
Abstract
Objectives
Following the election of the Labour government in 1997, policies were developed in England to reduce waiting times for NHS treatment with commitments to reduce health inequalities. Similar policies were adopted in Scotland but with less emphasis on the use of the private sector to deliver NHS treatments than in England. This study uses routinely collected NHS Scotland data to analyse geographical and socioeconomic inequalities in elective hip arthroplasty treatment before and after the introduction of the waiting time initiatives in Scotland in 2003.
Design
Ecological study design.
Setting
Scotland.
Participants
NHS-funded patients receiving elective hip arthroplasty delivered by the NHS and private hospitals between 1 April 1998 and 31 March 2008.
Main outcome measures
Directly standardised treatment rates and incidence rate ratios calculated using Poisson regression.
Results
There was a 42% increase in NHS-funded hip arthroplasties carried out in Scotland from 4095 in 2002–2003 (1 April 2002–31 March 2003) to 5829 in 2007–2008. There is evidence of a statistically significant reduction in geographical inequality (likelihood ratio test p < 0.001) but no evidence of any statistically significant change in socioeconomic inequality (p = 0.108), comparing the 5 years after 1 April 2003 with the 5 years before 1 April 2003. The number of NHS-funded hip arthroplasties undertaken privately rose from 1.1% in 2002–2003 to 2.9% in 2007–2008, whereas the NHS Golden Jubilee National Hospital increased its share from 3.3% to 10.6% over the same period.
Conclusions
The reduction in geographical inequality, or ‘postcode lottery’, in hip arthroplasty treatment in Scotland may be due to increased NHS capacity, in particular the development of the NHS Golden Jubilee National Hospital in Clydebank, Greater Glasgow as a dedicated centre to reduce surgery waiting times.
Introduction
Hip arthroplasty is one of the most frequently performed operations in the UK.1,2 It is cost-effective even among elderly patients and on average leads to an additional 6.5 quality-adjusted life years per patient. 3 Despite its effectiveness and the increasing needs of an ageing population, there is considerable pressure in England with commissioners limiting access to planned hip surgery.4,5
Reducing health inequalities is a priority of both UK and Scottish governments. Research has shown that patients living in areas of high socioeconomic deprivation are less likely to receive hip arthroplasty in both England and Scotland, even after adjusting for age- and sex-related differences and despite relatively high levels of need compared with patients from less deprived areas.6–10 Patients living in areas of high socioeconomic deprivation also undergo surgery younger, have more co-morbidities, more severe symptoms at presentation and are not as satisfied with the outcome of surgery compared with patients from less deprived areas. 11
Geographical inequalities also exist with patients in urban areas of England having lower rates of hip replacement than patients elsewhere as do patients living in the North of England compared with the South when adjusted for age differences.6–8,12 A study of patients treated in hospitals in the West of Scotland found higher age and sex standardised rates of primary total hip replacement among rural compared with urban communities. 13 The ‘postcode lottery’ in treatment access, where patients in need receive differing levels of treatment depending on where they live is known to exist for other treatments, for example, varicose vein and postbariatric surgery.14,15 Recent research by Dr Foster Intelligence Ltd 16 has found huge variation across clinical commissioning groups (CCGs) in England in hip arthroplasties commissioned between financial year 2010–2011 and 2012–2013, from a decrease of 29% in National Health Service (NHS) Hammersmith and Fulham CCG to an increase of 57% in NHS Leeds South and East CCG, leading to media speculation of a postcode lottery in these treatments.
The war on waiting in England
Following the election of the Labour government in 1997, the English Department of Health (DoH) introduced policies to reduce waiting times for patients to a maximum of 18 weeks from referral to treatment. Phase two of the ‘war on waiting’ between 2000 and 2004 saw the introduction of ‘Diagnostic and Treatment Centres’, for elective patients only, with the intention of avoiding the cancellation and rescheduling of appointments often encountered by patients in NHS general hospitals. 17 In 2002, the DoH concluded that the private sector would be needed to deliver the additional capacity on behalf of the NHS. 18 Consequently, £5.6 billion (€6.6 billion and $9.1 billion) was set aside to establish the Independent Sector Treatment Centre (ISTC) programme to pump-prime the for profit private sector. 19 From 1 January 2006, patients in England were given a choice of at least four hospitals, or what were termed suitable alternative providers, in which to have their NHS-funded treatments, including ISTC and non-ISTC private hospitals. 20 Accompanying these waiting time policies was a commitment by the Labour government to reduce health inequalities. 21
Scotland
The responsibility for health is devolved from the UK government to the Scottish government and the response to the drive to reduce waiting times in Scotland was different. In February 2003, the ‘Partnership for Care’ NHS Scotland White Paper set out a clear strategy to ensure prompt access to services within a patient’s local NHS backed up by the right to be treated ‘elsewhere in the NHS, in the private sector, or in exceptional circumstances elsewhere in Europe’. 22 As in England, these waiting time guarantees, reiterated in the Patient Rights (Scotland) Act 2011, were accompanied with a commitment to reduce health inequalities. 23 A key element of this strategy was the purchase of the Golden Jubilee National Hospital in Clydebank, Greater Glasgow as a specialist centre for elective NHS surgery from private healthcare company Health Care International after its failure to develop it as a health tourism venture. Scotland did not follow England in the development of an ISTC programme until December 2006 when it opened an experimental ISTC, the Scottish Regional Treatment Centre (SRTC) in Tayside. 24 The contract to run the SRTC in the building of Stracathro NHS hospital was awarded to South African private healthcare company Netcare, which had already been awarded ISTC wave one contracts in England for mobile cataract surgery, a surgical centre in Manchester and a walk-in centre in Leeds worth £137.1 million (€162.7 million and $223.9 million). The SRTC closed its doors in January 2010 when the Scottish government decided against renewing the contract following an analysis showing poor value for money. 25
In this study, we use primary elective hip arthroplasty treatment rates, a commonly used proxy to detect change in healthcare access inequalities,6,8,10 to assess if there were any changes in geographical and socioeconomic inequalities in access to treatment after the introduction of waiting time initiatives in Scotland.
Methods
We analysed an extract of secondary care admissions Scottish Morbidity Record (SMR01) data provided by the Information Services Division (ISD) of NHS National Services Scotland of NHS funded elective primary hip arthroplasties (including hip resurfacing and hybrid hip replacements) from 1 April 1998 to the 31 March 2008 for patients over 15 years of age identified using OPCS-4.4 codes as used by the Scottish Arthroplasty Project. 26
We calculated age and sex directly standardised hip arthroplasty rates by year of treatment for all of Scotland and by period of treatment defined as the 5 years before (1 April 1998 to 31 March 2003) and after (1 April 2003 to 31 March 2008) the introduction of the waiting time initiatives by health board of residence and Scottish Index of Multiple Deprivation (SIMD) quintile further adjusted by SIMD and health board, respectively.
We tested for an interaction between period of treatment and health board and separately, period of treatment and SIMD. We calculated age, sex and SIMD adjusted incidence rate ratios by health board and age, sex and health board adjusted incidence rate ratios by SIMD using Greater Glasgow and Clyde (the largest and most socioeconomically deprived of Scotland’s 14 geographical health boards) and SIMD quintile five (the most socioeconomically deprived fifth of Scotland) as reference categories, respectively, by period of treatment.
Finally, using a separate updated data-set from ISD which contained data on provider type (NHS or private), we analysed the change in distribution of NHS-funded patients treated in public and private hospitals by calculating the proportion of NHS-funded elective hip arthroplasties carried out in the private sector in the year prior to the waiting time initiatives, financial year 2002–2003 (1 April 2002 to 31 March 2003) and 5 years later in 2007–2008.
Our denominators were age- and sex-specific populations over 15 years of age from mid-year Scottish population estimates from the General Register Office for Scotland. Scottish population data by SIMD and health board were provided by ISD. Socioeconomic deprivation was measured using the SIMD scores for 2006 supplied by ISD where quintile one represents the least deprived fifth and quintile five the most deprived fifth of the Scottish population. To ease analysis and interpretation we combined the island health boards, Orkney, Shetland and Western Isles; for simplicity this is referred to throughout as one health board although actually comprising three health boards. All rates were directly standardised to the 1997 Scottish mid-year population. All incidence rate ratios were estimated using Poisson regression in the statistical package Stata version 12.1.
Results
There were 47,069 NHS-funded elective primary hip arthroplasties carried out in Scotland for the 10-year period 1 April 1998 to 31 March 2008 identified from data returned to ISD. The age and sex adjusted treatment rate fell from 106.3 (95% confidence interval 103.0, 109.5) per 100,000 Scottish population in 1998–1999 to 99.0 (95.9, 102.1) per 100,000 in 2001–2002, rose to 147.3 (143.6, 151.0) per 100,000 in 2006–2007 before falling to 138.7 (135.1, 142.2) per 100,000 in 2007–2008 (see Figure 1). There was a 42% increase in NHS hip arthroplasties carried out in Scotland from 4095 in 2002–2003 to 5829 in 2007–2008.
Elective primary hip arthroplasties in NHS-funded patients in Scotland (aged over 15 years). Total arthroplasties and arthroplasty rates directly standardised by age and sex, 1 April 1998 to 31 March 2008.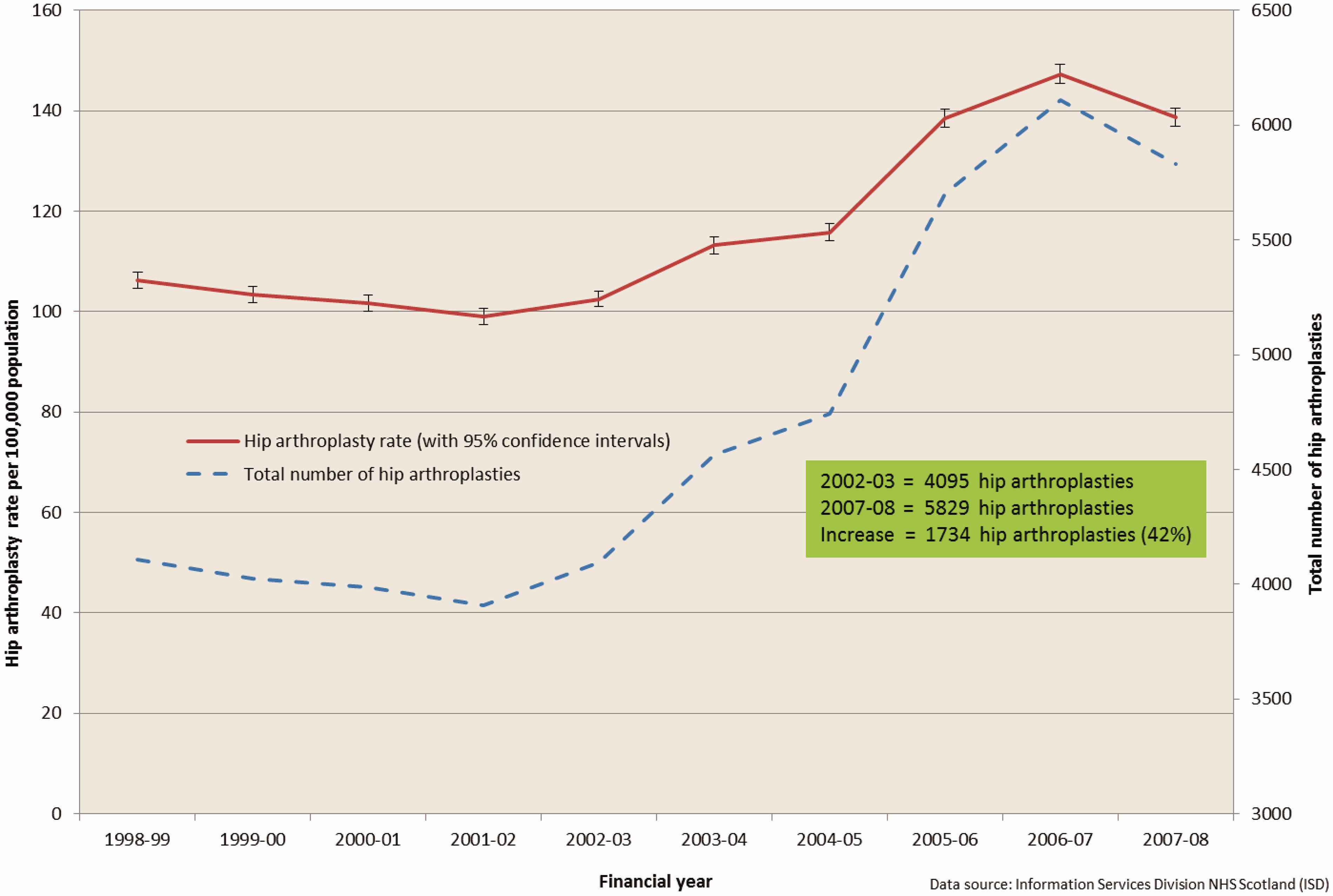
Scotland health board populations (over 15 years), elective primary hip arthroplasty rates and incidence rate ratios (relative to Greater Glasgow and Clyde), before (1 April 1998–31 March 2003) and after (1 April 2003–31 March 2008) the introduction of waiting time initiatives.
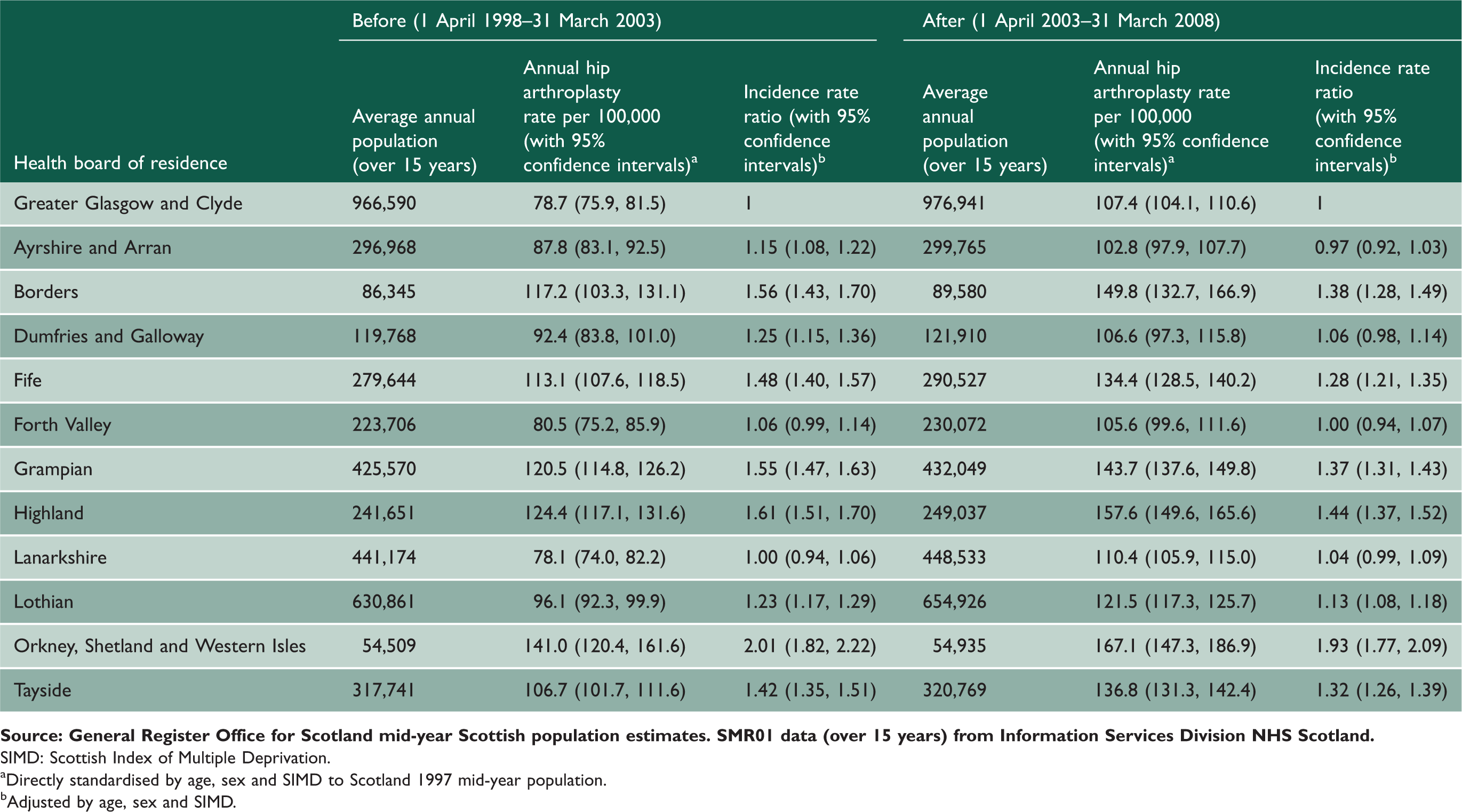
SIMD: Scottish Index of Multiple Deprivation.
Directly standardised by age, sex and SIMD to Scotland 1997 mid-year population.
Adjusted by age, sex and SIMD.
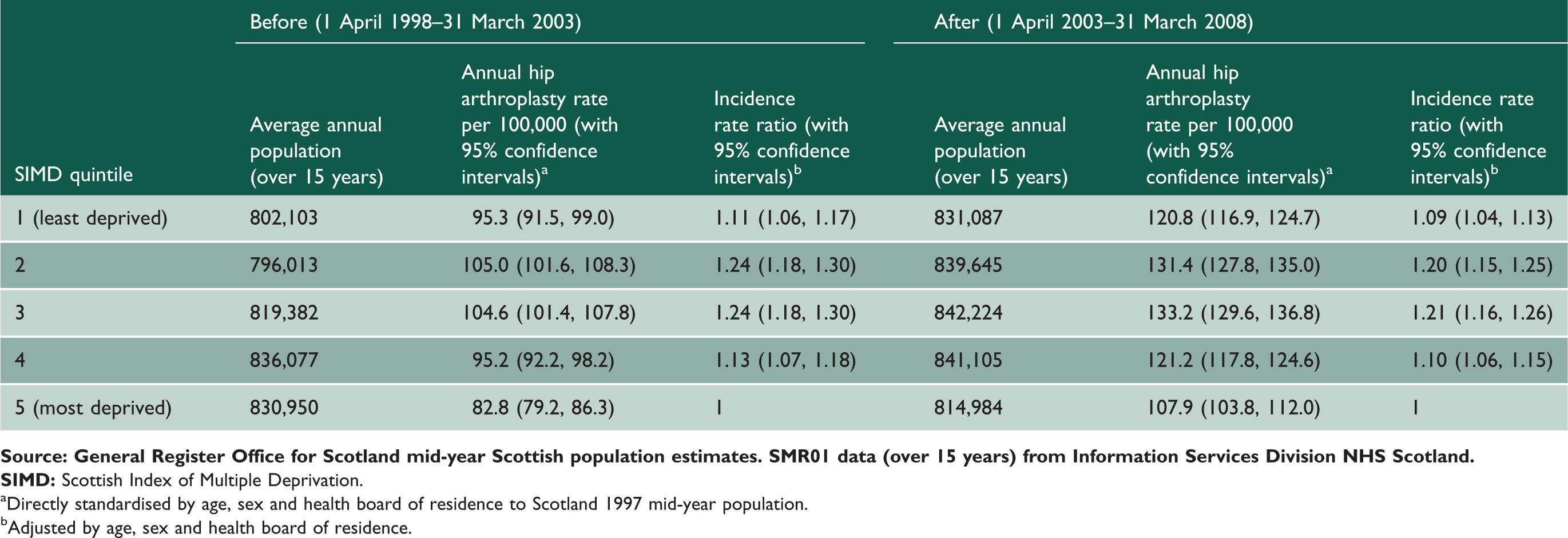
Hip arthroplasty rates were statistically significantly lower among the most socioeconomically deprived quintile of the Scottish population (SIMD quintile five) than among the other quintiles both in the 5 years before and after the 1 April 2003, 82.8 (79.2, 86.3) per 100,000 and 107.9 (103.8, 112.0) per 100,000, respectively.
There was a significant interaction between health board and period of treatment (likelihood ratio test p < 0.001) indicating that treatment rates in other health boards were significantly higher than Greater Glasgow and Clyde in the 5 years before the 1 April 2003 compared with the 5 years after the 1 April 2003. In the 5 years before 1 April 2003 there were nine health boards (Table 1, Figure 2) with significantly higher treatment rates than Greater Glasgow and Clyde, only Forth Valley and Lanarkshire were not significantly different, whereas in the 5 years after 1 April 2003 only seven health boards had significantly higher treatment rates than Greater Glasgow and Clyde, with Ayrshire and Arran, Dumfries and Galloway, Forth Valley and Lanarkshire not significantly different.
Elective primary hip arthroplasties in NHS-funded patients in Scotland (aged over 15 years). Incidence rate ratios adjusted by age, sex and Scottish index of multiple deprivation with 95% confidence intervals compared with greater Glasgow and Clyde health board.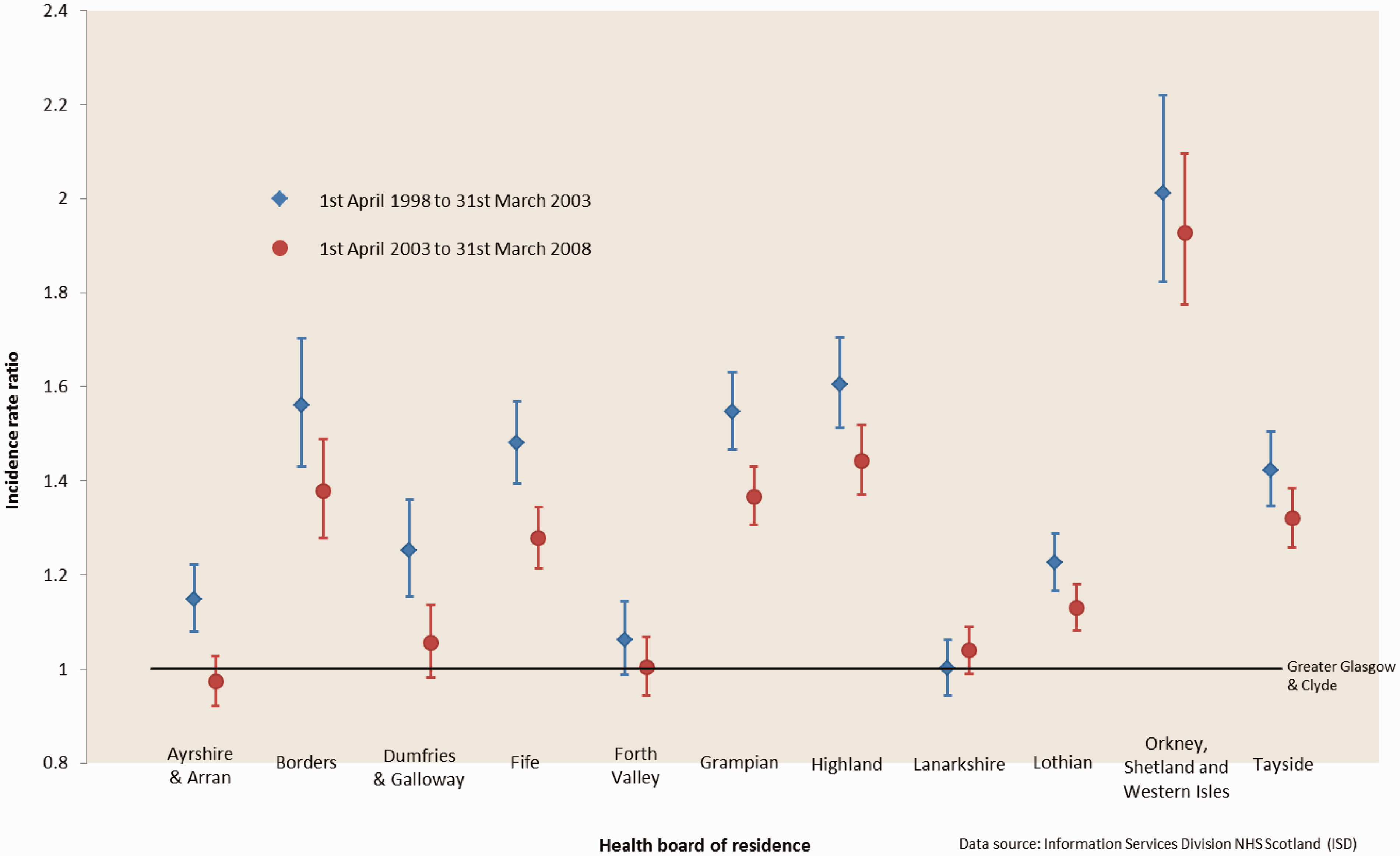
In four health boards, Ayrshire and Arran, Dumfries and Galloway, Fife and Grampian the incidence rate ratio relative to Greater Glasgow and Clyde decreased significantly for the 5 years after 1 April 2003 compared with the 5 years before 1 April 2003 (Table 1, Figure 2).
We found weak evidence of an interaction between SIMD and period of treatment (likelihood ratio test p = 0.108) but no evidence that the incidence rate ratios for SIMDs one to four relative to SIMD five in the 5 years after 1 April 2003 were significantly different to those calculated for the 5 years before 1 April 2003 (Table 2, Figure 3).
Elective primary hip arthroplasties in NHS-funded patients in Scotland (aged over 15 years). Incidence rate ratios adjusted by age, sex and health board of residence with 95% confidence intervals compared with the 20% most socioeconomically deprived population (SIMD 5). Scotland socioeconomic deprivation (SIMD) quintile populations (over 15 years), elective hip arthroplasty rates and incidence rate ratios (relative to SIMD five), before (1 April 1998–31 March 2003) and after (1 April 2003–31 March 2008) the introduction of waiting time initiatives.
Directly standardised by age, sex and health board of residence to Scotland 1997 mid-year population. Adjusted by age, sex and health board of residence.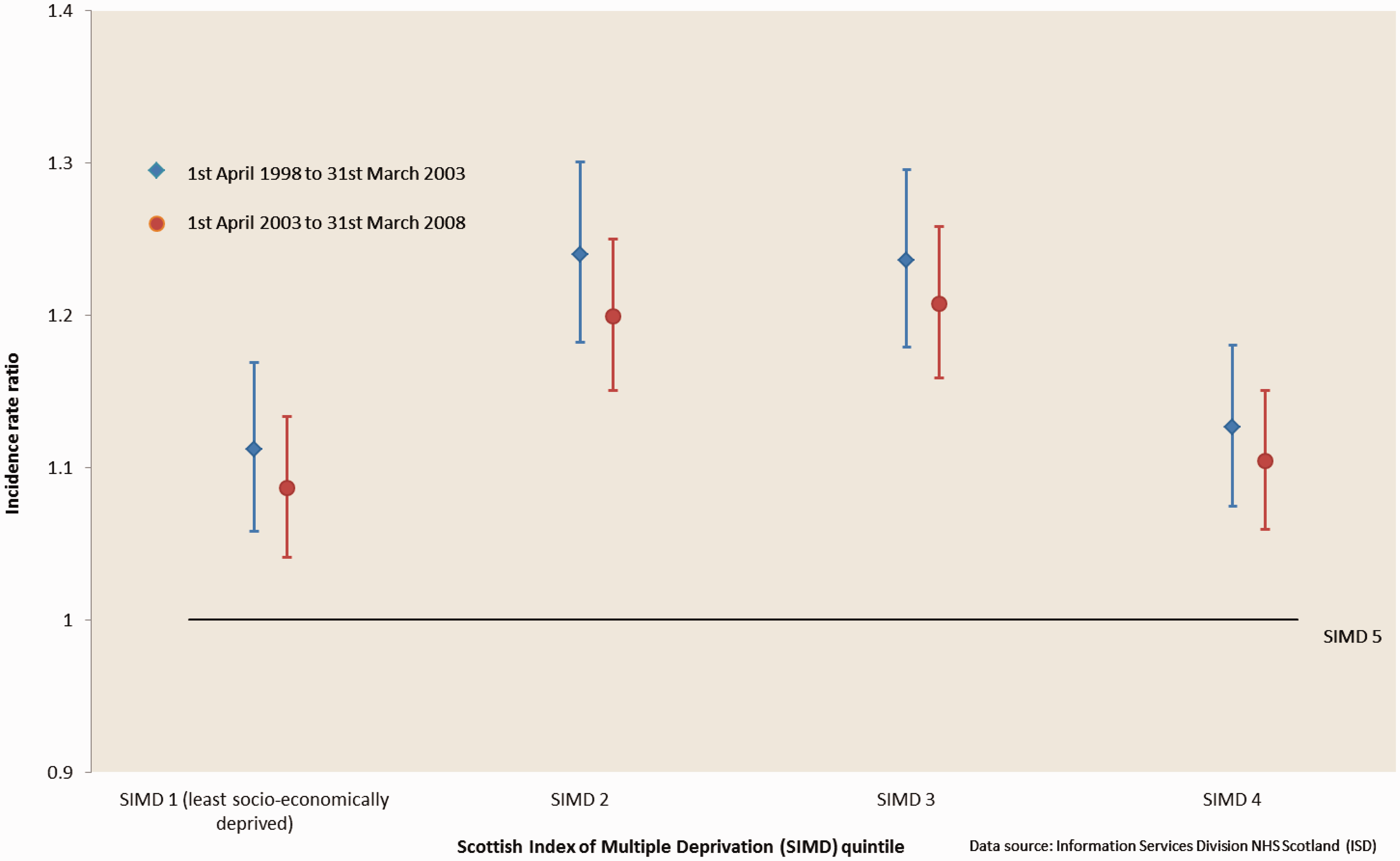
According to the separate updated data-set from ISD, the proportion of NHS-funded elective primary hip arthroplasties conducted in the private sector increased from 1.1% in 2002–2003 to 2.9% in 2007–2008. The NHS Golden Jubilee National Hospital in Clydebank (NHS National Waiting Times Centre Board) increased its share from 3.3% to 10.6% over the same period.
Discussion
We have found evidence of a statistically significant reduction in geographical inequality in elective primary hip arthroplasty treatment rates between health boards in Scotland in the 5 years after the introduction of waiting time initiatives in 2003 compared with 5 years before. We did not find any significant reduction in inequality by socioeconomic deprivation.
Research into access to NHS treatment in England between 2001 and 2008 has also found no reduction in socioeconomic inequality in hip arthroplasty treatment during this period of waiting time initiatives and NHS reforms. 10 Earlier research in one health board in Scotland has suggested that waiting time initiatives introduced there have not discriminated against patients from lower socioeconomic groups. 27 There has been no research into possible changes in geographical inequalities in either England or Scotland following the waiting time initiatives, although this is problematic in England due to frequent changes in NHS organisation and boundaries. Moreover, in England, there has been a deterioration in data quality and completeness because the private sector does not return complete, timely and accurate data. In contrast, health board boundaries in Scotland are more stable which facilitates geographical comparisons over time.
The reduction in geographical inequality we found in Scotland has taken place without any major expansion in the use of the private sector to deliver NHS treatments and may be as a result of increased NHS activity, in particular the major investment at the NHS Golden Jubilee National Hospital in Clydebank. The model chosen in Scotland to increase capacity within the NHS was very different from that followed in England where a major ISTC programme and extension of patient choice took place such that by 2010–2011, around 20% of all NHS-funded hip arthroplasties were being carried out in private hospitals. 28 In Scotland, in 2010–2011 only 0.8% of NHS-funded hip arthroplasties were performed privately down from a peak of 8.3% in 2008–2009 when the SRTC was most active. There is a need for an analysis in England to assess any change in geographical inequality which would make a useful comparison with the experience in Scotland although this is difficult for the reasons outlined above.
There are few studies of employment and risk of hip osteoarthritis, the main reason for a hip arthroplasty, but farming and agricultural labourers have an increased risk which may explain some of the rural/urban differences pattern.29,30 We were unable in this study to adjust for need for treatment or to adjust for any measure of co-morbidity. Factors contributing to the observed differences in treatment rates between health boards in Scotland might include competing priorities on limited budgets but might also include differing levels of need within geographical populations. The reduction we found in geographical inequality suggests that previously unmet need is being met as a result of increased capacity but more research is needed to understand why there has been no impact on socioeconomic inequality.