in 2008/2009 to 2010/2011, any appointment in 2011/2012 and 2012/2013), percentage able to see their preferred doctor, percentage of people who would recommend their practice to someone moving to the area (not measured in 2008/2009) and percentage satisfied with their general practice overall.
The QOF is the NHS's pay-for-performance framework in primary care. It provides financial incentives for achievement of quality indicators across a variety of clinical and organisational areas, with a focus on chronic disease management, and applies to all contract types. Specific clinical indicators also allow patients to be ‘exception reported’, the process by which a patient may be omitted from a pay-for-performance report. While there may be sound clinical reasons why this may occur, exception reporting could be inappropriately used to ‘game’ the system. 6 For the three specific clinical indicators used in this study, we have reported the raw levels of achievement without allowing exceptions and the exception reporting rate. No performance measures were included for safety or equity as it was not possible to identify any that had sufficient standardisation and availability at practice level.
Data sources
We obtained data on contract status for all general practices in England between 2008/2009 and 2012/2013 from the Health and Social Care Information Centre. Contract status data from previous years were not systematically collected at a national level, and the number of Alternative Provider of Medical Services practices was very small before 2008/2009. 7 Data on ACSC admission rates, tonsillectomy rates and use of low-cost statins were taken from NHS Comparators. 8 Measures of patient experience and access were taken from the national General Practice Patient Survey. 9 This is a mail-based survey sent to 2.7 million patients in 2011/2012 with almost one million responses (a response rate of 36%). 10 All other quality measures were obtained via the QOF system from the Health and Social Care Information Centre, and some were subject to minor changes between study years. 11 Population and practice characteristic data were the percentage of practice population aged over 65 years, the percentage male, the index of multiple deprivation (IMD) 2010 score (an area-based measure of socioeconomic status where a higher score indicates a more deprived population) for the practice, 12 the proportion of the practice population who reported their ethnicity as ‘white’, the number of full-time equivalent GPs per 1000 people served and the practice list size. These characteristics were obtained from the Health and Social Care Information Centre. 13
Exclusion criteria
We excluded practices with fewer than 1000 patients (n = 195) from the study, as these often provide specialised services (for example, a sexual health service) or services to specific populations (e.g. homeless patients). The total number of practices included in our study was 8300 (97.7% of the total number of 8495 practices in England in at least one year during the study period). The small number of practices using the Primary Care Trust Medical Services contract were also excluded from the analysis in years they had this contract (413 of 40,262 or 1% of practice years) – as Primary Care Trusts were abolished in 2013. Complete data on practice characteristics were missing for 191 practices. These practices were excluded from adjusted analyses.
Data analysis
We tested for differences in population and practice characteristics by contract type for the year 2012/2013 using t-tests. To examine within-year differences in practice quality by contract type, we built simple unadjusted ordinary least square regression models for each outcome variable in each year of the study period.
To measure the adjusted performance of Alternative Provider of Medical Services practices over time, we built ordinary least square time series regression models that used each of the primary care metrics as outcome variables. 14 The treatment variable was whether the practice was Alternative Provider of Medical Services in that year. Other practice level variables included in models were percentage over 65 years, percentage male, percentage white ethnicity, deprivation score, the number of GPs per 1000 people registered, list size and time (expressed as year). Performance was assessed in the year the practice was Alternative Provider of Medical Services, and the year after, to provide sufficient time for improvement. Finally, we built a time series regression model that included fixed effects for each individual practice, designed to examine the effect of changing to or from an Alternative Provider of Medical Services contract for a given practice. For this fixed effect analysis, we only included practices that were present in all five years of the study period to exclude the effect of new entrants. For regression analyses, outcome variables were transformed into natural logs. Analysis was conducted using Stata 12 software.
Sensitivity analyses
We performed sensitivity analyses to test the robustness of findings under different assumptions. These include analyses with all practices (not excluding those less than 1000 patients) and analyses without adjustment. In addition, we compared Alternative Provider of Medical Services practices to GMS and PMS practices separately for all of the models (rather than PMS and GMS combined). We also performed subgroup analyses examining the performance of Alternative Provider of Medical Services practices that were owned by limited companies only compared to traditional practices.
Results
In total, 4.1% of practices (347/8300) held an Alternative Provider of Medical Services contract in at least one year during the study period; 1.6% of practices were Alternative Provider of Medical Services in 2008/2009 (129/8064), 2.6% in 2009/2010 (216/8186), 2.7% in 2010/2011 (219/8182), 2.8% in 2011/2012 (222/7991) and 3.1% in 2012/2013 (242/7900). Fifty-three percent of these practices (185/347) were newly formed in the study period, while 47% had existed before. Thirty-nine percent (137/347) switched to Alternative Provider of Medical Services from another contract type in the study period. Thirteen percent (44/347) were existing practices that remained Alternative Provider of Medical Services in every year. Fifteen percent (52/347) switched from being Alternative Provider of Medical Services to another contract and 10% (33/347) closed during the study period.
Population and practice characteristics by contract type in 2012/2013.
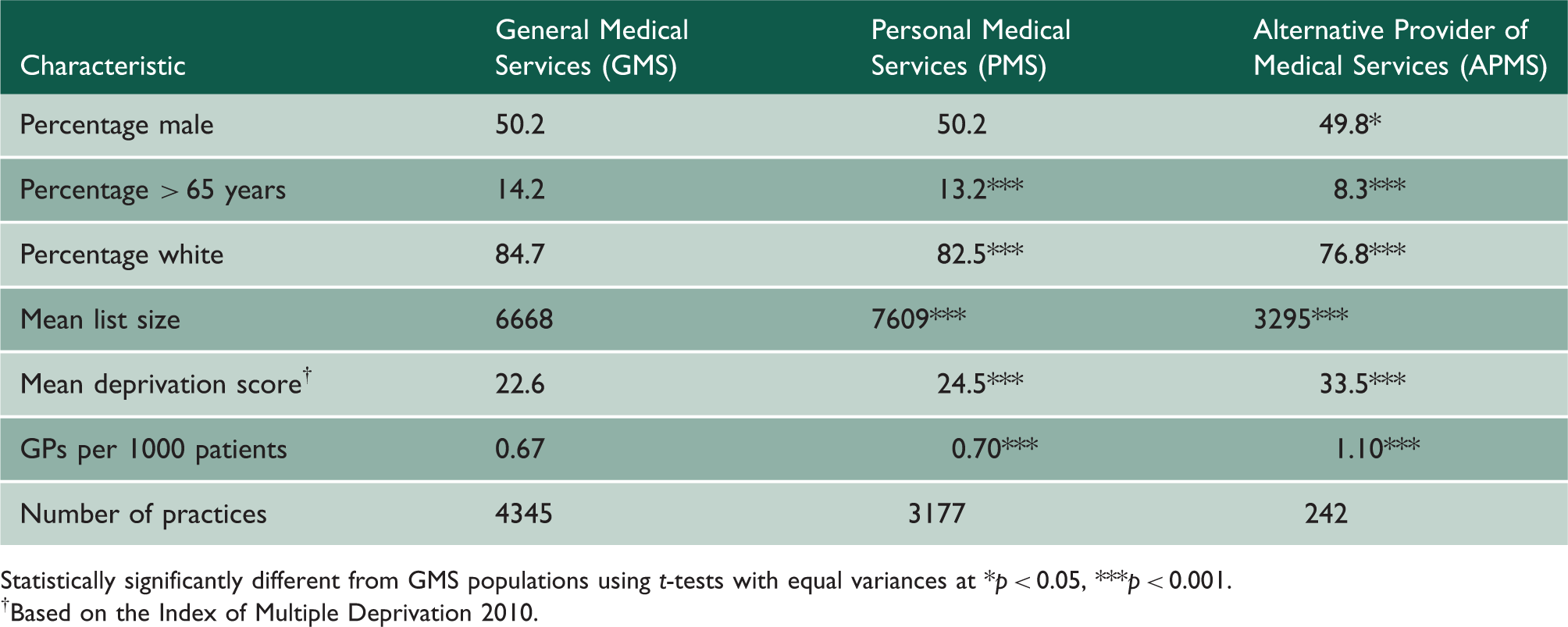
Statistically significantly different from GMS populations using t-tests with equal variances at *p < 0.05, ***p < 0.001.
†Based on the Index of Multiple Deprivation 2010.
Within-year comparisons of practice performance by contract status, 2008/2009 to 2012/2013.

p < 0.05,
p < 0.01,
p < 0.001
Association between practice contract status and primary care performance; time series regression.

Adjusted for age, gender, ethnic and deprivation profile of patients and for practice size and staffing.
Association between practice contract status and primary care performance; time series regression with practice fixed effects.

The results of the sensitivity analyses were all similar to the main results presented here (Technical Appendix e-Tables 3–11).
Discussion
This study presents the first national evaluation of the performance of new alternative providers of primary care services in England. The results suggest that alternative providers have not been widely contracted to deliver primary care services, making up only 4% of practices since 2004. Alternative providers of primary care services in England serve a different population – younger, more diverse and more deprived – compared to practices that use the traditional contracting arrangements. Practices run by alternative providers supplied consistently worse quality of care than traditional practices – across a broad range of indicators.
While some of this difference may be due to the different populations they serve, our models – which adjust for population and practice features and for underlying trends – found that Alternative Provider of Medical Services practices continued to do worse than would be expected compared to the national sample of general practices. The data also reveal that while many Alternative Provider of Medical Services practices began as new entities within the period studied, a minority had previously been run with a different contract. When we used a model designed to look for change within individual practices when they switched to Alternative Provider of Medical Services, we found no evidence that practices improved. Taken together, these findings suggest that allowing new alternative providers into the primary care market in England has not led to better care for patients – and may have even resulted in worse care.
Some of the patterns of poor performance are concerning and merit further examination. For instance, Alternative Provider of Medical Services providers, while meeting patients' desires for longer opening hours have higher levels of exclusions from a national pay-for-performance programme and higher referrals of ambulatory sensitive conditions to secondary care. These latter two findings raise the possibility that Alternative Provider of Medical Services providers may be acting to maximise profit from pay-for-performance systems and shifting costs from primary care to secondary care.
The strengths of our study are that it involves the first use of a national dataset to examine the performance on new entrant providers of primary care in England. Additionally, it uses a broad range of comparable performance measures which are collected according to rigorous standards and is able to observe trends over a five-year time period. Results from our sensitivity analyses were similar to our main analyses, suggesting our findings are robust. However, our study has a number of limitations that mean that our findings should be interpreted cautiously. As with all observational studies, there remains a risk of residual confounding – although our models were adjusted using available data on practice and population characteristics. Practices that were put out to tender as Alternative Provider of Medical Services may have been more likely to have been practices with a history of poor performance, perhaps as a result of bad prior management. The number of Alternative Provider of Medical Services practices, at 4.1% of the total, is only a small group to compare against the traditional model. Additionally, the limited number of practices switching to Alternative Provider of Medical Services contracts – and use of a statistically conservative fixed effect model – may have resulted in a model underpowered to detect the effect of change within practices of changing contract. We are aware that within the practices using the Alternative Provider of Medical Services contract, there is variation in provider type. Some are run by entrepreneurial GP groups, others by multinational corporations. While we found the subgroup of Alternative Provider of Medical Services companies run by limited companies were also providing worse quality care, further research is needed to assess whether the nature of the provider business model affects performance. There are also limitations in the GP patient survey and QOF as performance metrics. For many of the QOF measures, there is little variation and consequently little ability to differentiate performance. 15 The response rate of the GP patient survey means there is a risk of selection bias.
The findings of this study are consistent with earlier work. A study in 2006 examining only 10 practices using new contacting mechanisms found that these practices performed less well than peers. 16 Heins et al. used freedom of information to ascertain the extent of roll out of the new contract types in 2009, but only achieved a limited response from local commissioning organisations. They concluded that it was not possible to assess the quality and value for money of the new contracting arrangements and that further evaluation was needed. 7 They did find half of all Alternative Provider of Medical Services contracts were awarded to nationwide or multinational commercial companies.
These findings are relevant to the debate around the increasing provision of service by non-traditional NHS providers, including the private sector. There has been an increased emphasis on plurality of providers, competition and patient choice as mechanisms to the improve performance in the English NHS over the last decade. 17 The Health and Social Care Act in April 2013 is seen by many as a step change towards embedding competition within the NHS, 18 substantially increasing the scope for non-traditional NHS providers of care to enter the NHS market in England under an ‘any qualified provider’ policy. 19 The requirement for many services to be put out to competitive tender by Clinical Commissioning Groups in England has raised questions about how increasing diversity in healthcare provision will affect quality of care and cost-effectiveness. 20 Proponents of the Act claim new alternative providers will be able to innovate, stimulate competition and improve quality.21,22 Opponents have suggested that there is a risk that they will hinder integrated care, select the easiest services and patients and focus on maximising profit ahead of performance.23,24 New tendering policies may make Alternative Provider of Medical Services contracts – and similar arrangements in secondary care – more common in the future.
Information on the effect of competition on the quality, efficiency and responsiveness of health systems is limited and equivocal.25,26 Two recent studies have suggested that quality improved more quickly within hospitals operating in more competitive markets in England.27,28 However, the robustness of these findings and their implications for healthcare policy has been contested. 29 While debate has focused on the effect on quality of healthcare providers working in more competitive environments, this study looks at the effect of competition from another, simpler perspective – how well do the new entrants perform compared to the traditional providers. Although available data preclude drawing definitive conclusions for health policy in England, our findings provide little support for the hypothesis that increasing plurality of provision has increased quality of care. Our findings highlight the need for careful and independent evaluation of the current trend of increasing competitive tendering and encouraging the entry of new providers for a wide range of clinical NHS services.
In conclusion, given the current direction of healthcare policy in England, this analysis provides timely information about the potential impact of increasing provision of healthcare by the voluntary and private sectors in the NHS. These findings suggest that Alternative Provider of Medical Services practices serve a different population, perform worse on average, and when practices switch to become Alternative Provider of Medical Services, they do not improve their performance. As general practice in England gradually evolves from a ‘cottage industry’ into something that may look more corporate, it is important that the impact of these changes on quality, expenditure and utilisation is carefully evaluated. Similar considerations should apply in other countries considering a greater role for alternative and commercial providers in healthcare delivery.