
Abstract
Caesarean section (CS) on maternal request is increasing. There is a need to understand why, and find measures to help women give birth vaginally. The purpose of this study was to compare the rate of complications in the first birth of 129 second time mothers wanting caesarean section with the rate of complications in the general population; to determine how many changed their mind and wanted to give birth vaginally when given the opportunity to know their midwife in advance; and to examine whether there were any differences in the prevalence of health problems and labour complications between the known midwife group and those maintaining their wish for a CS. A quantitative study based on data from The Medical Birth Registry and from medical records was carried out. The findings show that 129 women had experienced significantly more complications than the general population during their first birth. Among the 48 women joining the ‘known midwife group’, 81% gave birth vaginally. The 81 women maintaining a demand for CS significantly more often had a health problem and fear of childbirth before their second pregnancy and were delivered by elective CS in their first pregnancy. Our conclusion is that interventions such as the ‘known midwife project’ help some women with a wish for a CS to give birth vaginally.
Introduction
In Rikshospitalet in Norway every fourth caesarean section (CS) in 2007 was performed on maternal request (unpublished data). From 2006 to 2012 there was a programme to help these women to cope with their childbirth fear, change their mind and decide on a vaginal birth. The 129 women in this study were referred to the known midwife group by the doctor or midwife to whom they initially presented a wish for a CS. The women then met with a midwife with special training in communication and were offered to take part in the ‘known midwife project’, which meant they got to know two or three midwives during pregnancy. The midwives met with the women and often their partners 2–5 times during pregnancy. During these meetings, they discussed an individual birth-plan and the midwife gave an opportunity for the woman to explain her particular fears and worries. At one of these meetings the woman and her partner were shown the labour ward. One of these midwives would then attend the birth.
Aim
The main purpose of this study was to compare the rate of complications in the first birth of 129 mothers wanting CS in their second pregnancy with the rate of complications in the general population of Norwegian first time mothers. Secondly, we wanted to determine how many changed their minds and decided to give birth vaginally when they got to know their midwife in advance. We also looked for differences in the prevalence of health problems and labour complications between those changing their minds and the ones maintaining their wish for a CS.
Review of the literature
The WHO states that the ideal caesarean section rate is 10–15%. 1 Above this rate there have not been shown to be any improvements in foetal or maternal outcome. On the contrary, a CS rate above this level leads to an increase in perinatal morbidity and in maternal morbidity and mortality, compared to vaginal births.2,3 Pregnancies after CS involve increased risk of miscarriages, stillbirths and death related to the scarred uterus which lead to placental complications and uterine rupture. 4 The limit on CS rate set by the WHO is by far exceeded by both Western and many non-Western countries. In 2011 the CS rate in the North American region was 32%, in Europe 22% and in Norway 17%. 5 A systematic review from 2003 shows the cost for a CS to be between £1238 and £3551, which is two to three times more than for spontaneous vaginal births. Patients having a CS stayed almost twice as long in hospital. 6 Given the high rates of CS today, this is a considerable economic burden on many nations’ health budgets.
The indications for CS have changed over time. A Swedish study reports that the CS rate increased from 11% to 20% from 1992 to 2005. In this period, the most frequent indications for elective CS changed from malposition or uterine factors, to CS without medical indication or on maternal request. However, including only urban women this study might not be representative for the general population. 7 The prevalence of CS on maternal request has been estimated to be between 7% and 22% of all CSs in the United Kingdom, Finland and Sweden. Of all pregnant women, 6–10% suffer from serious childbirth related fear often leading to a wish for a caesarean. 8 Many women with a wish for CS have experienced more difficulties earlier in life, both on the physical, social and psychological level, such as abortions, infertility problems or stillbirth. Women with a wish for a CS are more likely to be multiparous with negative experiences of previous births often with an operative outcome.9,10 A previous CS is a strong predictor for wanting a CS in a subsequent birth.10,11 It is known that a bad experience in the first birth can often lead to a wish for a CS in the next pregnancy, but little is known about these first births. 9
Given the health benefits of vaginal birth for women and children and the increasing number of CSs on maternal request, it is important to find ways to help these women to want to have vaginal births. There have been some studies on programmes aimed to help women with a fear of childbirth and who request a CS to cope with their anxiety, to change their mind and wish for a vaginal birth. In one Norwegian project, two midwives with psychiatric specialty had therapeutic conversations with the patients. Of these women, 86% changed their mind and wanted a vaginal birth after the therapy. 12 In a Swedish study, 68 women with serious childbirth related fear and who had requested a CS were treated in an out-patient psychosomatic clinic. Each woman got individual psychological and obstetrical support and 50% re-decided and opted for a vaginal birth. 13 A Finnish study of first time mothers with a fear of childbirth compared intensive therapy during five consultations with both midwife and psychotherapist, with two consultations with an obstetrician. Of the 102 women in the midwife and psychotherapist group, 82% changed their mind and planned a vaginal birth versus 67% of the 85 women in the obstetrician group. 14 The majority of women who wish to give birth by CS have experienced a previous complicated or traumatic birth. 15
Methods
Design
This paper presents a retrospective register study based on birth records from the hospital where the study reported was carried out, and on data from the Norwegian Medical Birth Registry.
Participants
The study population consisted of second time mothers who came to the Maternity Ward with a request for a CS and were offered to participate in the known midwife project. We chose to include only second time mothers to avoid possible bias associated with mixed experiences of women with more than one birth experience.
Data collection
The women presented their request for CS at different times during pregnancy, some in the first trimester others late in the last trimester. In order to identify the ones who did not wish to participate in the known midwife project, all 349 medical records of second time mothers with CS on maternal request in the years 2006–2010 were checked. The diagnostic code O99.3 is used in Rikshospitalet for all women with fear of childbirth and a request for CS. We found that 81 of the patients had been offered, but rejected to participate in the research. In order to identify those who accepted, we used a register of women who had participated in the known midwife project in the years 2006–2010. The 48 second time mothers with an initial wish for a CS who re-decided and gave birth with a known midwife were identified. From this register, we also determined the mode of delivery in the known midwife group. Data were collected from electronic patient journals for these 129 second time mothers initially wanting to give birth with CS on maternal request.
Data analysis
Unavailable data was noted as missing. The estimated amount of bleeding was coded in two categories: > 1000 ml and ≤ 1000 ml, to make interpretation simpler.
Complications during first birth in the whole study population, compared to the general population (figures from The Medical Birth registry of Norway and the study hospital 2010–2011).
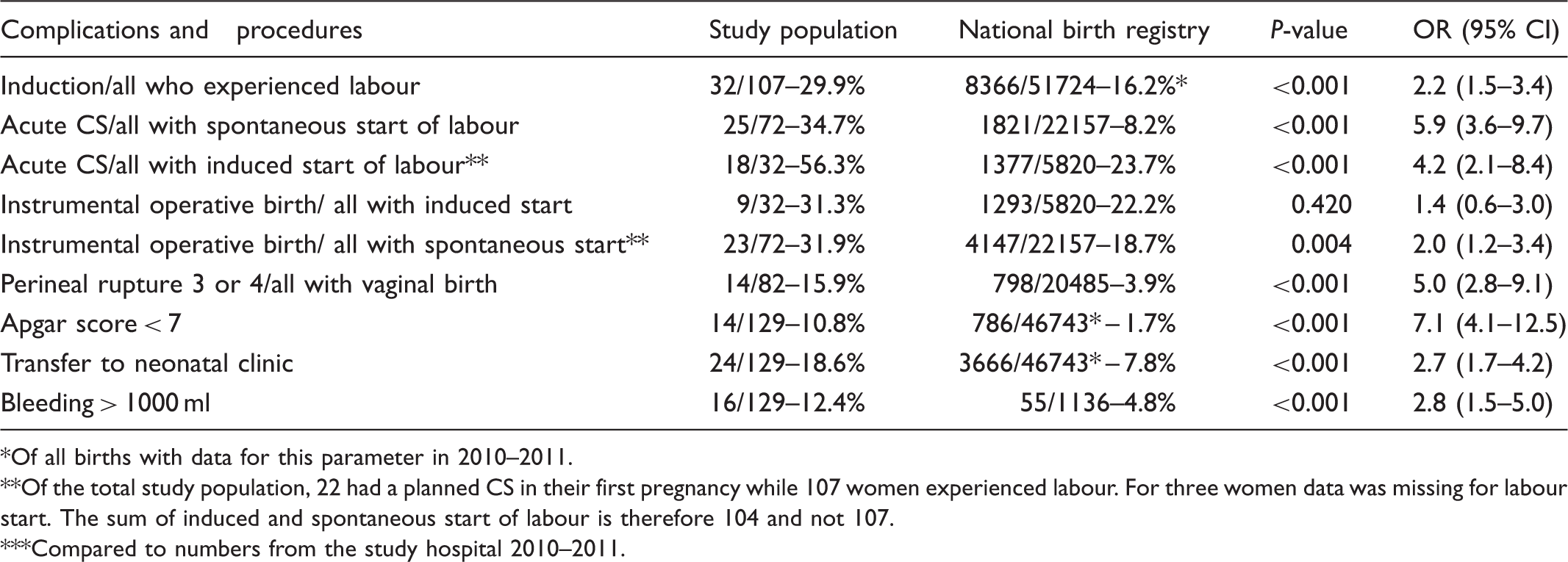
Of all births with data for this parameter in 2010–2011.
Of the total study population, 22 had a planned CS in their first pregnancy while 107 women experienced labour. For three women data was missing for labour start. The sum of induced and spontaneous start of labour is therefore 104 and not 107.
Compared to numbers from the study hospital 2010–2011.
Comparison of maternal and foetal diagnosis for women attending the known midwife program and women opting for planned caesarean section.

Procedures and complications during the first birth, comparing the planned CS group (n = 81) with the known midwife group (n = 48).

Ethical considerations
The register of women giving birth in the known midwife project was approved of by the regional ethics committee in 2006 as part of a practice improvement study. In April 2011 the regional ethics committee also approved the present study as a practice improvement study and concluded that it was not necessary to obtain informed consent from the patients as no identifiable or sensitive information is published.
Findings
There were no significant differences between the planned CS group and the known midwife group with respects to maternal age (34.1 versus 34.3 years) or average number of ultrasounds (3.3 versus 3.6).
The 129 women with a request for CS experienced significantly more complications during their first birth compared to the general population.
Of the 129 women in the total study population, 48 joined the known midwife group. The other 81 maintained their wish for a CS and gave birth by an elective CS, referred to as the planned CS group. Of the 48 women that planned a vaginal birth with a known midwife, 39 gave birth vaginally, nine by CS. Two of the nine women with CS were operated on after an induction of labour that they did not want to continue. These two had a CS performed before labour started, as induction failed and the women were delivered by CS by their own choice before onset of labour. The remaining seven giving birth by CS had an intra-partum CS (Figure 1). All nine women experienced a CS in their first birth.
Second time mothers with a request for CS at the study hospital in 2006–2010.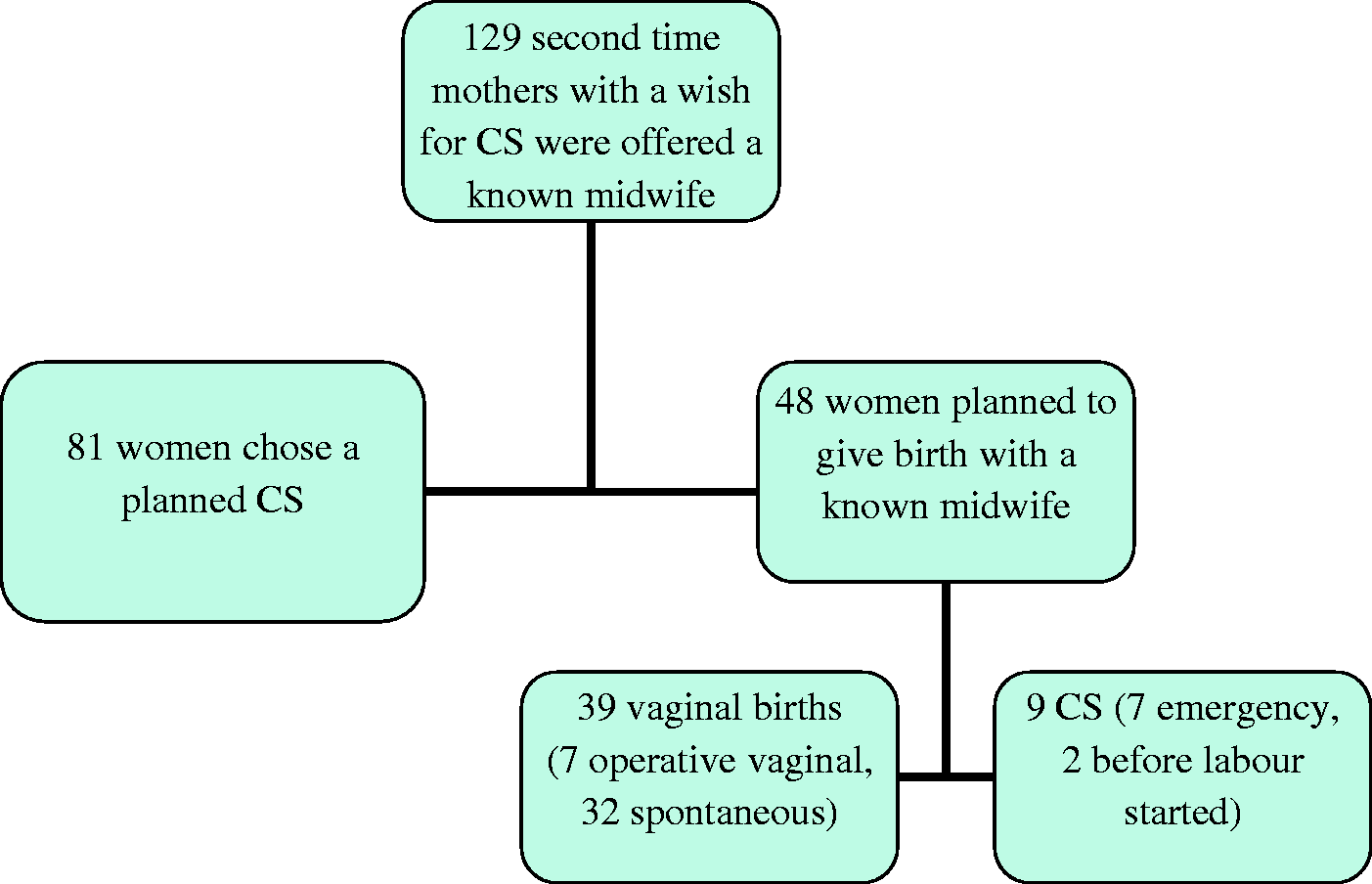
Regarding maternal health, it was three times more likely that a woman in the CS group had a medical diagnosis before she became pregnant. The most frequent diagnoses were: asthma, metabolic diseases, coagulation disorders and pain or discomfort related to the pelvic area. None of these conditions are medical reasons for CS.
Previous fear of childbirth was self-reported and noted in the medical records for the woman’s first pregnancy.
Discussion
Reliability and validity
Our results cannot necessarily be generalized to all second time mothers with a wish for a CS. A randomized controlled study, or a study including all second time mothers with a wish for CS in a certain time period, would have been preferable. However, this was not a possible design for the present study. A confounding factor might be that some women were not referred to the known midwife group because the doctor or midwife they first met believed that vaginal birth was not a possible option for them. If ‘known midwife’ had been an option for all women wanting a CS, the results might have been different. Unfortunately, this was not possible due to lack of resources.
Improving birth care for first time mothers
One of the main findings of our study was that a group of 129 second time mothers with a wish for a CS had experienced significantly more complications during their first birth compared to the general population (Table 1). A woman’s first birthing experience is of vital importance for her future attitude towards mode of birth. 15 The majority in our study had an operative birth as first time mothers. A former CS is associated with fear of childbirth and a wish for CS next time.10,11,15 It is a paradox, as shown by Kringeland et al., that only 29% of the primiparas who wanted as natural a birth as possible, i.e., without painkillers or intervention, achieved this. 16 The overall intervention rate in Norwegian obstetrics has increased from 3% in 1967 to 37% in 2006. 17 The increase in maternal request for CS might be a consequence of the overuse of interventions in obstetric practice. An unnecessary CS in first pregnancy can lead to the woman losing faith in her labouring abilities and wishing for a CS in her second birth. Having experienced one previous CS, there is a 50% chance of a recurrent CS, either a planned or an emergency one. 17 Therefore it is of great importance to avoid operative deliveries without medical indication.
Another area for improvement is induction of labour. As shown in Table 2, those with induced labour had significantly reduced probability of spontaneous birth, both in the study population and in the general population. Numbers from Rikshospitalet showed that in 2011 first time mothers with spontaneous onset of labour had a 6.6 % risk of having an emergency CS, while the women with induced onset of labour had a 25.8% risk for an emergency CS. 18
Failure to progress is a cause of a negative birth experience 19 which might cause fear of childbirth, the most common reason for a CS on maternal request in a later pregnancy.9,12 In our study, 57 of 107 women with a planned vaginal birth in their first pregnancy (the ones with a planned CS excluded) had experienced prolonged labour. Prolonged labour was a more common experience among those who chose a vaginal birth with a known midwife. This finding might indicate that prolonged labour can lead to a wish for a CS in the next pregnancy, but it may be the easier for these women to re-decide and give birth vaginally when given extra support.
Approximately 10% of all primiparas will experience a slow progress during birth. Some of these women might benefit from the so called proactive support of labour, 20 which means that they are given continuous support from a midwife who makes sure that labour progresses normally. Continuous support is shown to be a strong predictor of spontaneous vaginal birth. 21 In cases of prolonged labour, amniotomy will be performed and if necessary augmentation with oxytocin is provided. As shown in a Cochrane review from 2012, amniotomy and oxytocin augmentation performed in cases of slow progress shortened labour and reduced the rate of intra-partum CS. 22
Mode of delivery in the known midwife group
In the known midwife group all the women with one previous vaginal birth gave birth vaginally. It was not unexpected that as many as 30% of the women with a previous CS experienced an acute CS in their next birth. Statistics from Rikshospitalet for the years 2006–2010 showed that the CS rate in this group was 28–33%. 18
Health problems and CS on demand
The women in the planned CS group were four times more likely to have one or more health problems documented in their journals than the ones in the known midwife group. This is in accordance with other studies showing that women with health problems chose CS more often.9,15,23 Health problems might have given them the impression that they were less capable of giving birth, in spite of the fact that their diagnosis did not give medical indication for CS. Nine out of the 25 women with health problems in the planned CS group, had problems related to the pelvic area. The uncertainty as to whether a vaginal birth would increase these problems might have made them reluctant about giving birth, even when the midwife or obstetrician said it was no medical indication for CS. The presence of a diagnosis in the journal of a woman who has given birth by CS may also indicate that she or her doctor wanted to justify her CS. It might also be that the women in the CS group had a different view on health than others. The health belief model describes the health locus of control, which indicates who a person thinks has the main responsibility for his or her health: him/herself, or others, i.e., the health authorities or the physician. 24 It is possible that women who think others have the main responsibility are more likely to wish to be delivered instead of giving birth themselves.
Health promotion is the process of enabling people to increase control over and improve their health. Coping with a demanding situation can be seen as health promoting. A successful vaginal birth might have a redemptive effect on a former traumatic birth experience, 25 thus coping with a vaginal birth might enhance the woman’s health. Programmes such as the ‘known midwife project’ might be health promoting and should be supported and encouraged. They are in accordance with health political guidelines stating that it is health promoting to regard pregnancy and childbirth as natural conditions, and that medical interference should be avoided if possible. 26
Fear of childbirth in first pregnancy
In the planned CS group the participants were six times more likely to have experienced fear of childbirth in their first pregnancy and they were 4.5 times more likely to have had a planned CS in their first birth; 13 of these were CS on maternal request (Table 3). This might partly explain why they did not want a vaginal birth in their second pregnancy either. If childbirth related fear and traumatic labour experiences remain untreated or seem impossible to cure, the risk of a complicated, operative birth is increased and a planned CS might be the right choice.27,28 However, if the woman tries and feels safe during the effort, such an experience might give her a sense of coping even if she ends up with an intra-partum CS. 29
The effect of a known midwife
Several studies show that birth anxiety is often about lack of trust in health personnel, due to former negative experiences. A Swedish study on fear of birth states that ‘both women and men had fears related to not being treated with respect and not receiving sufficient medical care’. 30 A Finnish study finds that in a group of 100 women with fear of childbirth, the most common reason for fear was lack of trust in obstetric staff. 8 An explanation for why some women changed their mind and planned a vaginal birth in the known midwife group might be that knowing the midwife before delivery gave them the necessary confidence in the midwife’s skills and supporting abilities. Our study did not look into psychological aspects that might influence why women chose to join the known midwife project or not. For later research it would be interesting to perform a qualitative study looking into the women’s motivation for wanting a CS and why some re-decided and wanted to give birth with a known midwife. A relatively low percentage (37%) changed their mind and wanted a vaginal birth compared to other projects aimed at helping women with fear of childbirth. These studies show that between 42% and 86% of women with an original wish for a CS change their mind and plan a vaginal birth after interventions.12–14 In a study by Nerum et al., 12 86 % of the women with a wish for a CS changed their mind. Both midwives taking care of the women were also psychiatric nurses. They also cooperated with a psychiatrist. The first consultation lasted for two hours, and the patients were allowed as many subsequent consultations as needed. Some of these women had experienced sexual abuse. The same was the case with some of the women in our study. These women might be in need of more support than the known midwife project could offer. It is important to realize that our study population consisted of women with severe traumatic experiences and some had a CS on demand even in their first birth. These were women for whom talking through the former birth and making a birth-plan for the next was not enough. They were still too afraid to give birth and were therefore offered to participate in the known midwife project. Our findings are in accordance with the results of other studies10,11,15 and contribute to an increased understanding of how unfortunate obstetric events might lead to a maternal request for CS in a subsequent pregnancy. Our study population is small and future studies with larger populations are needed to confirm our findings. It may be a good idea to involve personnel with more psychiatric skills, as in the other programmes mentioned, in order to improve the outcome.
Conclusion
This study documents that unfortunate obstetric events occurring in first time births might lead to subsequent requests for CS and explains why such unfortunate events are important to prevent. Few previous studies describe programmes created to help women to give birth vaginally in spite of a primary wish for CS. The known midwife project has proved to be a useful programme that can help some women with a wish for a CS to change their minds and experience vaginal births.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.
Acknowledgements
We wish to thank all the midwives who volunteered to participate in the known midwife project and thereby made a valuable contribution to this study.