
Abstract
Objective
Rest and Recuperation (R&R) is a period of home leave taken during an operational deployment; we sought to examine the relationship between taking R&R and mental health.
Design
A survey-based post-intervention evaluation.
Setting
UK
Participants
232 members of the UK Armed Forces; 42 of which completed pre and post R&R surveys.
Main Outcome Measures
Alcohol use, Post Traumatic Stress Disorder, Common Mental Disorder Symptoms and R&R experiences.
Results
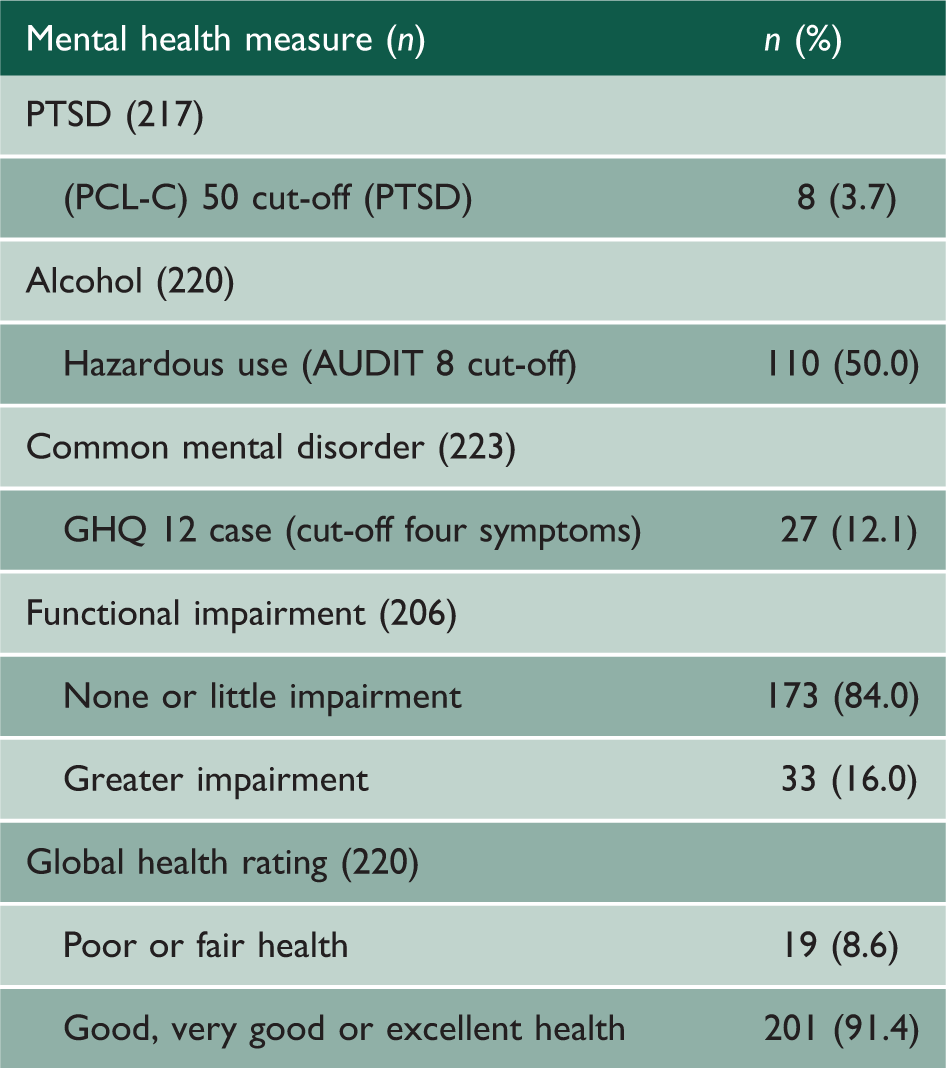
12.1% of respondents (n=27) reported symptoms of common mental disorder and 3.7% (n=8) reported probable PTSD. 50.0% (n=110) reported hazardous use of alcohol during R&R. In the pre- and post-assessed sample, mental health status and alcohol use levels were similar at both survey points. Using principal component analysis, five components of R&R were identified; mentally switching off from deployment, travel experience, physical recovery, relaxation, rest and social support. R&R was extremely popular and although it did not improve mental health overall, the ability to engage with or derive satisfaction from aspects of the five components was significantly associated with better mental health and less alcohol use at the end of R&R.
Conclusion
Operational commanders should advise personnel about the best way to actively engage with R&R before they leave theatre and be aware of the significant detrimental impact of disrupted travel arrangements upon the ability to benefit from R&R.
Introduction
Historically, armed forces have attempted to mitigate the cumulative fatigue arising from operations by providing a period of rest during the deployment. Currently, United Kingdom Armed Forces (UKAF) personnel deploying for six months or more receive a single continuous 10-day period of R&R at some point during their deployment. This includes travel to and from the place of departure and arrival within the operational theatre. 1 The stated aim of R&R is to ‘provide those who have been mentally and physically challenged by continuous operational service, time to rest out of the line and “recharge their batteries” in order to sustain operational effectiveness’. Military mental health studies suggest that R&R is popular and similar policies are widely implemented by other coalition nations. 2 The only published research on this topic considered United States personnel deployed to Bosnia in the 1990s which found no long-term benefits of R&R; 3 there is no current empirical evidence of a beneficial effect for R&R in UK personnel.
In civilian settings, rest and holiday-taking are much cherished and are thought to boost morale and reward employees, particularly those in high-stress occupations; however, there is little outcome data suggesting that there is an enduring positive psychological effect for holidaying. 4 Nawijn 4 reports that mood gradually improves mid-holiday with the maximal effect occurring just before going home; travel was reported as being the most stressful part of a holiday. Taris et al. 5 demonstrated that high levels of overtime were linked to adverse health outcomes and, although holidaying helped with physical recovery and general wellbeing, 6 the effects were short-lived. 7 A recent review of UK Offshore Oil work schedules noted that while the typical offshore rota allowed for over 26 weeks onshore, taking less frequent but longer breaks was associated with difficulty re-adjusting to oil platform work routines whereas short breaks were not.
The main aims of the current study were to examine whether taking R&R was associated with mental health status and to identify the elements of R&R associated with better deployment of mental health. While the findings derive from a sample of military personnel, we suggest that they may have implications for other organizations that deploy their staff away from home for prolonged periods of time.
Method
This study was approved by the Ministry of Defence Research Ethics Committee (MODREC, No V.6 149/Gen/10 dated 16 January 2011). Initial focus groups were conducted among infantry soldiers who had recently taken R&R to establish survey content. After establishing content validity using Cronbach’s alpha, the final scale consisted of 30 items which were rated using a four-point Likert scale indicating strength of agreement (details available from the authors). Study participants were UKAF personnel deployed to Afghanistan in 2011. The survey was administered as personnel returned to the operational theatre following a period of 10–14 days of R&R.
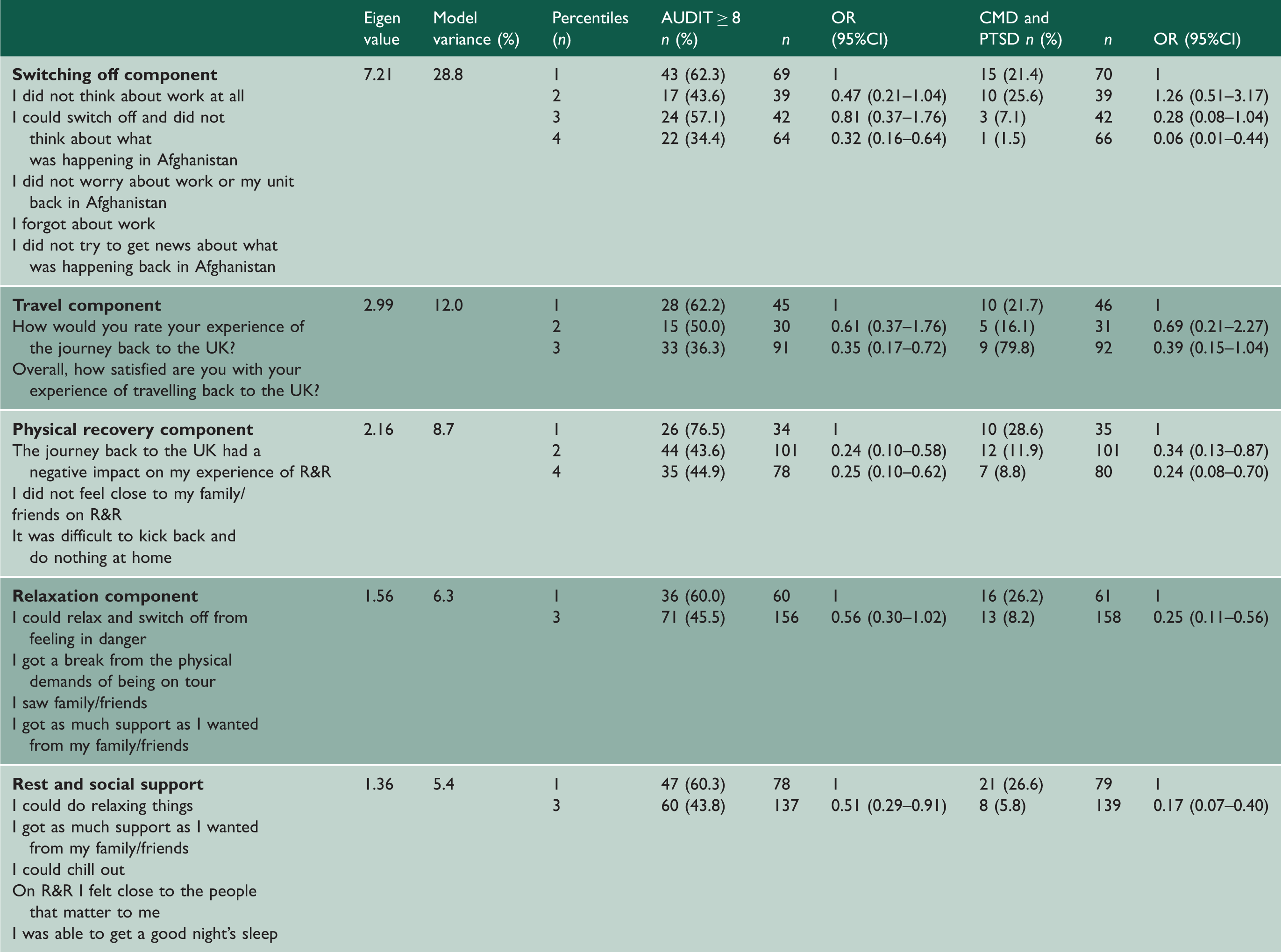
To identify patterns in the R&R experiences scale, principle components analysis (PCA) was conducted using 25 items which enquired about various aspects of R&R activity extracted from completed questionnaires. This process generated five components. Five additional satisfaction-based items which enquired about the overall experience of R&R were not entered into the PCA but were analyzed separately.
The survey asked about sociodemographic, operational and military factors; exposure to 17 combat and operational events, 8 a single item regarding perceptions of impending death or serious injury and R&R experiences. Common mental disorders (CMD) were measured using the 12-item General Health Questionnaire 9 (GHQ12), post-traumatic stress disorder (PTSD) symptoms using the Post-Traumatic Stress Disorder Checklist Civilian Version 10 (PCL-C), one item from the Medical Outcomes Study 36-item short-form health survey11 gauged functional impairment resulting from the mental health symptoms; usual alcohol use was assessed with the 10-item Alcohol Use Disorders Identification Test (AUDIT) 12 for those completing pre R&R measures. Consumption of alcohol is prohibited during deployment and the timeframe used in the AUDIT which enquires about alcohol use in the last year was therefore considered inappropriate for the post-R&R element of this study; we modified the responses to the post-R&R AUDIT so that personnel were asked to rate their use of alcohol during R&R only. Global health was rated from ‘poor’ through ‘excellent’ using a five-point Likert scale. Caseness for common mental disorder was defined as ≥4 symptoms for the GHQ, PTSD by a score of ≥50 on the PCL-C and hazardous alcohol use by a score of ≥8 on the AUDIT. To examine the relationship between the experience of R&R and mental health, we amalgamated the CMD and PTSD cases to generate a measure of reporting CMD and or PTSD.
Individual R&R items were reduced to binary variables indicating endorsement or not and satisfied or not. The R&R scale was subcategorized into components identified in the PCA. General satisfaction items were examined separately. Percentiles were generated for the subcomponents to examine their association with mental health and alcohol outcomes using logistic regression. We were able to obtain pre- and post-R&R measures of mental health in 42 subjects in order to compare them on PTSD, CMD and alcohol use.
Analysis
The Statistics Package for Social Sciences (SPSS – version 19) was used for the analysis. The associations of categorical data were assessed using either Pearson’s chi square (χ2) test or logistic regression which generated odds ratios (ORs) with 95% confidence intervals (CI). For those who completed pre- and post-R&R PCL, GHQ-12 and AUDIT scales, continuous scores were compared using Wilcoxon signed rank test. Statistical significance was defined as p = <0.05 throughout.
Results
A total of 232 personnel completed the survey. An accurate response rate could not be generated as flights returning to theatre could not be monitored continuously and we relied upon flight receptionists to collect the completed questionnaires.
Sociodemographic factors.
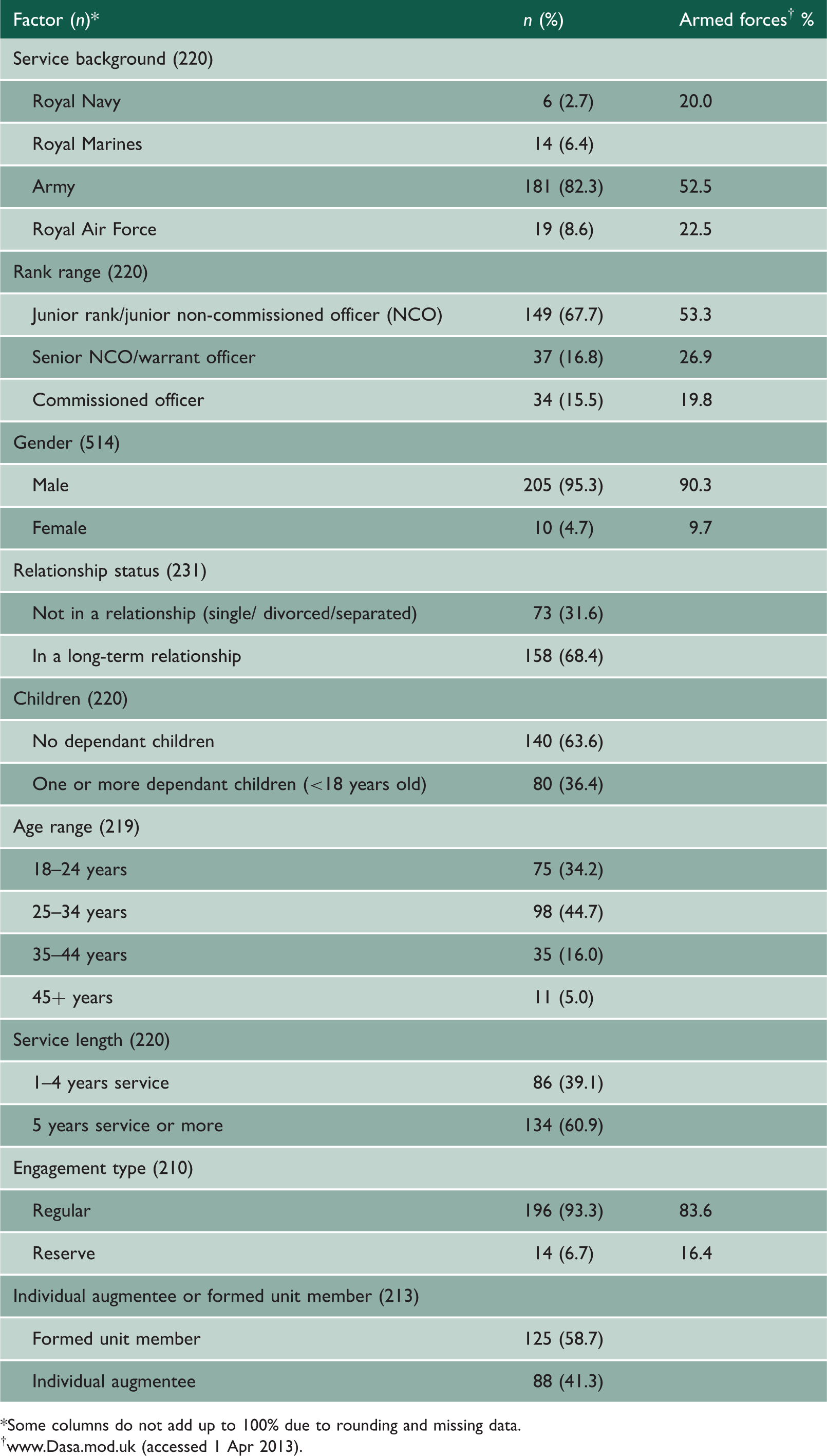
*Some columns do not add up to 100% due to rounding and missing data.
†www.Dasa.mod.uk (accessed 1 Apr 2013).
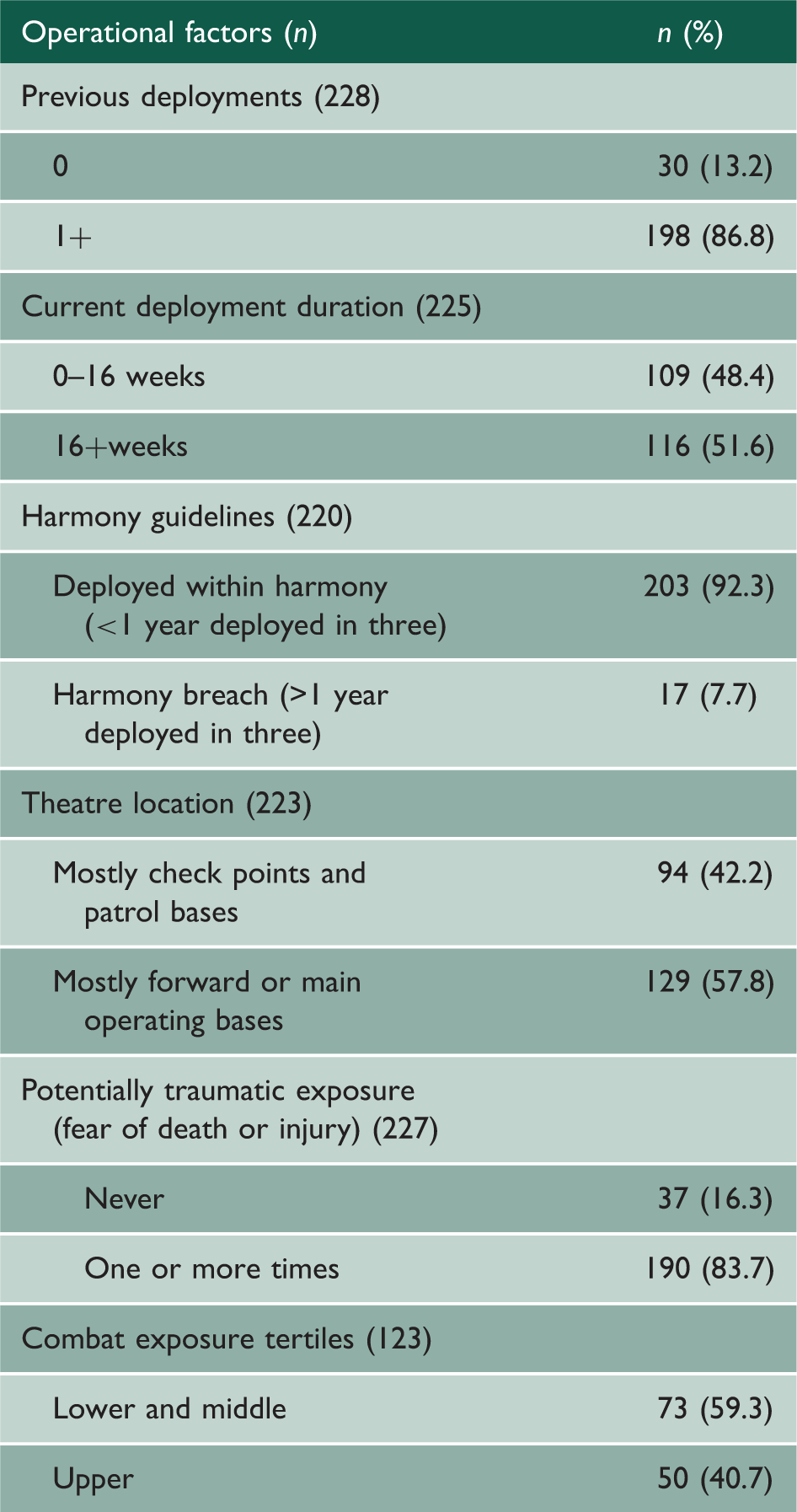
Operational factors.
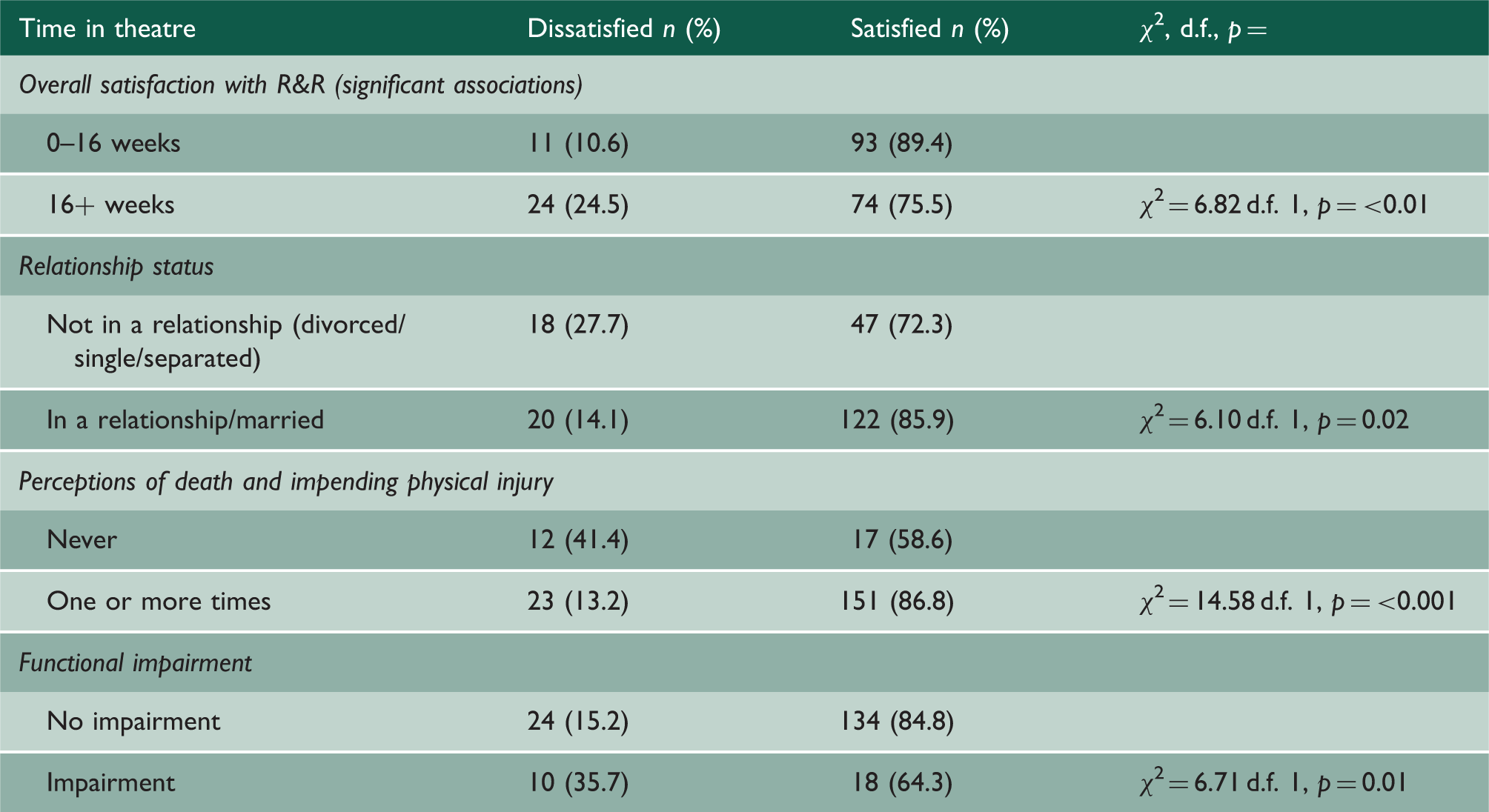
Overall satisfaction with R&R.
Mental health outcomes.
R&R components.
The difference between PCL-C, GHQ-12 and AUDIT scores pre- and post-R&R for those who completed the outcome measures at both time points was not statistically significant.
Discussion
This paper reports on the first study of the possible impacts of R&R within a western military. Our main findings were that taking R&R is highly satisfying and the vast majority of personnel would like to have R&R during future deployments. We also found that engagement with the R&R process was associated with better mental health. In the small number of personnel who completed pre- and post-measures, we found no evidence of significant change in mental health status post-R&R or significantly different patterns of alcohol use during R&R compared to normal levels of consumption.
Compared with other operational studies, we found relatively low levels of CMD and PTSD, although half of our respondents drank alcohol at hazardous levels during R&R. Our data suggested that greater engagement with R&R was associated with better mental health and less hazardous alcohol use. Fatigue resulting from having spent more time in theatre prior to R&R and fatigue associated with functional impairment from mental health symptoms was associated with lower satisfaction. It is perhaps understandable that being fatigued would impair engagement with R&R which was an important associate of gaining benefit.
The satisfaction levels reported in this study about R&R concord with those reported in other operational mental health studies;14–16 however, we found some evidence that being in a long-term relationship was significantly associated with greater satisfaction. The majority of respondents reported that they would value R&R during future deployments, most probably because most of them felt that R&R met their personal needs. Satisfaction is an important consideration as R&R is primarily an opportunity to rest and psychologically re-set; our data suggest that personnel were able to do this. Although we found that R&R did not reduce the burden of mental health symptoms or alcohol use in a small matched sample, personnel who engaged with some R&R components reported better mental health and less hazardous alcohol use. Given the cross-sectional nature of the majority of our data, we are unable to say whether better mental health and lower levels of hazardous alcohol use influenced the ability to engage with and derive satisfaction from R&R or if engagement promoted better mental health. Despite these limitations, we tentatively suggest that it might be helpful to prepare personnel to make the most of R&R via educational material or advice prior to leaving theatre to ensure that they are in the best possible position to actively engage with R&R.
Greater satisfaction with travel was associated with lower rates of hazardous alcohol use. This may have resulted from travel fatigue which was perhaps initially mitigated by using alcohol as a soporific agent. This result is consistent with the civilian literature where travel is the most stressful holiday activity. 4 We have previously reported that fatigue resulting from disrupted or prolonged travel from deployment is relatively common: 17 this adds impetus to the considerable efforts being made to improve travel to and from deployment. It might be useful to research whether allowing personnel to take adequate rest before going home, without shortening the duration of R&R could improve engagement and possibly reduce the use of alcohol during R&R.
Individuals who had more frequent thoughts of impending death and injury (a necessary component of the PTSD A criterion) reported significantly greater R&R satisfaction. R&R may have been an opportunity to access social support during which concerns about death and injury could be discussed in a physically, and psychologically safe environment. While communication with home support is possible during deployment, there is no evidence to suggest that such support is particularly helpful to deployment mental health.3,18 The opportunity to access support from family members is reflected in our finding that personnel in long-term relationships derived greater satisfaction from R&R and the ability to rest and engage with social support, to physically recover and to switch off decreased the probability of reporting PTSD and or CMD and hazardous alcohol use.
As reported in numerous military studies19,20 alcohol misuse is substantially more common among UKAF personnel than in the civilian population. A significant number of those taking R&R appeared to escalate their alcohol use from deployment enforced abstinence and those completing longer periods of deployment prior to R&R were especially likely to do so. With the exception of the R&R relaxation component, engagement with R&R generally and satisfaction with travel were associated with less hazardous use. Given that alcohol misuse is a particular concern for the UKAF and is likely to prevent engagement with R&R, influencing R&R drinking behaviour might be another area for future research.
R&R did not modify mental health symptoms when we examined data derived from a modest matched sample. It may be that focusing solely upon mental health when measuring possible R&R outcomes is not the most appropriate methodology, since personnel will shortly be returning to an operational theatre, a significant and unavoidable stressor. High levels of satisfaction alone may be a good measure of effectiveness, particularly as the majority of personal in this study would value R&R on a subsequent deployment, were able to do what they wanted on R&R and were able to meet most of their needs. R&R may also help maintain important supportive relationships (such as with family members) which in itself is likely to be helpful in the longer term. However, this topic needs to be investigated further in future studies.
Strengths and limitations
While we intended to assess personnel pre- and post-R&R, because of logistical problems, we were only able to assess a small matched group at both sampling points. This limited our assessment of whether R&R modified mental health. The R&R survey element was generated specifically for this study and, despite making every effort to ensure that the questions had ecological validity, we only tested the questionnaire in a small pilot study. However, the use of PCA allowed for a detailed examination of the association between the components of R&R and mental health outcomes. Although we used validated measures commonly used in military mental health research, the use of identifiable information may have given rise to response bias. 21 In addition, our data are largely cross-sectional and we cannot assess causality. Finally, as noted in previous point surveys of deployed personnel, satisfaction with R&R was high; however, this does not mean that this will positively influence mental health outcomes. The overwhelming majority of participants were from the army; therefore, inferences cannot be drawn about other types of rest such as shore-based leave for Navy personnel. Finally, the focus of this study is about the effect of R&R upon the deployed Service person, not the family, and we can therefore say little about the effects of R&R upon family and friends. In order to address the shortcomings of this research we recommend that further research be conducted using larger matched samples.
Conclusions
In our modest matched sample, R&R did not have a significant global beneficial effect upon mental health. However, there were no adverse effects and indeed when personnel engaged with certain specific elements of R&R, mental health was better and less alcohol was consumed. Furthermore, we found an incremental effect where increasing engagement was associated with incrementally better mental health although the direction of effect remains unclear. Future studies using larger matched samples with the addition of a follow-up component after personnel finally return home would be useful follow on investigations. However, while our conclusions are tentative, given the study’s limitations, the data suggest that it may be helpful for personnel about to go on R&R to receive some form of advice, be it written or verbal, about how to best engage with the process and avoid heavy alcohol use; similar briefings for Service personnel’s families might also be useful. Furthermore, those involved in planning the air travel to and from R&R should remain cognisant of the potential impact that smooth travel arrangements have upon the overall R&R process and specifically upon mental health. While the findings of this study derive from a sample of military personnel, we suggest that they may have implications for other organizations that deploy their staff away from home for prolonged periods of time.