
Abstract
Originating in south-western China, the Third Plague Pandemic reached the Pearl River Delta in the early 1890s, whereupon steamships took the disease to port cities worldwide. We examine the impact of responses to plague on the built environment in Hong Kong, a British colony, as well as the comparable experiences of Honolulu and San Francisco. Bubonic plague is not the result of polluted water, but officials drawing on contemporary understandings of miasmic theory believed it to be so. Fearing the epidemic would spread beyond crowded Chinese districts, governments quarantined affected areas, carrying out house-to-house inspections and in America, controlled burnings of condemned buildings. To improve sanitation, the Hong Kong government commissioned reports that recommended a sewerage system, lower density housing, and rat control, but large-scale urban redevelopment was not undertaken due to high costs, and water infrastructure would prove to be ineffective in the face of twentieth-century population growth.
When Bob Hope first visited Hong Kong, probably sometime in the 1960s or early 1970s, a local reporter asked him about his impressions of the city. “It seems fine,” the entertainer replied, “but what was that awful smell as we landed?” “That’s shit in the Kai Tak nullah,” said the reporter, pointing to the narrow channel that drains to Victoria Harbour. “Yes, I know—but what have they done to it?” 1
Hong Kong translates to “Fragrant Harbour,” the name given to it by Tanka boatpeople from the port of Shek Pai Wan, a hub that transported wood and premium incense from the Aquilaria sinensis tree that was burned in temples, homes, and at festivals. Soon after colonization by the British in the nineteenth century, however, Hong Kong developed a reputation for unpleasant aromas, as high population density and poor sanitation contributed to episodes of epidemics. During the Bubonic Plague Epidemic of 1894, the smell of Hong Kong was perceived to be symptomatic of serious sanitation problems.
Like anthropogenic climate change, water management problems defy simple solutions because they do not sit within the responsibility of one organization, require policy responses that transcended hierarchical models of governance, and call for ownership and action at a societal level. These were socially complex “wicked problems,” with multiple, contested causes and interdependencies, and deep disagreement about their nature and significance. 2 In Hong Kong, as in other cities, water’s physical qualities—fluidity, opacity, and trackless nature—enhanced the attraction of bodies of fresh and salt water as sites for waste disposal. 3 Managing this use of water, and addressing the problems it created, concerned multiple stakeholders with competing expectations and resources across political and cultural boundaries, an institutional setting that presented obstacles to collaborative governance.
Situated north of the South China Sea in a subtropical zone, Hong Kong’s climate is warm and mild. In winter, there is little rainfall and the temperature rarely drops below 41°F. In the summer rainy season, temperatures can rise to over 95°F. July to November is the typhoon season, when storms forming in the South China Sea and the Pacific Ocean strike the island. Despite an average annual rainfall of around ninety inches, Hong Kong is subject to periodic drought. 4 With continuing population growth, Hong Kong’s demand for water raced ahead of the capacity of its own reservoirs and catchments; until the 1960s when Hong Kong began importing water via a pipeline from mainland China, which in 2018 accounted for 80 percent of supply, the city faced regular water rationing. 5
Hong Kong was a Crown colony, developed while politically not part of China, under British administration and military protection. The colonial administration adopted a laissez-faire approach to the built environment outside the western commercial district. Both the European minority and the Chinese majority regarded Hong Kong as a place of sojourn rather than permanent residence, and resisted paying taxes and charges for infrastructure. 6 The built environment increased Hong Kong’s vulnerability to plague, and created path-dependent effects due to the costs of removing and replacing buildings and pipes, which limited options and delayed public policy responses to changing environmental conditions. 7 In foreign settlements, the influence of the British sanitary reform movement was powerful, and as elsewhere in the British Empire, residents “would come to regard the water closet and the flush cistern as indispensable markers of civilization.” 8 Westerners saw “oases of light in a waste of darkness and stagnation,” while they saw Chinese districts, where housing was crowded and low-cost private methods of waste management were used, as “inconceivably squalid and offensive to foreign eyes and nostrils, [filling] the foreign soul with a sentiment of unutterable disgust.” 9
When bubonic plague reached Hong Kong in 1894, first appearing in Chinese districts, westerners were concerned that the epidemic would spread to their own settlement. The colonial government drew on sanitary and medical expertise from within and beyond the British Empire, acting to quarantine victims and clear infected areas. However, the government did not act on the 1881 commissioned report of a British sanitarian, Osbert Chadwick, who followed miasma theory in recommending sanitary and housing reform. Hong Kong’s tenement houses had no artificial drainage, and sewers continued to channel sewage and storm water into its harbor without treatment. 10
Making the Miasma
Traditional cities in Asia served “inward-facing” states and were established to deal with internal concerns. With the exception of Japan, where the area of greatest population density was close to the sea, the largest cities, the capitals, were located at inland sites, chosen for ease of administration and defense. 11 Qing China was a “land” empire, which had expanded through military conquest, annexation, and alliances, as well as tributary trade with local rulers over large areas of Asia. From the late fifteenth century, European states began voyages of exploration that culminated in the establishment of “overseas” empires based on colonization and trade. 12 Portuguese traders established trading posts in India and Southeast Asia, obtaining rights in 1535 to anchor ships and develop a port at Macao. Spain founded Manila in 1571 as an entrepôt where Chinese products were exchanged for silver brought from Acapulco. In 1619, the Dutch East India Company turned the Muslim trading port at Jakarta into a fortified town, renamed Batavia. In 1757, the Qing made Canton (Guangzhou) the only official port of entry for Western traders.
By the late eighteenth century, Britain’s naval superiority had made it the major imperial power in the Indian Ocean, but Southeast and East Asian states held an advantage in coastal waters, where flat-bottomed junks could control access to ports. In the nineteenth century, innovations in transport (steam-powered riverboats), weapons, and medicine (the use of quinine to control malaria) gave Europeans the ability to wage war successfully on rivers and shallow coastal waters. 13 After the First Opium War (1839-1842), a series of international treaties turned large parts of China into an “uncolonized extension” of the British Empire. 14 The objective was not to acquire territory, but to further British interests by opening China to free trade and modern capital markets. Britain never established full settler colonies in East Asia, but treaty ports protected the rights of foreign merchants through the creation of designated “settlements” or “concessions”—European-style towns that were adjacent to but separate from the established city—and the granting of extraterritoriality. The arrival of Commodore Matthew Perry in Edo (Tokyo) Bay in 1853 prompted treaties that opened Japanese ports to American and later European traders. Siam (Thailand) retained political independence, but this was contingent on an 1855 free trade treaty with Britain. After the Second Opium War (1856-1860), around one hundred Chinese treaty ports were opened to British, French, and American merchants. By the end of the nineteenth century, almost all productive regions of Southeast Asia were under British, French, Dutch, or American control.
Eighty miles from Canton, Hong Kong Island was sparsely populated when it became a British territory under the Treaty of Nanking, which took effect in 1843. Attracted by the deep, ten-mile long harbor, the British developed a regional entrepôt for commercial activity in southern China, where goods were transferred between small Asian vessels and Western ocean-going ships. Hong Kong’s first governor, Sir Henry Pottinger, envisaged “possessing such a settlement as an emporium for our trade and a place from which Her Majesty’s subjects in China may be alike protected and controlled.” 15 Land auctions and peppercorn rents drew British, American, and Chinese merchants to the island, with commercial headquarters and warehouses soon crowding the waterfront. 16 British property rights, and the availability of work in construction and distribution, drew Chinese workers, especially during episodes of political instability on the mainland. Free of the restrictions of the traditional bureaucratic state, Chinese merchants embraced the new commercial opportunities the city offered. 17
In 1860, after Hong Kong’s population had almost quadrupled from 33,000 to 120,000 in ten years, the colony’s border was expanded to include three square miles on Kowloon Peninsula. In 1898, Britain leased the New Territories from the Qing government for ninety-nine years, increasing the size of the colony to 390 square miles (Figure 1). 18 The population grew to 246,000 at the time of the First Sino-Japanese War (1894-1895), 457,000 by the 1911 Revolution, and over a million before the Japanese Occupation (1941-1945). 19

Early twentieth-century Hong Kong.
In terms of location, Hong Kong was a typical colonial trading port, with a natural harbor close to productive land, and the Pearl River providing access to inland markets. Issues at these ports such as flooding, drainage, natural water sources, and the availability of flat land for building were afterthoughts to the founders. 20 Malaria and yellow fever—both transmitted by mosquito vectors living close to human habitation—had limited effects on indigenous adults, but were fatal to Europeans with no immunity. During the first decade of colonial rule, the British navy was so uncertain about whether it would remain in Hong Kong that it hesitated to build any permanent housing or drainage on the island. In 1843, malaria killed almost a quarter of British soldiers in Hong Kong. Over 5,000 military men died there during the first twenty-five years of colonial rule, mostly from contagious diseases. In the mid-1850s, outbreaks of cholera killed about 1,400 people. 21
Daron Acemoglu, Simon Johnson, and James A. Robinson observe that where high mortality and the proximity of large indigenous populations limited the number of European settlers, as in Spain and Portugal’s New World colonies, extractive institutions were likely to develop. These institutions exploited indigenous and slave labor, transferring the resources of the colony to the colonizer. Where mortality was lower and the indigenous population was smaller, settlers created “neo-Europes,” with strong property rights and institutions to check unproductive government activity and protect the economic welfare of colonists. 22 This distinction was made earlier by the Australian geographer, A. Grenfell Price, who noted that in colonies occupied by “migrant sojourners,” who aspired to make money through business in colonial ports and then return home, governments functioned as protectors of Western interests and were uninterested in the welfare of indigenous citizens. In migrant settler colonies of North America, Australia, and New Zealand, democratic institutions evolved in a path-dependent way, creating and sustaining high incomes among the colonial population. 23 Governments focused on ensuring the health of the settler population and created incentives to encourage their wider occupation of colonial lands, at the expense of Indigenous populations.
The colony of Hong Kong, and China’s treaty ports, occupies an intermediate point in this typology. Hong Kong’s European population numbered 6,000 in 1894, less than 3 percent of the total. 24 Immigrants from China entered voluntarily through an open border, and once present in the colony were subject to British law and regulation. In principle, this institutional framework was based on the British liberal ideal of equality; in practice, colonial justice and administrative regulation were applied unequally, with the Chinese cultural majority occupying a subordinate position to a dominant cultural minority. Chinese merchants and laborers who built and operated the city were mostly single males who intended to earn money and then return to their families. They did not use government schools and hospitals, and resisted increases in taxes and charges to minimize living costs. The colonial government did not see the Chinese as British subjects, and with limited public resources allowed local economic life and cultural practices to develop freely, as long as British interests were not compromised. 25 The production and control of the urban environment reflected and reinforced the group identity and sense of “self” within the foreign community; the ordering of complex social differences into homogenous zones made the Chinese “others” easier to control. 26
The spatial structure of the sojourner colonial city was made up of two components: an area of indigenous settlement, some of it pre-dating the colonial era, and an area of colonial settlement that included a military base and area of Western commercial activity. “What we have in the colonial settlement,” observes Anthony King, “is what one might mistakenly compare to an early twentieth-century upper, or middle-class European suburb: large residential plots containing spacious, one-storey houses, broad, tree-lined roads, low residential density (less than twenty persons per acre), and the generous provision of amenities.” 27 Colonial enclaves excluded working-class housing; this was located in indigenous areas, where residential density was high, levels of amenity were low, and narrow streets resembled the “walking city” of the pre-industrial era.
Plans for laying out the City of Victoria did not include areas reserved for Westerners and Chinese—segregation evolved as a product of the colony’s limited supply of land, high rents, housing shortages, and the absence of tax revenue from imports in a free port colony that the British government required to be financially self-sufficient. 28 Both Chinese and Europeans were free to bid in the 1841 land auctions (held two years before Hong Kong Island was formally ceded), with plots sold to investors hoping to capture future increases in land values. Soon after, the British Parliament declared that all land would be leased from the Crown on seventy-five-year terms, a policy that generated annual revenue from rents and property taxes. Chinese and European builders and developers preferred to invest in Chinese tenement houses (tong lau), as these could be constructed cheaply, rather than single-household European houses. In 1844, to allow for expansion of the Western business district, the government resumed the 1.5-acre Chinese-occupied Upper Bazaar district (consisting of 118 small lots of 504 square feet each). Displaced residents were offered plots (rent-free for four years) in an adjacent district called Taipingshan, where building regulations did not apply (Figure 2).
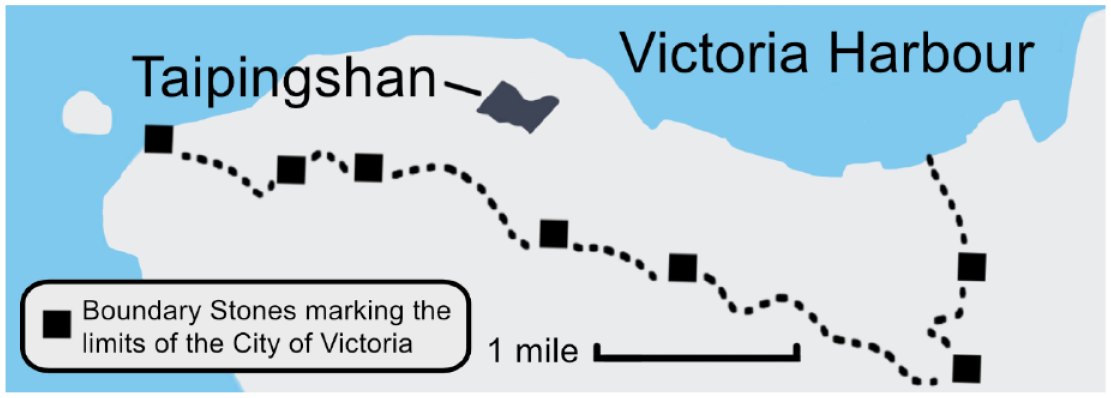
Detail of Hong Kong Island and the City of Victoria.
As Chinese housing districts became more crowded, with property owners meeting the demand for cheap shelter by economizing on space, government regulations encouraged segregation. Apart from police officers, no European was allowed to live in Chinese-populated districts. 29 By the 1870s, pressure was mounting on the colonial government to formalize this spatial demarcation. Europeans objected to living adjacent to the Chinese, fearing negative aesthetic impact and falling property values, potential safety issues if relations between Imperial China and Britain deteriorated, and perceived effects of Chinese hygiene and sanitation on the incidence of disease. Chinese districts epitomized “other-than European civility and order: they had become the literal embodiment, as it were, of darkness, noise, disease, and disorder.” 30 The European Residential District Ordinance of 1888 effectively prohibited the construction of Chinese-style houses in areas reserved for Europeans by specifying that only single-family houses could be constructed. In 1904, the Hill District Reservation Ordinance expanded these regulations, prohibiting Chinese families from living in the Peak District. 31
The Hong Kong government initially neglected the Chinese districts. Underinvestment in water management infrastructure and unenforced building regulations reduced housing costs and released resources for infrastructure, raising the profitability of commercial development. With flat land at a premium on the island, space for building close to Victoria Harbour was created through a series of public and private land reclamation projects. By the mid-1850s, the harbor’s shallow water zone had disappeared as trading companies created land for warehouses and docking space, and the government had begun draining and infilling swampy land to east and west of Victoria. Almost six hundred acres of land along the shore were created by 1904, through the construction of the Praya, an esplanade on the northern coastline, with the space between the seawall and coastline filled with rock and dirt from hillside cuttings. 32
Iam-Chong Ip argues that colonial urban policy in Hong Kong was mediated through a “sanitary syndrome,” a set of institutional and imagined relations between the state and the living environment, housing, and the people. 33 Accordingly, responses to sanitary problems were driven by concerns over the threat of disease to the minority elite posed by the growth and proximity of the Chinese population. The colony’s first housing ordinance, in 1856, requiring new houses to be provided with a water closet and ash pit, was motivated by considerations of public order—social and political stability—rather than the wellbeing of the Chinese majority. It was a complaint by a military official to the Hong Kong governor in 1881 that the sanitary state of the town was threatening the health of British soldiers that prompted the Colonial Office to commission a sanitary engineer, Osbert Chadwick (the son of Edwin Chadwick, who had spearheaded the British sanitary reform movement in the 1840s) to investigate the Chinese-built environment. 34
Chadwick’s report “not only showed the internal structure of the Chinese tenement house but also drew the colonial gaze to the Chinese-built environment and led the colonial administration to look at the everyday life of the Chinese.” 35 As with houses in contemporary British industrial cities such as Leeds and Manchester, tong lau were built back-to-back, without street paving and drainage. While housing in Canton was predominantly single-story, Hong Kong’s narrow brick tenements had second and third floors added using wooden planking. Each floor was typically rented by one tenant, then sublet by dividing the space into cubicles (“cabins”) of around ninety square feet. By 1881, adult males made up 64 percent of the population (out-numbering adult females four to one), and the number of inhabitants per house averaged 16.6, compared to 10 in Canton. 36 European houses offered more windows and living space—a European householder was likely to have ten to fifteen times the floor space of a Chinese householder. 37
Like his father, Osbert Chadwick conceived the problem of disease in spatial terms: to remove miasmas from the urban environment, he advocated public works to channel wastes out of the city and the clearing of areas of crowded housing.
38
In Hong Kong, Chadwick found a city that: . . . hitherto . . . has escaped the epidemics which have afflicted other places in the neighbourhood. The settlement is but 40 years old and the subsoil beneath the city may not yet be sufficiently saturated with filth to make it a hot bed for disease and a breeding ground of filth poison. It is somewhat premature to assume that this happy immunity will always continue, for the process of saturation is slowly but surely going on and if unchecked and cannot fail to bring forth abundant fruit, in the form of misery and disease.
39
“On a warm still day, at low tide,” Chadwick reported, “the stench along the Praya was most offensive.” 40 What Chadwick smelt was the accumulation of sewage, household waste, and silt from open drains laid on unpaved streets and alleys, intended only to carry storm water to the harbor. Outlets were above the low-water level, and tides were not strong enough to dilute and disperse the effluent. Several sewers could not be repaired, as they were built under private property, following natural watercourses, with the land then filled and sold. Inside houses, private drains, located in cook-houses, connected to sewers or open ditches. Earth floors were common in low-rent housing. Women and children used chamber pots, collected either daily, every second day, or weekly (according to each household’s ability to pay a fee) by unskilled “coolies,” who carried pots to the street or alley, emptying them into wooden tubs, and rinsing them over public drains. Twenty-five public latrines for men were available in the city; these were privately owned, drawing revenue from user fees and the sale of night soil shipped to Canton and sold as fertilizer to silk-producing farmers. In close proximity to dwellings and shops, latrines used metal tubes to separate solid waste from less valuable urine. The largest latrine had fifty-one seats over two stories, with tubes from the upper story connecting to wooden tubs and stoneware jars on the ground floor. 41
Drinking water was scarce. Some houses were not connected to mains; supplies to connected houses were only available for part of each day. The water was insufficient to flush waste from drains. Until the Pok Fu Lam Reservoir and distribution system was completed in 1863, Hong Kong residents relied on natural water sources. With aqueducts leading to pumps in densely populated areas, the system was only a stopgap measure; the reservoir held two million gallons (imperial)—enough to supply all citizens four gallons of drinking water per person each day for four days. Chadwick reported households drawing water from shallow wells, often located in the cook-house close to the house drain. As a result of Chadwick’s report, the Tai Tam Group of Reservoirs, capable of supplying eleven gallons per capita each day, was completed between 1883 and 1918. 42
Water management of the treaty port of Shanghai was more advanced than in Hong Kong. Initially, conditions in the two cities were similar. In 1862, a British doctor described Shanghai’s water supply as “surcharged with decaying matter,” drawn from canals that were “receptacles for all kinds of filth.”
43
Ratepayers in the International Settlement initially resisted pressure from health officers to build safe water supply infrastructure. By 1881, opinion in Shanghai had swung in favor of municipal subsidization of a private water company. As Kerrie MacPherson puts it, Commitment to the waterworks, to the extensive investment and construction that it entailed, along with substantial disruptions to their daily lives for several years as drains were opened, pipes laid, smells abetted, diseases risked, and streets cut up, represented a conscious commitment also to their own future in the city.
44
The laying of pipes and mains exposed private drains running from buildings to streets, raising concern about pollution from increased water supplies, but the city continued to rely on the system of removal of night soil by contractors for sale to local farmers. Progress in public health was less rapid in Chinese Shanghai, but by the late 1890s, the prosperous Chinese merchant community, supported by its doctors who had lived and trained in the West or Japan, was launching its own sanitary initiatives. In Shanghai’s French concession, the council purchased water from the British company for distribution to all residents, including Chinese, through public fountains. After the 1911 Revolution, Shanghai’s Chinese elites formed their own council, modeled on the Shanghai Municipal Council, which managed the Settlement, building four waterworks by the end of the decade. 45
Chadwick’s recommendations for sanitary reform in Hong Kong were more modest than those undertaken in Shanghai, reflecting the influence of Hong Kong’s geography and the path-dependent effects of earlier infrastructure and construction choices. With improvement in the water supply forthcoming, Chadwick’s preferred improvement to the sewerage system was the construction of an interceptor sewer that diverted sewage to a distant outfall, with the existing harbor sewers to carry storm water only. There were, however, practical obstacles to this. No suitable site for a sewage farm, with sufficient land for sewage to be used or treated, had been identified. Most building had taken place on sites where the land fall would not allow drainage by gravitation, the predominant means of disposal in outposts of the British Empire. Chadwick noted that “Every house (with few exceptions) requires re-draining,” but this would require houses to be demolished and streets dug up. Chadwick considered a dry-earth system, which “mixed with human excreta renders them inodorous, to some extent innocuous, enabling the mixture to be kept for considerable periods near habitations, without danger to health or causing a nuisance,” to be impractical, given the shortage of local soil and storage space. 46 “Considerable time must elapse before all is ready for the abolition of the hand-removal system,” Chadwick concluded, “for it would be madness to encourage the introduction of excreta into the present house drains.” 47
In the interim, Chadwick’s recommendations were focused on reducing crowding and improving housing conditions. These included the provision of open space at the rear of buildings, windows in every habitable room, a ban on earthen floors, a minimum room size per adult occupant, paving of streets—with effective drains—before buildings were offered for sale, government requisition and reconstruction of public latrines and uninhabitable houses, and improved waste collection. Chadwick’s 1882 report and a cholera epidemic the following year prompted the government to establish a Sanitary Board, consisting of medical and lay people, some government-appointed and others elected by limited public franchise. But the government considered Chadwick’s proposal for an interceptor sewer and sewage farm to be expensive, and was skeptical about its practicality. As Frank Welsh comments, “There was, after all, no money in it, always a powerful argument in Hong Kong, and the two thousand Europeans were adequately, if not luxuriously, housed.” 48 Although Chadwick took Chinese culture and habits into consideration, his recommendations for housing reform were resisted by Chinese property owners. Under subsequent ordinances, the regulations were made optional. An 1890 Squatters Ordinance allowed people who had built on Crown Land to apply for leases, but no new building code or sanitary standards applied. 49 It took the bubonic plague for the government to begin taking Chadwick’s ideas seriously. 50
From Miasma to Rats
Bubonic plague is endemic where the microparasite exists with rodents in a stable pattern of biological balance. When new patterns of human contact cross previous disease boundaries, the spread of plague can be rapid, as humans with little natural immunity suffer a high death rate, causing the parasite to seek new hosts. 51 Historians have identified the First Plague Pandemic, now known as the Plague of Justinian, which originated in central Africa, spread by ship to Egypt and through the Mediterranean, arriving in Constantinople (Istanbul) in 542. The Second Plague Pandemic, the Black Death of 1347-1352, moved from south west China along trade routes to the Crimea, then to most of Europe and Russia, with outbreaks recurring until the eighteenth century. The Third Plague Pandemic began when troops returning from Yunnan province brought the disease to other parts of China. Plague traveled along transport and trade routes, reaching the densely populated Pearl River Delta in the early 1890s. 52 For over two millennia, Canton has been the maritime gateway to China, and is possibly “the oldest continuously functioning port in the world.” 53 From 1759 to 1842, the “Canton System” provided the only official point of access for foreign merchants to the Qing Empire. Foreign monopolies were required to first land at Macao, then were piloted to Canton, where they traded silk, tea, porcelain, and, later, opium with licensed Chinese merchants (Cohong), who acted as wholesalers for goods from across the country. The system had collapsed by 1834 with the introduction of steamships, which allowed foreign traders to navigate the Pearl River. 54 Despite much of China’s foreign trade shifting to Hong Kong after 1842, Canton provided provisions as well as emigrants for the new colony, with frequent, unrestricted travel for business and family reasons taking place between the cities, and from Guangdong Province. 55
Almost two million people were living in Canton in 1894; contemporary estimates of the number of plague deaths in the city that year range from 80,000 to 100,000. 56 Plague was most severe in poor and overcrowded districts; death rates were lower among people who lived in the foreign quarter and on boats. The Qing regime was uncomfortable with quarantine measures, as segregation was perceived as equivalent to abandoning the sick, contradictory to Confucian principles. Officials ordered the cleaning of city streets, the burning of victims’ clothes, the collection of night soil before 10:00 a.m. each morning in covered buckets and boats, and set restrictions on pig slaughtering, fishing, and waste disposal in the Pearl River. 57
The Third Plague Pandemic differed from earlier episodes in that expansion in the movement of goods and people, due to free trade and technological innovations in transport (railroads and steamships) and communication (the telegraph), enabled rapid transmission of both the disease and news of its spread on a global scale. Hong Kong was a free port, and its sheltered harbor was open to ships and merchants of all nations. With 11,000 steamships entering and clearing each year, connecting to every major port in the world, “Hong Kong would proudly claim the title of the Empire’s third port after London and Liverpool.” 58 Within a decade of reaching Canton, plague killed roughly fifteen million people, most of them in India, China, and Indonesia/Dutch East Indies. In Hong Kong and other British colonies (such as Burma and Mauritius), the French colonies of Senegal and Madagascar, and the Portuguese Madeira islands, plague epidemics recurred in the first half of the twentieth century. In 1900, the pandemic reached port cities from Sydney to San Francisco and from Glasgow to Cape Town, but there plague was less virulent, as the northern rat flea (Nosopsyllus fasciatus) was less aggressive and less likely to bite humans than the Asian rat flea (Xenopsylla cheopis) prevalent in China and India. 59
Bubonic plague is not the result of polluted water, but officials in Hong Kong, drawing on contemporary understandings of miasmic theory, believed it to be so. Governor Robinson blamed the epidemic on the city’s “overcrowded and insanitary” condition, the “lack of any water or drainage system,” and an “increase in virulence” of the air after rain. 60 Working in Hong Kong in 1894, rival teams of Japanese and French researchers identified the Yersinia pestis bacterium as the source of plague, but not the means by which the bacillus was transmitted. 61 A French researcher working in Karachi discovered in 1898 that fleas on rats were responsible for transmitting the disease, but his discovery was not replicated and confirmed in other laboratory studies until 1905. 62 As with the British sanitary reform movement of the 1840s, observers who attributed the plague to miasmas correctly identified a correlation between disease, crowding, and poor sanitation. As Jeffrey Williamson observes, “Fortunately, the wrong theory and the right theory implied the same action—improved sanitation through drains, sewers, and clean water.” 63 Mobile rats, with high fertility rates, carrying fleas with plague bacilli flourished in dirty environments, containing waste that rats can eat, and poorly constructed housing, which allowed easy access for rodents. The likely exogenous causes of the eighteenth-century retreat of bubonic plague in Europe—the increasing use of brick and tile rather than wood and thatch in reconstruction after great urban fires, increased cleanliness, and the removal of small domestic animals from buildings—created urban conditions that were less conducive to the breeding of fleas. 64
Of 2,552 lives lost to plague in Hong Kong over five months in 1894, only 41 were from the non-Chinese population.
65
The death rate for the Chinese population was 10.6 per 1,000, and for the non-Chinese population was 4.1 per 1,000. Plague first appeared in Taipingshan, where 31,000 people lived in four hundred tenement buildings.
66
An 1894 government medical report found the district damp and badly ventilated, with drains of a most primitive and insanitary description. Earthen floors or floors laid with chunk of stones were the general rule while in most houses light seemed to be looked upon as an enemy to be carefully shut out.
67
Two-thirds of reported plague death victims lived in Kennedy Town, another Chinese district, which had been created by the infill of twenty-two acres to the west of Victoria in 1886. Dr. James Lowson, Medical Officer in charge of Hong Kong’s Epidemic Hospital, wrote in 1895: Predisposing causes are, speaking generally, insanitary conditions, and of these filth and overcrowding must be . . . two of the most important factors. The district of Tai Ping Shan supplied these factors in a marked degree at the beginning of the outbreak, the majority of houses being in a most filthy condition, as owing to the uncleanly habits of the people, the amount of . . . rubbish accumulates in a Chinese house . . . to an extent beyond the imagination of most civilized people. When to a mixture of dust, old rags, broken crockery, moist soil etc. is added faecal matter, and the decomposing urine of animals and human beings, a terribly insanitary condition of affairs prevails.
68
Fearing the plague would spread from Chinese districts to the rest of the city, the government took strong action. Teams of inspectors from the Sanitary Board, often comprised of both British and Chinese officials, carried out house-to-house inspections on a daily basis, with a “whitewash brigade” of military personnel disinfecting houses and floors, and burning infected belongings. Upper floors could not be washed because gaps between floorboards would have resulted in flooding of lower floors with dirty water. Infected patients were admitted to Tung Wah Hospital, a charitable organization founded and run by Chinese elites, using traditional Chinese medicine. After the government declared Hong Kong to be an infected port in May 1894, officials forcefully removed plague patients to the Hygeia, a hospital ship anchored in the harbor, and to the government-run Alice Memorial and Nethersole hospitals, where Western methods were used. Doctors gave patients alcohol and ice packs, and drained buboes, but these treatments were ineffective. 69 The government had to build mat sheds on Hong Kong Island to accommodate the large number of patients. 70 Buildings with large floor spaces, including a glass factory, a police station, and a not-yet-operating slaughterhouse, were converted into plague hospitals. 71
This regime of inspection and isolation was resented by the Chinese community. Of those treated in government hospitals for plague, 93 percent died, prompting suspicion from the Chinese population in Hong Kong and Canton that Western medicine was evil. 72 The dead were given neither individual graves nor traditional burials, which involved Taoist or Buddhist rituals where relatives continued to interact with the body. Immediate burial in mass graves made it impossible for families to pay respects to their ancestors and tidy up individual graves every spring as part of the Chinese traditional ritual. 73 The government’s unpopular and ineffective plague control measures sparked strong protest from Chinese residents, who blamed the Tung Wah and Chinese leaders for their failure to protect the patients’ welfare. Rather than be sent to hospital, many households hid sick members from inspectors. Almost half the Chinese population left the city in May and June, to be nursed by their own family, and to be buried in the villages where they had been born. 74
In September 1894, believing that the newly identified Yersinia pestis was present beneath wooden floors and in wall cavities in infected buildings, the colonial government “resumed” (compulsorily acquired) ten acres of land in Taipingshan and demolished 384 buildings, burning the rubble and removing the topsoil. New streets were laid out, and retaining walls, sewers, and storm water drains were built. 75 Building codes, wider streets, and the creation of public spaces (parkland, public latrines, and a Bacteriological Institute) reduced the area of land available for private residential construction from 272,000 to 97,000 square feet. 76 The landlords of Taipingshan, protesting the resumption and the new regulations, petitioned the Secretary of State. They felt that the government was infringing on their property rights, and they were unwilling to expend money and effort to maintain the tenement houses. 77
Different strategies were adopted in plague-affected cities of the U.S. Pacific. In Honolulu and San Francisco, the main policy action was, as in Hong Kong, directed at clusters of working-class, immigrant Chinese, where the disease first appeared. Plague was first reported in Honolulu in June 1899, and in San Francisco six months later. By March 1900, sixty-one plague deaths had been registered in Honolulu, a town of 40,000 inhabitants. This was a low rate of mortality, but two-thirds of those who died had lived in or close to Chinatown, adjoining the commercial waterfront. 78 With a jumble of narrow streets and alleys, two- and three-story wooden mercantile houses, shops, and rooming houses, with shacks, lean-tos, and storage sheds at the rear, Chinatown housed approximately 5,000 people at an average density of 143 per acre. Some officials estimated the area’s population at closer to 10,000. Destroyed by fire in 1886, Chinatown was rebuilt without safe water supplies or sewers. After initial reports of plague, the area was quarantined, and sanitary crews armed with solutions of carbolic and sulfuric acid found infected houses and stores built directly over cesspools, “gutters full of filth; lice, fleas, cockroaches, flies, and rats everywhere.” 79 Following the precedent of the use of fire as a disinfectant in Hong Kong, Honolulu’s Fire Department, at the order of the Board of Health, conducted daily controlled burnings of condemned dwellings. Three weeks after the burns began, a wind change fanned flames from a group of shacks to the center of Chinatown, and toward the harbor and city center. By the time the conflagration had burnt itself out, Honolulu’s Chinatown had been destroyed. 80
San Francisco’s Chinese, like other groups in the polyglot city, clustered by ethnicity in districts where they felt safe and could draw on networks of support. 81 The 1882 Chinese Exclusion Act, which banned Chinese coolies from the United States and prevented Chinese residents from obtaining American citizenship, was a product of increasing racial hostility separating the Chinese from other ethnic groups and confirming negative stereotypes. Accepting only half the pay rate of non-Chinese, Chinese workers predominated in labor-intensive clothing, boot and shoe, and cigar-making trades. Bounded by Kearney, Stockton, Sacramento, and Jackson Streets, Chinatown by 1900 had an estimated population of over 8,000, two-thirds of them single males, just under 60 percent of the city’s Chinese population. 82 San Francisco’s water supply was potable, if prone to shortages during dry spells, but the sewer system draining to the Bay was fragmented and prone to failure. 83 The Chinese lived in rooms in tenements, in sleeping spaces constructed on rooftops, and in dark, hand-dug cellars with earth floors, close to sewer pipes that leaked or failed to remove sewage effectively. Communal toilets, baths, and kitchens were used.
Public perceptions of the spatial elements of Chinatown—“dens, density, and the labyrinth . . . the unnavigable maze that characterized both the subterranean passageways within the buildings and streets and alleys above ground”—were established by press reports and government-sponsored inquiries from 1854 onward. 84 Before the outbreak of plague, public understanding of Chinatown was of a filthy, dangerous place, with the potential to spread disease to the entire city. As in Honolulu, Chinatown was quarantined after an increase in plague cases in the neighborhood, with police guarding every entry point and cable car routes blocked, sparking rumors among the Chinese population of official plans to burn the neighborhood, and re-build it for white habitation.
The Honolulu model of burning infected sites to kill the plague bacillus was accepted by physicians and health authorities worldwide, and was codified in international public health protocols adopted in Berlin in 1902.
85
In San Francisco, Joseph Kinyoun, head of the Marine Hospital Service who coordinated the city’s official response to the pandemic, was an advocate of site burning. “Chinatown, as it is at present, cannot be rendered sanitary except by total obliteration,” reported Dr. Williamson, president of the City Board of Health in 1901: It should be depopulated, its buildings leveled by fire and its tunnels and cellars laid bare. Its occupants should be colonized on some distant portion of the peninsula, where every building should be constructed under strict municipal regulation and where every violation of the sanitary laws could be at once detected. The day has passed when a progressive city like San Francisco should feel compelled to tolerate in its midst a foreign community, perpetuated in filth, for the curiosity of tourists, the cupidity of lawyers and the adoration of artists.
86
Despite the Honolulu precedent, the use of fire to eradicate plague was not continued in Hong Kong. The redevelopment of Taipingshan had taken five years, and the high cost reduced the government’s appetite for future works on that scale. 87 Plague had killed 8,600 people in Hong Kong by 1901; in four of the five years from 1897 to 1901, the death rate was around forty per 10,000 people. In 1902, Governor Sir Henry Blake requested expert advice from the Colonial Office on public health measures and housing policy. At the recommendation of the Colonial Office, “the British Empire’s leading plague authority,” William Simpson, a professor of hygiene at King’s College London, and a former health officer for Calcutta, traveled to Hong Kong to investigate the effect of sanitary conditions on plague. 88 Osbert Chadwick (then the inaugural Chadwick Professor of Municipal Engineering at University College London) also returned to Hong Kong, working collaboratively with Simpson to assess water supply plans and develop policies to improve sanitation. 89
Simpson’s and Chadwick’s reports, published in 1902 and 1903, broadly reflected the importance placed on improvements in standards of housing and sanitation, though Simpson was quite clear that “neither the scarcity of water nor the system of the drainage has anything to do with the plague epidemics.” 90 Simpson’s final report focused on plague policy measures that could be implemented quickly: increased surveillance by inspection of incoming vessels, reduce the rat population, and educate the population, activities all to be overseen by a new Plague Department. 91 Chadwick discussed engineering aspects of sanitation and water supply in two reports. The 1902 report on sanitation established that existing waterworks did not contribute to the plague, and referred matters of plague mitigation to Simpson. It focused on evaluating and suggesting improvements for the quantity and quality of water supply, and the city’s sewerage systems. In the report on water supply, Chadwick further elaborated his plans to expand the Tai Tam Group of Reservoirs, and the sanitary urgency for doing so. Guided by the reports, over the following decades housing and urban infrastructure reform took place at the individual household level and the redevelopment of small areas of the city. The Sanitary Board paved streets and alleys, added grates to drains, began daily trash collections, and from the 1930s provided metered water to every house. More specific plague prevention measures included rat-proofing houses by paving floors and filling rat paths with cement. 92
In San Francisco, Rupert Blue, who succeeded Kinyoun in 1903, rejected calls to raze Chinatown and pursued a strategy of “building out” the plague that was consistent with the Simpson’s and Chadwick’s recommendations for Hong Kong. State and city health official disinfected buildings with lime, and applied carbolic acid to cellar walls and floors. Landlords were required to concrete cellar walls and floors. Hundreds of dilapidated wooden buildings in Chinatown and the adjacent Latin Quarter (North Beach) were demolished, balconies and additions were torn down to increase natural light and eliminate rat nests, and rat traps were laid in Chinatown sewers. Dupont Street (renamed Grant Avenue in 1908) was asphalted to allow regular sweeping. 93
Bubonic plague was a shock that presented an opportunity to address features of Hong Kong’s built environment that were inimical to public health. However, the official response to the epidemic was not sufficient to alter a physical fabric with crowded housing and inadequate water infrastructure. Destruction on a larger scale, as with San Francisco’s 1906 earthquake, was an imperative to start over, with a “clean slate” that removed path-dependent obstacles to urban redevelopment. 94 Fire razed San Francisco’s Chinatown, rupturing water, sewer, and gas pipes, and creating nesting places for rats in the ruins. The district was soon rebuilt, much of it with salvaged bricks, but with wider streets, fewer blind alleys, concrete rather than planking sidewalks, and connections to new or repaired sewers. 95 When the plague recurred in 1907, rats, rather than the Chinese, were accepted as the source of the disease. Blue issued a directive to all citizens to set rat traps and poison, and burn garbage daily. A ten-cent bounty was offered for rats, living or dead, and teams of specialist rat catchers were appointed. Eleven thousand houses throughout the city were disinfected, with their backyards cleared. 96 Hong Kong developed similar methods of rat control, but little rebuilding took place. The city’s defective sewerage system and water scarcity would persist in the twentieth century, as the rate of population growth accelerated.
Conclusion
For Hong Kong, the bubonic plague epidemic of 1894 was a wicked problem that offered no easy solution. Public policy responses to the crises were slow to evolve. Plague was initially conceived in miasmic terms, as a problem of dirty water and inadequate sanitation, but as Chadwick’s 1882 commissioned report highlighted, practical difficulties impeded the construction of centralized water supply and sewerage networks. Rather than undertaking large-scale sanitary reform to combat plague, the Hong Kong government drew on sanitary and medical expertise from within the British Empire, and the experience of transnational approaches to plague mitigation in quarantining victims and clearing infected areas.
In the early twentieth century, after scientific confirmation of the role of fleas and rats in transmitting plague, policy responses gradually shifted from sanitizing infected houses and quarantining patients to rat eradication. While Chadwick reiterated broader policies to improve housing conditions, as well as large-scale sanitary reforms including the expansion of water supply and sewerage systems, only the smaller reforms were taken up immediately. Path-dependent effects of Hong Kong’s physical fabric prevented the government from implementing the recommendations in a timely manner. Resuming and reconstructing buildings on a large scale for a new sewerage system and improved sanitary conditions were not feasible due to the high economic and political cost. For Hong Kong, the infrastructure outcomes associated with the epidemic are part of a wider story of water slow infrastructure provision that was always one step behind the demands of a rapidly growing city. Although the construction rate of water storage capacity accelerated, modifications to the water supply system were limited due to its costly and contentious nature. As with responses to plague, social as well as scientific factors were critical in determining the speed and adequacy of response to the city’s water shortage crises.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Australian Research Council (grant no. DP35512900).