
Abstract

Medical schools equip students with the knowledge and skills to undertake the technical practice of medicine. It has been argued that there is inadequate attention paid to the shaping of the future generation to function safely and enable them, in exercising leadership, to transform and improve healthcare. 1 In the current NHS, clinicians are talked about as being placed at the forefront of designing and commissioning safe, high-quality models of care. 2 Junior doctors are a potential resource in shaping this agenda; in particular, bringing fresh perspectives to identify and act upon opportunities for improving healthcare. Yet, cultural barriers have long prohibited innovation and improvement in this group; their ability to lead change is often overridden by a clinical environment unreceptive to their skills and a lack of adequate training in medical school.3,4
Across the UK, junior doctors are overcoming those barriers by assuming an active role in improving healthcare. 5 Driven by their unrest and dissatisfaction of the status quo, they are forming a collective to challenge the accepted norms that potentiate poor quality outcomes for their patients. 5 We explore how social movements, defined by Della Porta and Diani 6 as ‘informal networks, based on shared beliefs and solidarity, which mobilise about conflictual issues, through the frequent use of various forms of protest’ (p.16), are driving these efforts and consider how students and junior professionals are using social movement theories to leverage change.
Preparing the workforce to deliver 21st century healthcare
Junior doctors are the ‘eyes and ears’ of healthcare organizations and they typically provide the resource to undertake clinical audits. Existing cohorts are now practising in an era where ‘quality improvement’ is an acknowledged priority, and is considered both a philosophy (i.e. we all have a role to continually seek to improve the systems within which we work) and a family of discrete technical and managerial methods (i.e. the knowledge and skills to lead changes that result in improvement). 7 However, the current generation have had brief (if any) professional preparation in patient safety, healthcare improvement and leadership competencies while at medical school. Thus, it is unsurprising that junior doctors are independently seeking knowledge and skills such as the systematic examination of processes used in healthcare delivery, teamwork assessment and improvement, and the use of measurement and statistics in daily work from organizations such as the Institute for Healthcare Improvement (IHI) Open School. 8
The IHI Open School is an educational programme founded in 2008 with three guiding principles: to provide educational content to equip members with the knowledge and skills to lead change; to establish community networks called Chapters at hospitals and universities where likeminded students and practising professionals can learn with, from and about each other's experiences of improvement while challenging each other to grow; and to support experiential learning through supporting members to lead improvements in practice. 8 Since its launch, it has become an international, interdisciplinary community with over 126,000 members from 57 countries. 8 Over 550 chapters exist and they are largely self-supporting and self-mobilizing by assuming leadership roles independent of their higher education institution or hospital. Through these local initiatives, students and junior professionals are proving to be agents of peaceful change.
Leading change in healthcare – a ‘Goliath’ task?
Psychologists remind us that change requires managing the loss individuals go through in a tolerable fashion. 9 Providing junior doctors with new knowledge and skills is only part of the solution; nurturing a confident workforce that practises the skills without feeling oppressed or in fear of reprimand is perhaps the biggest challenge for the NHS. Apathy or lack of support from senior colleagues can hinder and limit junior doctors’ participation. 3 Thus, it is unsurprising leading change in healthcare might be considered a ‘Goliath’ task.
Social organizer, Marshall Ganz of the Kennedy School of Government, Harvard University, has accrued decades of experience in mobilizing communities to achieve their goals. His method of community engagement is believed to be the game-changing tactic of the 2008 Obama Presidential Campaign. Ganz 9 believes ‘strategic capacity’ is an important influence of success, which is described as being emotionally and mentally motivated, having access to relevant expertise and knowledge, and being able to reflect on and identify areas of weakness in the opponent. Ganz 10 developed an organizational model based on these principles, and its key components are the development of effective working relationships, narrative to provide context, strategy to mobilize resources, and action to provide measurable effects.
Lessons from a junior professional-led patient safety social movement
In October 2009, healthcare students and junior professionals created the ‘Check a Box. Save a Life.’ campaign. Social movement methodology formed the backbone to the campaign. 11 Over 1400 participants contributed to the launch event, where students and junior professionals pledged to promote the use of the World Health Organization's Surgical Safety Checklist in operating rooms in developed and developing countries. 12
Effective working relationships
Interpersonal relationships are critical to forging shared understandings, commitments and collaborative action. 10 An initial organizing team of five students were united by a shared common goal to demonstrate a role for students and junior professionals to be active participants in healthcare improvement efforts, as well as creating a vehicle for engaging as many people as possible. 12 They partnered with organizations such as the American Medical Student Association (with a membership base of over 60,000) and the IHI Open School (then with a membership of over 16,000) to recruit others to do this work with them. 12 Each member of the core team took responsibility to work closely with an allocated group of new recruits, and offered coaching to support the development of a hub of activity at their hospital or educational institution in preparation for a launch event. 12 No rules confined the work relationships of the leaders, they regularly reflected to determine what worked best under which circumstances, and this served as an important step for identifying insights to be more resourceful with limited resources.10,12
Narrative to provide context
Social movement leaders must communicate their vision. Ganz 10 calls this a new ‘public narrative’ that consists of a story of self, a story of us and a story of now. The organizers were appealing to the experiences of others with unsafe healthcare, their shared values as future providers seeking better, safer medical practice, and their desire to produce change, not wait for it. 12 They focused their energy on cultivating a motivational narrative for their launch event. Through articulating a ‘story of self’, they conveyed their own calling to patient safety. In their expression of the ‘story of us’, they explored and emphasized shared experiences and values, which was contributing to the call to action. Their experiences as witnesses of unsafe healthcare built new friendships and shaped stories told to peers. Finally, in the articulation of their ‘story of now’, they illustrated to others what change might look like through painting a picture of what extraordinary action is possible when a group comes together around a shared common goal. Using their own public narratives, each new participant pledged to inspire at least two other friends or colleagues to join them. 12
Strategy to mobilize resources
Ganz 10 draws upon the biblical David versus Goliath story to outline an analogy of strategizing to mobilize resources:
David, a young unknown shepherd, goes to battle with the mighty and feared Philistine warrior, Goliath. Armed with a coat of mail, brass helmet and a sword, David realizes he cannot win with unfamiliar armour. He faces Goliath with his staff, slingshot and five stones from the brook. He skilfully slings a stone into Goliaths’ forehead through an opening in his armour and the giant falls to the ground.
Ganz argues that David saw resources that others did not see and opportunities they did not grasp. 12 David chose stones as his weapon since he was familiar with their use from protecting his flock from wolves and bears. The original core team of ‘Check a Box. Save a Life.’ organizers held no funds to kick-start the movement through in-person site visits or production of campaign materials; instead they used the social media wave to carry their message widely. 12 While it is now commonplace for a hospital CEO to hold a Twitter account to reach out to employees and the public, in 2009 this approach would have been considered radical in healthcare. New campaign participants were reached through social media including Facebook, Twitter and the IHI Open School Blog, which became a virtual narrative and action community for students to stay connected throughout the course of the campaign. 12 There were no funds to physically convene keynote speakers to endorse and launch the event; instead the keynote speakers – Don Berwick and Atul Gawande – delivered their talks virtually via their own webcams.
Action to provide measurable effects
Ganz 10 believes participants' hold the resources that social movements can mobilize. By reaching out to leaders across the world, the ‘Check a Box. Save a Life.’ campaign was able to utilize the resources of already established interest groups at their places of work and study. 12 This included the time and energy of their leaders, as well as existing relationships with their members and the know-how of dealing with any problems arising locally. A supportive learning community was established via regular conference calls so leaders could learn with, from and about each other's leadership challenges and solutions to overcome obstacles. 12 This fostered a ‘we're in it together’ approach. In addition, the campaign team was not prescriptive about how participants should engage with the campaign because they wanted new recruits to identify solutions and opportunities themselves and in turn feel ownership of the movement. 12
Characteristics of social movements
Social movements offer an opportunity to move from autocratic, top-down decision-making to autocatalytic, grassroots-led change. Medical students and junior doctors in the United States formed ‘The PharmFree Initiative’ to encourage healthcare professionals to seek out evidence-based and unbiased sources of information, rather than relying on pharmaceutical industry personnel for education. 13 A recent study suggests that the movement has altered prescribing practices and reduced harm in patients, and exposure to a gift restriction policy during medical school was associated with reduced prescribing of two out of three newly introduced psychotropic medications. 13
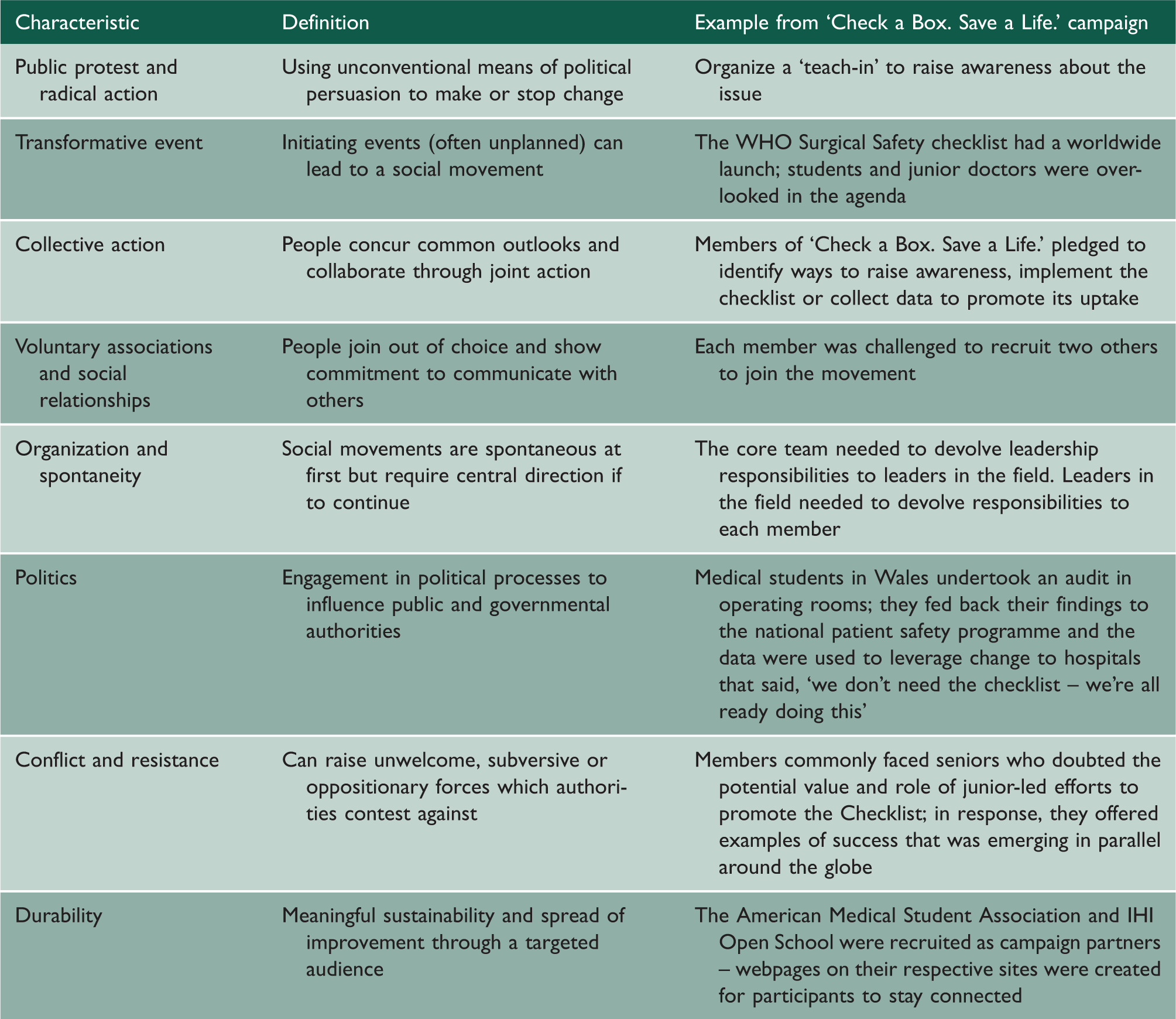
Characteristics of a social movement in relation to the ‘Check a Box. Save a Life.’ campaign.
A bright future for the NHS
While the current generation of junior (and senior) doctors are largely independently seeking knowledge and skills to improve healthcare, important steps within undergraduate and postgraduate education are being made. Examples include the Royal College of Physician's Learning to Make a Difference initiative, 15 as well as the promulgation of clinical leadership jobs for junior doctors such as the NHS Clinical Fellows’ Scheme. 16 Informal efforts in the UK are now thriving and examples include: over 40 IHI Open School chapters in hospitals and universities, 8 the Faculty of Medical Leadership and Management have an active ‘doctors in training’ division, 17 the online networking platform ‘the-network.org’ have published two casebooks of quality improvement projects, 18 and NHS Change Day brought over 180,000 pledges from NHS staff to demonstrate their commitment to improving patient care. 19 As these movements grow, and their numbers reach a critical mass within the healthcare workforce, perhaps the collective attitudinal shift will permit a profound shift in the stubborn culture of healthcare.
Conclusion
Change can perhaps present as an unwelcomed burden for the already busy junior doctor. Despite this, students and junior doctors are independently seeking skills to lead change. Their energy and efforts have culminated in national initiatives and a global patient safety campaign. Healthcare has been, and will continue to be, subject to discussions of reform to improve care; however, as Sheila Leatherman and Donald Berwick 20 put it, ‘emphasising learning over regulation is the linchpin strategy for improving care’. Knowledge and reflection combined with personal courage may be the key assets for confronting cultural resistance to change in healthcare. Junior doctors must embrace the current climate and be the architects of high quality services for patients. The time to act is now.