
Abstract
This paper probes how temporality is integral to the health examination regime that aims to protect citizens from infectious diseases in Taiwan. The paper finds that migrant workers in less-skilled occupations are examined more frequently than foreign professionals. Analyzing such differentiation, this paper argues that a hierarchy of sanitization is built on and increases the inequality between them and perpetuates instability in migrant workers’ circumstances. Applying a temporal approach to the study of health examination opens new inroads into our understanding of how a “migration state” achieves the exclusion of migrant workers by making them outsiders subject to permanent intrusion into their bodies.
Health examination and temporality
The COVID-19 pandemic brought the relationship between health and temporality into the headlines globally when the suppression of this infection relied partly on regular testing on a large scale. However, prior to the COVID-19 outbreak, that relationship had already been established in the practice of health examinations when migrant workers cross state borders. Stigmatized as a potential source of contagious diseases (Teo et al., 2005), migrant workers are often required by their host states to submit health examination certificates before or after their arrival (e.g., Öhd et al., 2019). Failing to pass the examination may result in the rejection of a visa or repatriation from the host country. If taking overseas employment is a temporal sequence, then passing health examinations before arrival marks its beginning and staying healthy is a precondition for continuing the journey. Failing health examinations may lead to repatriation and bring a disruption to the temporal sequence or terminate migration. Hence, being healthy, or at least passing health examinations, is pivotal to securing overseas employment and obtaining its benefits, such as remittances. In this light, health examinations are critical events that mark the temporal progression of labor migration (or the lack thereof).
Taking the temporality of health examinations as a vantage point, this paper raises two interrelated questions: (1) How is temporality integrated to the making of health examinations in order to prevent infection? (2) What kind of impact does temporality have on foreign nationals seeking overseas employment? Using Taiwan as a case study to answer these critical questions, this paper adopts temporality as an innovative lens through which to underline how inequality is deepened among different categories of foreign nationals whose control by health examination is differentiated by their perceived usefulness, occupation and country of residence. This paper will analyze how in Taiwan such time-sensitive inequality has been guided, before and during the COVID-19 pandemic, by the principle of “lax for the white-collar, strict for the blue-collar” (Chang et al., 2017: 9). This paper argues that before the pandemic, this principle was applied through the sequencing of health examination, medical treatment and repatriation with the possibility of prolonged ineligibility for re-entry. During the pandemic, this principle was more pronounced as health examination continued to apply to migrant workers but was suspended for foreign professionals. 1 This paper will analyze how this principle establishes a hierarchy of sanitization and geography of epidemiology to sanitize foreign bodies in order to stamp out infection. These temporal-spatial insights will enliven our understanding of the making of biopolitical governmentality. Seen from the perspective of health, it will underline inequality between migrant workers and foreign professionals, a hallmark of the guest worker system exemplified by Taiwan and commonly adopted by high-income economies in East Asia (Chan, 1999; Cheng, 2020; Hoang, 2017, 2020; Lan, 2003, 2006; Ruhs and Martin, 2008; Surak, 2017; Tierney, 2011).
In the following pages, this paper will firstly outline key arguments in the current literature on migrant workers’ health, including rights, productivity and security. This lays the foundation on which to emphasize the criticality of the time-sensitive sequencing of health examination and advocate a temporal approach to investigating this neglected aspect of health examination. It will then inform the sources analyzed by this research. Afterwards, this paper will explain how, under the principle of “lax for the white-collar, strict for the blue-collar” (Chang et al., 2017: 9), the sanitization of foreign nationals is categorized and differentiated, leading to a hierarchy of sanitization and geography of epidemiology. These analyses are conceptualized as a “temporal regime” (Donnan et al., 2017: 4), founded on temporal-spatial demarcation. Building on this pre-pandemic analysis, this paper further delineates how this temporal regime applied to health examinations conducted during the pandemic continued the inequality between migrant workers and foreign professionals, whilst the geography of epidemiology gives way to the interest of securing productivity in order to revive the suffering economy.
Migrants’ health and health examination
Maintaining physical and mental health is at the core of migrant workers’ well-being. Conceptualizing health as an essential right, migration scholarship is concerned with migrant workers’ access to healthcare that is either publicly funded or privately purchased (Ambrosini, 2015; Jones, 2005). Access to and costs of healthcare have a direct impact on migrant workers’ treatment for illness, whether it is occupational, non-occupational, infectious, or mental (Harrigan et al., 2017; Ho, 2004; Isarabhakdi, 2004; Lee, 2008; Preibisch and Hennebry, 2011). Concerned with whether migrant workers can receive timely and affordable healthcare, such scholarship examines how the quality and availability of healthcare is contingent on the cost of healthcare and on migrant workers’ gender, language, occupation, wage, location, accommodation, working conditions, access to information, relationship with their employers and/or brokers and access to healthcare. On the other hand, migrant workers’ health is also an issue of financing (Freeman and Kessler, 2008; Loganathan et al., 2020; Tangcharoensathien et al., 2017) and of their productivity (e.g., Flouris et al., 2018).
However, what has been less noticed by the public and scholarship alike is that migrant workers are also seen as a container and spreader of diseases, particularly during the COVID-19 pandemic (Guadagno, 2020; Lan in this issue). Their illness, particularly if it is infectious, is viewed by the receiving state as a threat to public health. As such, they are rendered an object for biopolitical governmentality. Examination of their bodies, or rather, intrusion into them, is justified as defending public health and assuring security. This rationale forms the foundation of the modern quarantine system in tandem with the issuance of visas (Schneider, 2011); it appeared globally during the COVID-19 pandemic. Thus, examining, reporting and responding to infectious illness enters the realm of public policy and migrant workers bear associated legal consequences (Nessel, 2012; Pysklywec et al., 2011; O’Connell, 2009; Orkin et al., 2014; Voo et al., 2021). Although studies on migrant workers’ health in general, and those on repatriation in particular, show that poor health contributes to their inequality, scholarship does not focus on the very governmentality of health examination, particularly the time-sensitive sequencing of health examination. Health is, by default, a matter of temporality, since physical conditions change as time goes by. It is particularly the case in regard to contagious diseases and the containment of their spreading. Implemented to catch this time-sensitive change in migrant workers’ physical condition, health examination offers an optimal lens through which to explore how temporality is embedded in the process of regular examination and documentation, with timely reporting, leading to eventual removal of the sick and infectious bodies from the territory.
In this vein, a temporal lens facilitates a unique, but overlooked, perspective from which to demonstrate how the passing of time is integral to migration governmentality, and how health examination affects foreign nationals divided by their perceived usefulness and country of residence. To utilize this temporal lens, this paper adopts the concept of “temporal regime” used by Donna et al. (2017: 4), which refers to the fact that migrant workers are considered temporary by their receiving state. In the guest worker system commonly adopted in East Asia, this temporariness (Devasahayam, 2010) is enforced by depriving them of naturalization and perpetuating their foreignness (Cheng, 2020). This paper argues that the regular, frequent and persistent examination of migrant workers’ bodies is an overlooked “temporal regime” that further perpetuates their temporariness, foreignness and inequality.
Research method
To uncover the intricate relationship between health examination and temporality, this paper investigates how health examination is implemented in Taiwan and how temporality is embedded in the legislation and implementation. Centering on the state (Hollifield et al., 2008) and its biopolitical governmentality, this paper employs a top-down approach and contextual analysis of primary sources including related legislation and governmental pronouncements. The legislation is a constellation of laws and regulations that determine the level of threat to public health posed by foreign nationals and examine their bodies accordingly. They comprise the Employment Service Act (henceforth the Employment Act) and the Immigration Act, as well as their respective enforcement rules, namely the Regulations Governing Management of the Health Examination of Employed Aliens (henceforth the Health Regulations 2 ), the Regulations Governing Visiting, Residency, Residency of Aliens (henceforth the Residency Regulations) and the Operational Directions for the Entry Ban on Foreign Nationals (henceforth the Ban Directions).
To investigate how the legislation is implemented, this paper also uses other primary sources of governmental pronouncements. They include the Legislative Yuan Gazette, the Health Examination Certificates, statistics and memorandums issued by the Taiwan Centres for Disease Control (TCDC), meeting minutes and memorandums issued by the Ministry of Labour (MoL), and the Control Yuan’s investigation report (Control Yuan, 2019). This paper also benefits from online interviews with foreign workers and activists in Taiwan, Hong Kong, Macau, Malaysia, Singapore and Indonesia for their insights into specific aspects of the guest worker system conducted in March, April, August, September, December 2021 and March 2022. As analyzed below, these laws and regulations embody a temporal regime and establish a hierarchy of sanitization and geography of epidemiology. Before and during the pandemic, they served the purpose of securing Taiwan’s competitiveness by recruiting high-skilled workers and assuring the supply of cheap low-skilled labor, while reducing the possibility of their introducing infectious diseases to Taiwan.
Health examination as a temporal regime
A temporal regime with its sanitization of foreign bodies is written into the Immigration Act and the Employment Act. The former forbids the entry of foreign nationals who carry “a contagious disease, a mental disease or other diseases that may jeopardize public health or social peace” (Article 18). The latter further stipulates that those who fail a health examination shall be expelled (Article 48) and Article 48 authorizes the implementation of the Health Regulations that monitor foreign workers’ health, or, rather, sanitize their bodies. While this Article applies universally to any foreign nationals, the Health Regulations establish a temporal regime that is intended to stamp out contagious diseases specifically brought in by migrant workers since the inception of labor migration in 1992 when Taiwan formally opened its domestic labor market to workers from the Philippines, Thailand, Malaysia, Indonesia and later from Vietnam. This intention, and the perception of migrant workers from the Global South as contagious bodies, was explicitly spelled out at an interagency meeting chaired by the MoL in March 2017. At this meeting, when a representative of the electronics industry suggested recruiting workers from Cambodia, Bangladesh, India, Pakistan or Syria as a form of “humanitarian aid,” the MoL dismissed the suggestion, explaining that it had to prevent the prospect of their “infectious disease invading” Taiwan (MoL, 2017: 15).
Categorization: Hierarchy of sanitization, geography of epidemiology
The temporal regime is built on categorizing foreign nationals according to their occupation and country of residence. Adopting the principle that no foreign nationals are allowed to work in Taiwan unless their employers have acquired prior permission (Article 43), the Employment Act divides the occupations of foreign nationals into two broad categories: high-skilled or white-collar (Category A, B in this paper), and labor-intensive or blue-collar (Category C in this paper). Guided by the principle of “lax for the white-collar, strict for the blue-collar,” this categorization leads to a hierarchy of sanitization in terms of the diseases that each category has to be checked for as required by the Taiwanese state.
Category A includes professionals, investors or corporate executives, athletes or coaches, missionaries or persons specializing in arts and performance. In general, they are exempt from health examinations, unless their employment requires them to stay in Taiwan for more than three months. In the latter case, there is no specific examination required of them. Instead, they are subject to the state’s discretionary power “according to the epidemic situation or the specific circumstance of the country [emphasis added]” where they have previously resided (Articles 3, the Health Regulations). This means that they are de facto exempt from examinations unless their staying in Taiwan reaches the threshold of three months’ duration and except for country-specific diseases.
Before 2015, Category B included foreign nationals teaching at publicly or privately funded education institutions and foreign-language cram schools. 3 If their employment in Taiwan was for more than three months, then they were required to submit a health examination certificate when they applied for or renewed their work permit (Articles 2 and 4 of the Health Regulations, 13 January 2004). Before 2005, the diseases for which they were compulsorily checked included HIV, tuberculosis and syphilis. Since 2009, they have also been required to submit proof of positive antibody or vaccination certificates for measles and rubella (Article 4 of the Health Regulations, 26 February 2009). In July 2015, HIV was taken off the mandatory examination list (Article 4 of the Health Regulations, 31 July 2015), after the government complied with the “international trend” of protecting HIV patients and relinquished its power to check non-citizens and expel those who were found positive (LY, 2015). Another change taking effect in July 2015 was to move educational professionals to Category A and keep foreign language cram school teachers within Category B. This makes cram school teachers the only group of foreign professionals subject to the abovementioned compulsory checks, a rationale of which, as stressed by the TCDC, was to reduce tuberculosis infection given the small teaching facilities at cram schools (Control Yuan, 2019: 19). Currently, as shown on the Health Certificate for Foreign Language Teachers, they are also subject to the state’s discretionary power to screen for any disease that is related to “the epidemic situation or specific circumstances” of their countries of residence (Article 4, the Health Regulations). This means that, subject to the same threshold of a three-month stay, cram school teachers’ additional examination is justified by their occupation, whilst they are also expected to be examined for country-specific diseases.
In Category C, resource-poor migrant workers engaged with “blue-collar” work in the care, construction, manufacturing, agriculture, fishing, livestock, forestry and aquaculture industries. Between 2001 and 2020, the numbers of migrant workers doubled from 326,515 to 711,539 (MoL, n. d.). Valid for contracts of two to three years, their employments constitute a taxonomy of “dirty, dangerous, and difficult” (3D) work, that is a key criterion applied by the MoL for permitting the employment of migrant workers which makes this “3D taxonomy” an entry ticket to the labor market of Taiwan. On the other hand, as Article 6 of the Health Regulations stipulates, this “3D taxonomy” also obliges them to undergo additional checks “in accordance with the nature of the occupation and the epidemic situation or the specific circumstances of the labor exporting country” [emphasis added].
The screening required by the Health Regulations was documented by the TCDC’s annual records between 2001 and 2020 (TCDC, 2021a). As detailed in these reports, migrant workers were examined for tuberculosis, HIV, syphilis and hepatitis B, the examination of which was also required of Category B workers. In addition, migrant workers were also checked for malaria, amoebiasis-related diseases, morphine and amphetamine addiction, typhoid fever, and leprosy (renamed as Hansen’s disease in 2009), mostly diseases that are more associated with the Global South. In addition to these geography-dependent diseases, female migrant workers were additionally screened for pregnancy between 1992 and 2017 (Cheng, 2020). This meant that for 25 years, the bodies of all Southeast Asian women employed in Taiwan had been regularly checked with a frequency (as discussed further below) that treated their sexuality and reproduction as contagious diseases. Although pregnancy clearance has been abolished, giving contraceptive injections to prospective female workers, including those hired by Taiwanese employers, remains a practice widely adopted by brokers in Indonesia (Cheng, 2020; 2021; online interviews with Indonesian workers in Macao and Hong Kong, 29 August and 20 September 2021). Currently, migrant workers are required to be checked by X-ray for tuberculosis, serological tests for syphilis, stool examinations for parasites, skin examination for Hansen’s disease, and to provide proofs of positive measles and rubella antibody or vaccination certificates.
To summarize, the above delineation shows that the hierarchy of sanitization is founded on differentiating between foreign bodies according to the duration of their presence in Taiwan, occupation and country of residence. This hierarchy is further enhanced by a geography of epidemiology where infection routes are mapped onto the residence of these foreign bodies. That is, the four “labor exporting countries”—Indonesia, Vietnam, the Philippines and Thailand— are reportedly high-risk for infection with measles and rubella, malaria, parasites and Hansen’s disease (Chang et al., 2017), whereas Indonesia was singled out for infections of typhoid fever, paratyphoid fever and bacillary dysentery (TCDC, 2015). In contrast, foreign professionals are presumed to come from less contagious countries. This presumption is endorsed by the TCDC, which stated that “their employment is stringently approved. Most of them come from advanced countries in Europe and America where infection monitoring and prevention is better than in labor exporting countries in Southeast Asia. … Moreover, we need their talent and skills and the infection risk is lower [in those countries]” (Control Yuan, 2019: 190–20). It is clear that although tasked to protect public health, the TCDC contributes to the belief in the economic benefit of employing foreign professionals.
In effect, this geography of epidemiology separates the “advanced countries in Europe and America” from the “labor exporting countries in Southeast Asia” (Control Yuan, 2019: 129–20). This geography of epidemiology is explicitly demonstrated on the Health Certificate for Residence Application used by foreign professionals when they apply for residency. The Certificate gives a list of countries where there is a lower rate of infection of tuberculosis, parasites, and Hansen’s disease, in Europe, North America and a few high-income countries in East Asia. A legal effect of this list is that foreign professionals from these countries are exempted from these intrusive examinations, whereas professionals from countries not in this list are subject to the state’s intrusion, particularly examination for Hanson’s disease for which examinees are required to remove their clothes except for underclothes. Obviously, there is a mismatch between this geography of epidemiology and the mobility of talents and skills. That is, although the Taiwanese state’s interest is to recruit talent and skills and strengthen international competitiveness, it can either privilege or discriminate against foreign professionals, the bodies carrying those talents and skills, depending on whether their country of residence is in the list of exempt countries. A professional worker, who is Indonesian by nationality and whose transnational family members are European passport holders, described this as a “privilege of passport.” That is, the European passport holders in the family were exempted for a stool examination but the Indonesian worker in the same household was required to submit a stool sample for examination (in-person interview, 13 July 2022). Clearly, this country-specific dichotomy between privileging and discriminating results in another hierarchy between professionals from “advanced” countries and those from countries perceived to be contagious.
A temporal regime and temporal–spatial demarcation
Temporality is essential to the sanitization of foreign bodies, since health, or illness, is time-sensitive. Thus, sanitization is sequenced into examination, treatment, re-examination, and the ultimate repatriation, which, in effect, constitutes a “temporal regime” that further differentiates between foreign professionals and migrant workers.
As mentioned above, foreign professionals are de facto exempted from health examination except for being subject to the state’s discretion based on their country of residence. For cram school teachers, for their employment, they are checked only once per contract. Should someone in these two groups decide to apply for residency, they are checked once upon application (Article 11, the Residency Regulations) for tuberculosis, syphilis, parasites, measles and rubella, and Hansen’s disease (Control Yuan, 2019: 12), with the possibility of exemption for those from “advanced” countries.
In contrast to this none-or-once-only examination, migrant workers are required to be regularly screened. This temporal regime constructs a chronological spectrum along which checks are conducted pre-arrival, upon arrival and post-arrival, with the entry port separating the space inside and outside the territory of Taiwan. This means that this temporal regime is also built on a clear spatial demarcation to shield Taiwan against the invasion of infectious diseases carried by migrant bodies from outside. This temporal–spatial demarcation is enforced by the first check conducted when migrant workers apply for a visa and work permit three months before entering Taiwan at one of the 74 hospitals recognized by Taiwan in the four Southeast Asian source countries (Control Yuan, 2019: 17). Failure to pass the pre-arrival examination will result in rejection of a visa (Article 5, the Health Regulations) and this will put an end to the employment and migration journey even before it starts (Lin and Chang, 2014). The second check is conducted within three days of their arrival in Taiwan. Afterwards, they are required to attend routinized screening in the sixth, 18th and 30th months of their residence (Article 5, the Health Regulations). Failing to pass post-arrival examinations or refusing to undertake examinations will terminate a work permit, leading to deportation. It is not uncommon for migrant workers who fail the health examination and fear the resultant deportation to abscond from their contract and government-monitored treatment. Absconding renders them a “runaway” in the eyes of the mass media. When law enforcement agents take them in for treatment, it has been described as arresting a criminal; infection increases the level of their perceived criminality (e.g. CNA, 2021).
The temporal regime is strengthened by the scheduling of follow-up checks or treatments since medical professionals advocate their effectiveness at reducing the threat to public health (Hsieh et al., 2010). Using “directly observed treatment short-course” (DOTS), which is premised on precisely dating patients’ treatment as a monitoring tool, Article 7 of the Health Regulations sets up a clear chronological chart marked by calendar days that require migrant workers to obtain another clearance or a certificate documenting their successful treatment. The effect of the temporal regime can be extended even after repatriation if it results from infection with amoebiasis-related disease or tuberculosis, since infected migrant workers are banned from re-entering Taiwan until they are cured or their illness stabilizes (Article 2, the Ban Directions). The ban is not lifted until the National Immigration Agency receives a Chinese- or English-language translation of their medical statement that has been verified by Taiwanese embassies in Southeast Asia. For tuberculosis patients, the medication has to meet the international standard of tuberculosis care (TCDC, 2021b).
Health examination as a temporal regime.
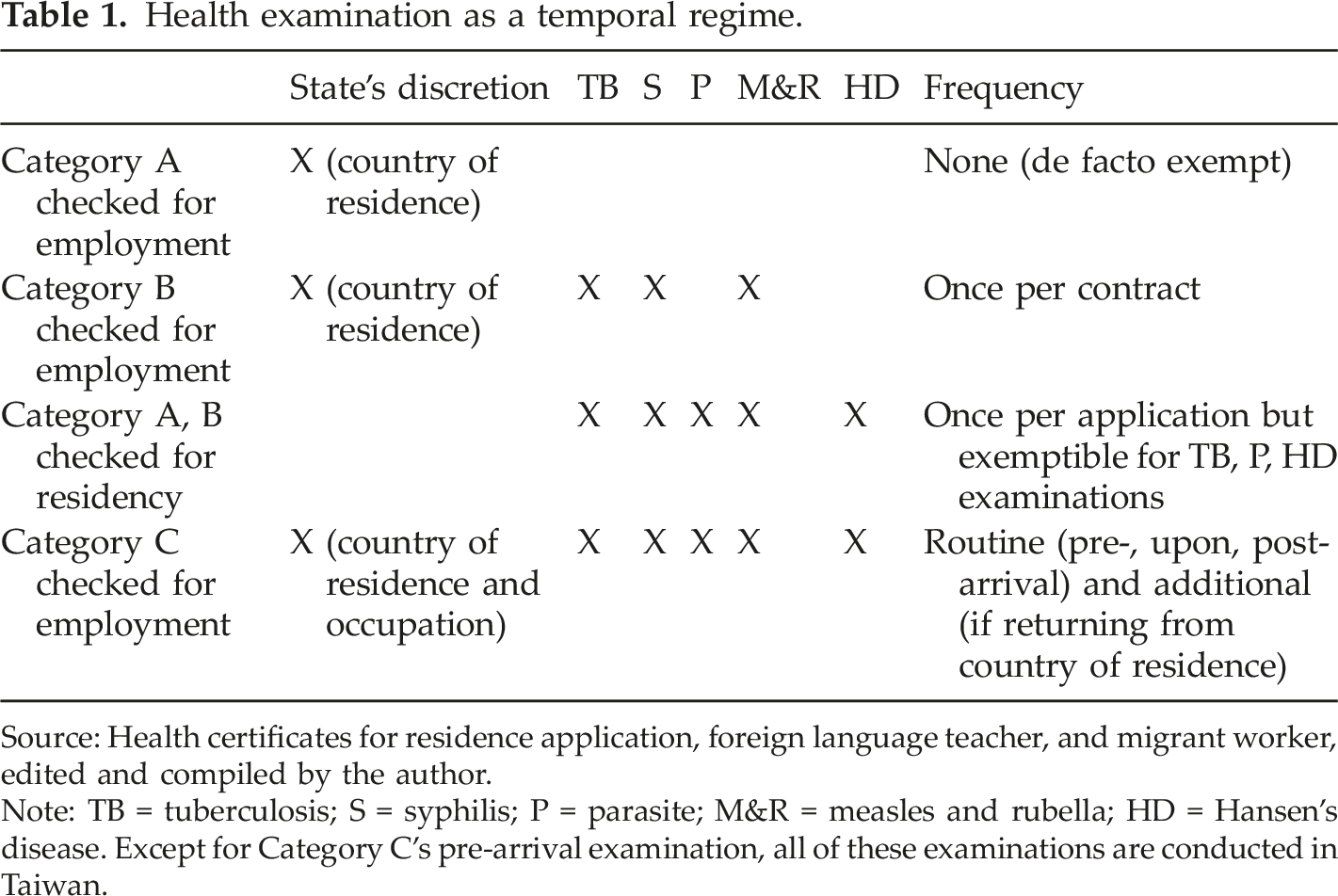
Source: Health certificates for residence application, foreign language teacher, and migrant worker, edited and compiled by the author.
Note: TB = tuberculosis; S = syphilis; P = parasite; M&R = measles and rubella; HD = Hansen’s disease. Except for Category C’s pre-arrival examination, all of these examinations are conducted in Taiwan.
This inequality is experienced in migrant workers’ everyday lives when the impact of the temporal regime is manifested as financial burdens, mental stress and, ironically, ill health. Financial burdens include the costs of examination (approximately USD 50 per examination) (MoL, 2022), transport, lost wages and, potentially, treatment if found infectious. Although the Prevention and Treatment of Infectious Diseases Act authorizes the government to provide funding for tuberculosis treatment and Hansen’s disease treatment is covered by National Health Insurance, migrant workers have to pay for treatment for amoebiasis-related disease, which costs between USD 100 and USD 240 (TCDC, Memorandum No. 1082100358, issued in 2019). By law, employers are obliged to assist migrant workers to receive treatment to ensure their rights to medical care and reduce the possibility of migrant workers’ absconding. However, without brokers assisting migrant workers with transport and interpretation, migrants may not be able to receive treatment, as brokers often ignore their requests for medical attention (Liang, 2019: 283–284; online interview with an Indonesian activist in Taiwan on 3 December 2021; interview with a Vietnamese worker in Taiwan on 17 December 2021). In fact, brokers make a profit out of repatriation since it creates vacancies that allow them to “import” workers from abroad or transfer workers within Taiwan to replace the ones dismissed and thus provides opportunities to charge recruitment fees. The indispensable cooperation of employers and brokers exacerbates migrant workers’ structural vulnerability and may lead to ill health and dismissal since poor health is perceived by employers as reduced productivity and a liability.
To sum up, before the pandemic made health examination in the form of regular lateral flow tests or ad hoc PCR tests a global routine, health examination implemented in the guest worker system adopted in Taiwan has built up a detailed temporal regime intended to keep contagion out of its territory. Categorizing foreign bodies according to their occupation, duration of stay in Taiwan and country of residence, this temporal regime processes them against a hierarchy of sanitization in which the bodies of professional and migrant workers are examined at different frequencies. This temporal regime is also supported by a geography of epidemiology where contagion is exclusively mapped onto routes from the Global South to Taiwan. The element of geography is further enhanced by the temporal–spatial demarcation whereby the sequencing of examinations is determined by whether migrant workers are inside or outside Taiwan. While all these deepen the inequality between migrant workers and foreign professionals (and within them), the inequality is also experienced by migrant workers as financial burdens, structural vulnerability vis-à-vis their brokers and employers, and potentially poor health. As analyzed below, the temporal–spatial demarcation and inequality continued during the pandemic when border-crossing was halted at the peak of the pandemic.
Temporal–spatial demarcation during the COVID-19 pandemic
From 7 February 2020 to the time of writing in March 2022, following the spread of COVID-19 from China to Taiwan in early 2020 (Wang et al., 2020), the Taiwanese government revised the restrictions on the entry of foreign nationals into Taiwan several times. In more than two years, different degrees of restrictions on entry and mobility with varying levels of rigidity concerning testing and quarantine were set, according to the levels of infection inside and outside Taiwan. On 19 May 2021, a semi-lockdown was announced (known as Tier 3 restriction), when a threshold between 2,533 confirmed cases were recorded as of that day (including 1,094 imported cases) and 23,393 confirmed cases (including 7,470 imported cases) as of 31 March 2022 (TCDC press releases, 19 May 2021; 31 March 2022). From 19 May 2021 to 7 March 2022, a blanket ban was implemented on the entry of all foreign nationals, except for international students, citizens’ families, residency holders and their families, and those who were granted special permission on humanitarian grounds (MoFA, 2022).
Without releasing the number of infected migrant workers, the TCDC continues to distinguish “domestic cases” from “imported cases” in its daily reporting on COVID-19 infection. This distinction clearly conveys the perception that contagious bodies from outside will bring infections into Taiwan. However, an overlooked aspect is that, at the peak of global infection, the previously unnoticed, or even mundane, temporality became the center of cross-border movement when temporality was experienced through PCR tests. In Taiwan, as early as in June 2020, no border-crossing could be attempted without a PCR test conducted 72 hours prior to take-off, followed by another PCR test immediately after landing and one more conducted between the 12th and 14th days of the mandatory 14-day quarantine (MoFA, 2022). The sequencing of pre-, upon-, and post-arrival PCR tests is determined by whether the tested body is outside or within the cordoned territory with the entry port conceptualised as the borderline. This temporal–spatial demarcation is the same as that for health examinations required of migrant workers, albeit the interval between each PCR test is measured by smaller temporal units of hours and days rather than by months. This precise “temporal regime” punctuated by itemised intervals saw the state and individuals jointly entering an exercise of counting the passing of time when temporality meant lineal progression.
On the other hand, when the prospect of border-crossing was written off, individuals, citizens and foreign nationals, were deprived by the Taiwanese state of their agency for forward planning. In this light, temporality lost the meaning of chronological and lineal progression. For migrant workers stranded in Taiwan, the deprived border-crossing movement and the lost temporal progression meant that they were locked in a state of “eternal present” (Anderson et al., 2011: 77). The “eternal present” was particularly lived by workers who did not have a legal residence status due to absconding from their contracts or overstaying their visitation visa or work permit. Stepping outside of legality meant being out of reach for testing or vaccination, a perceived threat to public security popularly known as “infection control breach.” The threat was potentially mitigated by the government’s offer of amnesty and deportation when flights were still available; later it was met with free vaccination when air travel became scarce in supply (Lan in this issue; interview with an irregular Vietnamese worker in Taiwan, 17 December 2021).
On top of the ban on entry, the precise and itemized temporal regime, the potential of failing PCR tests, and the resultant immobility destabilized the supply of migrant labour to Taiwan, contributing to an economic recession. As discussed above, migrant workers’ health is viewed by the receiving state as an issue of productivity and a threat to public health. Under the challenges of a pandemic-induced economic downturn and pressure from employers for cheap labour (MoFA, 2022), the interests of productivity outweighed security concerns, and Indonesian workers were permitted to enter Taiwan from 11 November 2021 onwards. Thai, Vietnamese and Filipino workers were permitted from 30 December 2021 and 15 February 2022 respectively (MoFA, 2022). This permission was based on the “sound” prevention measures adopted by the Indonesian government and its promise to closely monitor brokers’ prevention measures (MoFA, 2022). This permission belies the fact that, as noted above, before the pandemic, Indonesia was singled out as a particularly infectious country with the likelihood of rigging health examination results and during the pandemic, Indonesia was declared a high-risk country in March 2021 (Cheng, 2021; MoHW, 2021: 4; MoFA, 2022). This contradiction suggests that in order to ensure productivity and international competitiveness, the Taiwanese state was willing to accept health examination results obtained outside of Taiwan (MoHW, 2021: 4).
A temporary solution to the interrupted cross-border labor supply and the subsequent “scramble for labor” is to allow limited mobility among migrant workers who were locked in an “eternal present” in Taiwan. This is another instance where the Taiwanese state, similarly to its Singaporean and Malaysian counterparts (online interviews with activists in Singapore and Malaysia on 28 September 2021, 7 March 2022), chose to deviate from its practice of denying migrant workers occupational mobility, a hallmark of the guest worker system adopted by all three states. That is, in the “state of exception” (Schmitt, 2011) and in the name of emergency, the MoL temporarily (between 29 October 2021 and 30 June 2022) allowed workers to move from one employer or industry to another to meet employers’ pressing need for cheap migrant labor (MoL, 2021a). The loosening of occupational mobility prolongs migrant workers’ stay in Taiwan, which requires them to be checked during their extended presence. Thus, Article 13 of the revised Health Regulations (effective since 19 May 2021) grants the government the power to adjust health examination requirements on migrant workers. This enables the government to show flexibility towards, rather than suspension of, the scheduling of the arrival and post-arrival examinations. First of all, on 11 March 2020, the government announced a grace period of three months for migrant workers to undertake their pre-defined arrival and post-arrival examinations. Secondly, for those workers who are allowed to move to a new contract, if they have not undertaken an examination for more than one year after their thirtieth-month examination, the TCDC requires them to receive a “supplementary examination” within seven days after their contract is renewed (TCDC, Memorandums No. 1093600382 issued on 12 October 2020, and No. 1102100467, 15 October 2021). On 19 May and 19 July 2021, the 3-month grace period was reinstated and also applied to “supplementary examinations” (TCDC, Memorandums No. 1103600193 issued on 19 May 2021, and No. 1103066386). Despite this flexibility, the insistence on examining migrant workers’ bodies is in strong contrast to the suspension of health examinations for cram-school teachers, effective from 9 July 2021 until the COVID-19 prevention measures are lifted (MoL, 2021b). This is another clear example of the implementation of the “lax for the white-collar, strict for the blue-collar” principle and its resultant inequality.
The analyses above show that the temporal regime and its constituent elements of temporal–spatial demarcation and hierarchy continued to apply during the pandemic. In ways identical to the pre-pandemic health examination, the sequencing of PCR tests also boasted a temporal–spatial demarcation that was intended to stop COVID-19 from entering Taiwan or to contain its spread once the suspect foreign body entered Taiwan. The difference was that during the pandemic the demarcation and screening was measured by the hour and day rather than by the month. The closure of borders left migrant workers stranded and fixed them in an “eternal present,” frozen in time with dim prospect for forward planning. The hierarchy of sanitization also continued and was manifested by temporarily exempting cram-school language teachers from their once-per-contract examination but insisting on examining migrant workers for non-COVID-19-related infectious diseases. On the other hand, the pressing need for cheap labor temporarily weakened the grip of the geography of epidemiology and wrote off the contagious image of Indonesia and three other “labor-exporting” countries when their workers were allowed to return to Taiwan in order to reinvigorate the ailing economy.
Conclusion
Seeing that health is time-sensitive and temporality is an understudied aspect of migration, this paper set out to investigate how temporality is embedded in the biopolitical governmentality of foreign nationals’ health examinations as regulated by the Taiwanese state. Analyzing how the differentiation of health examination regimes evolved, this paper shows that although foreign professionals and migrant workers are desired, for their skills and as cheap labor respectively, they are also seen as a potential source of infection. However, this perception does not equally affect the two groups, who have unequal resources to ensure their personal health. Instead, they are slotted into a hierarchy of sanitization whereby the degree of the state’s intrusion into their bodies is contingent on their perceived economic usefulness and their countries of residence.
In elucidating the creation of this hierarchy of sanitization guided by the principle of “lax for the white-collar, strict for the blue-collar,” this paper found that it is built on the perception of a geography of epidemiology. Therein, the four “labor-exporting” countries in Southeast Asia are seen as more contagious than the “advanced” countries in Europe, America and East Asia. As a result, better-resourced foreign professionals are far less frequently checked and are most likely to be exempt from intrusion into their bodies. On the other hand, the geography of epidemiology also erects a dichotomy amongst foreign professionals by privileging those from “advanced” countries and discriminating against those from elsewhere. In comparison, not only because of the geography of epidemiology but also due to their contagious occupations, migrant workers are routinely and far more frequently checked. This regularity and frequency render migrant workers, who have fewer resources to protect their health, more likely to be repatriated because of the temporal regime as well as their employers’ interest in shedding liability. Thus, although health examinations are justified as protecting the health of the public against epidemic infection, in effect, it also serves the interests of the state and employers in ensuring that migrant workers deliver the level of productivity expected of them. In this sense, this biopolitical governmentality is similar to that of the examinations used in the German Gastarbeiter (guest worker) system (Topp, 2014). In everyday life, this temporal regime is experienced by migrant workers as financial burdens and structural vulnerability vis-à-vis employers and brokers. Although treatment is available to them, lacking brokers’ cooperation as well as their concerns with financial loss and repatriation can potentially lead to ill health.
Built into the temporal regime, the temporal–spatial demarcation that determines the sequencing of health examination is at the core of the fight against the COVID-19 infection. It became a joint exercise between the state and individuals to count the passing of time by hour and day, rather than by month. When cross-border mobility was halted, temporality lost its sense of chronological progression and stranded migrant workers in the frozen situation of an “eternal present.” Although COVID-19 knows no ethnicity when causing illness or claiming lives, the temporal regime continued to distinguish between foreign cram school teachers and migrant workers. In the name of emergency and to reduce risk, health examinations for the former have been suspended, whereas the latter continue to be checked, although with a degree of scheduling flexibility.
To conclude, this paper demonstrates how a temporal approach to health examination facilitates an innovative lens through which to understand the temporal–spatial complexity of migration (Donnan et al., 2017). It elucidates that before and during the pandemic, the biopolitical governmentality, realized by the temporal regime, hierarchy of sanitisation, geography of epidemiology and temporal–spatial demarcation, deepened the inequality between migrant workers and foreign professionals. It perpetuates the former’s temporariness by subjecting their bodies to regular, additional and intensive intrusion. A temporal approach to health examination shows how a “migration state” (Hollifield et al., 2008) takes advantage of migrant labor and excludes them as eternal outsiders suspected of carrying and spreading contagion because of their occupation and origin.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ note
This is a paper for the Special Issue on: “The politics of sanitization: Pandemic crisis, migration and development in Asia-Pacific,” organized by Yuk Wah Chan and Pei-Chia Lan.