
Abstract
Takotsubo's Cardiomyopathy is an acute cardiac syndrome precipitated by sudden emotional stress. Left ventricular dysfunction is reversible and prognosis excellent.
Introduction
Takotsubo cardiomyopathy or left ventricular apical ballooning syndrome is an acute cardiac syndrome precipitated by emotional stress.
Patients present with chest pain, ECG changes and elevated cardiac enzymes consistent with acute myocardial infarction but have normal coronary arteries on angiography.
We report the case of a 68-year-old woman who was referred to our Acute Medical Unit with chest pain after having been burgled.
Case Report
A 68-year-old woman awoke at 4.30 am and realised that she had been burgled. Shortly afterwards, whilst she was on the telephone to the emergency services, she developed retrosternal chest discomfort described as feeling like someone ‘sitting on her chest’. There was radiation to her left arm and associated nausea with profuse sweating. She did not describe shortness of breath or palpitations. This episode lasted approximately 1 hour in total.
She consulted her General Practitioner (GP) the following morning and developed a further episode of chest discomfort whilst in the surgery. After being given 300 mg aspirin she was referred to hospital. The GP letter described her to have been very ‘panicky’ prior to the onset of this second episode.
Her risk factors for coronary disease were hypercholesterolaemia, a positive family history and being a recent ex-smoker of 18 months with a 30 pack year history.
On arrival to hospital she was pain free and looked comfortable. On examination she was in sinus rhythm at a rate of 70/min, a blood pressure of 130/70 and oxygen saturations of 100% on air. The jugular venous pressure was not elevated and auscultation confirmed normal heart sounds and minimal bibasal crackles.
Initial ECG showed sinus rhythm with <1mm ST elevation in leads V3, V4 and T wave flattening in leads V5 and V6.
Repeat ECG showed evolving anterior T wave changes with the T waves becoming biphasic followed by deep T wave inversion in leads V3–V6, with milder T wave inversion in I, II, and aVF (Figure 1). She did not develop q waves. Chest X-ray was normal with no evidence of pulmonary oedema
Electrocardiogram showing widespread T wave inversion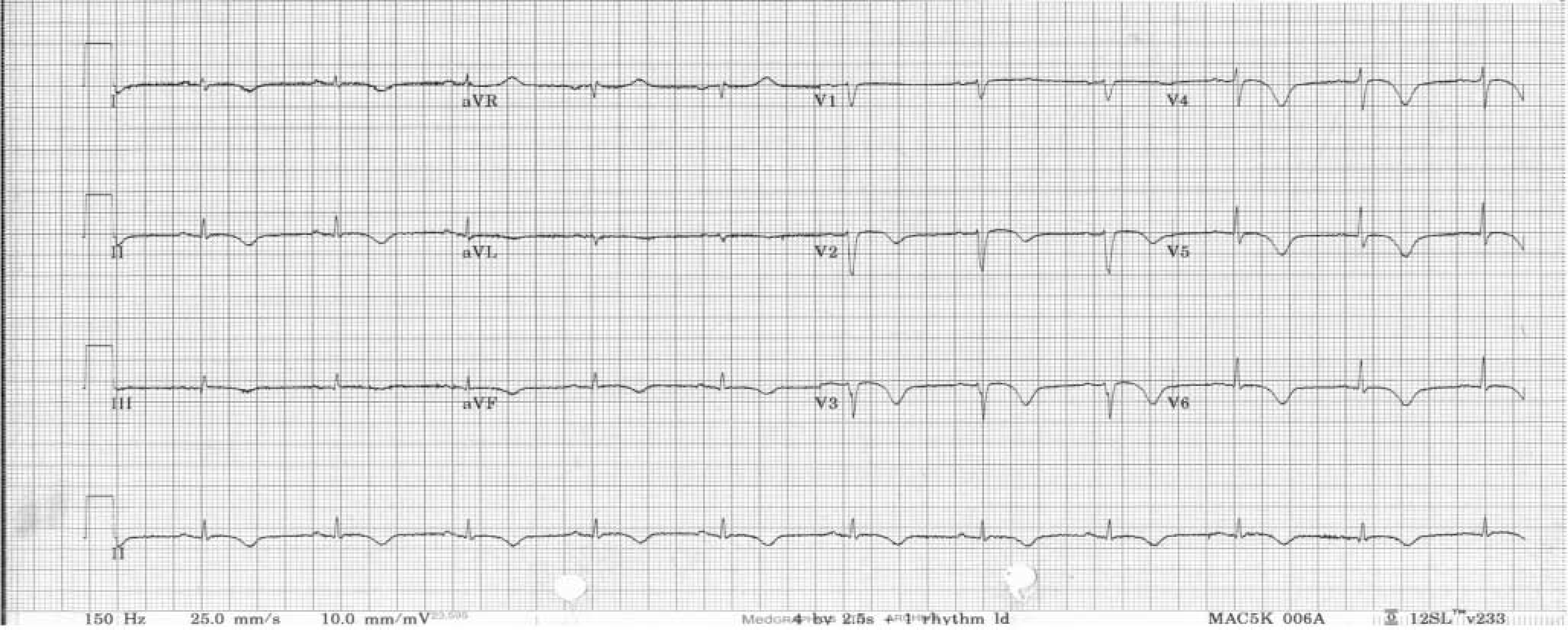
Throughout this time she remained pain free and comfortable.
Serum Troponin I was elevated at 1.9 and the working diagnosis was non-ST elevation myocardial infarction (NSTEMI).
She was treated with aspirin, clopidogrel, low molecular weight heparin (LMWH) and beta blockade.
Subsequent echocardiography revealed a non-dilated left ventricle (LV) with mild hypertrophy and severe apical hypokinesis but otherwise good LV function.
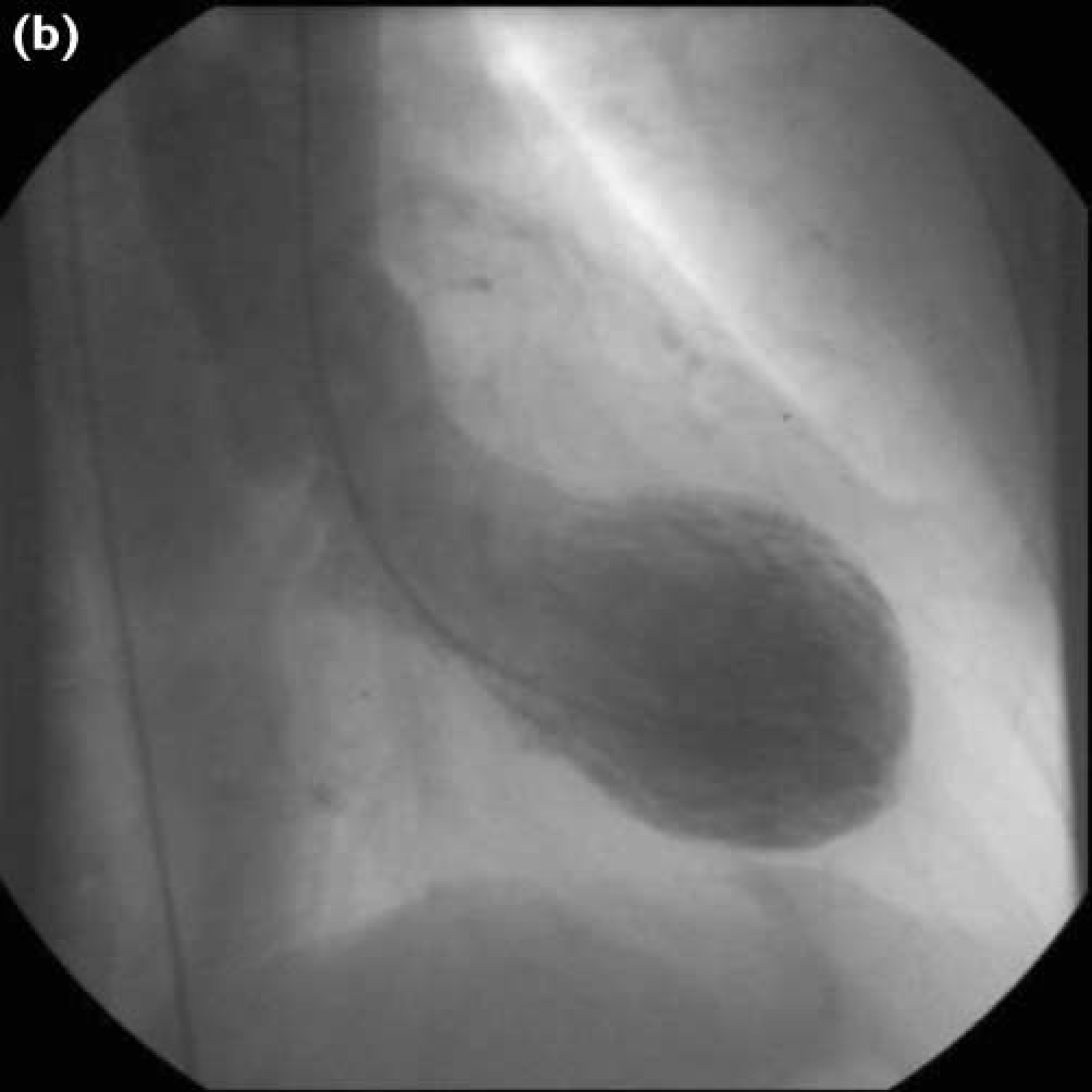
Coronary angiography revealed completely normal coronary arteries. Left ventricular angiography revealed an akinetic, aneurysmal apex (Figures 2a and 2b).
Left ventricular angiogram in diastole Left ventricular angiogram in systole showing apical ballooning (akinesia)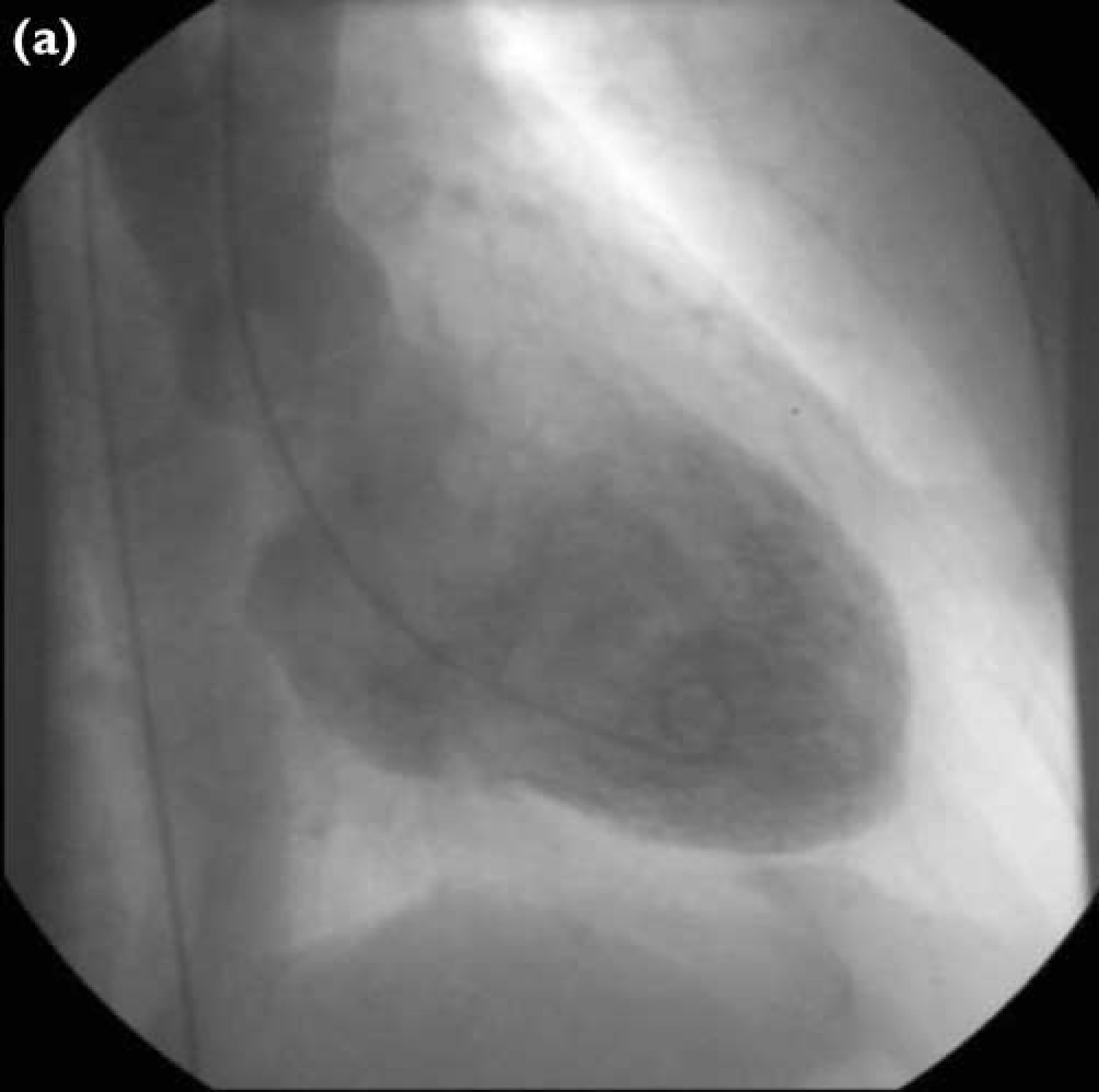
She was discharged home on aspirin, clopidogrel, atenolol, isosorbide mononitrate, losartan, and sublingual glyceryl trinitrate (GTN).
Repeat echocardiography 3 months later showed normal left ventricular function with no dilatation, aneurysm or regional wall motion abnormalities.
Outpatient review confirmed complete recovery. She had no further episodes of chest discomfort or shortness of breath and there were no features of left ventricular dysfunction on examination.
Discussion
Takotsubo cardiomyopathy was first described in Japan in 2000. 1 It was named after the Japanese fishing pot used to trap octopus. There have been numerous reports in the Japanese literature and to a much lesser extent in the USA.2,3 More recently it has also been reported in Europe. 4
The syndrome is usually precipitated by emotional stress. The most common precipitant is death of a close family member but other reported precipitants include court appearance, fear of a procedure, arguments and surprise parties/reunions. 3 The vast majority of patients are postmenopausal women.
Chest pain is almost always present and dyspnoea is common. 3 ECG changes on presentation are variable and may consist of ST segment elevation or depression, T wave inversion, q waves, prolonged QTc or a combination of the above.1–4
Cardiac enzymes only show a modest rise but are usually in the range consistent with ‘myocardial infarction’.
Despite symptoms, ECG changes and cardiac enzymes suggesting acute myocardial infarction, coronary angiography shows normal coronary arteries with no focal stenosis or ‘culprit lesions’. The LV angiogram has a characteristic appearance with LV apical hypokinesis/akinesis and basal hyperkinesis leading to a ‘ballooned’ appearance.1–4
Echocardiographic findings show similar appearances with an akinetic or hypokinetic apex but with good remaining LV function.3,4 Right ventricular apical akinesia may also be present.
The prognosis of this group of patients is very good beyond the acute phase with the LV function normalizing over 3 days to several months.1-4 Although death is rare, during the acute phase patients may develop pulmonary oedema, arrhythmias, thrombus and very rarely cardiac rupture.5,6 In these cases management should usually be active as complete recovery of LV function is to be expected. Long-term follow up confirms good prognosis with a low incidence of ischaemic heart disease. 3
Various mechanisms that could account for the reversible LV dysfunction caused by emotional or physical stress have been postulated. These include massive catecholamine release leading to epicardial coronary spasm, microvascular spasm or perhaps direct myocyte injury. Epicardial spasm however, has not been consistently demonstrated during provocative angiography. 3 Catecholamine release causing direct myocyte injury has been observed in phaeocromocytoma and subarachnoid haemorrhage and in a recent case series the majority of patients with Takotsubo cardiomyopathy had elevated serum catecholmines. 3 In addition, the five patients who underwent endomyocardial biopsy had features consistent with an elevated catecholamine state. 3
Due to the similarities with acute myocardial infarction patients may occasionally receive thrombolytic therapy and often undergo coronary angiography, which is diagnostic. However, gadolinium-enhanced cardiac MRI is also able to distinguish between myocardial necrosis and takotsubo cardiomyopathy.3,7 It may offer a non-invasive method of diagnosis.
7
Other features that may point to a diagnosis of takotsubo cardiomyopathy include:
ECG changes: extensive ST-T wave changes not confined to a single vessel territory, evolving T wave changes, prolongation of QT interval and a lower progression to abnormal q waves.
8
Cardiac enzymes: limited rise out of proportion to ECG changes and akinesia Echocardiography: Typical findings of hypokinetic/akinetic apex with basal hyperkinesis-wall motion abnormalities involving multiple coronary territories. Right ventricular apical akinesia in addition is not an uncommon finding, making the diagnosis more likely.
9
History of physical or emotional stress.
The history of emotional stress may well be relatively ‘minor’ and may need to be ascertained by direct questioning or may become apparent retrospectively once the diagnosis is considered.
All patients should have repeat echocardiography to confirm complete recovery of left ventricular function and consideration should be given to the gradual withdrawal of secondary prophylactic medication such as ACE inhibitors.
Takotsubo cardiomyopathy may be more common than previously thought and although under-reported it is an important diagnosis to make, with an excellent prognosis.
Guarantor JTW.
Contributorship IAF wrote the case report, obtained relevant images and the patient's consent prior to submission. KA was involved in the patient's care, had the idea to publish as a case report and edited the report prior to submission. JTW was the patient's consultant, edited the report prior to submission and is acting as guarantor.
Footnotes
Competing interests None declared.