
Abstract
The release of radioactivity into the atmosphere from the Fukushima Daiichi accident has been estimated by Japan’s government as about one-tenth of that from the Chernobyl accident. The area in Japan contaminated with cesium-137—at the same levels that caused evacuation around Chernobyl—is also about one-tenth as large. The estimated number of resulting cancer deaths in the Fukushima area from contamination due to more than 1 curie per square kilometer is likely to scale correspondingly—on the order of 1,000. On March 16, 2011, the Nuclear Regulatory Commission advised Americans in the region to evacuate out to 50 miles (NRC 2011a). If the Japanese government had made the same recommendation to its citizens, it would have resulted in the early evacuation of about two million people instead of 130,000. Because contaminated milk was interdicted in Japan, the number of (mostly non-fatal) thyroid cancer cases will probably be less than 1 percent of similar cases in Chernobyl. Unless properly dealt with, however, fear of ionizing radiation could have long-term psychological effects on a large portion of the population in the contaminated areas.
Keywords
The Japanese government’s estimates of the releases into the atmosphere from the 2011 Fukushima Daiichi Nuclear Power Station accident compared with the estimates from the 1986 Chernobyl accident, in millions of curies 1
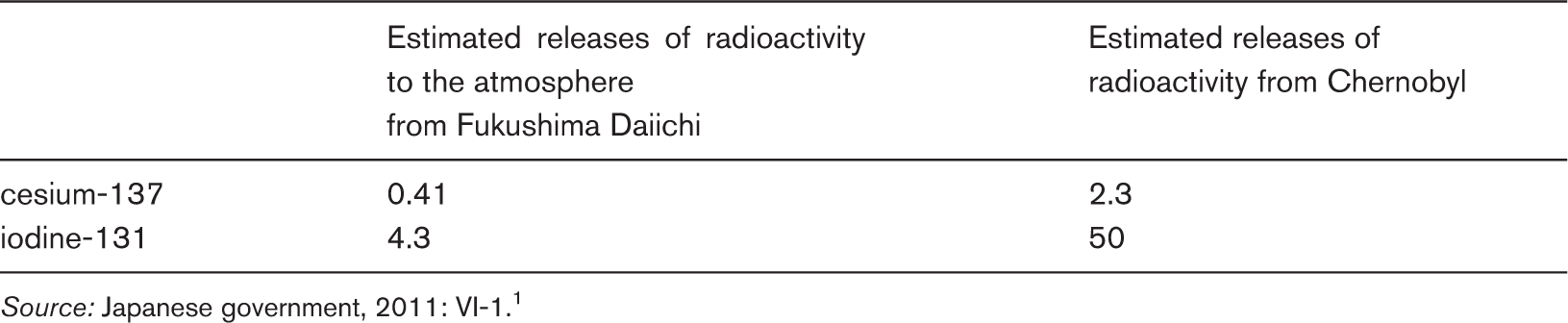
Source: Japanese government, 2011: VI-1. 1
It is not clear what the long-term health consequences of the Fukushima Daiichi accident will be. About 16,000 Chernobyl-caused cancer deaths are projected during the lifetime of those who were exposed in Belarus, Ukraine, and western Russia and in Europe farther downwind. About half of these deaths are projected among the six million people living in areas contaminated with levels of radioactive cesium-137 above 1 curie per square kilometer—and half among the remaining population of about 570 million in Europe, who live in less contaminated areas (Cardis et al., 2006). The average estimated increase in cancer deaths in the two populations are about 0.1 and 0.001 percent, respectively. For comparison, the overall cancer death rate in the developed world is about 27 percent (American Cancer Society, 2008). It is not surprising that detecting and distinguishing the Chernobyl-related cancers statistically is challenging.
A corresponding estimate of the cancer consequences of the Fukushima Daiichi accident has not yet been conducted, but it is possible to make a very preliminary order-of-magnitude guesstimate. Out of the two million people who live within a 50-mile (80-kilometer) radius of the Fukushima plant, about one million live in areas contaminated with cesium-137 to levels greater than 1 curie per square kilometer. 2 Scaling to the six million people in areas contaminated to similar levels by the Chernobyl accident, one might expect around 1,000 extra cancer deaths related to the Fukushima Daiichi accident, that is, a 0.1 percent incidence rate. This is much less than the direct toll—about 20,000—from the earthquake and tsunami that caused the accident (McCurry, 2011).
More accurate estimates will be possible if national collective-dose estimates are pulled together, as they were after the Chernobyl accident. For now, in order to frame the discussion, it is useful to consider the problems of long-term land contamination, evacuation decisions, and thyroid cancers. Finally, it is important to note that, if not dealt with properly, the psychological consequences associated with accidents such as Chernobyl and Fukushima could damage many more lives than the cancer consequences.
Land contamination
As the world tuned in to watch the unfolding of the catastrophic reactor failures at the Fukushima Daiichi plant, perhaps the most dramatic events were the four hydrogen explosions signaling that a loss of coolant had occurred. Following this loss, radioactive heating drove the fuel temperature up past 1,000 degrees Celsius (about 1,800 degrees Fahrenheit), and the zirconium alloy cladding (the outer covering of the fuel rods) began to react with the hot steam in the reactor pressure vessel (Alvarez et al., 2003). The zirconium removed oxygen from the water molecules and created the hydrogen gas that then leaked into the outer reactor buildings, mixed with air, and exploded—destroying the superstructures of the buildings.
More important, however, the hydrogen explosions were indicators that the fuel cladding had failed and released cesium-137 and iodine-131, fission products that have relatively low boiling points. 3 Cesium-137 has a 30-year half-life—the amount of time it takes for half the atoms to disintegrate. Today, it and its shorter-lived cousin, cesium-134 (with a two-year half-life), are the major radioactive contaminants of the land in Fukushima and the surrounding prefectures. As the contaminants decay they emit gamma rays that raise the radiation levels, and the magnitude of the resulting danger will determine the decontamination efforts or long-term evacuation plans. 4
Around the Chernobyl plant, cesium-137 contaminated over 1,000 square miles (about 3,000 square kilometers) to a level greater than 40 curies per square kilometer. In this area, the population was encouraged to leave permanently. Residents were allowed to stay in an additional 7,000 square kilometers contaminated to levels between 15 and 40 curies per square kilometer. 5 By “strict control”—that is, partial decontamination of the soil and building and road surfaces, along with ensuring that people did not eat heavily contaminated produce—radiation doses were limited to less than 0.5 rems per year. 6
Figure 1 shows a map of the cesium-137 contamination levels around Fukushima (US Department of Energy, 2011). The circles and arcs show different distances (20, 30, 60, and 80 kilometers) from the Fukushima Daiichi Nuclear Power Station. It appears that the wind was blowing in a northwesterly direction when the largest on-shore releases occurred. These releases apparently occurred on March 15.
7
Contamination levels of cesium–137 based on gamma-ray measurements from 42 fixed–wing and helicopter survey flights at altitudes ranging from 150 to 700 meters.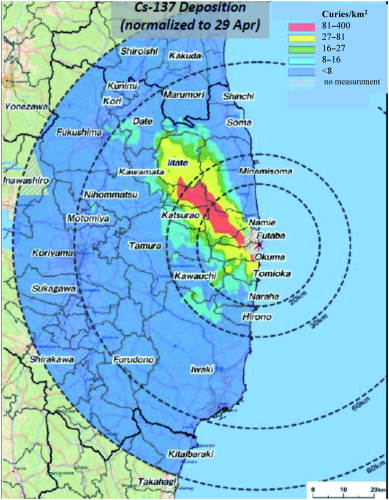
The contamination measurements were obtained between April 6 and April 29, 2011 in a cooperative program between the Japanese and US governments. Fukushima, Koriyama, and Iwaki each have some 300,000 residents and together account for about half of the total population living within 50 miles (80 kilometers) of the Fukushima Daiichi Nuclear Power Station.
The areas shown in red and adjoining parts of the yellow area (very roughly 175 square kilometers) are contaminated to the levels of regions that are still evacuated around Chernobyl. The green area and adjoining parts of the yellow area (very roughly 600 square kilometers) are contaminated to levels comparable to those in areas where the population stayed after the Chernobyl accident, but with strict control of their exposure to radiation. Thus, the heavily contaminated areas in Fukushima Prefecture are on the order of one-tenth as large as the corresponding contaminated areas around Chernobyl.
In Japan’s report to the IAEA, it is estimated that, cumulatively from March to May 2011, the highest external doses outside the 20-kilometer evacuation area were 2 to 4 rem. Extrapolated to a year, it was estimated that the highest doses will rise to 5 to 10 rem (Japanese government, 2011: Attachment V-13). Assuming that the risk is proportional to dose (the linear no-threshold hypothesis), a 10-rem whole-body dose would bring with it a risk of cancer death later in life of about half of one percent. 8
On April 10, Japan’s government advised evacuation of the population in areas where expected first-year doses were greater than 2 rem (Japanese government, 2011: Attachment V-3, Table 1). On April 19, the government released the “Provisional Guideline for the Utilization of School Buildings, Grounds, and Related Facilities in Fukushima Prefecture,” which allowed annual doses of up to 2 rem for students. This produced widespread outrage (see, for example, Japan Federation of Bar Associations, 2011). Radiation doses to 10-year-old children are estimated to bring with them about twice as great a risk as to the age-averaged population (National Research Council of the National Academies, 2006: Figure 12-1A). In one contaminated schoolyard in Fukushima, concerned parents and teachers reduced dose rates tenfold by removing the topsoil (Tabuchi, 2011).
The debate over evacuation
Within a day of the accident at Fukushima Daiichi, nearly 130,000 people living within 20 kilometers of the power plant were ordered to evacuate. And on March 15, four days after the accident, an additional 354,000 people living between 20 and 30 kilometers of the plant were advised to stay indoors to reduce exposure to radiation (Japanese government, 2011: Attachment V-3, Table 1).
Population living within 50 miles (80 kilometers) of the Fukushima Daiichi Nuclear Power Station
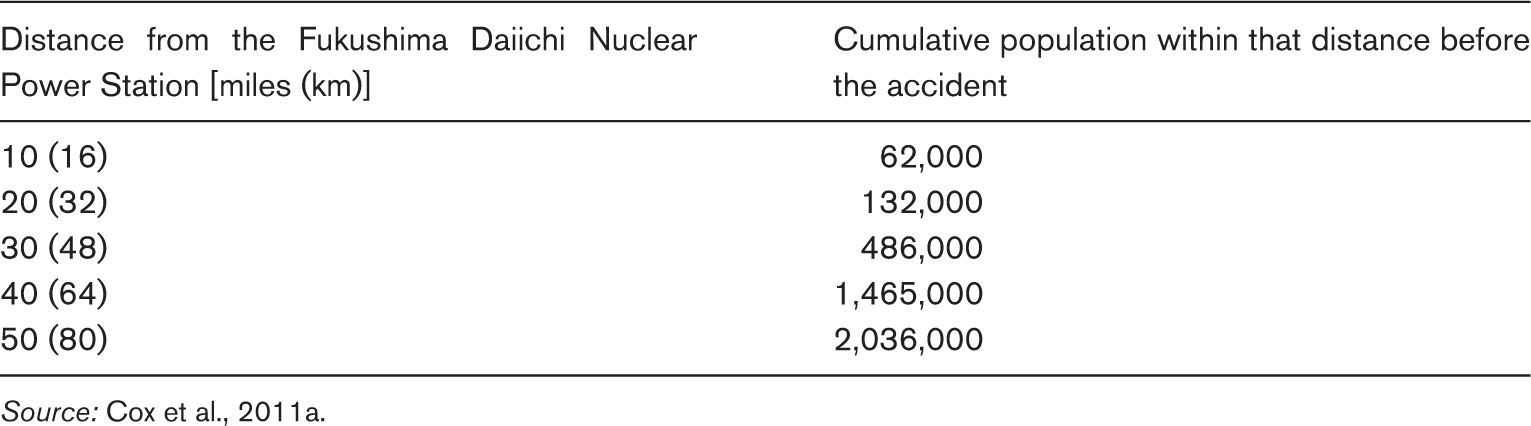
Source: Cox et al., 2011a.
On April 7, during an NRC staff briefing to the Nuclear Regulatory Commission’s Advisory Committee on Reactor Safeguards, a committee member challenged the NRC staff on this evacuation recommendation: [L]et me reverse this. Thirty-two years ago, if Japan would have done a what-if calculation about Three Mile Island, and said all the Japanese within 50 miles of Harrisburg should get out, what would be our response to that, from a policy standpoint? (NRC, 2011b: 91–92)
He could also have noted that 17 million people—including most of the population of New York City—live within 50 miles of the Indian Point Nuclear Power Station on the Hudson River (Donn, 2011). 11
Thyroid cancers
The most visible and undeniable health consequence from Chernobyl has been an epidemic of thyroid cancer from high doses of radioactive iodine. Among the children and adolescents in Belarus who were exposed to the radioactivity from the Chernobyl accident in 1986, almost 7,000 cases of thyroid cancer had been diagnosed as of 2005. The majority of these cases were attributed to iodine-131 (UNSCEAR, 2008: 14–15). 12 Fortunately, most of these cancers are likely to be non-fatal. 13
Iodine-131 has a half-life of eight days and concentrates in the thyroid if inhaled or ingested in contaminated food or water. For children under 18 years of age, there is approximately a 0.3 percent risk of incurring thyroid cancer from a 10-rem thyroid dose. 14
Among other cancers caused by Chernobyl, the unique visibility of the thyroid cancers stems from the relative sensitivity of the thyroid to cancer induction by ionizing radiation 15 and the fact that thyroid doses to children in areas contaminated by the Chernobyl accident were about 100 times higher than whole-body doses. 16
The very high thyroid doses from the Chernobyl disaster were due in large part to the failure of authorities to block the consumption of milk produced by cows grazing on contaminated grass. 17 By contrast, in Japan, shipments of raw milk and vegetables from Fukushima and three neighboring prefectures were blocked on March 21, six days after the large release that caused the high contamination. Screening of produce for radioactivity began the next day (Japanese government, 2011: Table 1). Between March 21 and 23, some 1,080 children evacuated from the 20-kilometer zone around the Fukushima Daiichi Nuclear Power Station were screened for iodine-131 exposure. Authorities concluded that none had received a thyroid dose greater than 5 rem. 18 It is not clear whether additional tests were done between the initial screenings in March and more than three months later—when the local government announced its plans to check the radioisotope levels in the bodies of selected residents, including checking their thyroids for iodine-131 (Yomiuri Shimbun, 2011). Given that the iodine-131 had decayed for 14 half-lives by then, it would have been barely detectable, if at all. 19
It is not clear how widely and how early the authorities in Japan attempted to prevent thyroid uptake of iodine-131 by providing the population with potassium-iodide tablets. 20 If taken in appropriate doses before exposure to radioactive iodine, the tablets saturate the thyroid with non-radioactive iodine, thereby blocking the absorption of iodine-131. Very little potassium iodide was distributed in the Soviet Union after the Chernobyl accident. In Poland, however, more than 10 million children, 16 years of age and under, and approximately seven million adults received at least one dose of potassium iodide, reducing their thyroid doses to “negligible levels” (UNSCEAR, 2008: 7). According to the US Food and Drug Administration (FDA), “The side effects among adults and children were generally mild and not clinically significant” (FDA, 2001: 4–5.).
Psychological consequences
It is well known that there is a special dread associated with exposure to ionizing radiation (Weart, 1988; Slovic, 1996: 165). This may be due to the invisibility of the damage and the long latency of cancer and genetic defects.
A report by the Chernobyl Forum, a two-year effort by representatives from the IAEA, other UN organizations, and the governments of Belarus, Russia, and Ukraine, states that: Any traumatic accident or event can cause the incidence of stress symptoms, depression, anxiety (including post-traumatic stress symptoms), and medically unexplained physical symptoms. Such effects have also been reported in Chernobyl-exposed populations. Three studies found that exposed populations had anxiety levels that were twice as high as controls, and they were 3–4 times more likely to report multiple unexplained physical symptoms and subjective poor health than were unaffected control groups. … [I]ndividuals in the affected population were officially categorized as ‘sufferers,’ and came to be known colloquially as ‘Chernobyl victims,’ a term that was soon adopted by the mass media. This label, along with the extensive government benefits earmarked for evacuees and residents of the contaminated territories, had the effect of encouraging individuals to think of themselves fatalistically as invalids. It is known that people’s perceptions—even if false—can affect the way they feel and act. Thus, rather than perceiving themselves as ‘survivors,’ many of those people have come to think of themselves as helpless, weak, and lacking control over their future. (Chernobyl Forum, 2006: 20–21)
Japan, given its similar experience with the survivors of Hiroshima and Nagasaki, should be especially sensitive to this issue. Putting the added cancer risks into perspective by showing how small an addition they represent to the risk of cancer from other causes may help to some degree, but psychological counseling and group therapy may be required as well.
Footnotes
Acknowledgements
This article is part of a special issue on the disaster that occurred at the Fukushima Daiichi Nuclear Power Station in March 2011. Additional editorial and translation services for this issue were made possible by a grant from Rockefeller Financial Services.
1
One curie equals 37×109 becquerels (disintegrations per second).
3
Cesium has a boiling point of 671 degrees Celsius, iodine 184 degrees Celsius, and cesium-iodide 1,277 degrees Celsius.
4
In areas distant from the Chernobyl accident, where volatile fission products such as those released by the Fukushima accident dominated, the cesium isotopes accounted for 70 percent of the external dose two months after the accident and 85 percent four months after the accident (UNSCEAR, 2000: Figure XIII).
5
Initially, Belarus, Russia, and Ukraine all planned to evacuate zones contaminated to levels above 15 curies per square kilometer and give residents in areas with contamination levels between 5 and 15 curies per square kilometer the right to evacuate (UNDP and UNICEF, 2002: Table 3.1).
6
UNSCEAR, 2000: Tables 8 and 26; p. 475. One rem = 0.01 sieverts.
7
The wind direction shifted to the northwest at about noon on March 15 and continued to blow in that direction until midnight. The wind speed was low (about 4 kilometers per hour). The dose rate in Fukushima, 40 kilometers to the northwest, increased at about 6 p.m. See the detailed chart of this data at: http://dl.dropbox.com/u/16653989/NuclPlants/index.html. The releases occurred after an explosion-like sound was heard from Unit 2 at 6:20 a.m. on March 15, and a pressure decrease inside the containment suggested that the containment had failed (Tokyo Electric Power Company [TEPCO], 2011).
8
The sex-averaged and age-averaged estimated extra risk of cancer death from a radiation dose of 0.1 sievert (10 rem) is 0.26–1.2 percent (![]() : Table ES-1). This risk estimate is scaled to lower doses assuming the linear, no-threshold (LNT) hypothesis, that is, that the cancer risk from ionizing radiation is proportional to dose. Some—especially in the nuclear industry—refuse to believe this hypothesis and some of those even subscribe to the “hormesis” hypothesis that a little radiation can be healthy because it stimulates the DNA-repair mechanisms of the body. Others argue that ionizing radiation at low doses may be more damaging than the LNT hypothesis suggests. However, the National Research Council of the National Academies’ reports on the Biological Effects of Ionizing Radiation (BEIR), which have most thoroughly reviewed the issue, continue to favor the LNT hypothesis.
: Table ES-1). This risk estimate is scaled to lower doses assuming the linear, no-threshold (LNT) hypothesis, that is, that the cancer risk from ionizing radiation is proportional to dose. Some—especially in the nuclear industry—refuse to believe this hypothesis and some of those even subscribe to the “hormesis” hypothesis that a little radiation can be healthy because it stimulates the DNA-repair mechanisms of the body. Others argue that ionizing radiation at low doses may be more damaging than the LNT hypothesis suggests. However, the National Research Council of the National Academies’ reports on the Biological Effects of Ionizing Radiation (BEIR), which have most thoroughly reviewed the issue, continue to favor the LNT hypothesis.
9
Reportedly, on March 14, after the second hydrogen explosion at the plant, the president of Tepco asked Japan’s prime minister for permission to withdraw all employees from the site because it was too dangerous for them to remain (Onishi and Fackler, 2011).
10
About 300 Americans were registered with the US State Department as living in Fukushima Prefecture, which is 14,000 square kilometers in area (personal communication). About 10,000 square kilometers lie within a radius of 50 miles around the Fukushima Daiichi Nuclear Power Station.
11
Many other major US cities are within 50 miles of nuclear power plants (The New York Times, 2011b: D1).
12
The estimated average thyroid dose to 47,000 children aged seven and under in two towns in eastern Belarus was about 70 rems. For the country as a whole (one million children aged seven and under), it was 13 rems (UNSCEAR, 2000: 477; Tables 39 and 40), assuming the 2.3 ratio of child to average thyroid dose observed in the two towns and a 10 percent ratio of children aged seven and under to the total population.
13
The mortality from thyroid cancer in the United States is about 13 percent, versus about 50 percent for other solid cancers plus leukemia, not including non-melanoma skin cancers (National Research Council of the National Academies, 2006: Table 12-4).
14
The sex-averaged and age-averaged estimated extra risk of cancer from a thyroid radiation dose of 10 rem is 0.1 percent (National Research Council of the National Academies, 2006: Table 12-5 A), increased by a factor of three for children because of the greater sensitivity to exposure at a young age (National Research Council of the National Academies, 2006: Table 12-2).
15
It is estimated that about 5 percent of the cancers expected from a uniform whole-body dose of radiation would be thyroid cancers, while thyroid cancers constitute only about 1 percent of all solid cancers in the United States (National Research Council of the National Academies, 2006: Tables 12D-3 and 12-4).
16
The average whole-body dose to two million people living in contaminated areas of Belarus during the first decade after the Chernobyl accident was 0.8 rem (UNSCEAR, 2000: Table 53). The average thyroid dose to children less than seven years of age in the same areas was about 70 rem (UNSCEAR, 2000: Table 39).
17
“The high thyroid doses among the general population were due almost entirely to drinking fresh milk containing iodine-131 in the first few weeks following the accident” (UNSCEAR, 2008). The ratio of the releases of iodine-131 and cesium-137 was 8 in NRC calculations of the hypothetical doses from a meltdown accident in Fukushima Unit 2 versus about 20 for Chernobyl (Jaczko, 2011) and about 10 for Fukushima Daiichi (see Table 1). The resulting ratios of NRC-calculated adult thyroid dose to the whole-body inhalation dose and the first-year doses were 10 and 0.34, respectively (NRC, 2011a).
18
The screening level was 0.02 rem per hour. Taking into account the eight-day half-life of iodine-131 would multiply that dose by 269 (IAEA, 2011: 127).
19
A one-rem dose to the thyroid of an adult would require the ingestion of about 0.6×10−6 curies of iodine-131 (Hamby and Benke, 1999: 245). The dose to a five-year-old child’s thyroid would be several times larger (NRC, 1975: Table VI-D-6). The minimum detectable level of iodine-131 in the thyroid is about 35×10−12 (Plato et al., 1976: 539). It would take 14 half-lives (about 110 days) for 0.6×10−6 curies to decay to 35×10−12 curies.
18
The IAEA report on the accident states, “On 16 March the local headquarters instructed the local government to administer iodine tablets whenever evacuation is performed. However, by this time the great majority of the evacuation has been completed” (IAEA, 2011: 127).