
Abstract
Objective
We sought to determine the primary care-based prevalence of moderate-to-severe atopic eczema/dermatitis in children and to estimate what proportion had co-morbid aero-allergy and/or food allergy that was contributing to their atopic eczema/dermatitis.
Design
Multi-centre, cross-sectional study.
Participants
Infants, children and young people aged between 0–17 years.
Setting
Primary Care.
Methods
General practice electronic health records were interrogated to identify children (0–17 years) with current moderate-to-severe atopic eczema/dermatitis. Eligible children were assessed by an allergy specialist nurse, this involving a detailed allergy history, examination and, if appropriate, measurement of total IgE and specific IgE to relevant aero-allergens and/or food allergens.
Main outcome measures
Prevalence of atopic eczema, moderate to severe atopic eczema, IgE-mediated atopic eczema.
Results
We recruited eight practices, which together enrolled 16,877 children. Of these, 4331 (25.7%; 95% CI 25.0, 26.3) children had a recorded diagnosis of atopic eczema/dermatitis and 1316 (7.8%; 95% CI 7.4, 8.2) had treatment indicative of current moderate-to-severe atopic eczema/dermatitis. We recruited 159 children for clinical assessment, and complete data were available for 157. The clinical assessment revealed that 130/157 (82.8%) had no indication of IgE-mediated allergy contributing to their atopic eczema/dermatitis; the remaining 27/157 (17.2%; 95% CI 12.1, 23.9) were on clinical assessment considered to possibly have underlying IgE-mediated disease. Specific IgE tests were positive in 14/27 (51.9%; 95% CI 34.0, 69.3) children. Of the 14 children who tested positive, six (42.9%; 95% CI 21.4, 67.4) were positive to food allergens and six (42.9%; 95% CI 21.4, 67.4) to aero-allergens; the remaining two (14.3%; 95% CI 4.0, 40.0) were positive to both food and aero-allergens.
Conclusions
Although atopic eczema/dermatitis is a very common diagnosis in children in primary care, most appear to be relatively mild and/or transient. Only a small proportion of children had evidence of ongoing underlying IgE-mediated atopic eczema/dermatitis.
Introduction
The prevalence of allergic diseases has increased very considerably over recent decades in the Western world to the extent that recent estimates indicate 50% of children will be affected by an allergic condition at some point in their lifetime. 1 In the UK, the majority of these children will be managed predominantly within a primary care setting, with only those with particularly severe and/or disabling disease being referred to specialist services. 2 Access to allergists is known to be poor in many parts of the UK. 3
Atopic eczema/dermatitis is one of the most common manifestations of allergy in early life. Although mild and transient in many children, in some individuals the disease follows a more aggressive course; the atopic eczema/dermatitis is in such children typically early in onset, difficult to manage with simple advice and emollients, and more persistent than the atopic eczema/dermatitis experienced by the majority of children, often heralding the onset of other allergic disorders. 4 Filaggrin gene defects are an important precursor, which may increase the risk of allergic sensitisation.5,6 It is this group of children with moderate-to-severe atopic eczema/dermatitis in whom underlying allergy to foods (e.g. cow’s milk and hen’s eggs) and/or inhalant aero-allergens (e.g. house dust mite, pollens and pets) may be particularly important and who may therefore benefit from appropriate allergen avoidance advice and allergen-specific therapies in order to improve outcomes and reduce the risk of disease progression. 7
A major evidence-gap in knowing how best to deliver the systematic assessment of those with more troublesome atopic eczema/dermatitis advocated by national guidelines is knowing what proportion of children seen in community settings with atopic eczema/dermatitis are likely to have underlying allergies. 8 The current very high estimates, which indicate that approximately one-third of all children with moderate-to-severe atopic eczema/dermatitis have an underlying allergic trigger, are derived from specialist care settings raising the possibility that selection biases are likely to substantially inflate prevalence estimates.9–11 We, therefore, sought to estimate the prevalence of moderate-to-severe atopic eczema/dermatitis in children in primary care and estimate what proportion of these children had underlying aero- and/or food allergy.
Methods
Overview of methods
We undertook a multi-centre, cross-sectional study in general practice which involved the interrogation of electronic health records and detailed clinical assessment of children (aged 0–17 years) with likely moderate-to-severe atopic eczema/dermatitis. This involved taking a detailed clinical history, physical examination and, if appropriate, specific IgE testing.
Ethical considerations
This work was undertaken with research ethics committee approval from South East Scotland Research Ethics Committee 1, and research management approvals were obtained from participating practices. Consent was obtained from all parents of participating children and accompanying assent of young people who the research nurse considered able to comprehend the nature of the study; this decision was made through discussion with parents of participating children.
Recruitment of practices
We wrote to general practices inviting them to participate in this study, and this was then followed up with a phone call and site visit to those who expressed an interest in participating. Practices were offered a modest honorarium (£250) to support their involvement in this study.
Recruitment of patients
Children aged ≤17 years with a clinician-recorded diagnosis of atopic eczema/dermatitis were initially identified through interrogation of GP records by practice staff using searches based on a sensitive set of READ codes. We then identified those with evidence indicative of active, moderate-to-severe atopic eczema/dermatitis; this being defined as those requiring topical corticosteroid use and/or immune-modulatory treatments in the preceding 12-month period. Those who were: aged ≥18 years; had atopic eczema/dermatitis which was no longer active or had mild atopic eczema/dermatitis controlled with emollients; unable to give informed parental/child consent/assent; or not willing for child/young person to have a blood test (if indicated) were ineligible for inclusion.
The parents of potentially eligible patients were sent a letter from their GP inviting them to participate in the study and an accompanying study information sheet and consent/assent form(s). Patients who confirmed that they met the eligibility criteria and were interested in participating were then seen by a trained allergy nurse in their local practice.
Patient assessment
A detailed allergy/clinical history and examination were undertaken in all recruited children by the study nurse; the findings being documented onto a structured study pro-forma (see Appendix 1). If the clinical assessment was suggestive of underlying IgE-mediated allergy to aero-allergens and/or foods contributing to the atopic eczema/dermatitis, then appropriate in vitro specific IgE testing (immunoCAP) was undertaken to the suspected allergens together with a measure of total IgE to aid interpretation. All samples were analysed by The Doctors Laboratory, London, UK (www.tdlpathology.com/). The results of any blood tests undertaken were subsequently communicated to the research team, the families of participating children and their GPs.
If the clinical picture was suggestive of non-IgE-mediated food allergy, then this was recorded and communicated to participating families and GPs, but no further investigations were undertaken.
If the clinical picture was not indicative of allergy-triggered atopic eczema/dermatitis, then this was communicated to the parent/patient and also to their GP.
Data handling and analysis
Data were entered into an Excel spreadsheet and then transferred to SPSS, and simple count and descriptive analyses were undertaken to provide prevalence estimates of the percentages and 95% confidence intervals (CIs) of children with moderate-to-severe atopic eczema/dermatitis, and the proportion of these children with evidence of IgE-mediated allergy to foods and/or aero-allergens.
Sample size considerations
No formal sample size calculations were undertaken for this prevalence study. We however a priori aimed to recruit 7–10 group general practices with a combined list size of 75,000–100,000 patients, as we estimated that this would give us the numbers needed to have reasonable precision in our prevalence estimates.
Results
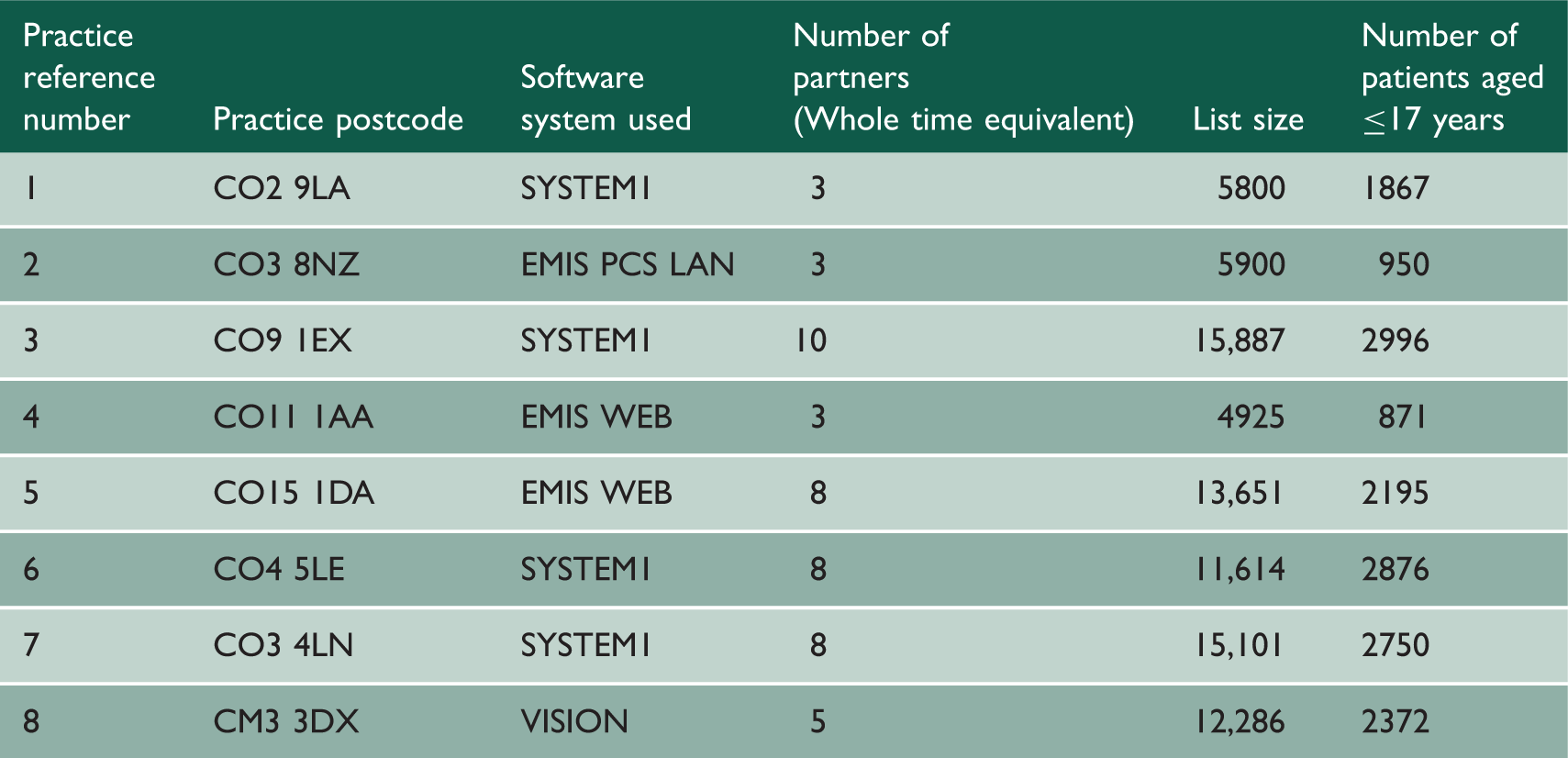
Characteristics of recruited practices.
Prevalence of atopic eczema/dermatitis and current moderate-to-severe atopic eczema/dermatitis
There were 16,877 children aged ≤17 years registered in the participating practices. Of these, 4331 (25.7%; 95% CI 25.0, 26.3) children had a recorded diagnosis of atopic eczema/dermatitis and 1316 (7.8%; 95% CI 7.4, 8.2) had treatment indicative of current moderate-to-severe atopic eczema/dermatitis, respectively.
Prevalence of underlying aero-allergy and/or food allergy triggered current moderate-to-severe atopic eczema/dermatitis
We recruited 159 of these children for clinical assessment, and complete data were available for 157 (see Figure 1 and Table 2). The clinical assessment revealed that 130/157 (82.8%) had no indication of IgE-mediated allergy contributing to their atopic eczema/dermatitis; the remaining 27/157 (17.2%, 95% CI 12.1, 23.9) were clinically assessed as having underlying IgE-mediated atopic eczema/dermatitis and appropriate tests were ordered to investigate this further.
Flow diagram for identifying patients with current potential moderate-to-severe atopic eczema/dermatitis. Patient blood test results.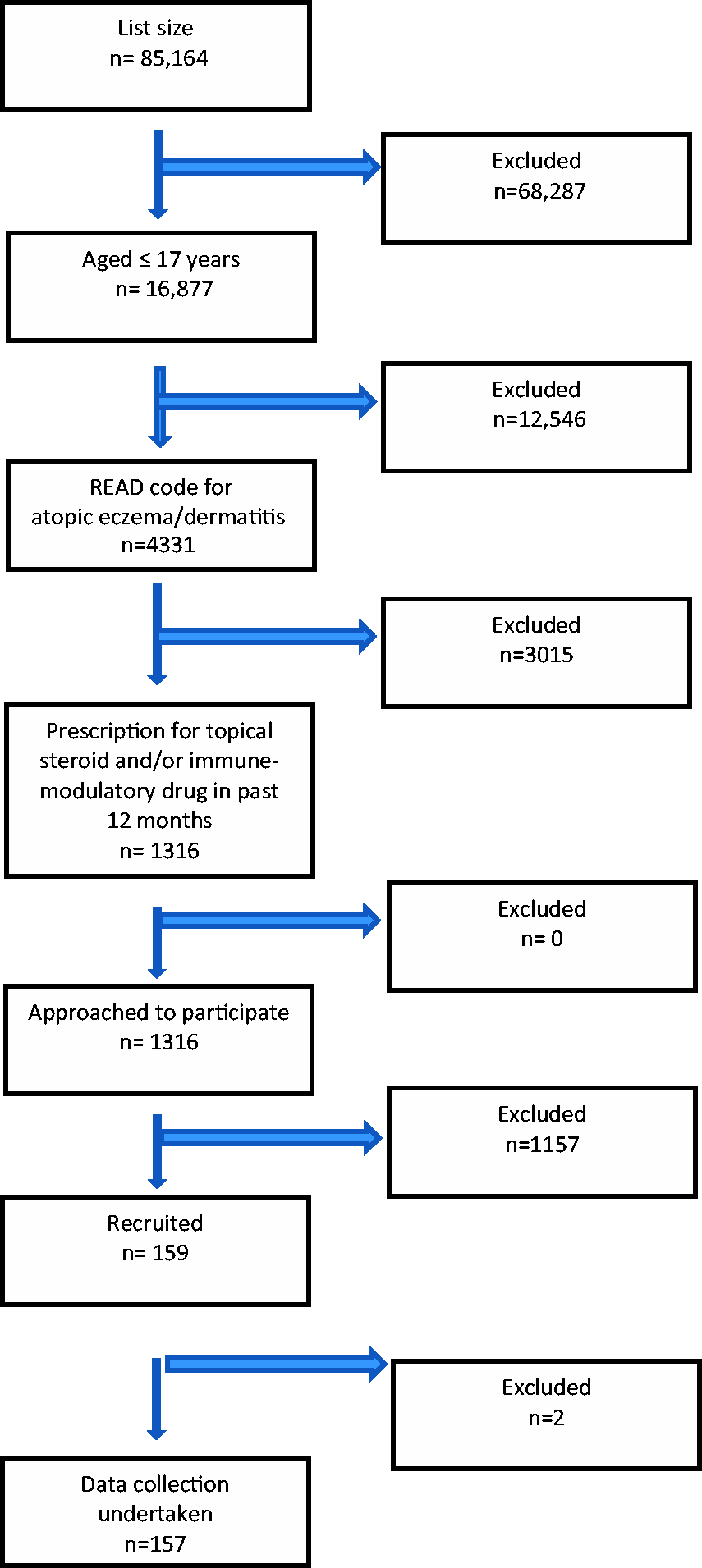
In the 27 children who had allergy testing undertaken, a total of 82 blood tests were ordered (i.e. 27 total IgE and 55 specific IgE tests), this equating to a mean of three tests per child. Of the specific IgE tests, 19 (34.5%) were performed for food allergens and 36 (65.5%) for aero-allergens.
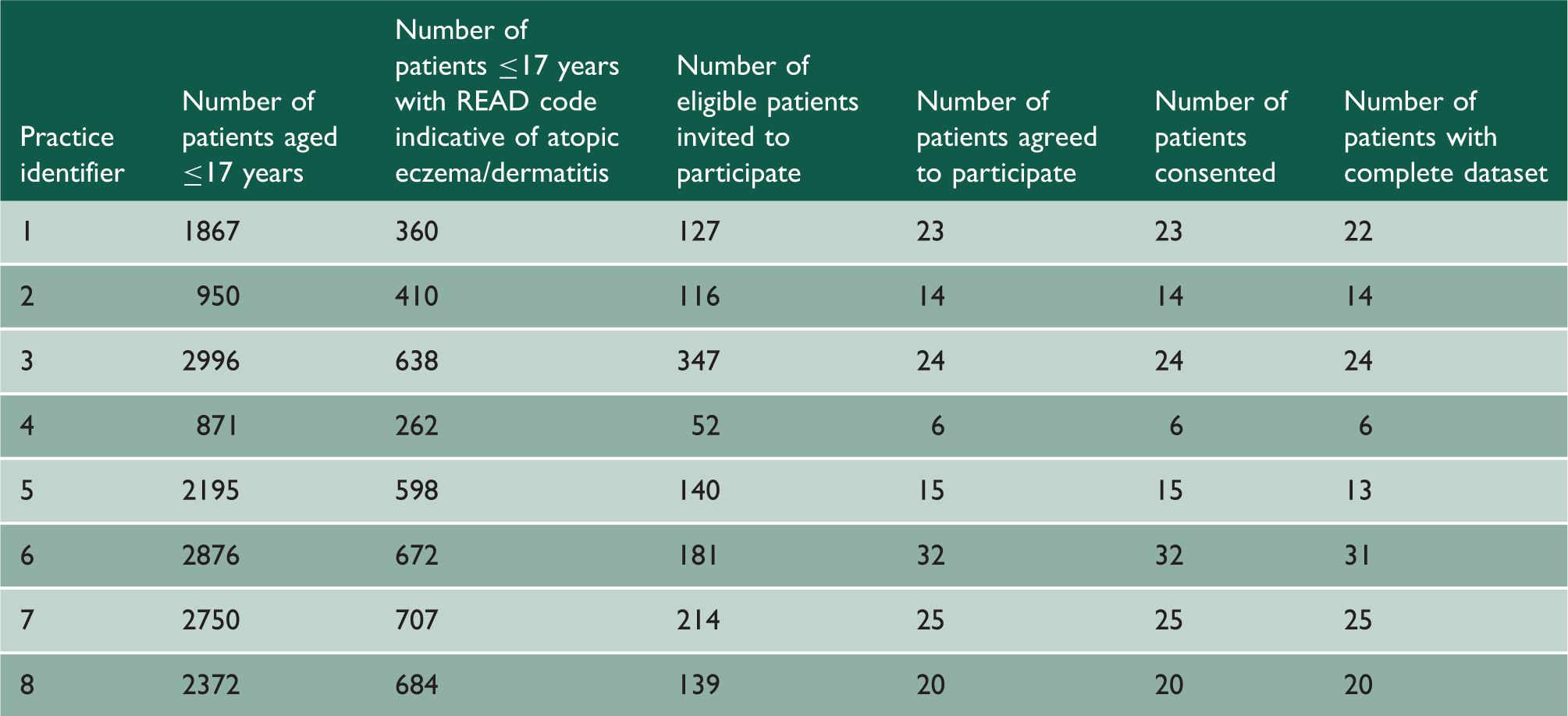
Patient recruitment log.

Discussion
Statement of principal findings
Based on a detailed clinical assessment, allergy was considered a contributory factor in approximately 20% of children with current moderate-to-severe atopic eczema/dermatitis and approximately half of these children tested positive to food and/or aero-allergens.
Strengths and limitations
This is one of the first studies undertaken to estimate the prevalence of underlying aero- and/or food allergy in children with atopic eczema/dermatitis in a primary care setting, where the majority of UK children with atopic eczema/dermatitis is seen and managed. We achieved our target recruitment figures for both practices and overall registered practice list size. Other key strengths include: that we had good precision in our estimates of atopic eczema/dermatitis, those with moderate-to-severe disease and the proportions of those with underlying IgE-mediated allergy; the combination of interrogating electronic health records and supplementing this with a detailed clinical assessment in children with suspected underlying allergy. We then sought to confirm this clinical suspicion with formal specific IgE testing to a range of potential candidate allergens. Blood tests were performed rather than skin prick testing as the former is in general more sensitive and the latter requires specialist training and resources that are not typically available in a GP surgery.12–14 Total IgE was measured in order to have a baseline to compare against as many allergic individuals will have greatly elevated levels making it difficult to interpret results accurately. 13
The study population was diverse covering the North Essex region, and all GP practices in the region were invited to participate. However, given the relatively low rate of recruitment of practices and patients, care needs to be taken in interpreting the findings from this study. Although we employed a sensitive search strategy, which should have enabled us to identify the overwhelming majority of children with atopic eczema/dermatitis, there is always the possibility that some cases may have been misdiagnosed and miscoded by the GP and may, therefore, not have been detected. Given that atopic eczema/dermatitis is a very commonly seen condition in primary care, we consider it unlikely that this had a major bearing on the results. Non-IgE food allergy was not formally investigated in this study, but we identified at least 14 children who on clinical assessment were thought to have possible non-IgE-mediated food allergy contributing to their atopic eczema/dermatitis. Further investigation of these children using formal challenge testing was beyond the scope of this particular study, but this is clearly an area in which future research is needed.
Interpretation in the context of wider literature
Our estimates of the prevalence of moderate-to-severe atopic eczema/dermatitis and underlying allergic disease were substantially lower than suggested by the previous literature on this subject. Prior estimates have, however, been derived predominantly from academic hospital-based specialist dermatology/allergy clinic settings and these are, therefore, unlikely to be representative of more population-based settings.9–11 The findings from the present study are, however, likely to be much more representative of the true picture in the general population. This suggests, therefore, that the vast majority of children with atopic eczema/dermatitis seen in general practice settings has relatively mild disease in which allergy is unlikely to be a major contributory factor. Allergy should, however, be more routinely considered by GPs and their teams in the small subset of patients with relatively moderate-to-severe atopic eczema/dermatitis and in this group a detailed allergy assessment is likely to identify individuals with underlying allergy who may have the potential to benefit from allergen avoidance advice and, in some cases, immunotherapy.15–17
Implications for policy, practice and research
This is the first study to estimate the prevalence of allergy in children with atopic eczema/dermatitis in general practice settings and it, therefore, provides the first population-based estimates of aero- and/or food allergy in children with atopic eczema/dermatitis. Scaling these data up to a population level, the findings suggest that approximately 25% of UK children have atopic eczema/dermatitis, 8% have current moderate-to-severe atopic eczema/dermatitis, 2% require allergy testing and 1% have underlying IgE-mediated allergy, which has the potential to be incorporated into the workload of GPs and their teams. Guidelines on the management of atopic eczema/dermatitis correctly highlight the possibility of food allergy as a possible trigger;18,19 future iterations of these guidelines will, however, need to be cognisant of these primary care-based prevalence estimates in order to provide realistic estimates of the likely scale of the problem. Notwithstanding this, there is a need for additional educational training and support for GPs and other hospital-based general paediatricians in order to enable them to correctly diagnose and manage this important sub-group of children with atopic eczema/dermatitis. 20
Future research needs to confirm these estimates through additional population-based studies in other parts of the UK and elsewhere. 21 There is in addition, a need for associated research to assess whether intervening in children with confirmed IgE-mediated atopic eczema/dermatitis improves outcomes in these children. Trials are, therefore, needed of allergen avoidance measures and specific immunotherapy and other potential immuno-modulatory therapies.12,17
Conclusions
atopic eczema/dermatitis is a very common diagnosis in primary care with approximately one in three children being diagnosed within the first 17 years of life. Approximately one in three of these children had current moderate-to-severe atopic eczema/dermatitis. Based on a detailed clinical assessment, allergy was considered a contributory factor in approximately 20% of children with current moderate-to-severe atopic eczema/dermatitis and approximately half of these children tested positive to food and/or aero-allergens. Such work once conducted has the potential to inform guidelines on the optimum management of children with atopic eczema/dermatitis seen in primary care settings.8,22