
Abstract
The aim of this study was to examine differences in distribution of neonatal jaundice by migration indicators. In this population-based study at the low-risk maternity ward at Baerum Hospital in Norway, 11,516 mother–child pairs were enrolled and divided into 7 groups by regions/country of origin. First registered live birth babies of mothers who gave birth between 1 January 2006 and 31 December 2010 were included. The study found that a total of 769 infants were treated for neonatal jaundice. Compared to Norwegians, infants born to mothers from East, Southeast and Central Asia had an increased risk and African infants had a decreased risk of neonatal jaundice. Jaundiced infants of African origin were more often transferred to neonatal intensive care units. Ethnicity is an important factor affecting the risk of neonatal jaundice requiring hospitalization in our clinic. To reduce this risk, parents should be adequately informed about the signs of neonatal jaundice requiring medical intervention.
Keywords
Introduction
As many other Western countries, Norway has experienced a large increase in the immigration population over the last decades. This has led to more frequent births to immigrant mothers and has extended the pool of multi-ethnic patients at our maternity clinic. Thus, almost 40% of women giving birth at our clinic are not ethnic Norwegians but represent all the continents. This complex cultural, socioeconomic and ethnic diversity increases the need for attention to specific medical conditions.
Neonatal jaundice, a yellow discoloration of the sclera and skin of new born babies because of accumulation of unconjugated bilirubin, is the most common condition requiring treatment during the neonatal period. 1 In most cases, this hyperbilirubinaemia is a normal physiological phenomenon resulting from elevated bilirubin production caused by the short life span of foetal erythrocytes and their large numbers. In addition, newborns have a limited ability to excrete bilirubin because of the low activity of the liver enzyme that conjugates bilirubin and the low concentration of the binding protein.2,3 However, some newborns develop very high levels of bilirubin in the serum, which can lead to neurotoxicity and death if left untreated. The possible reasons for this pathological jaundice of the newborn include, among others, blood group incompatibility and immunization, infection, liver disease, haematoma, Gilbert’s syndrome and metabolic disorders. It can also be due to the deficiency of the enzyme glucose-6-phosphate-dehydrogenase (G6PD), which is common in certain ethnic groups.2,4,5
The purpose of this study was to determine whether there are differences in the distribution of neonatal jaundice by migration indicators. In addition, we aimed to identify immigrant groups with excessive risk of neonatal jaundice compared to ethnic Norwegians at our low-risk maternity ward in Norway.
Materials and methods
This population-based cohort study included data on the first registered birth for mothers who delivered at Baerum Hospital in Norway from 1 January 2006 to 31 December 2010, excluding stillbirths. In cases with twin birth, only the first-born twin was included. Baerum Hospital is located near Oslo. The maternity ward is a first-level maternity unit with no neonatal intensive care unit (NICU) and is therefore considered a low-risk maternity ward. However, the postnatal unit cares for preterm newborns who have reached at least gestational week 350.
The Medical Birth Registry of Norway (MBRN) was used to identify study participants and obtain the information on pregnancy and childbirth. Statistics Norway, the Norwegian statistics bureau, provided information on maternal and paternal country of birth and descendancy from the Ministry of Foreign Affairs as well as information on maternal education from the Norwegian Tax Administration. A de-identified file was then sent to the research team.
For the purpose of this study, a woman’s (and infant’s) country of origin was determined based on the woman’s own, her mother’s or her father’s country of birth. In cases where the woman’s parents had different countries of birth, we chose the mother’s country of birth. The women were divided into seven groups primarily based on the geographical regions defined by the United Nations Statistics Division: Norway; Eastern Europe; Latin America and the Caribbean; East, Southeast and Central Asia; South and Western Asia; and Africa. Another group comprised the women from Western Europe, including the Nordic countries, as well as North America, Australia and New Zealand.
Measures and statistical analysis
The main outcome measure was the occurrence of neonatal jaundice. Maternity wards in Norway fill out a standardized notification form for all births and pregnancies ending after 12 weeks of gestation and submit it to the MBRN. The notification form includes information on neonatal health, including dedicated check boxes that are marked if the newborn was treated for neonatal jaundice, either by phototherapy or blood replacement therapy. The corresponding variable is registered by the MBRN as ‘treated for neonatal jaundice’. Therefore, all the newborns were treated for elevated serum bilirubin levels with phototherapy or more extensive therapies at a NICU according to the national guidelines for the treatment of neonatal jaundice, which are based on measurements of total serum bilirubin level. 6 Presence or absence of treatment for neonatal jaundice was used as the dichotomous variable.
We examined if there were differences in the distribution of neonatal jaundice by migration indicators (country of origin, time since migration and place of birth), socioeconomic factors (marital status and educational level) and obstetric factors (parity, health during pregnancy, labour dystocia, operative delivery, gestational age, sex of baby, twin birth and birth weight of baby). We also compared mothers whose babies developed neonatal jaundice in two of the immigrant groups (East, Southeast and Central Asia and Africa) to Norwegian mothers, including details of delivery and characteristics of the babies. Crosstab analyses with the Pearson’s chi-square test or Fisher’s exact test were used in order to identify risk factors for neonatal jaundice as well as compare the immigrant groups to Norwegians. Continuous variables were analysed using the Student’s t test or Mann Whitney U test, depending on whether linearity was present. We then created an explorative multiple logistic regression model of neonatal jaundice in order to identify factors that could predict its occurrence. A backward stepwise approach was utilized with the following variables included in the model at the first step: immigrant group (Norway; East, Southeast and Central Asia; Africa), time since migration (in years), maternal age (in years), marital status (married/cohabitant or single), educational level (≥12 years, <12 years, or undocumented), parity (0 or ≥1), consanguinity (blood relationship between spouses), maternal health before pregnancy (any registered health issues), maternal health during pregnancy (any registered health issues), cigarette smoking at the end of pregnancy, meconium-stained liquor, twin birth, labour dystocia (oxytocin infusion during labour), vaginal instrumental delivery (vacuum or forceps), elective caesarean section, sex of baby and birth weight (normal, 2.5–4.5 kg; low, <2.5 kg; macrosomia, >4.5 kg). The variables that did not significantly contribute to the model were then removed one at a time until all remaining variables contributed significantly with p values <0.05. The model fit was tested using the Hosmer and Lemeshow goodness-of-fit test. Since the variables gestational age and birth weight were closely correlated and we do not have many preterm newborns at our maternity ward, birth weight was used in the analysis. No interactions were detected between the variables included in the regression model.
Ethical considerations
Permission was obtained from the Regional Committees for Medical and Health Research Ethics (REC South East; Ref no 2012/267). The ethical committee is regulated by the Act on Medical and Health Research and Regulations for Processing of Personal Data.
Results
Distribution of neonatal jaundice by migration indicators and socioeconomic and obstetric factors. N = 11,516.
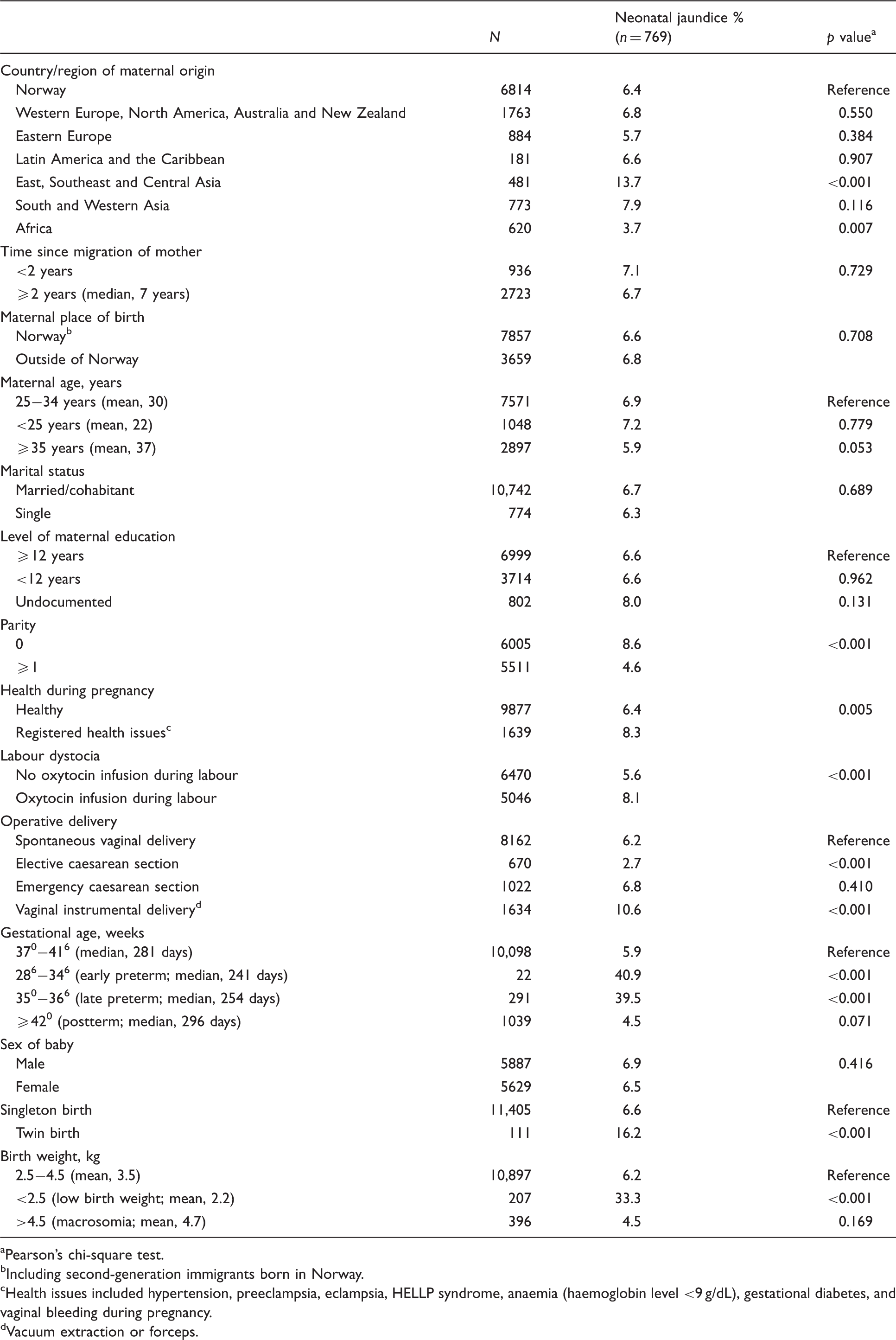
Pearson’s chi-square test.
Including second-generation immigrants born in Norway.
Health issues included hypertension, preeclampsia, eclampsia, HELLP syndrome, anaemia (haemoglobin level <9 g/dL), gestational diabetes, and vaginal bleeding during pregnancy.
Vacuum extraction or forceps.
Comparison of characteristics of 526 mother-infant pairs whose infants were treated for neonatal jaundice by country/region of origin.
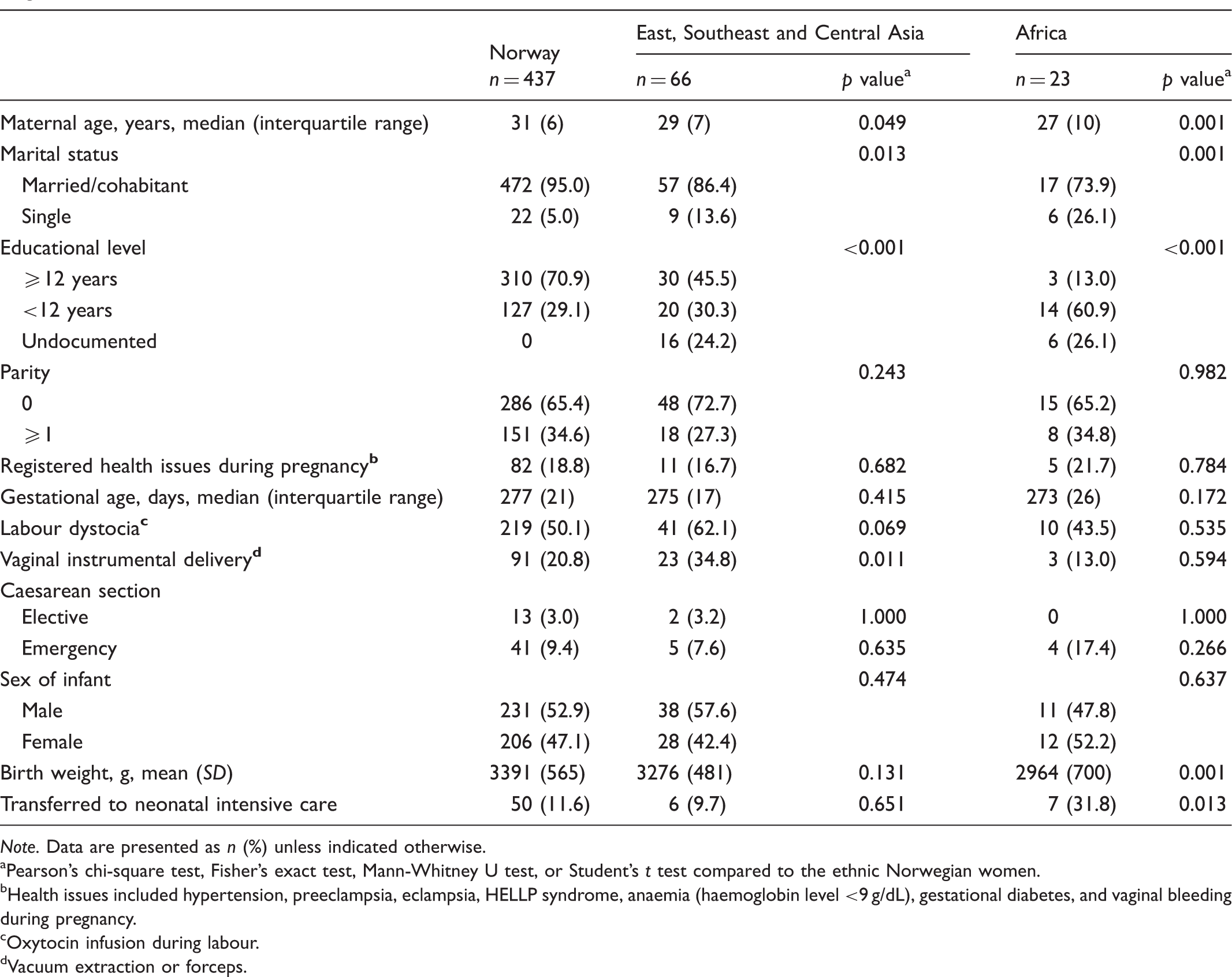
Note. Data are presented as n (%) unless indicated otherwise.
Pearson’s chi-square test, Fisher’s exact test, Mann-Whitney U test, or Student’s t test compared to the ethnic Norwegian women.
Health issues included hypertension, preeclampsia, eclampsia, HELLP syndrome, anaemia (haemoglobin level <9 g/dL), gestational diabetes, and vaginal bleeding during pregnancy.
Oxytocin infusion during labour.
Vacuum extraction or forceps.
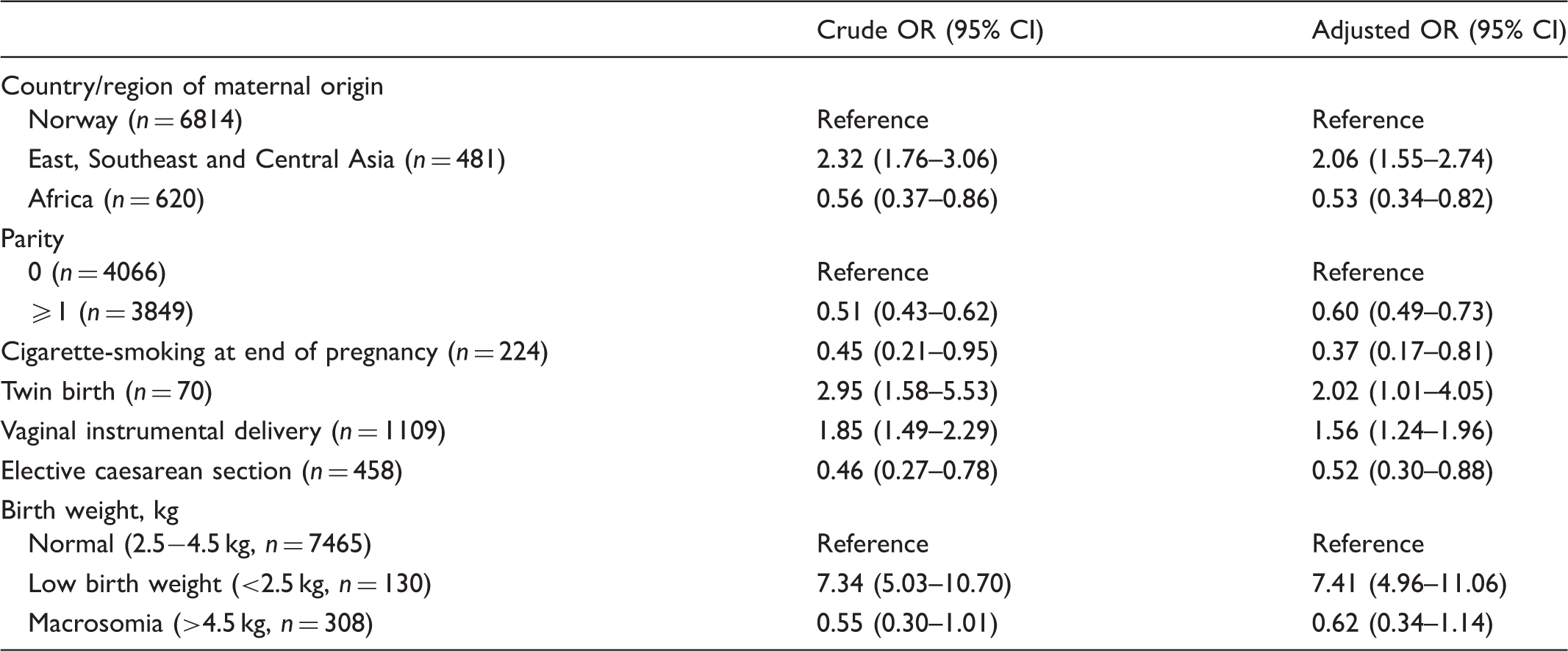
The logistic regression model of neonatal jaundice based on 526 cases out of 7915 births included in the analyses.
Discussion
The following maternal and infant factors identified in the present study as increasing the odds of neonatal jaundice have been described earlier: first-time mothers,7,8 vaginal instrumental delivery9,10 and low birth weight.10,11 The association between maternal smoking during pregnancy and reduced odds of neonatal jaundice in infants has also been reported earlier. 10 However, Sarici and colleagues did not find the same association in Turkey. 12
African mothers had a lower proportion of infants with neonatal jaundice compared to Norwegian women, which is also in line with previous studies.7,10 Among the infants treated for neonatal jaundice in our study, however, those born to African mothers were transferred to a NICU more frequently. We speculate that the detection of jaundice in the African infants was delayed, which led to its higher severity and, consequently, treatment at a NICU rather than at the normal newborn nursery. It might also be that jaundice in these infants was a manifestation of other, more serious conditions that required intensive care. Unfortunately, data on other diagnoses were not collected in our study. It is also possible that the information provided to the African mothers on detecting the signs of jaundice after discharge from the hospital was incomplete, resulting in delayed treatment. In this regard, such written information is not available in English or in any of the African languages at our normal newborn nursery, whereas Norwegian women receive a folder developed at our hospital, which includes information on the indicators of neonatal jaundice and instructions on when to contact the hospital.
Our finding that the infants born to mothers from East, Southeast and Central Asia had an increased risk of neonatal jaundice compared to the Norwegian infants agrees with the results of previous studies.10,13–16 As early as in 1965, Brown and Wong reported that Asian infants had elevated serum bilirubin levels when compared to British infants born in a British military hospital and a government maternity hospital in Singapore. 17 Chinese infants had the highest values of serum bilirubin, which exceeded those in British infants 2.5-fold. Moreover, it was also found that the highest peak in bilirubin level was delayed in the Asian infants compared to British infants, and these high levels of bilirubin lasted longer. Several studies have identified genetic mutations, deficiencies and differences that may explain these differences.5,18–22 The most examined genetic defect that leads to neonatal jaundice is an X-linked hereditary mutation in the G6PD gene. G6PD deficiency is much more common and severe in men than in women.22–24 The highest frequencies of this deficiency have been detected in Africa, Asia, the Mediterranean region and in the Middle East. Hence, the difference in proportions of Asian and African infants treated for jaundice in our study may not be explained by G6PD deficiency alone. Infants with G6PD deficiency have a delayed peak in serum bilirubin level compared to infants whose jaundice is due to immunization and blood group incompatibility. Furthermore, neonatal jaundice is more typical and more severe in preterm infants with G6PD deficiency than in term infants. 23 A genetic defect in uridine-diphosphoglucuronosyl transferase 1A1 leads to the accumulation of unconjugated bilirubin, 20 and therefore infants with G6PD deficiency coexisting with a mutation in uridine-diphosphoglucuronosyl transferase 1A1 have an increased risk of neonatal jaundice.18,23,24
In addition to genetic deficiencies, the effect of breastfeeding on hyperbilirubinaemia has been examined. Breastfed infants more often have neonatal jaundice extending into second and third weeks of life compared to formula-fed infants, which is known as breast milk jaundice. 25 Inadequate breastfeeding in the first week of life may also increase the risk of hyperbilirubinemia. 26
We found no effect of infant’s sex on the distribution of neonatal jaundice. This is in contradiction to the findings of several previous studies, which suggested that boys have an increased risk of jaundice compared to girls.8,10
The mothers with labour dystocia had an increased proportion of infants with neonatal jaundice in our study, which is in line with previous findings. 11 In this regard, we used 5% glucose when administering oxytocin, and a Nigerian study reported that the use of 5% glucose instead of isotonic saline solution for oxytocin infusion during labour was associated with higher neonatal bilirubin levels in the infants. 27
In the present study, the numbers of infants with neonatal jaundice in the immigrant groups were relatively small, which may have resulted in detecting only large differences using statistical methods. It is therefore possible that other differences between immigrant and Norwegian infants with neonatal jaundice will be detected after increasing the number of participants. Our findings should therefore be interpreted with caution and should not be generalized to the whole Norwegian population. However, our data on country of birth and descendancy were accurate, and the study was conducted at a single low-risk hospital in Norway, which has a high proportion of immigrants in the public health systems. The study population was well suited for examining obstetric differences by country of origin because many confounding factors were eliminated as a consequence of the good general health of the mothers and foetuses (i.e., a healthy baby was expected). A study conducted at our hospital between March 2008 and June 2009 sought to examine how the new Norwegian national guidelines affected the need for phototherapy among healthy newborns. 28 Although the authors found that 3.1% of babies needed phototherapy, their study only included Norwegian infants with >36 weeks of gestation and whose parents provided informed consent.
Despite the presence of developmental differences between immigrant and Norwegian infants, the role of ethnic disparity in occurrence of neonatal jaundice has not been, to our experience, a matter of sufficient focus among personnel in Norwegian maternity wards and normal newborn nurseries. Transcutaneous bilirubin measurements are utilized in infants with darker skin when screening for hyperbilirubinaemia. Thus, most of our colleagues at normal newborn nurseries believe that this screening is only needed to evaluate newborns with darker skin, as the natural pigmentation makes the colour contribution from bilirubin more difficult to detect by eye. They are unaware that the screening is also instrumental for the earlier detection of jaundice among Asian infants, who are at a higher risk for neonatal jaundice. Jaundice has been reported as a common cause of readmission to hospital after early discharge of newborn infants. 29 The modern standards of postnatal care in Norway result in most mothers and their infants being discharged from the hospital within 48 hours after delivery. Given this short time spent under medical observation and a delayed peak in bilirubin levels in some infants, efforts should be made in order to inform parents about the signs of neonatal jaundice and instruct them when to contact the hospital. This information should be provided to immigrant mothers in their native language and in a manner that facilitates easy understanding.
Conclusion
Our study revealed that infants born to mothers from East, Southeast and Central Asia had increased odds of neonatal jaundice when compared to Norwegians. We also found that although the proportion of the African infants with neonatal jaundice was lower than that of the Norwegian infants, they were more often transferred to a NICU for its treatment. It is essential to educate parents in their native language about signs of neonatal jaundice and provide clear instructions on when to contact the hospital.
Footnotes
Abbreviations
G6PD – Glucose-6-phosphate-dehydrogenase MBRN – The Medical Birth Registry of Norway NICU – Neonatal intensive care unit OR – Odds ratio CI – Confidence interval
Acknowledgements
The authors wish to thank Lien My Diep at Oslo University Hospital for the assistance with statistical analysis. We also wish to acknowledge the services of the Medical Birth Registry of Norway and Statistics Norway.
Disclaimer
This study has used data from the Medical Birth Registry of Norway. The interpretation and reporting of these data is the sole responsibility of the authors, and no endorsement by the Medical Birth Registry of Norway is intended nor should be inferred.
Funding
Funding for this study was provided by the Vestre Viken Hospital Trusts research fund.
Conflict of interests
The authors declare that there is no conflict of interest.