
Abstract

Additional material for this article is available from the James hind Library website [http://www.jameslindlibrary.corg], where this paper was previously published.
BACKGROUND: EARLIER STUDIES OF PERTUSSIS VACCINATION
During the late 1920s and early 1930s statistics published by the League of Nations 1 made clear that whooping cough (pertussis) was an increasingly important cause of childhood mortality. Scientific interest in preventing the disease had begun in France in 1913 when Charles Nicolle began developing a series of whooping cough vaccines. 2 These vaccines produced inconsistent results, however, and it was not until the late 1920s that Danish researchers 3 developed a new generation of vaccines based on whole, killed pertussis bacteria, spun by centrifuge and partly purified. Between the mid-1930s and mid-1940s several field studies of this second generation of vaccines were conducted. 4 9 These studies also yielded widely differing estimates of vaccine efficacy, however. In an early cohort study done in the Faroe Islands, Madsen reported that the proportion of vaccinated individuals protected ranged from 94% to 24%. 3 Other estimates of the proportion protected ranged from 80% 6 to only 11%. 9
These varying estimates of vaccine performance had at least two possible explanations. They might have reflected either differing manufacturing processes, or variations in the methodological rigour of the studies: for example, while Doull 4 had used alternation to generate comparison groups and McFarlan 9 had expressed concern about possible observer biases, Bell 7 had conducted an exemplary randomized trial with several measures taken to prevent biased assessments of outcome. 10
THE MEDICAL RESEARCH COUNCIL TRIALS
Despite more than a decade of intensive assessment of different formulations of whooping cough vaccines, the question of the field effectiveness of the vaccines remained inadequately answered. It was against this background that the Whooping Cough Immunisation Committee of the Medical Research Council decided to do ten randomized field trials of different formulations of whole-cell, killed, pertussis vaccines. 11 The studies were done between November 1946 and April 1948 and involved four vaccines in six batches (produced by Parke Davis Ltd, Glaxo Laboratories and the Michigan Department of Health) and a placebo (a ‘catarrhal vaccine’ produced by Burroughs Wellcome Ltd).
The MRC studies were carried out in London, Manchester and Leeds after a publicity campaign inviting participation. After signed consent had been received from their parents, 8927 children aged 6 to 18 months with no previous history of whooping cough or pertussis vaccination were initially included. Table II in the paper records the numbers of children in the vaccine and control groups who
Were excluded before completion of inoculations; Received the full course of inoculations; Were excluded during follow up; and Remained for analysis at the end of the follow–up period.
After classification by sex and age, the children were allocated to one of four groups. For each age and sex group, sheets had previously been drawn up on which the letters A, B, C and D in random order (using a system of cards) were repeated a sufficient number of times to deal with all the expected numbers of volunteers. On arrival at the clinics, the children were inoculated (mainly by intramuscular injections) with material from a bottle with the appropriate letter.
These precautions taken to prevent foreknowledge of allocations was reflected in comparison groups with very similar characteristics (as shown in Table III in the paper). Care was also taken to reduce observer bias among those assessing outcomes:
‘Although four vaccine letters were used, two of them in fact indicated the pertussis vaccine being tested in the trial and the other two the “anti-catarrhal” vaccine. It was thought that by employing this method field-workers would be less likely to distinguish the pertussis vaccine from the “anti-catarrhal” vaccine. As the early trials progressed it became evident that more cases of pertussis were occurring in children inoculated with vaccines A and C–the “anti-catarrhal” vaccines–than in children with vaccines B and D–the pertussis vaccines. There was also some difference in the incidence of slight inoculation reactions between the pertusssis and “anti-catarrhal” vaccines. To ensure, therefore, that follow-up observations remained unbiased, the vaccine letter on each record card was covered by a thick label until the end of the investigation or until the duration or severity of an attack of pertussis had been recorded on the card.’
Follow-up was for between two and three years (27 months on average). Surveillance was carried out by teams each consisting of a doctor, a nurse and a clerk, as well as by parents, using a system of pre-paid envelopes. Exposure to the disease was reported as at ‘home’ or ‘other’, and the data were reported in these categories. Cases of pertussis were defined as a cough with positive culture, and 806 out of 836 suspected cases were confirmed in this way. Data on disease severity were also reported, using duration of cough (in weeks), number of paroxysms in 24 hours, and the presence of respiratory complications. One child in five was visited within 72 hours post-immunization to assess adverse effects.
The authors of the report concluded that, despite notable variability in effectiveness, all of the vaccines tested afforded considerable protection. The vaccine that performed best was the Michigan Health Department's product. The only adverse effects reported were six sterile abscesses in recipients of alum-precipitated vaccines.
THE ENDURING IMPORTANCE OF THE MRC WHOOPING COUGH VACCINE TRIALS
The MRC pertussis vaccine trials are important not only in the history of randomized, placebo controlled trials, but also in the history of vaccine assessment. The results showed that all the available whole-cell vaccines were significantly more effective than placebo against pertussis. However, there are two nearly forgotten related spin-offs from these trials.
First, the trials and subsequent follow-up work 12 confirmed that the mouse protection test, introduced in the USA in the 1940s, was adequate to assess the minimum required potency of whole-cell pertussis vaccines. The mouse protection test is a potency assessment based on the capacity of the vaccine to protect a mouse from direct intrcerebral challenge with virulent pertussis micro-organisms. 13 Confirmation of the reliability of the mouse protection test enabled the MRC to set a minimum quality standard for assessing such important vaccines.
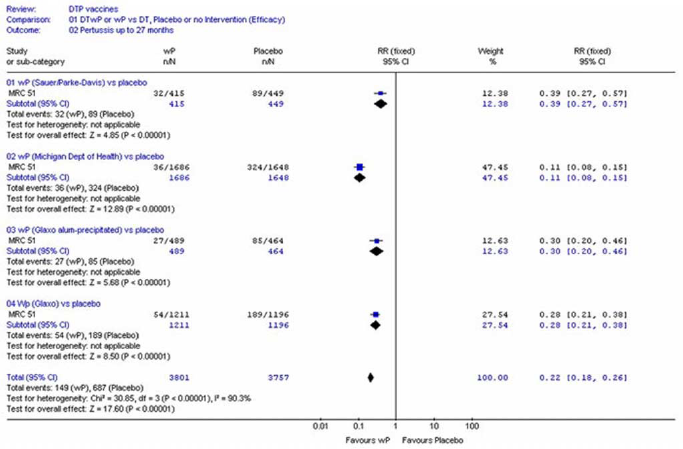
Second, although the mouse protection test was a good predictor of vaccine performance against placebo, it could not adequately distinguish the differential effectiveness of different vaccines used in the field in children. The MRC trials showed that the effectiveness of vaccines as measured in children varied from manufacturer to manufacturer, from 61% to 89% (Figure 1). 14 The practical consequences of these findings are that (1) it is difficult to forecast the field performance of any whole-cell pertussis vaccine without randomized placebo controlled trials using clinical outcome measures; and (2) it is impossible to extrapolate from the result of an assessment of one type of whole-cell vaccine to reliable assessments of the effects of another vaccine.
The practical implications of these conclusions were largely forgotten until the 1980s, 15 when ‘breakthrough epidemics’ of whooping cough in vaccinated populations and questions about the safety of whole-cell vaccines led to the development of modern acellular vaccines. Most developed countries are now using acellular vaccines, but countries that persisted until recently in using whole-cell vaccines that had never been tested against placebo face the possibility of further pertussis-related disease. For example, 37% of immunized school age children in Britain presenting with a cough lasting two weeks or more have serological evidence of recent Bordetella pertussis infection. 16 Had the lessons of the MRC pertussis vaccine trials been fully understood and implemented, no whole-cell pertussis vaccine would have been introduced without evidence from placebo-controlled field evaluations.
The failure to grasp this lesson has probably resulted in substantial potentially avoidable morbidity and mortality in so-called ‘breakthrough epidemics’ occurring in populations vaccinated with whole-cell vaccines of low field effectiveness. As exemplified by the MRC pertussis vaccine trials, what matters most in assessing the effects of vaccines is reliable evidence on their effects on outcome measures that are of importance to the people vaccinated, not just their effects on antibody responses in vitro or in animals.
Competing interests None declared.
Acknowledgments
I am grateful to Harry Marks for references to the early development of pertussis vaccines.