
Abstract
Objective
Internationally, increasing numbers of women are practising medicine. Gender differences in doctors’ working hours, specialty choices and communication styles are well documented, but studies often neglect contextual factors such as the role of socialised gender expectations on behaviours in the workplace and the medical profession. These may be important as recent studies have reported gender differences in doctors’ activity rates that cannot be explained by specialty or contracted hours, suggesting other sources of variation. This study sought to explore the working lives of hospital doctors and how their work is negotiated according to gender and context.
Design
Gender differences in the day-to-day work of hospital specialists (consultants) in the NHS were investigated using a qualitative approach, including observation and interview methods. Data were analysed inductively using qualitative observation and interview methods.
Setting
Two NHS hospital trusts in England.
Participants
Data were collected from 13 participants working in a variety of specialties and in a range of clinical and non-clinical settings.
Main outcome measures
Various behaviours, attitudes and experiences were explored, such as doctor–patient communication, interactions with colleagues and workload.
Results
Influences at both individual and situational levels, appear to affect differentially the work of male and female doctors. Female consultants described awareness of the impact of behaviours on relationships with colleagues, and their interactions appeared to be more carefully performed. Nurses and other colleagues tend to demonstrate less cooperation with female consultants. Gender differences also exist in patient communication, feelings of work–family conflict and barriers to career progression.
Conclusions
These variations in hospital consultants’ work may have implications for both the quantity and quality of care provided by male and female consultants. This is timely and of importance to the medical workforce as the gender composition approaches parity.
Introduction
Internationally, the gender composition of the medical workforce is changing, described by some as the ‘feminisation’ of medicine. 1 Studies have demonstrated differences in the activity rates of male and female doctors, with full-time female doctors’ recorded activity estimated to be up to 20% lower than that of their male counterparts in the NHS in England, after accounting for confounding covariates such as age and specialty. 2 Factors other than work preferences, such as specialty and working hours, may therefore differentially influence male and female doctors’ work. Exploration of the mechanisms behind such differences is important and timely given the increasing priority that has been placed upon productivity over recent years.
Evidence exploring gender differences in medical work is sparse in the UK medical setting. Differences in communication during medical consultations and longer consultation times have been reported,3–7 but none of these studies are from a UK hospital setting. 7 Earlier observational studies from the US and Sweden suggest that a complex social system may influence the working lives of male and female doctors differently, with female doctors torn between behaving according to stereotypically ‘feminine’ traits of being a woman and the ‘masculine’ stereotype of being a doctor.8,9 Since these studies were undertaken, the gender composition of the medical workforce has changed substantially, with estimates suggesting women will soon comprise over half of the UK medical workforce. 10 In this study gender differences in the working lives of hospital specialists (consultants) working in the English NHS are explored, as part of a body of mixed-methods research which explored the potential sources of gender variations in activity rates in the English NHS. 2
Methods
Study design
An interactionist approach 11 was used to explore consultants’ work within the social system of hospital medical practice. Medicine has traditionally been associated with gender stereotypes, and individuals’ work may be influenced by perceptions about how their interactions may be discredited or approved depending on whether they fit ‘appropriate’ gender expectations. 12 We used a pragmatic, exploratory qualitative design. Data were collected (November 2010–October 2011) using observational methods and interviews aiming to capture the ‘real world’ work of consultants.
Participants
Participant characteristics.
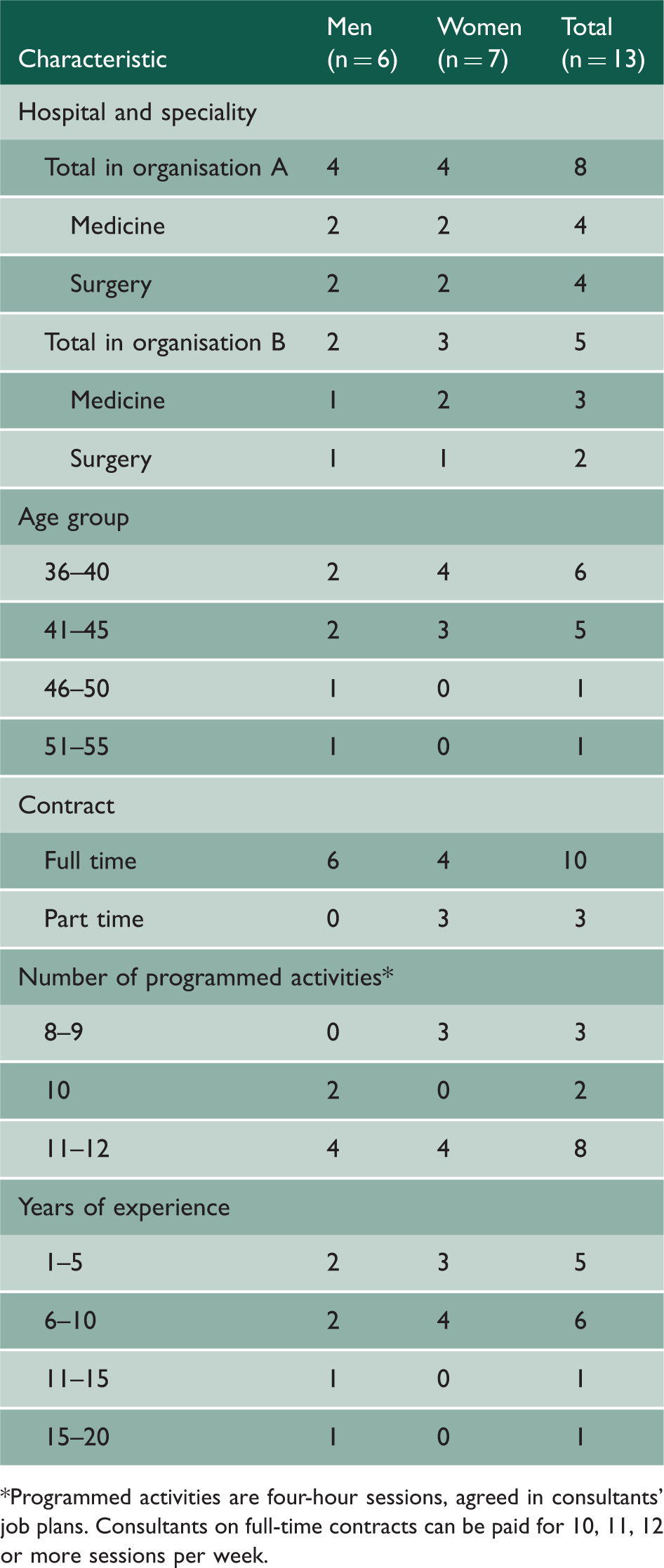
*Programmed activities are four-hour sessions, agreed in consultants’ job plans. Consultants on full-time contracts can be paid for 10, 11, 12 or more sessions per week.
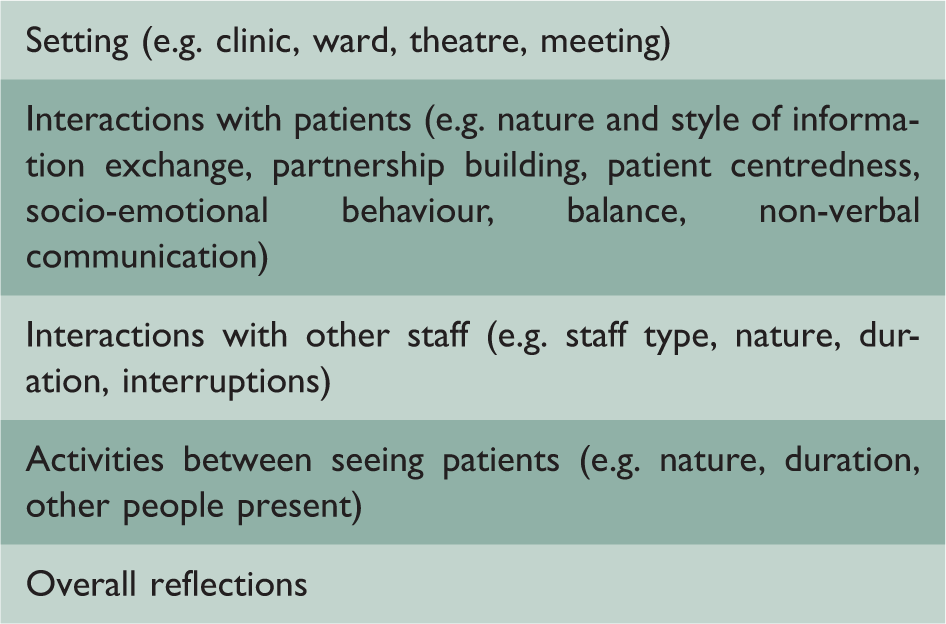
Data collection
Summary of observation framework.
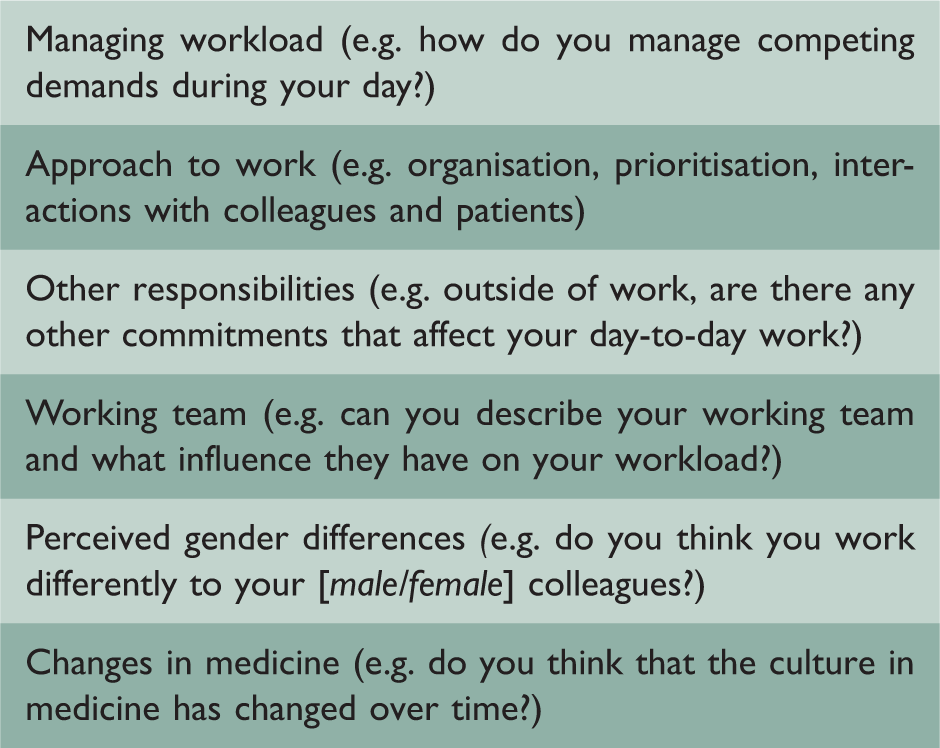
Summary of consultant semi-structured interview.
Data analysis
Data analysis was conducted by one researcher (LJ) in consultation with coauthors. Data were managed using Atlas ti® version 5.0 (Scientific Software Development, Berlin, Germany). Analysis was inductive, following the stages of framework analysis: familiarisation, developing a thematic framework, indexing according to themes and sub-themes, revisiting and recoding data as analysis progresses and themes develop, exploring relationships between codes and developing theoretical understanding. 14 Overarching themes were entered into matrices to map themes and promote comparative analysis of data across participants and settings, build patterns from the data and draw wider interpretations. Observation and interview data were triangulated for convergence and divergence, negative or deviant cases were identified, and findings contextualised to strengthen the transferability of the findings.
Findings
A range of influences affect the working lives of hospital consultants which help to explain differences in their activity rates. These include individual characteristics of the consultants, over which they have a level of control, as well as situational factors that they cannot control directly. The findings are presented through four themes, although these are interrelated and may reinforce one another.
The act of being a consultant
Medical dominance has for many years been the organising principle for healthcare delivery, as manifested through relations between occupations, professional autonomy, medical influence in health service finance and administration, as well as the collective influence of medical associations.
15
Gender differences between participants in this study related to the degree of dominance and how it influenced interactions with patients and colleagues. Dominant traits have stereotypically been associated with medicine and masculinity, whereas women’s behaviours have traditionally been more deferential in nature as a result of social roles and expectations.
8
In contrast to male consultants, who often demonstrated direct, abrupt and didactic communication styles, female consultants in this study were more accepting of problems with nursing staff, more affable with patients and less inclined to immediately redirect patients’ conversation back to their line of medical enquiry: The patient initiates social chat (approximately 5 minutes), then asks the consultant about the new car parking arrangements, ‘which part of the world are you from?’ and discusses cricket scores (FMedA4: observation fieldnotes). I put brakes on myself, I’m always aware that if I lose my temper it’s just going to affect me for the rest of the day… I try not to affect my relationship [with the nurses] (FMedA4: interview).
Nurturing the consultation
Consultations observed with female consultants could broadly be described as more psychosocial and holistic in nature than those observed with males. Women tended to use more affective communication during consultations, with greater displays of nurturing, empathy and sympathy through their voice and body language. Gender differences were particularly apparent when discussing upsetting news with patients. Male consultants, although clearly sympathetic, tended to focus on biomedical information. Female consultants conveyed greater warmth through their voice and body language and used touch more frequently. Some male consultants mentioned discomfort about discussing personal issues with patients, and also a concern that this can lead to excessive patient conversation, referred to by one (male) consultant as ‘opening the flood gates’ (MSurgB10: observation fieldnotes). Cohort differences were also evident, potentially relating to increased psychosocial approaches in medical training. 17
We observed female consultants routinely asking patients if they had any questions at the end of consultations, but this occurred less often with men. This opportunity was often taken by patients to open social conversations, raise medical concerns that were outside the consultant’s specialty or to discuss psychological aspects of their condition. Female consultants’ lower dominance in interactions may also relate to patients’ greater tendency to discuss these ‘additional’ topics, as they were less likely to steer patients’ conversations or interrupt them.
The ‘additional’ conversations created time pressure for all consultants and while they acknowledged the importance of patient-centred care, both men and women commented on how they struggled to strike a balance between conversation and efficiency: One of the patients in clinic was telling me something that was completely off the subject, and I had to sit for about ten or fifteen minutes and talk to him about it and at the end when he stopped crying he said “thank you very much doctor, I feel much better” and left. Probably didn’t do much about his [condition], but hopefully he felt a bit better, but is that the most effective use of my time? (FMedA1: interview) The only thing that can make a consultation go quicker is if you just don’t talk … there’s the sort of joke as a trainee that if you’re trying to work in a busy clinic, the last thing you want to ask the patient is how they are. (MSurgA8: interview)
Tensions across social roles: balancing the personal and professional
Both men and women reported struggling with workload and craving greater work–life balance, but greater expressions of stress were revealed by women. Expressions of feelings of stress centred on the pressure women experienced from responsibilities outside work. Gender differences remained even when comparing only those consultants with dependent children. Male consultants with children described the support they received from wives who had taken career breaks to care for the family: [My wife’s] not working, so she’s at home full-time, and that’s useful for me, hence this is why I don’t feel that I’m under a lot of pressure from that side, while some of my [female colleagues] are under a lot of pressure … who’s going to pick them up from school, who’s going to feed them their tea. (MMedB12: interview) I used to be a good doctor and when I was off for a year I was a brilliant mother and now I’m a crap mum and a crap doctor (FMedA4: interview).
Gendered culture in medicine and progression
Participants described aspects of a gendered culture that they felt existed in medicine, such as gendered specialty choices. While male consultants did not comment on the potential negative effects of this, female consultants discussed potential barriers to progress in their careers, categorised here as either indirect or direct.
Indirect barriers described by female consultants included unpredictability of working hours, influencing their career choices. Organisational structures were not always compatible with their needs, despite growing numbers of women in medicine: When I became pregnant there was utter shock and surprise and the organisation of my maternity leave was haphazard and incredibly stressful … you know, I even considered not having the second child, purely because of work reasons (FMedA2: interview). When [part-time female consultants] are away, who is taking their post up? It’s the males who are taking up their job. So we are taking up extra work, their work, which we’re not getting paid for (MMedB12: interview).
Confused identities and expectations
During observations, gender differences in the behaviours of consultants’ patients and colleagues seemed to arise as a result of perceptions held about male and female doctors. Potentially related to displays of dominance in interactions, patients appeared to perceive women as more approachable than men, interrupting them and becoming tearful more often in both medical and surgical specialties.
Female doctors were also more likely to be interrupted by colleagues. Colleagues often appeared more comfortable approaching female consultants when making requests, in contrast with observed hesitancy to interrupting male consultants: A female [health assistant] comes into his clinic room to ask him something and he is doing admin, she waits in silence until he says ‘start talking’ (MSurgA8: Observation fieldnotes). If they don’t [know me] then they naturally assume that [the male registrar] is the leader (FMedA4: interview).
Instances of uncooperative behaviour occurred across male and female consultants, however, and also with those who demonstrated dominant characteristics with their colleagues. This suggests that these behaviours may be complex and cannot be solely explained by gender differences or perceptions of dominance. Theatre nurses, for example, were observed rolling their eyes when asked to do things by a male consultant who adopted a direct and dominant communication style. An alternative explanation could relate to the legitimacy of doctors, as viewed by their colleagues. In an interview, a female consultant commented on the de-legitimation of consultants in their roles and suggested that lack of respect or de-legitimation may be more of a problem for female consultants: I don’t want to use the word respect but that’s what it is isn’t it? [Nurses are] a bit more deferential to male colleagues, older ones I think especially … if you watch the way they get treated, it’s very different. (FMedA4: interview)
Discussion
This study provides a contextualised exploration of the effect of doctors’ gender on their day-to-day work in hospital settings in the English NHS. Previous studies have been conducted primarily in North America, at a time when there were fewer women in medicine and many earlier studies focused on gender differences in communication in primary care consultations. Despite the substantial increase in proportion of women practising medicine today, these findings suggest that cultural norms and historically gendered customs in medicine continue to exist and may influence male and female doctors’ careers and working practices.
Influences exist at both individual behavioural and organisational levels. Situational factors, such as the behaviours of colleagues and patients, have been identified that appear to relate to a complex system of structures and expectations, previously described by Davies as ‘all imbued by gender’ (p. 721). 8 Individual behaviours, associated with gender perceptions themselves, may create and maintain social expectations of gendered behaviours, thus influencing interactions. Greater displays of dominance by male consultants, for example, may reflect social acceptability of this ‘masculine’ trait, but may also contribute to patients’ and colleagues’ gendered perceptions about how male and female doctors’ behaviours differ. This can be observed in their interactions, such as the lower levels of cooperation with female consultants found in this study.
Female doctors may feel torn between nurturing, caring behaviours, traditionally associated with women’s roles, and more dominant and powerful interactions, traditionally associated with medical doctors. 8 Our findings are consistent with Cassell’s US findings, 9 in particular that female surgeons portrayed typically female traits (such as lowered dominance) with nursing staff and patients, and more masculine behaviours (such as directive behaviours) with fellow doctors. 9 The lack of assistance and greater interruptions observed with women in this study may relate to their lower displays of dominance or to colleagues’ perceptions of legitimacy. 19 Both men and women in this study were aware of the importance of psychosocial communication, but male consultants demonstrated less comfort and engagement with this in practice. This supports earlier survey evidence that female doctors feel better equipped in psychosocial skills. 20 External factors also affected this: women were viewed as more approachable, and their patients demonstrated greater social conversation and likelihood of becoming tearful.
It appeared that women face greater responsibilities outside work, leading to tensions in personal and professional roles. Female consultants expressed more feelings of guilt about their roles, and higher levels of stress associated with this, replicating findings from previous studies internationally.21,22 Interviews with consultants also revealed experiences of a gendered culture in medicine, and some women experienced gender discrimination first-hand.
Study implications
The gendered behaviours identified through this study have generated insights which may contribute to explaining lower reported clinical activity rates amongst female consultants in the UK setting. 2 Female consultants’ working style, including relatively lower dominance and a more holistic approach, may contribute to reduced overall activity if they struggle to gain support from colleagues or consultations overrun. This is supported by previous findings that female doctors spend longer on consultations with patients. 7 Additionally, situational factors such as poorer levels of cooperation from nursing staff, identity confusion, greater responsibilities outside work and potentially greater negative spillover from home to work lives may differentially affect male and female doctors, all of which may contribute to lower activity rates.
As the gender composition of the medical workforce approaches parity, increasing emphasis needs to be placed on supporting female consultants and reducing gender differences. Policy makers and hospital managers could take steps to reduce the difficulties that female consultants encounter, challenging stereotypes and promoting ‘family friendly’ working environments. 23
Aside from this potential impact on the quantity of care provided by female consultants, their greater tendency to engage in a patient-centred approach also has implications for the quality of care provided. The importance of patient-centredness in healthcare is recognised internationally24,25 as well as in the NHS. Although training in patient-centred consultations forms an important part of UK medical curricula, 26 gender differences could be considered by medical educators.
While quality and quantity in healthcare appear to be two opposing forces – for example women may engage more in psychosocial communication (increasing quality) but this may be related to longer and fewer consultations (reducing quantity) – there may be productivity gains of more patient-centred consultations if outcomes are ultimately improved. Research suggests that patient-centredness may affect patients’ emotional health, symptom resolution, physiological outcomes and quality of life.27,28
Study limitations
These findings necessarily relate to the specific settings studied in the NHS in England. Nevertheless, they represent the experiences and attitudes of hospital consultants across a range of medical and surgical specialties in two organisations, and findings are supported by previous studies in other settings.8,9,29 While it is possible that individuals in this study may have altered their behaviours as a result of being observed, this risk is reduced by undertaking observations on multiple occasions in different settings. Consultants are often shadowed as part of the teaching process, and several participants commented that they felt at ease or forgot that they were being observed. By using two researchers to undertake data collection and discuss the stages of analysis, the influence of an individual researcher’s own beliefs, values and attitudes in this research process has been reduced. Piloting both observation and interviews, and data triangulation across observational and interview methods also strengthen the findings. It is possible that the topics discussed by participants during interviews may have been influenced by the gender of the researchers, for example it may have encouraged greater openness about negative experiences among female consultants in this study.
Conclusions
Findings from this study provide insight into the ways that doctors’ gender affects aspects of their working lives, with potentially important implications for the quality and quantity of healthcare provision. Expectations of the behaviours of female doctors may lead patients to spend longer on psychosocial communication, can mean that colleagues on occasion are less cooperative and may influence the behaviours of doctors themselves, perpetuating the cycle and reinforcing perceptions and even stereotypes. Policymakers and medical educators should consider these findings and their implications, particularly during this time of substantial change in the gender composition of the medical workforce.