
Abstract
Non-cirrhotic portal hypertension (NCPH) is becoming an increasingly recognized entity in the setting of infection with human immunodeficiency virus (HIV).
DECLARATIONS
None declared
None declared
Written informed consent to publish the article was obtained from the patients
KAF
KAF undertook the literature review and prepared the initial manuscript draft. SB, SH and KWR provided useful resources and edited and advised on subsequent drafts
Introduction
We report two cases of non-cirrhotic portal hypertension (NCPH) in persons infected with HIV, one of which was unusual in occurring in the absence of exposure to any antiretroviral therapy (ART).
Case 1
A 65-year-old MSM (man who has sex with men) gentleman commenced ARTat the time of his HIV diagnosis 16 years previously. Since his diagnosis, he had been on a number of different ART regimens including those containing the nucleoside reverse transcriptase inhibitor didanosine (DDI).
Five years after diagnosis with HIV, abnormal liver function was noted, with alkaline phosphatase (ALP) 289 μ/L and aspartate amino-transferase(AST) 132 IU/L. Splenomegaly was detected on abdominal ultrasound scan (USS). Investigations as to the aetiology of splenomegaly (including autoimmune, infective, haematological and metabolic) at this time were unremarkable and the transaminitis resolved some months later on further change in ART regimen.
Two years later, the patient presented with abdominal swelling and visible abdominal veins, with recurrent mild elevation of AST. USS again revealed splenomegaly, however, on this occasion with a shrunken liver of coarse echotexture. Subsequent computed tomography (CT) imaging revealed gastro-oesophageal varices. Histological analysis of liver biopsy revealed mild sinusoidal dilation, consistent with NCPH.
Thrombophilia screen was notable for protein S and C deficiencies. The patient was subsequently commenced on propranolol as primary prophylaxis against variceal bleeding.
Currently he remains well, with well controlled HIV on ART (abacavir, zidovudine, lamivudine and efavirenz). He is asymptomatic from the NCPH point of view and has regular clinical review by the hepatology team.
Case 2
A 40-year-old Eritrean gentleman was referred by his general practitioner (GP) to the hepatology team with deranged liver function tests. These tests were undertaken by his GP during diagnostic work-up for epigastric discomfort. His past medical history was notable for previous episodes of malaria.
Leucopenia (2.2 × 109/L), thrombocytopenia (59 × 109/L) and elevated ALP (343 μ/L) were noted on blood tests taken by the hepatology team. Other liver function tests were within the normal range. Abdominal USS revealed splenomegaly and periportal reflectivity. Hepatic elastography was unremarkable.
An HIV test was undertaken in view of the haematological abnormalities in conjunction with the patient's ethnic origin being a potential risk factor for HIV infection. The HIV test result was positive. Significant liver disease was thought unlikely in view of the mild aforementioned liver function derangement and unremarkable hepatic imaging. At this point the patient was discharged from hepatology care, and referred to the HIV team for ongoing management.
Baseline CD4 count was 52 cells/mm3 and HIV RNA viral load was 7128 copies/mL. Medical and sexual history findings, in conjunction with results of serological investigations (including a stable low baseline CD4 count), were not in-keeping with recent HIV acquisition/seroconversion.
ART in the form of tenofovir, emtricitabine, lopinavir and ritonavir was commenced, in addition to co-trimoxazole as prophylaxis against Pneumocystis jirovecii pneumonia (formerly Pneu-mocystis carinii pneumonia).
Due to persisting mild intermittent epigastric discomfort, upper gastrointestinal endoscopy was performed. This revealed oesophageal varices. Subsequent abdominal CT imaging revealed an irregular liver with periportal low attenuation change, splenomegaly and oesophageal and splenic varices.
Based on these findings, a further hepatology opinion was sought. A transjugular liver biopsy was performed. The hepatic venous pressure gradient was unremarkable. Histological analysis of the biopsy (Figure 1) revealed small portal tracts with portal vein abnormalities and mild sinusoidal dilation, consistent with NCPH.
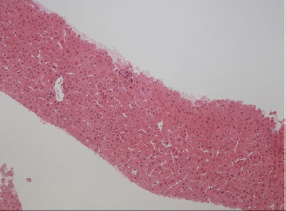
Liver biopsy specimen showing small portal tracts with portal vein abnormalities and sinusoidal dilatation
Concurrently the patient was treated appropriately for Helicobacter pylori and schistosomiasis as a result of positive serologies for these two conditions.
His HIV RNA viral load became undetectable within six months of commencing ART. Additionally, of note, subsequent serological testing revealed a mild protein S deficiency. Currently the patient is clinically stable, takes propranolol as prophylaxis against variceal bleeding and continues to respond satisfactorily to ART.
Discussion
NCPH should form part of the differential diagnosis as cause for liver dysfunction, particularly in the setting of HIV. NCPH is seen more frequently in developing countries and in those from low socioeconomic groups. 1
Recent case series have shown oesophageal variceal bleeding as the commonest presenting feature in patients with NCPH. 2 Another case series has suggested an increased risk of pulmonary hypertension in HIV-infected individuals with NCPH. 3
Two main forms of NCPH are recognized. Firstly, hepatoportal sclerosis (HPS), characterized by portal vein sclerosis, obliterative venopathy and sinusoidal dilation. And secondly, nodular regenerative hyperplasia (NRH), characterized by hypertrophic hyperplastic periportal hepatocytes.
The aetiology of NCPH is poorly understood. Autoimmune factors, portal tract thrombosis and genetic factors have been associated with HPS. Additionally, malignant conditions including myeloproliferative disorders have been associated with NRH. 4
The majority of NCPH cases in the HIV setting have been reported in the context of current or prior, particularly prolonged exposure to the ART drug DDI. 5 In 2010 the FDA issued a labelling revision for DDI highlighting the association of DDI and NCPH. 6
Endothelial cell damage in the portal system causing veno-occlusion, and underlying thrombo-philic states 7 are proposed mechanisms, due to ART and/or HIV. The term HIV-associated oblit-erative portopathy has been proposed. Both cases discussed in this report had evidence of protein S and/or C deficiencies. Additionally, a recent case report has described the successful use of anticoagulant therapy in a patient with HIV-associated thrombophilia and NCPH. 8
Conclusion
NCPH is an increasingly recognized entity in the setting of HIV. It is, however, rare in HIV-infected individuals unexposed to ART, particularly DDI.
This report first illustrates the importance of pursuing a thorough diagnostic work-up in the HIV-infected patient with liver dysfunction. Second, it importantly highlights liver function derangement as a trigger for HIV testing in those with risk factors for HIV acquisition.
As per the British HIV Association, however, HIV testing should be considered in all patients registering in general practice and in all general medical admissions in settings where the diagnosed HIV prevalence in the local population exceeds two in 1000 population, irrespective of risk factors for HIV-acquisition. 9 Late diagnosis remains an important factor associated with HIV-associated morbidity and mortality.
Footnotes
Acknowledgements
None