
Abstract
Objectives
Medical schools need to ensure that graduates feel well prepared for their first medical job. Our objective was to report on differences in junior doctors’ self-reported preparedness for work according to gender, ethnicity and graduate status.
Design
Postal and electronic questionnaires.
Setting
UK.
Participants
Medical graduates of 2008 and 2009, from all UK medical schools, one year after graduation.
Main outcome measures
The main outcome measure was the doctors’ level of agreement with the statement that ‘My experience at medical school prepared me well for the jobs I have undertaken so far’, to which respondents were asked to reply on a scale from ‘strongly agree’ to ‘strongly disagree’.
Results
Women were slightly less likely than men to agree that they felt well prepared for work (50% of women agreed or strongly agreed vs. 54% of men), independently of medical school, ethnicity, graduate entry status and intercalated degree status, although they were no more likely than men to regard lack of preparedness as having been a problem for them. Adjusting for the other subgroup differences, non-white respondents were less likely to report feeling well prepared than white (44% vs. 54%), and were more likely to indicate that lack of preparedness was a problem (30% non-white vs. 24% white). There were also some gender and ethnic differences in preparedness for specific areas of work.
Conclusions
The identified gender and ethnic differences need to be further explored to determine whether they are due to differences in self-confidence or in actual preparedness.
Introduction
An important task for medical schools is to ensure that graduating doctors feel prepared, as best they realistically can, for their first medical job. We have reported previously on the extent to which UK-trained doctors in their first year of medical work felt well prepared and have focused, in particular, on differences between medical schools.1,2 In this paper, we report on whether there are differences in perceived preparedness between men and women, different ethnic groups and by graduate status at entry to medical school. We update earlier findings on these subgroups, from surveys of qualifiers in 1999, 2000, 2002 and 2005,2,3 and present findings here from the UK-trained graduates of 2008 in 2009 and of 2009 in 2010. As in many other countries, numbers and percentages of women graduating from UK medical schools have substantially increased over the past decade. 4 The UK medical student body is more ethnically diverse than the general population.4,5 Graduate entry to medical school has also increased. 6 These changes underline the importance of awareness of any differences between these subgroups in how well prepared they feel for work. Our aim was to determine whether there were any important differences in self-reported preparedness comparing men and women, ethnic groups, and graduate and non-graduate entrants.
Method
Design, participants and materials
The UK Medical Careers Research Group undertakes surveys of career intentions and progression, and views about training and working in medicine, from medical qualifiers of all medical schools in the UK in selected cohorts defined by year of qualification. Details of its methods can be found elsewhere. 1 Contact details were provided by the General Medical Council for all registered graduates of 2008 and 2009 who had given their permission to be surveyed. The graduates were surveyed towards the end of their first postgraduate (F1) year; non-respondents received up to five reminders.
The survey included the following statement about feeling prepared for work: ‘My experience at medical school prepared me well for the jobs I have undertaken so far’, to which respondents were asked to reply on a five-point scale from ‘strongly agree’ to ‘strongly disagree’. Those who specified anything other than agree or strongly agree, were asked ‘Was lack of preparation a serious, medium-sized or minor problem for you?’. We also asked the doctors to indicate in which areas they did not feel well prepared, selecting from ‘clinical knowledge’, ‘clinical procedures’, ‘administrative tasks’, ‘interpersonal skills’ and ‘physical/emotional/mental demands’.
Analysis
We explored the data using simple cross-tabulation. We then used binary logistic regression to study the association between questionnaire responses and gender, ethnicity, graduate status at entry to medical school, and having an intercalated degree (a research degree taken during medical school in addition to the final medical degree), controlling each for the other three and for medical school. Binary dependent variables were constructed by, for example, combining respondents who agreed or strongly agreed that medical school had prepared them well, as one group, and all other responses as the second group. First, logistic regressions were performed predicting whether the respondents: (1) agree or not, (2) disagree or not that their medical school prepared them well for the jobs they have undertaken so far; and (3) whether lack of preparation was perceived to be a problem (serious or medium-sized problem vs. other responses). Medical school, sex, ethnicity (white vs. non-white), graduate entry status and intercalated degree status were entered as predictors. We then, in similar ways, compared (4) strongly agree with disagree and strongly disagree and neither agree nor disagree, combined, and (5) strongly disagree with agree and strongly agree and neither agree nor disagree, combined.
Since multiple similar analyses were performed on the same dataset, we regarded the attainment of a level of significance of P ≤ 0.01 as evidence of real difference.
Results
Response rates
Excluding medical graduates who were deceased, declined to participate or were untraceable, the overall response rate was 49% (3302/6705) for the 2008 cohort and 47% (2918/6252) for the 2009 cohort. However, the fifth postal mailing of the surveys contained a shortened version of the questionnaire, which did not include the questions regarding preparedness for work. Therefore, the response on this specific topic was 41.4% (5369/12967).
Feeling prepared for clinical work and extent to which lack of preparation was a problem
For ease of initial presentation, agree and strongly agree responses were combined into a single ‘agree’ category and disagree and strongly disagree responses were combined into a single ‘disagree’ category.
Of the 2008 and 2009 graduates combined, 51.3% agreed that their medical school prepared them well for the jobs they have undertaken so far, 30.1% neither agreed nor disagreed and 18.5% disagreed. Lack of preparedness was considered to have been a serious problem by 2.7% of respondents and a further 22.6% specified it as a medium-sized problem.
Subgroup differences
Percentage of doctors who agreed, or disagreed, that their medical school prepared them well for work; and percentage who considered that lack of preparedness as a problem (serious or medium-sized) one year after graduation.
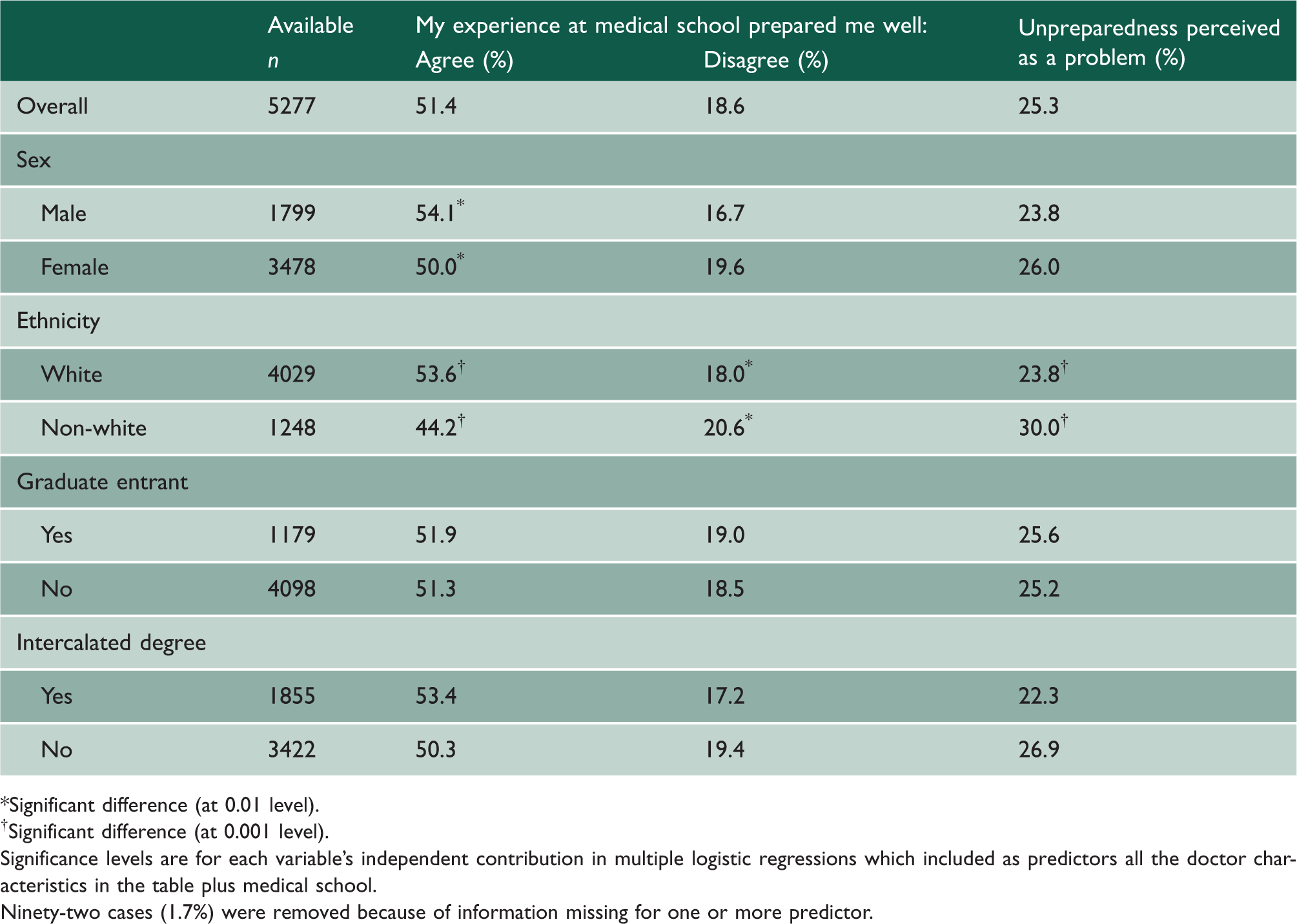
Significant difference (at 0.01 level).
Significant difference (at 0.001 level).
Significance levels are for each variable’s independent contribution in multiple logistic regressions which included as predictors all the doctor characteristics in the table plus medical school.
Ninety-two cases (1.7%) were removed because of information missing for one or more predictor.
Medical school was a significant independent predictor in all regressions (as previously reported by us 1 and Table 3).
Unadjusted numbers and percentages for subgroup comparisons are available in Appendix 1.
We also found that, adjusting for other factors, white doctors were more likely than non-white doctors to strongly agree that they felt well-prepared for work (17% and 12%, respectively, Wald χ21 = 9.3, P = 0.002). Men were more likely to strongly agree than women (18% vs. 15%), though the difference did not quite reach significance (Wald χ21 = 5.6, P = 0.017). None of the subgroup variables, apart from medical school, were a significant independent predictor of strongly disagree responses. However, these were very uncommon (2.6% of all doctors).
Areas in which respondents did not feel well prepared
Differences between subgroups of doctors in the percentages that indicated feeling unprepared in five particular areas of work one year after graduation and the significance of the groupings as independent predictors of feeling unprepared in each area.
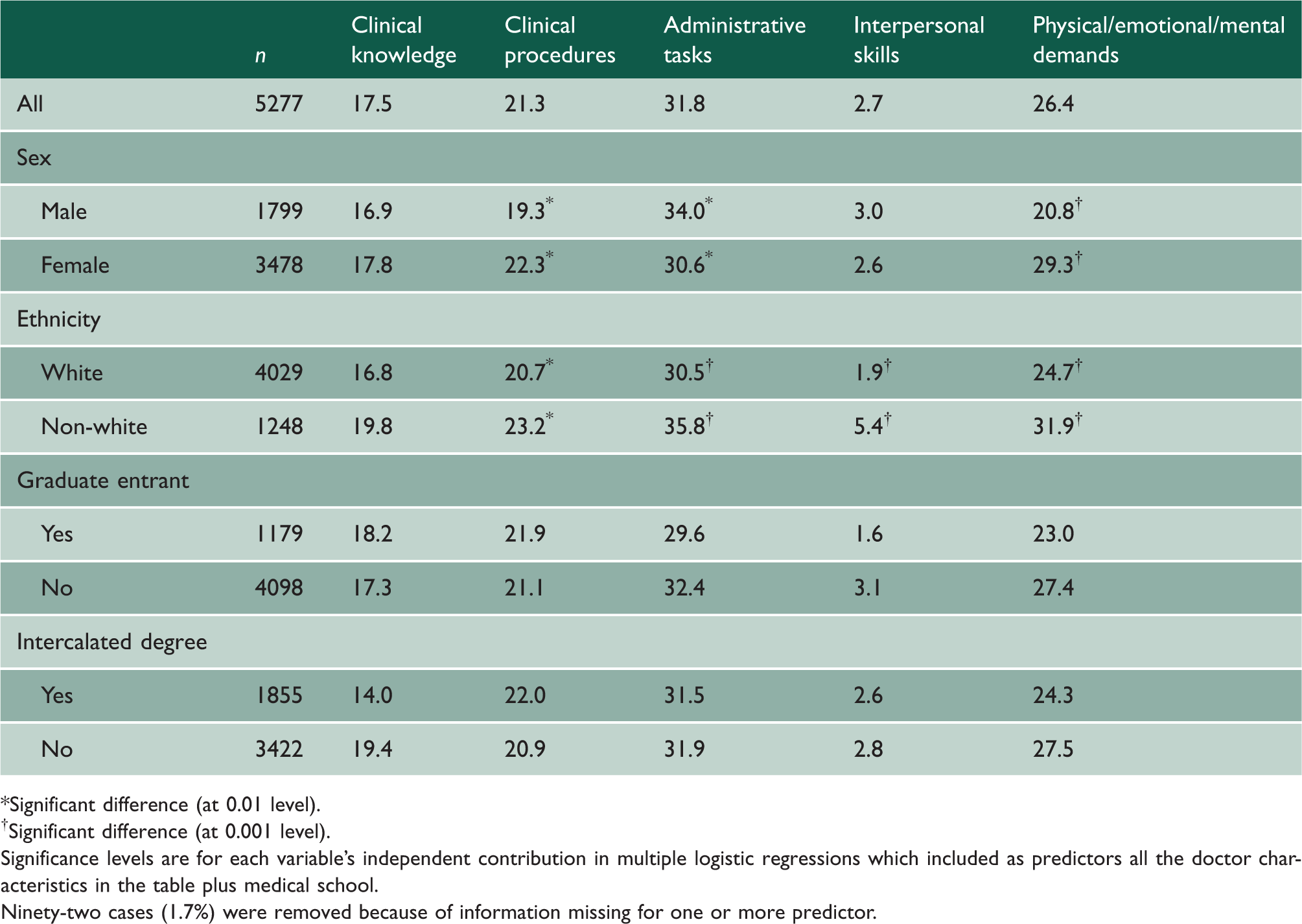
Significant difference (at 0.01 level).
Significant difference (at 0.001 level).
Significance levels are for each variable’s independent contribution in multiple logistic regressions which included as predictors all the doctor characteristics in the table plus medical school.
Ninety-two cases (1.7%) were removed because of information missing for one or more predictor.
Logistic regression results: contribution of sex, ethnicity, intercalated degree status, graduate entry and medical school to outcomes related to medical graduates’ preparedness for work.
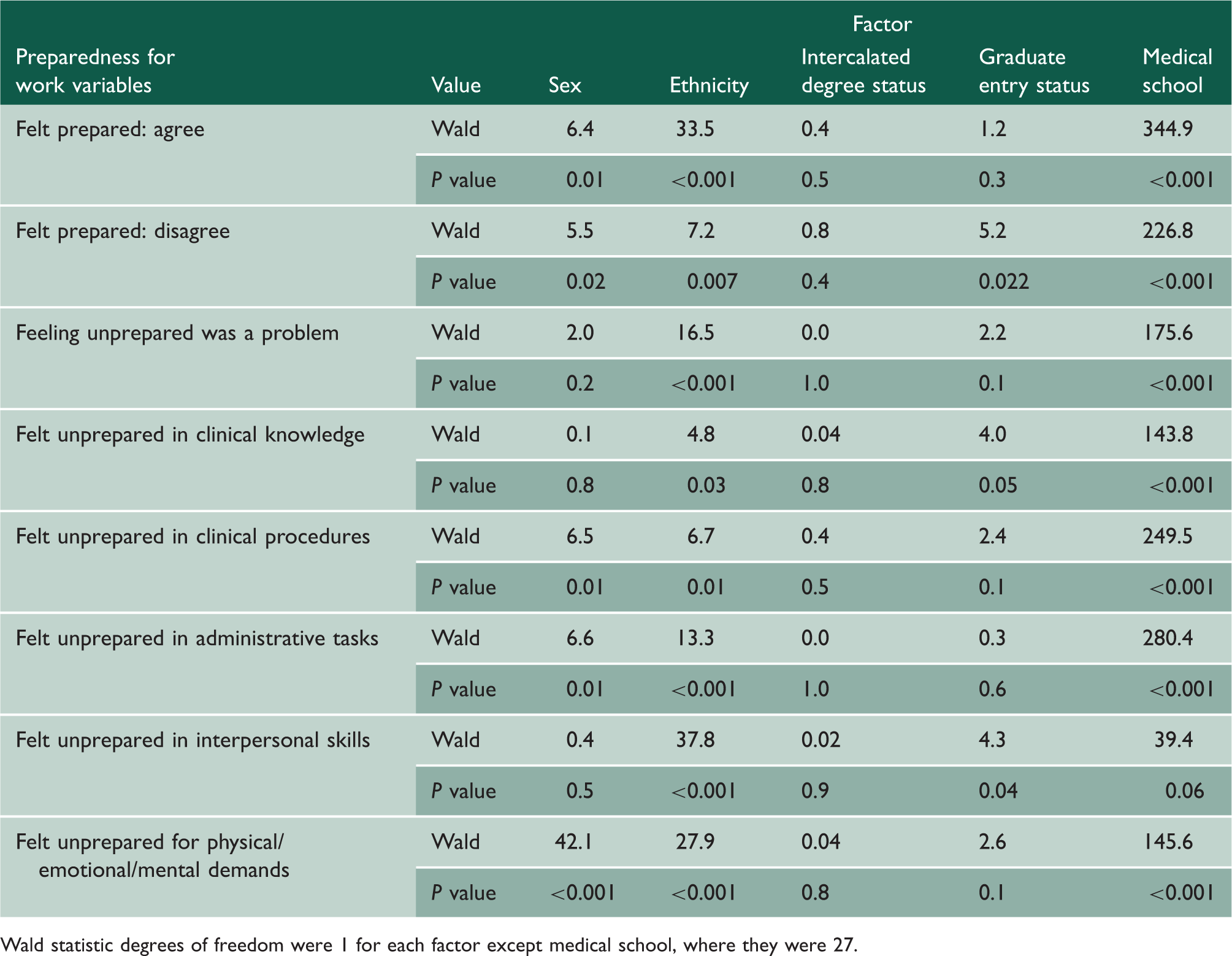
Wald statistic degrees of freedom were 1 for each factor except medical school, where they were 27.
Logistic regression was performed for each of the investigated areas to determine which doctor characteristics were associated with finding the area problematic (while adjusting for the other characteristics). There were no significant differences between men and women, or ethnic groups, or other categories, in feeling prepared in respect of clinical knowledge (Table 2). A significantly higher percentage of non-whites than whites felt unprepared in respect of clinical procedures, administrative tasks, interpersonal skills and physical/mental/emotional demands. A significantly higher percentage of women than men felt unprepared in respect of clinical procedures and physical/emotional/mental demands; and a significantly higher percentage of men than women felt unprepared in respect of administrative tasks (Table 2). Differences between graduates and non-graduates and between those with or without intercalated degrees were not significant. Medical school was a significant and very substantial independent predictor for all specific areas with the exception of interpersonal skills (Table 3).
Further investigation into the differences between the ethnic groups
We conducted further analyses to explore whether the lower level of preparedness reported by non-white students may be due to language problems, cultural adjustment or other factors.
First, we repeated the analysis of the association between ethnicity and the preparedness for work variables, restricting the analysis to doctors who were UK home students when they entered medical school (n = 5112), as defined by family home and fee status. The general pattern of results remained the same as shown in Tables 1 to 3.
Percentages of doctors feeling prepared for work and percentages for whom lack of preparedness was a problem by detailed ethnicity group.
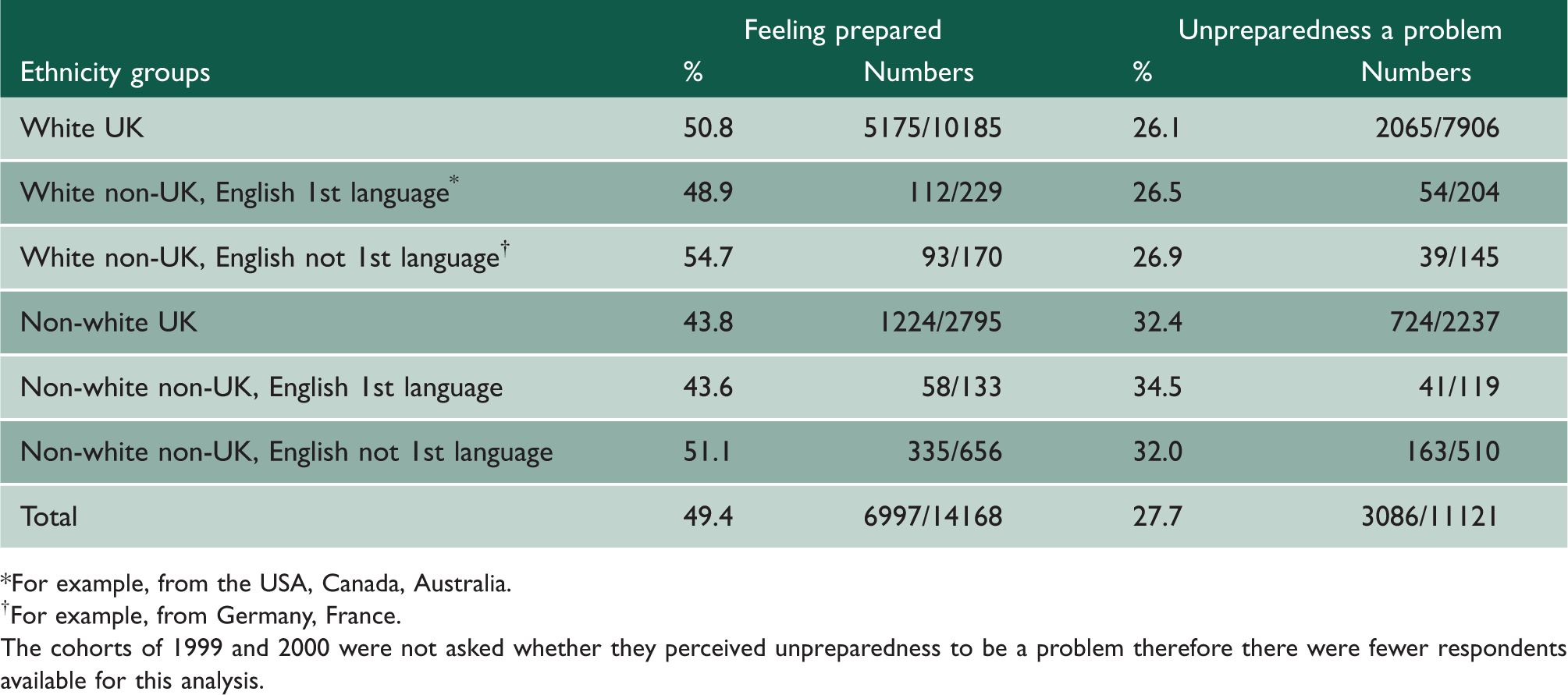
For example, from the USA, Canada, Australia.
For example, from Germany, France.
The cohorts of 1999 and 2000 were not asked whether they perceived unpreparedness to be a problem therefore there were fewer respondents available for this analysis.
The figures in Table 4 indicate that non-white respondents from the UK and other English-speaking countries were the least likely to agree that their medical school prepared them well for work. All non-white groups had a higher percentage of respondents reporting lack of preparedness to be a serious or medium-sized problem than the white respondent groups.
Chi-squared tests showed that the differences between ethnic and language groups were significant both for preparedness for work (χ25 = 47.7, P < 0.001) and for specifying that unpreparedness was a problem (χ25 = 41.6, P < 0.001). Examination of residuals revealed that in both cases the most notable difference was between white UK and non-white UK groups.
Discussion
Main findings
We have found small but significant differences in self-reported preparedness for work between men and women and between white and non-white F1 doctors, but we found no differences between those who entered medical school as a graduate and others or between those who did and those who did not do an intercalated degree.
Women were slightly less likely than men to feel well prepared for work, independently of medical school, ethnicity, graduate entry status and intercalated degree status. Considering specific work areas, women were notably more likely to feel unprepared for physical, emotional and/or mental demands of medical work and slightly more likely than men to feel unprepared in the area of clinical procedures. Men were a little more likely than women to feel unprepared for administrative tasks.
Non-white respondents were less likely to feel well prepared, and more likely to indicate that lack of preparedness was a problem, than white respondents after controlling for other factors. Non-white doctors were more likely than whites to report feeling unprepared in four of the five investigated areas of work, the exception being clinical knowledge where there was no significant difference by ethnicity.
The pattern of results remained after excluding graduates who came from non-UK homes. Thus, language and/or ‘culture shock’ are unlikely to account for the differences between white and non-white graduates. This conclusion is supported by the additional analysis reported in Table 4. It indicates that the groups that might experience language difficulties, white and non-white doctors from non-English speaking countries, actually showed the highest levels of agreement with the statement about feeling well prepared for work. Thus, more complex social/cultural factors must be involved in the ethnic differences found.
The gender and ethnic differences were small in comparison with the large differences between medical schools indicated by figures in Table 3 and reported elsewhere. 1
Strengths and limitations
The study includes the views of a very large number of recently qualified junior doctors studied on a national scale. As with all surveys, the results may be susceptible to non-respondent bias. In order to ascertain whether there is likely to be non-respondent bias, we compared the preparedness responses of those who replied to the first or second survey mailing and those who only replied to one of the subsequent mailings, on the grounds that, if we had not persevered past two mailings, those who responded after two would otherwise have been non-respondents. We found no difference in ‘preparedness for work’ between early and late respondents. 1
In the analysis reported in Table 4, the sizes of some comparison groups were relatively small and statistical power may have been low.
Interpretation
Two systematic reviews, one on the effectiveness of self-assessment as motivators for change in learning behaviour 7 and one on the accuracy of physicians’ self-assessment of competence 8 concluded that the evidence base for the accuracy of self-assessment of competence was mixed. We therefore suggest a cautionary note in the interpretation of our results. Self-reported preparedness for work might indicate the actual levels of preparedness or it might reflect respondents’ confidence (or lack of it) or their self-awareness. These explanations could only be distinguished by the use of objective testing alongside self-reported responses.
Gender
Recent research overwhelmingly concludes that women outperform men in academic and clinical assessments at medical school.9–11 Thus, there is little reason to suppose that female students leave medical school less prepared than men for work. On the other hand, there are well-documented gender differences in personality, which could result in gender differences in self-evaluation. Women tend to score higher than men on neuroticism 12 and anxiety, 13 and tend to score lower than men on measures of self-esteem. 14 There is evidence that some female medical students tend to be more anxious and less self-confident than their male colleagues. 15 Furthermore, Blanch-Hartigan, 16 in her recent review of medical students’ self-assessment of performance, summarizes the evidence that female students underestimate their performance more than male students. Thus, the significant gender differences in our study may be explained by some women trainee doctors underestimating their levels of preparedness (or some men overestimating theirs). This explanation fits well with the finding that, out of the five work areas investigated, the biggest gender difference was found for physical/emotional/mental demands of working as a doctor.
Ethnicity
It has been well documented that some non-white UK medical students perform less well academically than white students.17,18 This conclusion extends to different types of examinations including clinical assessments.10,17 Thus, unlike the case of gender, there are some grounds to suspect that differences in self-reported preparedness may reflect actual differences in preparedness for work between white and non-white F1 doctors. However, as with gender, the responses may also reflect differences between subgroups in self-confidence or self-awareness. There has been remarkably little research conducted in the UK on the ethnic differences in doctors’ self-confidence and self-esteem.
We consider, briefly, why such ethnic differences might emerge. Seabrook 19 followed up an ethnically mixed group of students during their five years of studies at a UK medical school, collecting data from them through focus groups and in-depth interviews. Non-white students reported no overt discrimination but felt that they were treated differently in subtle ways. In medicine, apprenticeship-type training plays an important role in the acquisition of skills and competence. Therefore, differential treatment from the educators starting from medical school and presumably continuing throughout hospital and specialized training could result in differences in performance. Roberts et al. 20 conducted focus groups with medical students at two British universities. The focus groups explored the issues of ‘ethnicity’ and ‘culture’, among others. As in Seabrook’s study, non-white students raised the issue of being viewed as ‘different’. Roberts et al. postulate that such perceptions may result in some non-white students staying in the ‘periphery’ in medical school and not fully coming into their own.
Another factor may be cultural differences in the expectations of what working in the medical profession entails. Woolf et al. 21 describe an existing stereotype of a typical Asian clinical medical student, which includes characteristics such as over-reliance on books and poor communication with patients. The existence of such a stereotype suggests that some non-white students may be focusing too much on their clinical knowledge and skills, to the detriment of the other aspects of being a doctor, because while they are in medical school they perceive the latter to be less important. Some studies in Britain 22 and the US 23 suggest that non-white students adopt a different communication style from whites, when examining patients, which is not quite so patient-centred. In our study, the areas in which a higher percentage of non-white than white respondents felt unprepared were administrative tasks, physical, emotional and mental demands and interpersonal skills, rather than clinical knowledge.
Conclusions
Although the gender and ethnic differences we have identified are small in comparison with differences in self-reported preparedness between medical schools, medical educators need to be aware of them and consider steps to remedy them.