
Abstract

Peripheral vascular disease remains a common condition that is associated with a functional disability and risk of limb loss. Arguably more importantly, the presence of peripheral vascular disease signifies a high risk of cardiovascular morbidity and mortality even in asymptomatic subjects.1,2 Furthermore, peripheral vascular disease remains a process which is linked with a number of other significant common medical conditions, and represents a differential diagnosis for a number of conditions producing lower limb pain. The issue therefore is to improve the detection of subjects with peripheral vascular disease to prevent further cardiovascular morbidity and mortality and improve the accuracy of diagnoses.
Peripheral vascular disease remains a grossly underdiagnosed condition, with current epidemiological projections estimating the prevalence of peripheral vascular disease in North America and Europe to be 27 million cases. It is further estimated that while 10.5 million of the subjects are symptomatic, the 16.5 million majority are asymptomatic and possibly unidentified. 3 A study from Maastricht showed that when following up 3070 asymptomatic patients with peripheral vascular disease the adjusted hazard ratio was 1.7 for a fatal cardiovascular event and 3.1 for a fatal cerebrovascular event. 1
Symptomatic peripheral vascular disease is independently associated with up to a six-fold increase in cardiovascular mortality risk as compared to the normal population. 2 The aim is therefore to accurately diagnose and aggressively medically treat subjects with peripheral vascular disease, not only to improve the patients’ functional ability, but also to prevent disease progression and the occurrence of other cardiovascular events such as myocardial infarction and stroke.
The Ankle Brachial Pressure Index (ABPI) is a simple, quick, non-invasive tool that can accurately identify peripheral vascular disease but is grossly underutilized by medical practitioners outside of the vascular surgical arena.
Diagnostic criteria for peripheral vascular disease
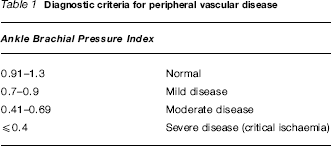
ABPI greater than 1.3 indicate poor compressibility of the arteries and signify the presence of medial arterial calcification, common in diabetes mellitus. This makes the diagnosis of peripheral vascular disease less reliable and is the main limitation of the ABPI. The only other limitation of note is where patients with a high grade aorto-iliac stenosis or occlusion present with a normal ABPI at rest due to the presence of a rich collateral network. 3 When compared to the gold standard of angiography, hospital studies have shown ABPI <0.9 to be 95% sensitive in detecting angiogram-positive disease, and it is nearly 100% specific in detecting healthy subjects. 6 Clinicians basing their diagnosis of peripheral vascular disease on history alone could miss 85—90% of cases. 7
Low ABPI is associated with a 4.2-fold increase in cardiovascular mortality relative risk as compared to those with normal ABPI. 8 Interestingly, the Strong Heart Study showed the adjusted hazard ratio for cardiovascular mortality in the high ABPI group (>1.4) was 2.09 as compared to those with normal ABPI. 9 The importance of ABPI in predicting mortality is further highlighted by comparing these values against those of the traditional atherosclerotic risk factors. When using myocardial infarction, stroke or cardiovascular death as an endpoint, the age- and sex-adjusted models showed hazard ratios of 1.79 and 1.48 for current smoking and diabetes mellitus, respectively. 10 Additional studies using myocardial infarction or death due to myocardial infarction as an endpoint calculated adjusted odds ratios of 1.75 and 2.87 for current smoking, 1.50 and 1.91 for hypertension, 2.37 for diabetes mellitus, and 2.38 for hypercholesterolaemia.11,12 The evidence supports the theory that low ABPI and the presence of peripheral vascular disease predict cardiovascular morbidity and mortality to a similar level as the currently accepted risk factors.
The accuracy of this simple, non-invasive tool, as illustrated by the high sensitivity and specificity, is also of great importance where peripheral vascular disease constitutes a differential diagnosis. Lower leg pain can be secondary to non-atherosclerotic arterial disease, venous disease, musculoskeletal pain or neurological pain. ABPI can differentiate between lower limb pain secondary to osteoarthritis of the knee, neurological pain due to spinal stenosis, and genuine atherosclerotic peripheral arterial disease and the wider issues that come with that diagnosis.
The evidence presented demonstrates the importance of the accurate and actual diagnosis of peripheral vascular disease, whether clinically symptomatic or silent. ABPI is a quick, accurate, non-invasive, simple tool to aid in diagnosis of this condition and there is a clear argument for this investigation to be incorporated in the routine practice of a number of different medical and affiliated specialities. Within the hospital, cardiology, renal and diabetology teams—who deal with patients whose risk of peripheral vascular disease is elevated—should incorporate ABPI into their routine practice. In orthopaedics, where peripheral vascular disease remains a significant differential diagnosis for common presenting conditions such as arthritis and sciatica, and subjects have potential vascular trauma, ABPI could improve the accuracy of their diagnosis. If ABPI was performed by general practitioners and practice nurses it would allow timely recognition, diagnosis and treatment of peripheral vascular disease, and ensure appropriate referral. This quick test could be incorporated into the introductory medical assessment of appropriately aged patients enrolling in a practice or the ‘well person health checks’.
If this quick, easy, non-invasive tool was commonly employed by general practitioners, physicians, surgeons and affiliated practitioners it would improve the timely and accurate and diagnosis of peripheral vascular disease and allow early intervention. The overall effect of this change in practice would inevitably reduce disease progression, the incidence of generalized cardiovascular complications, and ultimately improve patient outcome.
Footnotes
Competing interests None declared.