
Abstract

Introduction
The Health and Social Care Act 2012 abolishes primary care trusts (PCTs) in England and hands responsibility for decisions about allocation of local healthcare resources to newly established clinical commissioning groups (CCGs). The NHS Constitution emphasizes patients’ rights to expect these decisions to be made ‘rationally’. 1 The National Prescribing Centre (NPC), now the Medicines and Prescribing Centre at the National Institute for Health and Clinical Excellence, has directed considerable effort in recent years at defining the parameters of rational decision-making, and supporting PCTs in improving their approaches to prioritization and resource allocation.2-5 A key driver for this activity has been the so-called ‘postcode lottery’ of local decision-making (whereby a patient in one geographical area may receive NHS funding for a particular drug or treatment while a patient with similar clinical needs in another area may not), and a requirement to ensure that local resource allocation decisions are able to withstand public challenge and judicial review. 4
DECLARATIONS
None declared
JR and TG are (respectively) the lead researcher and principal investigator of a study exploring local decision-making about individual funding requests in the NHS, and were invited to join the NPC steering group as a result of their involvement in this study. They acknowledge the funding support of NIHR Research for Patient Benefit Programme (PB-PG-1207-15061).
The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
JR
All authors conceptualized the paper and were members of the steering group that oversaw the development of the competency framework. JR wrote the first draft of the paper, to which all authors subsequently contributed.
Aziz Sheikh
Responding to concerns that significant organizational learning will be lost with the abolition of PCTs, and that new clinical commissioners will lack the skills, expertise and experience to make resource allocation decisions that have public and legal legitimacy, the NPC, commissioned by the Department of Health, embarked on a systematic process to develop a national ‘competency framework’ resource for those involved in making difficult prioritization decisions at a local level.
This paper reports on how the NPC competency framework was developed, and presents a potentially transferable methodology for advancing a competency framework to support individual and organizational learning and improvement.
The strengths and limitations of competency frameworks
In September 2011 the NPC invited a group of academics and practitioners, including opinion leaders in local decision-making and individuals with expertise in local, regional and national resource allocation, to form a steering group to oversee the development of a robust competency framework. As members of the steering group, our challenge was to support a process that delivered an evidence-based resource, capitalizing on the recognized value of competency frameworks (in providing a common language for describing effectiveness in organizations, and a ‘benchmark’ for achieving consistency in organizational practice 6 ), while staying mindful of their limitations (see below). Our role was to respond to the urgent educational needs created by the government's NHS reforms, and provide novice clinical commissioners with a timely starting point for assuring the quality of their processes. The aim was to produce a framework that could help identify individual and team learning needs, clarify roles and responsibilities, support design and commissioning of training programmes, and provide a signpost to further educational resources.
Although competency frameworks are familiar and widely used tools for educational development in the NHS,7-9 critical appraisals of the concept have highlighted a number of limitations, and raise important questions about educational value. Lingard, 10 for example, notes how competency frameworks tend to focus on the individual learner; she argues instead for a ‘collectivist discourse of competence’, based on social learning theories that ‘move our focus beyond capturing, codifying and documenting knowledge of individuals, and towards the ways through which knowledge is shared, discussed, and innovated in a collective setting’ (p. 627).
A second criticism of competency frameworks is that they are inherently reductionist since they over-rationalize human and organizational behaviour and reduce complex practice to a set of distinct behaviours and technical skills, while ignoring less tangible qualities (such as accumulated experience, tacit knowledge, intuition and virtues such as kindness and integrity) that contribute to effective action. 11
Thirdly, competency frameworks may ‘freeze’ the behaviour and skills that are useful in the present and may not support the skills and behaviour needed in the future. 11 Fraser and Green-halgh 12 suggest that the challenge is for educators to enable not just competence (what individuals know or are able to do in terms of knowledge, skills and attitude) but also capability (the extent to which individuals can adapt to change, generate new knowledge and continue to improve their performance).
While we were mindful of these criticisms and took them seriously, we also considered that by applying established principles for developing effective competency frameworks, we could reduce these limitations sufficiently to make the exercise worthwhile. In particular, we used four guiding principles: user involvement in the development process; a consideration of competence as collective and individual; an emphasis on practical and technical reasoning processes; and recognition of the competency framework tool as one part of a wider programme of capacity building and organizational improvement.
The development process
In keeping with evidence that intended users of a competency framework must be involved in its development to encourage ownership and acceptance of it as a valid tool, 6 we adopted a ‘bottom-up’, empirically based approach to identify and develop the competency sets, drawing on the experience, identified needs and naturalistic language of practitioners engaged in local decision-making. At an early stage in the development process, NPC invited key stakeholders, including those with an emerging clinical commissioning role, to a one-day workshop to share experiences of local decision-making, and to identify the scope of the framework. Later in the process, a ‘user-testing group’ met to assess the draft framework for relevance, usability and gaps. Thus the process of development ensured that throughout, the identified needs and experience of practitioners framed our conceptualization of competency.
Second, mindful of the limitations of the conventional individualist notion of competencies, we conceptualized them as characteristics of the individual, group, and organization, dynamically produced through social interaction. We recognized that robust local decision-making is a joint accomplishment, dependent on an interplay of personal, interactional and situated factors.
Thirdly, our epistemological perspective took on board mounting evidence from published research findings13,14 and experiential reports from stakeholders, that local decision-making is as much a social practice of deliberation and judgement, involving tacit knowledge, ‘common sense’ and ‘phronesis’ (practical reasoning), as a technical process of searching for and applying the relevant research evidence and correct ethical principles. For example, at the stakeholder workshop one participant commented that the most difficult aspect of the process was ‘recognising the role of judgement - my bugbear is when everyone talks about evidence based practice and [the] reality is with IFRs [individual funding requests] that there isn't much evidence. So we have to use judgement’. We sought to capture a competency set on deliberation, reasoning and judgement, acknowledging (a) the wide variety of evidence and the role that different kinds of evidence (such as local and experiential knowledge) may play in improving the quality of judgements in decision-making, (b) that emotion may impact on ethical engagement with an issue and can serve as well as hinder good judgement, and (c) the need for ‘competent’ CCGs to be able to discuss issues of ambiguity, complexity and uncertainty with an appropriate level of patience and tenacity.
Finally, we recognized from the outset that the development of a competency framework was always going to be a starting rather than an endpoint, and must be part of a broader programme of capacity building and addressing educational needs, rather than a standalone ‘product’. 11 Alongside the development of the competency framework, the NPC has produced a collection of guides, e-learning and newsletter resources, available on its website (http://www.npc.nhs.uk/local_decision_making/), to provide support and learning opportunities to those now poised to take over responsibility for this often very difficult, high-profile and frequently contested aspect of local decision-making. We also recognized that, in addition to the final ‘product’, the process of developing the competency framework helped to build the key relationships, reciprocities and commitments that would enable this work to be taken forward.
The competency framework
The NPC competency framework covers nine competency sets for local decision-making (see Figure 1), providing a ‘road map’ to orientate CCGs to the complexity of resource allocation decision-making, a self-assessment tool to help in the identification of areas for personal and group development, and a reading list of further educational resources. A copy of the framework is available here (http://www.npc.nhs.uk/local_decision_making/resources/LDM_comp_framework.pdf).
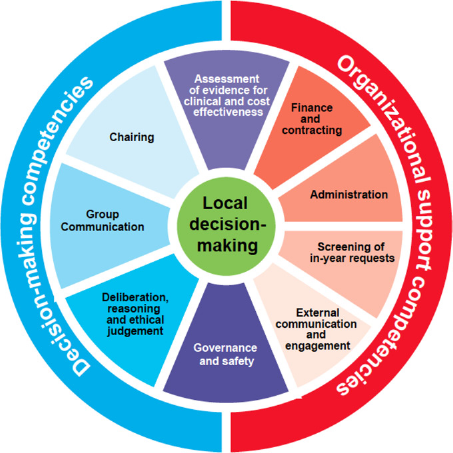
Competency framework for local decision-making about resource allocation: the nine competency sets. 16
The framework was launched in April 2012 and evidence is emerging from some CCGs to suggest that it is being used as a starting point to help CCGs reflect on their future needs as resource allocators. In one locality, for example, the diagnostic tool has been used to assess the competence of the local area prescribing committee against each of the nine domains on a scale of 0-10, highlighting areas for action and improvement, for example, the need for the committee's terms of reference to include an explicit statement of the ethical principles guiding decision-making, and for improved external communications and engagement with local stakeholders. Feedback from other localities, however, indicates that the timing of publication of the framework, just as local decision-makers are grappling with the challenges of the organizational changes arising from the NHS Health and Social Care Act, means that they have not yet implemented the framework, and we await further evidence of the key issues arising from use of this new tool.
Conclusion
A national competency framework for local CCGs embodies the tensions between attempts to tackle local variation in decision-making practices and so reduce the so-called postcode lottery, and the ‘hands-off approach of the government's NHS reforms, ‘liberating’ clinical commissioners to become more autonomous in their decisionmaking. 15 Within the constraints of this wider policy context, the NPC has produced a resource that recognizes the highly complex nature of resource allocation decisions, provides a valuable starting point for CCGs to identify training needs and acts as a tool for reflective practice.
We hope that the approach to developing the NPC competency framework described in this paper, grounded in evidence-based principles and offering a potentially transferable methodology, may help other groups tasked with supporting individual and organizational learning and development.
Footnotes
Acknowledgements
The authors wish to thank Jenny Wright and the other members of the steering group, and the participants who contributed to the scoping and user-testing workshops for the development of the competency framework.