
Abstract
The objective of this study was to describe a panel process of selecting interventions to reduce unnecessary interruptions in clinical nursing. Interruptions in nursing may jeopardise patient safety, disorganise planning, and lead to ineffective working procedures. The Delphi panel process may be useful to create consensus on interventions to reduce interruptions. Using the Delphi method, a structured group-based decision-making tool, a panel of 14 nurses agreed on interventions to reduce interruptions. The results showed that a consensus on reducing interruptions was reached in four focus areas: expectations, physical framework, work procedures, and medication room procedures. The panel process was chosen as a means to involve nursing staff to create consensus and ownership about interventions. Our conclusions are that the Delphi panel process was a feasible method of selecting multi-factorial interventions to reduce interruptions. The panel process contributed to dialogue, staff involvement, and competency development. Further prospective studies are needed to explore whether these multi-factorial interventions can reduce unnecessary interruptions and improve patient safety.
Introduction
It is said that nurses can be interrupted every sixth to ninth minute. An interruption means leaving a task, and creates a change in context or thoughts. Interruptions may lead to delay in working routines.1,2 The consequences are wasted time, disordered planning, ineffective working procedures and disrupted reflective processes.3,4 Additionally, there is a growing problem with errors caused by interruptions.3–9 Thus, it may lead to reduced patient safety if nurses are not concerned about interruptions. There is a need for new knowledge to develop interventions to reduce unnecessary interruptions in clinical nursing.2,9–11
Background
Within the last decade, research on interruptions and especially the association between interruptions and medication has expanded.3,4,8,9,12–14 Interruptions challenge nurses due to a dilemma between being accessible and staying focused. 2 Interruptions lead to a constant rearrangement of priorities and may induce a feeling among staff of being ineffective and under time pressure; this can cause reduced job satisfaction and produce stress-related symptoms.5,15
Interruptions affect decision-making processes because of changed awareness and a shift of focus. 16 They may lead to reduced precision and increased time spent on problem-solving. 10 The consequences for nurses are feelings of incompetence, being under time pressure, and disrupted care relations, leading to a need for strategies to keep up with the pace of work. 12
Depending on the context, nurses distinguish between necessary and unnecessary interruptions.17,18 Necessary interruptions can be external or self-inflicted, and contribute to getting an overview of work procedures, sharing information, competence development or teamwork. Unnecessary interruptions negatively affect organisation of work, attention, relations with colleagues and patient safety, and may also impact negatively on patient–nurse interaction.2,9 An interruption is different for the interrupted and for the sender respectively, and interruptions distress behaviour differently depending on the person, frequency, period, complexity and circumstances.8,19
The primary sources of interruptions are health professionals, followed by the surrounding environment such as background noise and small talk. 20 An observational study showed that in 41% of interruptions, people never returned to or finished the original task, keeping in mind that it takes up to 20 minutes to restart the task. 21 The short-term memory only contains five to nine units at a time; if new information appears, other information is tossed aside. 22
Studies describe different ways of reducing interruptions but they are often based on single interventions and mostly related to the administering of medication.9,23 Few studies suggest multi-factorial interventions as a more effective way of reducing interruptions during medication procedures.14,15,24 Relihan et al. found that by using no-talk signs, quiet zones and ‘please do not disturb’ vests, interruptions could be reduced during administering of medication. 24 Furthermore, certain educational and environmental interventions have been shown to reduce interruptions.14,25 Studies have investigated the consequences of interruptions in clinical nursing, but there is inconsistency concerning the process of choosing interventions to reduce these interruptions.
The aim of this study was to describe a panel process for choosing interventions to reduce unnecessary interruptions in clinical nursing.
Methods
A pilot study was carried out in 2011 to identify the nature of interruptions in our department, and to investigate how nurses cope with interruptions in clinical practice. 26 The participating nurses found interruptions to be aggravating and stressful, but interruptions also contributed to gaining an overview, sharing knowledge, and to being part of a team. Furthermore, nurses often interrupted their own colleagues with doubts/questions. This pilot study was used to prepare the first-round panel meeting to choose interventions to reduce interruptions.27,28
We selected the Delphi method (Delphi) to develop meaningful interventions to reduce unnecessary interruptions for nursing leaders and staff. In this paper we focus primarily on describing the panel process of this method. We will only briefly present the selected focus areas and derived interventions to prevent interruptions, since we have not yet investigated the impact of implementing these interventions.
Delphi is a structured group-based decision-making tool that affects ways of thinking through dialogue and prioritising. 29 It is a validated and widely accepted method to achieve convergence of opinions concerning everyday-world knowledge from different perspectives.26,29 It has been used in various studies on programme planning, needs assessment, policy determination, resource utilisation, and development of nursing practice.26,29,30 It can facilitate the development of alternatives, be used to explore or expose underlying assumptions as well as to correlate judgments on a topic spanning a wide range of disciplines.26,29 We assumed that the Delphi was suitable for our purposes.
The process encompassed self-administered scoring forms and panellist meetings between August and October 2011 at a surgical department with a nursing staff of about 170 nurses. The process consisted of rounds of feedback from the panellists using both anonymous surveys and round table meetings.
The number of subjects in a Delphi panel is recommended to be between 10 and 50 to constitute a representative and homogeneous pooling of judgments and information processing capabilities. 29 The panellists included the head nurse, five charge nurses, six registered nurses – all interviewed in the pilot study – an education and development nurse, and a senior nursing researcher. We chose these 14 panellists strategically to represent different job positions and competencies, up-to-date knowledge on the topic, and experiences in clinical nursing. 29 To avoid impact of pre-understandings, the panellists were unaware of the results of the pilot study before starting the panel process.
Data collection and analysis
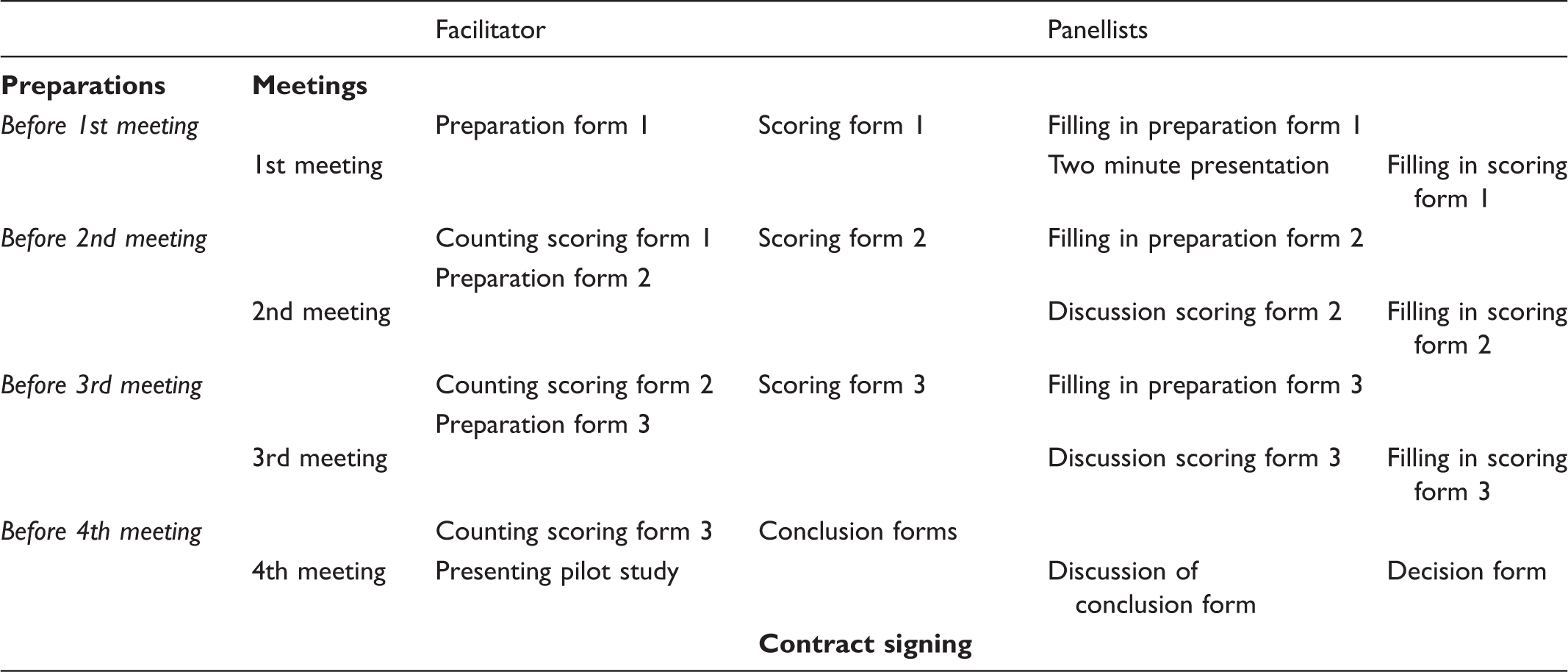
The process was based on anonymity, repetition, validation and feedback to ensure broadness, convergence, creativity, effectiveness and consensus. 29 The repetitions related to the meetings were expected to make the panellists more oriented towards problem-solving, to encourage them to offer their opinions more insightfully and to minimise noise. The process consisted of interactions between the panellists where prioritisation, dialogue and summaries of intervention were emphasised. The content of the panel meetings was listening and responding to written statements, and exchange of opinions, positions and attitudes. Each panel meeting round consisted of a preparation, a meeting and a compilation phase. 26 The rounds were held at two-week intervals during the daytime to involve as many panellists as possible.
Distribution of roles of the panellists in the four Delphi panel round meetings.
Ethical considerations
The department management approved the study. Participants were informed about the Delphi process in a briefing session concerning: the purpose of the project, the content, information about their role, and their right to withdraw from the project. Before the briefing session, participants received a short description about the project by email. The panellists gave written and oral informed consent during the briefing session, and complied with rules on confidentiality. An open and trustful atmosphere was pursued to secure loyalty to personal statements and content of the meetings. Researchers and participants were acquainted with each other, which might have impacted on their voluntariness. However, the request to reduce unnecessary interruptions came from the clinical nurses. In this way the project was a joined decision. All tape-recordings were deleted after completion of the study. Due to Danish law the study was exempt from approval by the local Human Research Ethics Committee and the Danish Data Protection Agency.
Rounds in the panel process
To develop consensus concerning interventions, we took 60 days and used four panel meeting rounds.
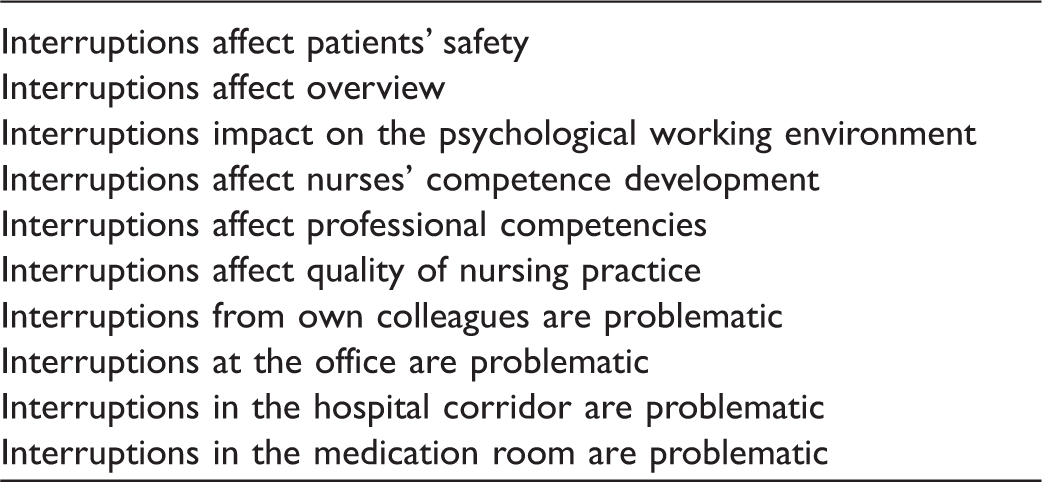
Before the first meeting: Preparation form 1 included 10 statements based on findings from the pilot study; this was emailed to the panellists, who scored the statements. The 10 statements are shown in Table 2.
Ten statements from a pilot study on interruptions in nursing practice. The statements appeared in interviews and observations.
First-round panel meeting: This meeting featured only reflection and no dialogue. The first round is typically qualitative and designed to ascertain the broadness of the topic for the panellists.26,27 Initially, each participant gave a two-minute presentation. The other panellists were not allowed to comment or interrupt. Afterwards scoring form 1 was handed out and panellists were given 1.5 minutes to mark their agreement of the statements. Then each panellist’s scoring form was circulated among the panel for one minute each. Each panellist responded to the scorings of the other panellists by marking their level of agreement.
Before the second meeting: The facilitator listened to the tape-recording from the first meeting to extract the essence of panellist presentations, and counted the completed scoring forms, on the basis of which preparation form 2 was composed. Preparation form 2 was emailed to the panellists, who scored the statements. The facilitator counted the scorings and composed scoring form 2.
Second-round panel meeting: Scoring form 2 was handed out to the panellists to form the basis of a 30-minute plenum discussion. Afterwards each panellist wrote the two most important conclusions from the discussion. The panellists were given 1.5 minutes to mark agreement of the statements on scoring form 2. Then these scoring forms were circulated among the panellists for one minute each. Each panellist responded to the scorings of the other panellists by marking their level of agreement.
Before the third meeting: The facilitator listened to the tape-recording from the second meeting to extract the essence of the discussions, and counted the completed scoring forms, on the basis of which preparation form 3 was composed. Preparation form 3 was emailed to the panellists, who scored the statements. The facilitator counted these scorings and composed scoring form 3.
Third-round panel meeting: Scoring form 3 was handed out to the panellists for a 30-minute plenum discussion. Afterwards each panellist wrote suggestions and ideas for possible and relevant interventions to reduce unnecessary interruptions. The panellists were given 1.5 minutes to mark agreement of the statements on scoring form 3. Then these scoring forms were circulated among the panellists for one minute each. Each panellist responded to the scorings of the other panellists by marking their level of agreement.
Before the fourth meeting: The facilitator listened to the tape-recording from the third meeting, gathering suggestions and ideas for interventions, and counted the completed scoring forms 3. A conclusion form was composed and emailed to the panellists.
Fourth-round panel meeting: The facilitator presented the findings from the pilot study and the conclusion form was discussed. Afterwards interventions were determined and a decision form was composed. The panel process ended with all panellists signing a contract and by evaluating the panel process.
Results
Benefits of the panel process
The benefits of involving nursing staff in the panel process were mainly positive both personally and professionally: It was a positive process with many eye-openers and extra benefits. (Head nurse of the department) It has given more insight into other peoples’ working procedures. (Department nurse) It has contributed to my own competence development. (RN)
As intended, the panel process created time, space and room for reflection and for presenting considerations about interruptions without being disturbed. This was pointed out as important for further reflection. Even though the panellists had different in-depth knowledge of interruptions, and although the process was time consuming, sharing these experiences qualified the results and created new angles to the topic. It created awareness of and legitimised the problem of interruptions. The process has been a revelation for managing complex problems: The big blurred subject has become more tangible. (Department nurse) I have become more curious; it is exciting, practice-related and applicable. (Department nurse)
Furthermore, the process has created alternative ways of thinking: It was another way to meet, not only talking knowledgeably about things. (Department nurse) There is recognisability related to my participation in an interview, where it then was more emotional and experience-based, it is now more concrete. (RN)
Interventions to reduce interruptions
Focus areas and interventions to reduce interruptions in clinical nursing developed through a Delphi panel process.
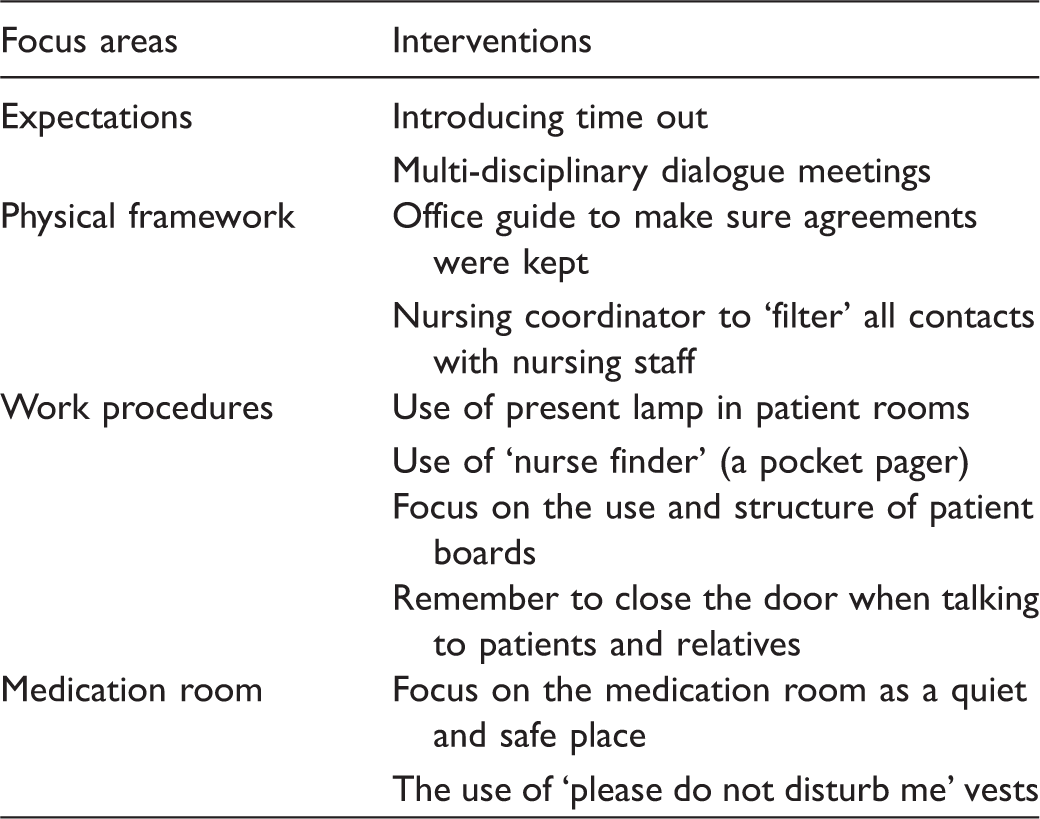
Time out was chosen to legitimise the right to put one’s foot down in situations when the nursing staff did not wish to be interrupted. Simultaneously, time out will be introduced in each shift to minimise interruptions related to progression of work. Dialogue meetings with other health professionals will be held to optimise the right time for e.g. the physiotherapist to ask about a patient’s condition or when to mobilise a patient.
Physical framework encompassed introducing an office guideline promoting a quiet atmosphere in the nursing office, reducing traffic jams in the hallway, optimising administrative working procedures, and reducing small talk at the office. The nursing coordinator will be used as a gatekeeper for interruptions e.g. by prioritising external calls, and making arrangements with doctors, physiotherapists or relatives.
For work procedures, we reached consensus about the use of lamps to indicate when nurses are caring for patients in patient rooms. Additionally, by operating a pocket pager in the team the nurses can triage patients’ calls as the pager selectively chooses the appropriate team members. The pocket pager also contributes to a quiet working environment (reducing background noise). The patient board will be more structured and used optimally, and encompass agreed-upon information. Moreover, we will focus on closing doors and using the occupied sign when having conversations with patients and relatives.
Finally, to minimise interruptions in the medication room, attention will be on displaying ‘do not disturb me during administration of medication’, and ‘do not disturb me’ vests will be implemented.
Discussion
In the Delphi panel process we aimed at selecting interventions to reduce unnecessary interruptions in nursing practice. We demonstrated that the process was a feasible way to involve nursing staff through dialogue and to achieve consensus about selected interventions. The outcome of the panel process was agreement on four focus areas to reduce interruptions: expectations, physical framework, work procedures, and medication room procedures.
We chose to highlight the panel process in Delphi. The process is described as multi-stage where each stage builds on the results of the previous stages. 28 This forecasting activity is defined to be iterative to achieve consensus as well as to determine, predict and explore panellists’ attitudes, requirements and main concerns.26,28 Delphi has been used in different fields including nursing and healthcare. 26 However, Delphi is often not used in the same way, and modifications to the original version are extensive. 28
To avoid subject bias, anonymity offers an opportunity for each panellist to introduce and respond to ideas without bias based on the identities of others. Anonymity may thereby facilitate an open-minded and truthful approach. In this way each opinion carries the same power and is considered equally important when reaching consensus. 28 The panel process also includes plenum discussions. Most of the panellists knew each other and to prevent panellists feeling pressured, and to divide speaking time equally, the facilitators led the panel meetings, discussed the process after each meeting, and listened to the tape-recordings of the meetings. Hence, our process reflected quasi-anonymity rather than anonymity.28,32
Earlier studies have focused on single interventions to increase patient safety by reducing interruptions related to medication. 9 Multi-factorial interventions could result in a higher level of compliance since different approaches appeal to people in diverse ways. According to the Theory of Planned Behaviour, different background factors affect the ability to change habits beside reasoned modes of operation; these factors are impulsivity and ability to act on intentions. 33 Different interventions could motivate different individuals to change habits, as nurses adapt to changes in different ways. 34 However, individual learning and working styles have a considerable impact on the success of implementing the selected interventions. Willingness to adapt is personally and socially processed. 33 Since interruptions are related to habits, we believe the chosen interventions to reduce interruptions should involve changing habits in a social context. We assume that multi-factorial interventions have more impact on successful change of habits, because interruptions affect behaviour depending on the person, frequency, duration, content, complexity and context. 8 While nurses have different attitudes towards interruptions it is important to involve all parties for whom Delphi was appropriate. 29 It is, however, unknown whether the chosen multi-factorial interventions can reduce interruptions; further prospective studies are needed to confirm this.
Obtaining consensus in our panel process does not necessarily mean that the right intervention to reduce interruptions was identified, since the result from the process cannot replace rigorous scientific work. 26 In this thinking Delphi can lead us to place larger confidence in our results than might be reasonable. 28 Yet, the role of the facilitator has been described as to ensure that all participants are able to express their understandings by controlling the dialogue, and to prevent a particular interest or predetermined opinion from dominating. 30 Hence, we aimed at not forcing through consensus, and allowed the participants to debate subjects letting opportunities arise for respondents to elaborate on their perceptions.
Jones and Hunter describe two levels of making agreements. 30 Firstly, the level to which each participant agrees with the question rated on a numerical or categorical scale. Secondly, the level to which respondents agreed with each other. During the panel process different competencies and interpretations about interruptions were clarified among the panellists (i.e. how listening to reflections of others affected own attitude and position among panellists). We thus used the process in both levels of agreement with consensus measurement and consensus development. 30 As a spin-off in the panel process, we made it possible to become more familiar with each other and learn how to work together. 29 Additionally, the panel process may be a useful revelation, which may be transferred to similar processes where teamwork is important.
Strengths and weaknesses
This study aimed at following the Delphi approach. 29 The 14 panellists represented leaders and nurses from all wards in the department with different competencies, interests and insights into the field of interruptions. Literature suggests that the panellists must at least be practising in the field under consideration.26,30 Nurses being interviewed in the pilot study were involved; this may likely have impacted on their reflections about interruptions. However, there is always a risk of bias in the selection of participants, which may have affected the chosen intervention to reduce interruptions. 30 Nevertheless, having knowledge of and experience with interruptions does not automatically mean being an expert on the topic. Furthermore, the panellists can often not be both a representative sample of the nursing staff and experts – these characteristics may be mutually exclusive. 28 We assumed that the number of panellists was representative of different positions and attitudes that needed to be challenged. Regarding implementation, more panellists might have enhanced the chance of success. The panel process is based upon the hypothesis that more participants are less expected to reach a wrong conclusion than a single individual. 26 However, the evaluation showed agreement among the participants about their opinions being respected, the process being fair, and no one altered their responses or opinions as a consequence of being pressured. Furthermore, the use of successive rounds and the progression in the preparation forms may have helped us to enhance validity. Still, it is uncertain if a repetition of the panel process with other panellists would result in exactly the same interventions to reduce interruptions.26,28
To reach consensus about statements in the panel we used a cut-off at 60% on the four-point Likert Scale. The Likert scale is frequently used in Delphi studies. 35 However, the methodology is criticised for being sub-optimal, since a transformation of nominal to numeric measurement can result in the panellists failing to recognise their contributions. 27 Different cut-off points and different scales are used in the literature. Some have made the criterion for consensus at 80% of the panellists’ scoring within two categories on a seven-point scale; others recommend that at least 70% of the panellists rate three or more on a four-point Likert Scale with a median at 3.25 or higher.27,29,35 Nevertheless, the use of different scales and different cut-off points makes it difficult to compare our results with others.26,36
The facilitators chose only to present the statements from the pilot study, not the findings of the interviews and observations, to avoid the impact of panellists’ pre-understanding of interruptions and to make the process as objective as possible. On the other hand, knowledge of the pilot study could have motivated and qualified the interventions during the panel process.
Some panellists were present at all meetings and others were not. This might have influenced the insight and continuity of the process, misinterpretations or loss of nuances and ownership.26,37 The panel process is highly dependent upon the participants’ obligation in the process. It is central that those who have agreed to contribute sustain involvement until the process is completed. 26 To minimise cancellations, meetings were held after day shifts, and written information was delivered accompanying the first round. The panellists’ understanding of the purpose of the process was highlighted to encourage ownership. Still, although all agreed on the final decisions, the consequences of cancellations may be lack of ownership and thus commitment to prioritise interventions to reduce unnecessary interruptions.
The panel process was time-consuming, as we emphasised the importance of making room for reflection. This resulted in the process being educational both personally and professionally. Furthermore, to obtain an adequate level of consensus, four rounds were necessary as described in the classic original Delphi approach.28,30 Four rounds have been criticised for creating sample fatigue. 26 We did not experience sample fatigue, as the process demanded reflection on each participant’s own response as well as the response from the other panellists.
Conclusion
In this structured Delphi panel process we created consensus about interventions to reduce interruptions in nursing practice. We found the process a feasible and transparent method to select multi-factorial interventions. The panel process has led to inspiration, competence development and enthusiasm among the panellists. It has created awareness of individual and group-based positions and behaviours, and has strengthened team spirit. The selected interventions were related to four areas: expectations, physical framework, work procedures, and medication room procedures. Further prospective studies are needed to explore whether these multi-factorial interventions can reduce unnecessary interruptions and improve patient safety.
Footnotes
Acknowledgements
We wish to thank the nurses from Department of Cardiothoracic and Vascular Surgery at Aarhus University Hospital for participating in the Delphi panel and for helping us in identifying and prioritising interventions to reduce interruptions in clinical nursing.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.