
Abstract
Summary
Keywords
Introduction
In 1990, the Commission on Health Research for Development declared that ‘strengthening research capacity in developing countries is one of the most powerful, cost-effective, and sustainable means of advancing health and development’. 1 It is widely recognised that in those countries suffering the greatest number of avoidable deaths, particularly in sub-Saharan Africa, there also tends to be weak and under-developed national health research systems. Consequently, these countries are less able to generate new information and knowledge for:
While research capacity strengthening initiatives, largely focused on the training and development of individual researchers, became increasingly common during the 1990s, their limited overall success pointed to the lack of a systems perspective for understanding national health research. A systems perspective recognises that capacity for research resides at a number of interconnecting levels, such as individuals, institutions, nation states and networks, with a variety of individuals and organisations performing a wide range of functions. A systems perspective helps us to see that each of these levels, actors and functions are interdependent on each other and that if the capacity of the system is to be developed, they all must be taken into account. 5
The idea of a national health research system has grown since 2000. A well-functioning system is needed by each country to:
‘identify priorities, mobilize resources and maximize the use of existing ones, develop and sustain the human and institutional capacity necessary to conduct research, disseminate research results to target audiences, apply research results in policy and practice, and evaluate the impact of research on health outcomes’.
6
The systematisation of such processes is vital to improve the transparency and accountability of health research activities.
While there are some crude indications of weak research capacity in African countries (e.g. the paucity of research reported in international journals; the shortage of research and development scientists compared with wealthier regions; the underdevelopment of research training opportunities within the countries concerned), there remains little understanding of where, and in what way, capacity is weak. 7 Most attempts to assess, and indeed strengthen, capacity have been at the individual level. Capacity assessment at the institutional level and wider, at the level of the national system, is much more complex and has received much less attention. 8
In order to help this assessment, the World Health Organization (WHO) began work to develop a conceptual understanding of health research systems. 9 It formed the Health Research System Analysis (HRSA) Initiative, which progressed this work and developed a framework for describing and analysing national health research from a system’s perspective. 10
In this framework, stewardship is identified as one of the four functions of a health research system, along with financing, creating and sustaining resources, and producing and using research. Stewardship is perhaps the most complex of the four functions since it is difficult to describe exactly what it entails, and what capacities are important for good stewardship. Yet it is also the most important since it has a fundamental influence on all the other functions. 11
The term ‘stewardship’ is used interchangeably with the term ‘governance’. Both concepts relate to the functions, systems and processes that collectively ensure that research is ethically conducted, relevant to the people it is targeted for, and of recognised scientific quality. The governance of health research can be assessed by criteria such as representativeness, transparency and accountability. It concerns both how and how well decisions are made regarding what research is supported and conducted, by whom, and for what ends. 12
In the assessment of research capacity at either institutional or national level, capacity for stewardship has received almost no analytical attention to date. The key capacities required to implement the stewardship function include:
13
Skills to formulate a vision, mission, goal and policy for health research Skills to prioritise health research, using appropriate methodologies and approaches Capacity to address ethical considerations in research projects Capacity to collect, analyse and use information to assess and evaluate the various aspects and steps in the research process Capacity to design and implement policies that address in an effective way existing inequities in health research, including the financing of research, setting the research agenda, the gender bias, and inequities in knowledge publication and utilisation
In a similar vein, stewardship includes defining and articulating a vision for a national health research system, identifying appropriate health research priorities, setting and monitoring ethical standards, and monitoring and evaluating the health research system. 10
This report presents an analysis of data drawn from a survey of national health research systems in 42 sub-Saharan countries in Africa. Analysis of the data from this survey offers a new opportunity to explore aspects of capacity related to governance. The survey approach identifies a number of core indicators and key descriptive variables to help describe and assess core functions within the health research system.
Methods
The methods followed to assess national health information systems are described elsewhere 14 but are summarised briefly here.
The survey used Tool 6 from the Health Research System Analysis (HRSA) Initiative Toolkit: Methods for Collecting Benchmarks and Systems Analysis Toolkit. 15 Within the institutional survey, seven questionnaires representing separate ‘modules’ were completed by the respondent institutions. The tool was initially pilot tested by WHO in 10 low- and middle-income countries, including three African countries (Cameroon, Senegal and the United Republic of Tanzania). The tools were translated into French and Portuguese before their use in the surveys. Questionnaires in English were sent to institutions in 19 countries, in French in 19 countries and in Portuguese in four countries.
This report draws on data from three of those questionnaires:
Module 1000 – Identification, introduction and background information Module 2000 – Types and approaches to research Module 7000 – Ethical review of research
These questionnaires are designed to focus on issues pertaining to the governance and stewardship of research at the institutional level. The main criterion for considering an institution as a ‘health research institution’ was that it should be engaged in the conception or creation of new knowledge, products, processes, methods and systems related to any aspect of health, such as factors affecting health and ways of promoting and improving it. Institutions could be departments of medical schools, universities, teaching or non-teaching hospitals, independent research institutions, governmental agencies, pharmaceutical and other for-profit and not-for profit businesses, charities and non-governmental organisations.
WHO initially created a database of research institutions in the Region from various sources in order to build a reasonably comprehensive inventory. The list of health research institutions corresponding to a particular country was then sent to the country focal team to verify and confirm whether the listed institutions still existed and were operational, and whether they had carried out research on health or health-related topics in the past five years. A regular exchange with the coordinating team at the WHO Regional Office for Africa to rectify discrepancies and inconsistencies, and add or remove relevant or irrelevant institutions, eventually led to a final list of all institutions conducting health research in countries, totalling 1882 institutions in the 42 countries of the Region. Of these, a total of 847 institutions responded to the survey and were included in this report.
For response to questions where institutions were asked to rank items in the questionnaire, we used weighting schemes to arrive at composite ranks. For example, where the response required ranking an item on a 1 to 5 scale, a weight of five was given to the first rank, four to the second rank and so on, with the fifth rank getting the least weight of one. The average of these was used to derive a composite rank of items.
We used IBM® SPSS® Statistics Version 19 statistical software to analyse the data.
Results
Characteristics of health research institutions in 42 sub-Saharan African countries, 2009.

Number of respondent health institutions, out of 847 surveyed.
Types and approaches to research in institutions conducting health research in 42 sub-Saharan countries, 2009.

Number of respondent health institutions, out of 847 surveyed.
During the previous 12 months, the heads of 358 of the respondent institutions (49%, n = 729) participated in the setting or coordination of national research priorities. For national health research priorities, the number was similar (316 or 44%, n = 714) (not shown in table). The most frequently cited priorities for contributing to or performing research were improving health programmes (19%, n = 701), producing new knowledge (17%), influencing health policies (16%) and conducting operational research (12%) (Figure 1).
Priorities of health research institutions for contributing to or performing research in the WHO African Region, 2009.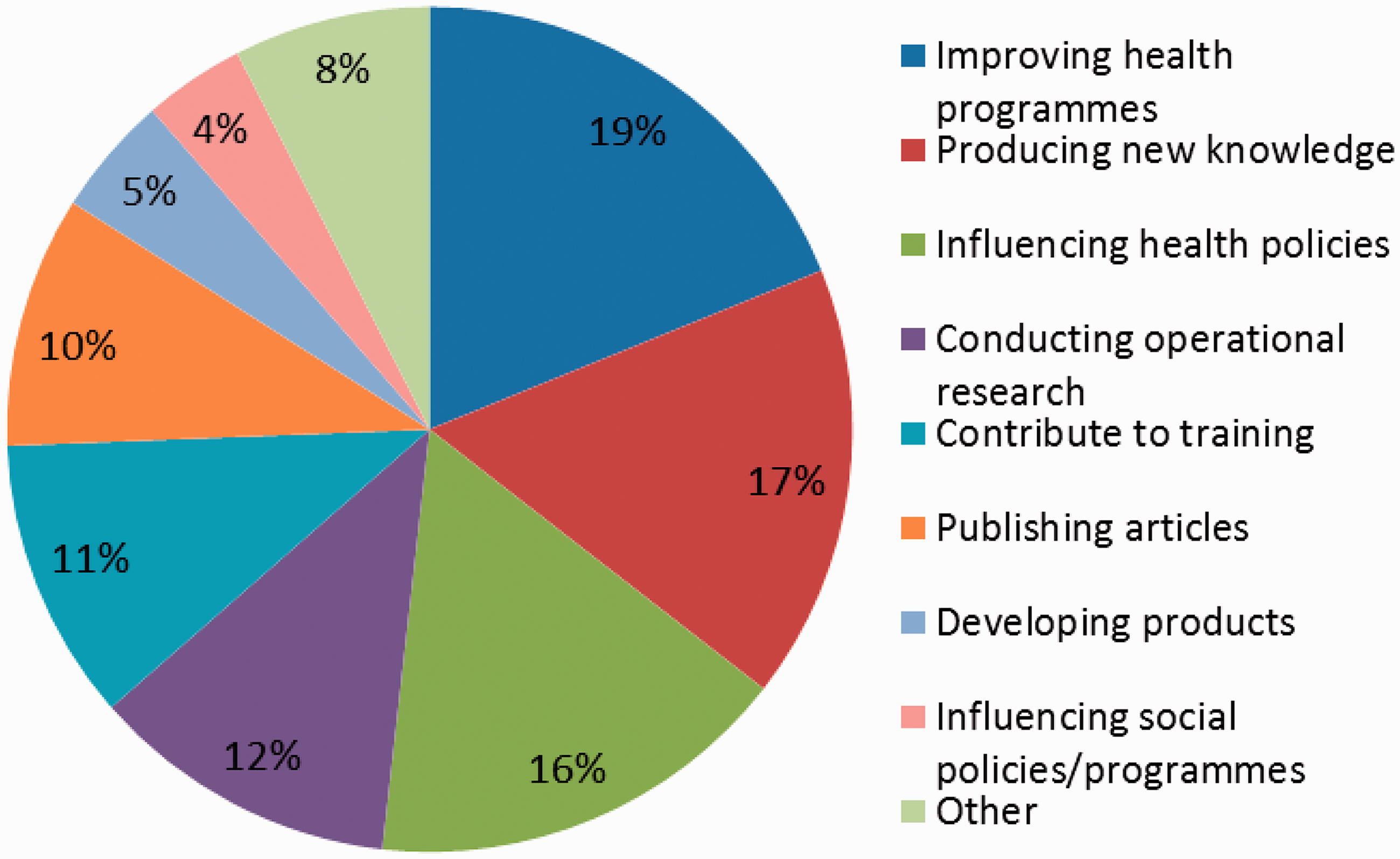
Scientific review of research in health research institutions in the WHO African Region, 2009.

Number of respondent institutions out of 847 surveyed.
Those with policies for review of proposals were asked what these reviews addressed. The five most frequently mentioned criteria were relevance of research topic to institution’s goals, mission and priority; scientific merit; comprehensive review of literature and reports; ethical review; and project budget.
In response to questions about the written policies or guidelines for the scientific review of proposals, 165 of respondent institutions (67%) stated that their written criteria addressed ethical review.
Only 190 of respondent institutions (29%) had a standing or established scientific review committee that met regularly. Of these, 157 institutions reported that the committee had explicit standard operating procedures. Only 169 (28%) of respondent institutions had a written policy requiring research projects to be evaluated while in progress; the proportion requiring them to be evaluated after the research was completed was only slightly higher (33%).
Existence of institutional policies on research ethics in health research institutions, WHO African Region, 2009.

Governance of health research institutions in 42 sub-Saharan African countries, 2009.

Number of respondent institutions out of 847 surveyed.
In most cases, the heads of the respondent institutions were appointed either by a Board of Governors, Directors or Trustees of the institution (in 50% of cases), or by a political process such as by a Minister, Prime Minister or President within the country (in 26% of cases). Nominations for the applicant pool for the position of head of the institution were generally made by members of the Board of Governors, Directors or Trustees (in 32% of cases) or based on recommendations either from politicians or other policy-makers (in 24% of cases). In 45% of cases, the applicant pool was obtained through a widely advertised open call.
When asked what were the three most significant barriers or limitations the institution faces in order to achieve its mission (Figure 2), the five most frequently mentioned issues were:
Limited level, sustainability and transparency of funding (22%, n = 719) Low salary and benefits of professional staff (15%) Reliance or dependence on extra budgetary support for institution's activities or projects (12%) Limited skilled human resources (11%) Poor quality or lack of workspace or equipment (10%) Significant barriers (top chart) and strengths (lower chart) to health research faced by health research institutions in 42 sub-Saharan African countries, 2009.
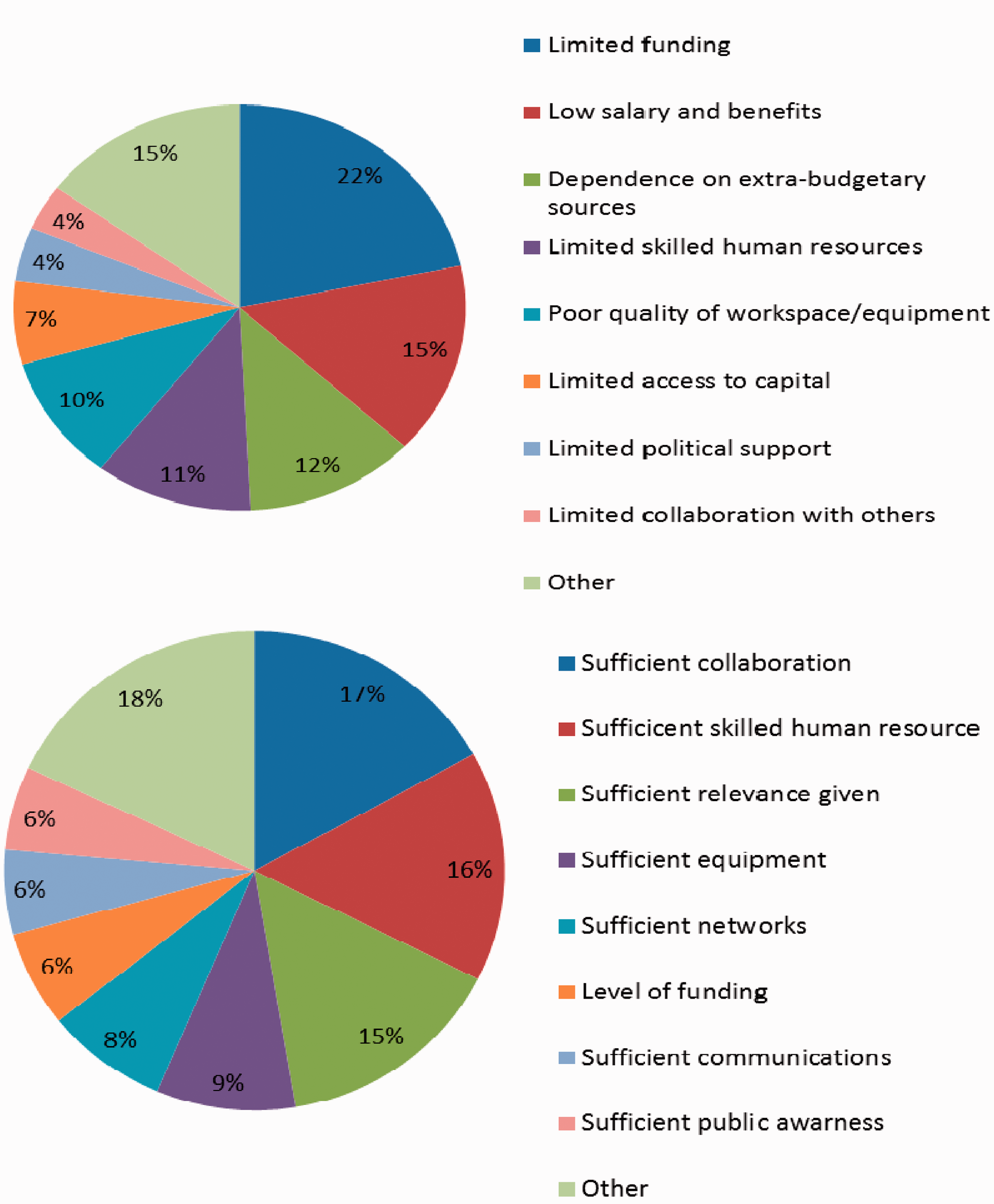
When asked what were the three most significant strengths or successes the institution had that contribute to achieve its mission (Figure 2), the five most frequently mentioned issues were:
Sufficient collaboration with others (17%, n = 723) Sufficient skilled human resources (16%) Sufficient perceived relevance of activities given national problems and priorities (15%) Sufficient quality or availability of workspace or equipment (9%) Sufficient access to professional networks (8%)
Collaboration between stakeholders of health research in 42 sub-Saharan African countries, 2009.
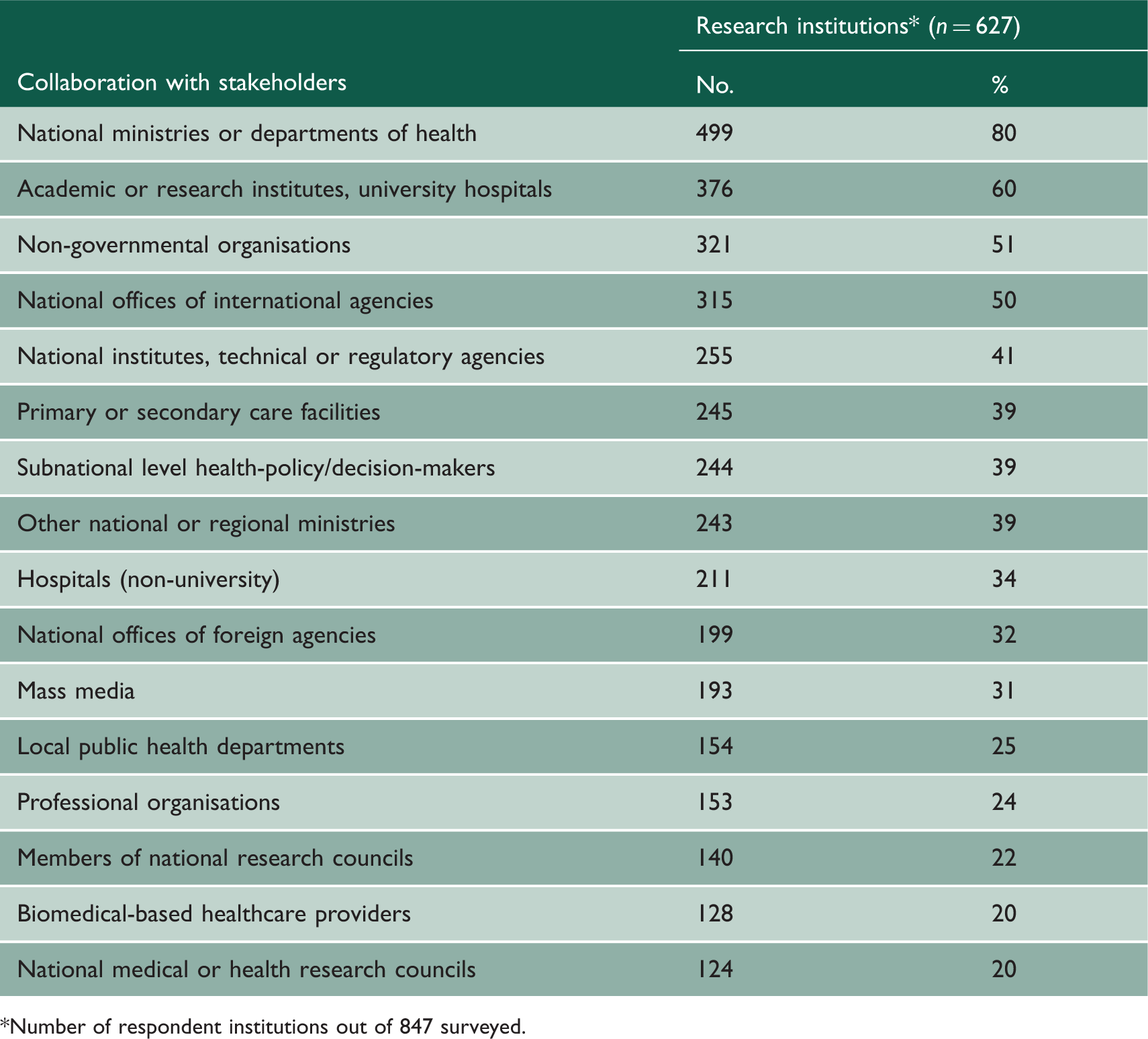
Number of respondent institutions out of 847 surveyed.
Many institutions reported having no explicit incentives to encourage or mandate collaboration beyond general discussion. A small proportion of institutions reported that collaboration with various actors was encouraged or mandated through requirements for funding, financial incentives for budget, career development opportunities or other specific incentives.
Obstacles to collaboration between stakeholders of health research in 42 sub-Saharan African countries, 2009.
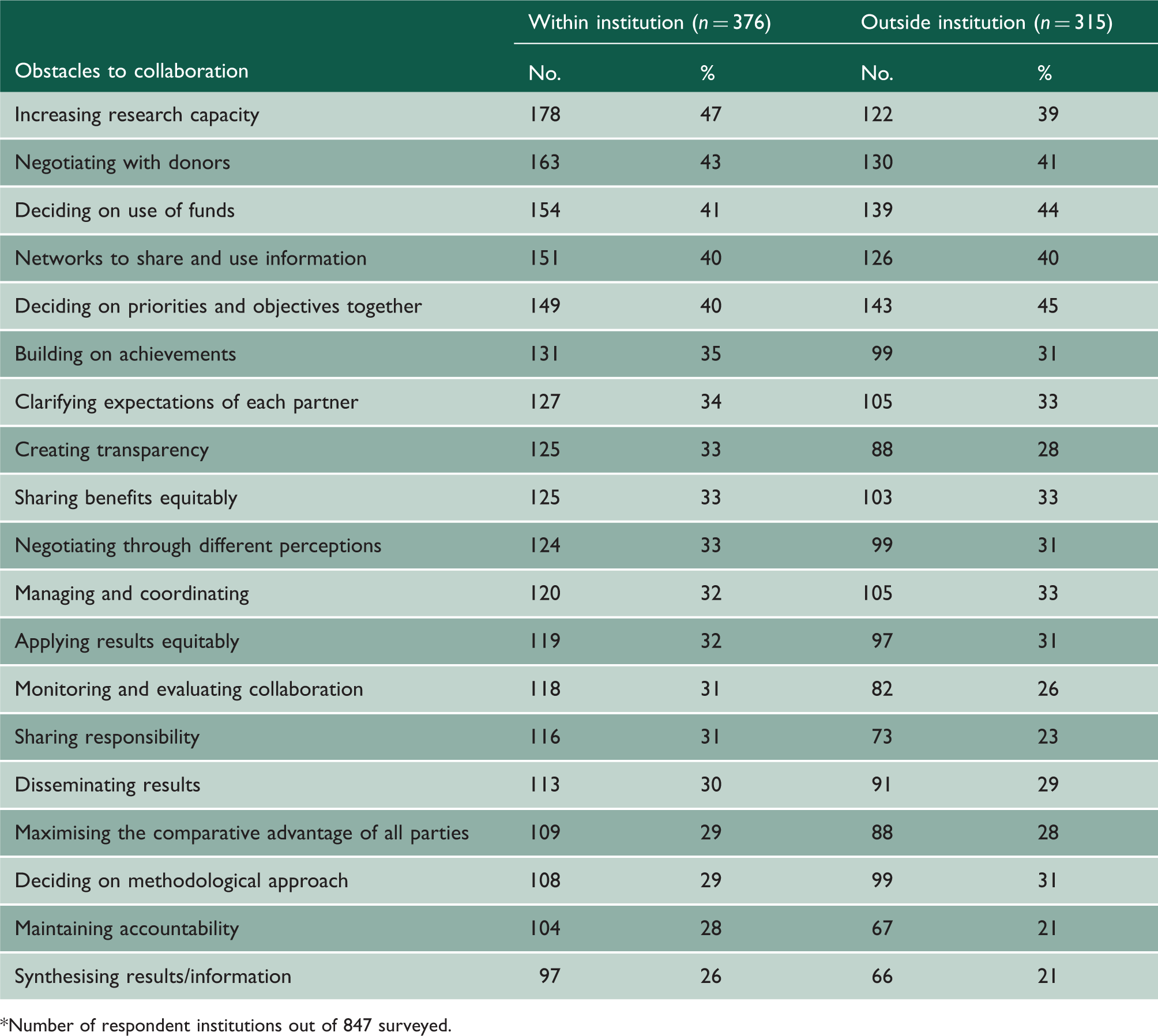
Number of respondent institutions out of 847 surveyed.
Discussion
Almost half of the respondent institution heads said they had contributed during the previous 12 months to the setting or coordination of national and/or health research priorities. However, perceived relevance of activities to health problems and health systems was one of the five most significant success factors to performing or sustaining health research activities. This relevance, whether real or perceived, might be increased by a greater involvement of the institutions in national health research priority-setting processes.
Almost two-thirds of the respondent institutions operate at a national level. Theoretically, this should mean that they are geared towards national health issues. However, leadership and coordination at the national level is lacking, given that only one-fifth of countries have a functional national health research management forum. 16 The paucity of respondent institutions (8%) that focused on regional health research issues may reflect the under-developed state of health research systems in general.
In order to develop a rich and varied research culture, the practice of health research should extend beyond academic institutions and laboratories to include health service providers, policy-makers and civil society. Moreover, it should encompass a range of actors across a variety of sectors such as agriculture, finance and education, and investigate a broad range of issues in addition to life sciences or clinical medicine. 11
The respondent institutions represent a number of fields of science and technology, spread across a range of different ‘types’ of institutions. Non-medical institutions clearly play an important role in the conduct of research for health. While health sciences are broadly represented, other fields such as agricultural sciences, physical sciences, earth and related environmental sciences, and the humanities are less so. The institutions contribute to research on a wide range of topics, although research on specific diseases or conditions appears to feature more frequently than other topics (such as research on health impact, or research on injuries). Research on health systems, while less prominent than that on specific diseases, is contributed to by almost half of the institutions overall, with a little over one-third of institutions contributing to health policy and systems research. Health policy and systems research is known to be relatively neglected at the global level, but its importance to the development of strong national health systems, and appropriate, feasible and equitable health policies, has been underlined in recent years. 17
Poor coordination between research institutions at national, regional and international levels is cited as an important impediment to the effectiveness of health research systems in the literature. 18 Collaboration with others and strong, equal research partnerships can help to ensure not only that good-quality research is conducted and research capacity within institutions is strengthened, but also that appropriate research priorities are identified, and that there are strong links between research and policy/practice. Such collaboration should be supported by national guidelines that ensure equality of partnerships and appropriateness of research. The data show that such guidelines are lacking in most countries, both at country level and within institutions.
Among the respondent institutions there were three important barriers to performing health research activities, highlighting poor coordination as an issue:
Limited or lack of a network of relevant actors in health research Limited or lack of collaboration with other researchers, institutions and organisations Poor quality or lack of communication between researchers, institutions and organisations
Coordination could be usefully supported and encouraged through a national network of health research and development. However, only nine of the 42 respondent countries (21%) have such a network. 16
Communication between researchers and policy-makers has proven to be an important facilitator in increasing the use of evidence in health policy. 19 Most of the respondent institutions mentioned having collaborated with national ministries or departments of health. Moreover, providing technical support to the ministry of health was cited by one-third of institutions as an activity that they had been involved in during the previous 12 months. Collaboration with other key actors such as national offices of international organisations, national institutes, and technical or regulatory agencies was also fairly high. However, most institutions had no explicit incentives to encourage or mandate collaboration beyond general discussion with agencies or institutions outside of their own.
Regional and global networks, and the inclusion of national-level actors in them, can play a key role in supporting appropriate national research priority-setting and in influencing international and regional funding priorities. 20 Only a small proportion of the respondent institutions operate at either a regional or an international level. The development of networks to collect, share, access and use information and data is one of the obstacles in establishing or maintaining balanced research partnerships, either within or outside the country (cited by 40% of respondent institutions).
In order for health research to realise its potential to impact positively on health development, close links are needed between the health research community, the broader health system and the development community. In addition, researchers need to communicate far more effectively among themselves and with other stakeholders. Institutions can support and reinforce each other’s efforts through exchange of resources and personnel, and by working together towards mutually agreed goals. 7
Continuous monitoring and evaluation is required to ensure that resources are used efficiently and in line with agreed priorities, and to ensure that the conduct of research is appropriate and ethical. Countries and institutions need clear guidelines and capable ethical review mechanisms that can guide the appraisal and oversight of all research projects. 13 Research agendas at both institutional and national levels need adequate, sustainable and transparent funding, professional research managers, ethical standards, and accountability in the use of public funds, in order to succeed. As already mentioned, lack of funding is identified as a key barrier for research institutions. At national level, since functional national health research systems are deemed to exist in only 15 of the respondent countries, monitoring and evaluation are likely to be extremely weak. 16 The absence in most countries of a law relating to health research, of functional research management forums, and of functioning scientific review committees means that processes overall are unlikely to be transparent and accountable. Also, the lack of a functional ethical review committee in one-quarter of respondent countries highlights an important area of weakness.
Similarly, the presence of some key policies or guidelines within the institutions is lacking. The majority of institutions do not have written policies or guidelines, either for the scientific review of proposals or regarding conflict of interest on scientific review committees. Even fewer have a written policy requiring research projects to be evaluated, either while in progress or after the research is completed.
Less than two-thirds of respondent institutions have a Board of Governors, Directors or Trustees. Strategic planning is an important role of these board members (recognised by 41% of respondent institutions). The presence or absence of a Board, and the structure, composition and power of that Board, is likely to influence the transparency of decision-making within the institutions and the institutions’ accountability. The way in which the head of the institution is identified and appointed is an important indication of transparency; among our sample, the Board (where there was one) was influential in making the appointment, although the applicant pool was obtained through a widely advertised open call in only 45% of cases.
The strength of a national health research system will depend upon both institutions within the government and those outside government, with varying degrees of independence. The presence and strength of government research institutions is a sign of the prominence of research at government level – and perhaps of the importance placed on the relationship between research evidence and health policy decision-making. The respondent sample shows a variety of research institutions, including civil society and health service providers. The relative ‘youth’ of research institutions overall is cause for concern. On the other hand, independent research institutions, which might have a greater ability to operate outside of the pressures to defend certain policies or investments, are also important. These constituted about 12% of all the respondent institutions included.
The data analysed in this paper have limitations that warrant a careful interpretation of the results. One issue is that the data were not complete. While respondents were asked to leave no questions blank, data for many questions were missing for some of the respondent institutions and countries. This could be seen as a symptom of weak health research systems, where data are not easily available. Nevertheless, the high number of respondent institutions ensures that analysis was still robust. Another limitation relates to the analysis of the survey at a country level because some countries conducted a complete census of their institutions, while others only surveyed a sample. A complete list of the sampling fractions is described elsewhere. 5 Thus, results of comparison of countries should be interpreted with caution. However, comparisons of countries were not attempted in the present study.
The results of this survey show the broad range and types of research institutions, and consequently of the research activities they contribute to, and show that there is a good basis for the strengthening of research capacity within the Region. While these institutions face many barriers, notably related to funding and the ability to attract and retain skilled staff through appropriate salaries and other benefits, they also present many strengths. Many have a long history and have a strong combination of primary functions that might enable them to link research with higher education, government decision-making or health service delivery. Although some institutions demonstrate good practice in terms of the establishment of structures and processes that help ensure accountability and transparency (such as the presence of a governing Board, the open appointment of institute heads, the presence of review committees and of written guidelines for these), many others do not. There is, perhaps, potential for newer, less-established institutions to learn from and strengthen their capacity alongside more established institutions.
Most institutions operate at a national level and there are indications of communication and collaboration between a wide range of different individuals and organisations. However, communication, collaboration and partnership among institutions and individuals within the national health research system, and with others outside the national system, is an important area requiring further development. This will help to develop a strong national system in which actors can work together to define and work towards a shared vision for health research. But this will require national leadership and coordination. From this survey, there is little evidence that such leadership is currently provided.
While it is positive that almost half of institution heads had contributed to the setting or coordination of national and/or health research priorities in the previous 12 months, the absence of national health research policies or plans in many of the countries is clearly cause for concern. Many institutions had difficulties relating their activities to health problems and health systems, and there was little consistency in institutions’ priorities for contributing to research.
Without strong national leadership and clear prioritisation processes, it is unlikely that research activities will correspond closely with need. It is also unlikely that health policy and systems research will be emphasised, despite a recognised understanding of its need to inform the development of strong national health systems and appropriate, feasible and equitable health policies.
From the national-level survey and the data from the institutional survey, the setting and monitoring of ethical standards appears to be a neglected function. There is a clear need to support the establishment of functioning ethical review committees at national and institutional levels, guided by laws and written guidelines.
Data indicate that the function of monitoring and evaluating the health research system is also neglected. While this function will be improved through better collaboration both inside and outside the country, it also needs to be strengthened at institutional level through the independent evaluation of institutions contributing to research, and through the rigorous evaluation of research projects when they are ongoing and upon completion. This will help to ensure that research is conducted according to best practice, that research activities are in line with priorities and needs, and that research funds are spent appropriately and transparently.
Conclusions
It is clear that the results of the survey provide a valuable snapshot of the key stewardship functions, and some useful benchmarks by which to assess current governance at institutional and national levels. When combined with further national-level data, and preferably some more in-depth case studies on national health research systems, they will help to provide a broader picture of national health research capacity.