
Abstract
This article examines the causes and consequences of the diffusion of modern water supplies in Germany during the period from 1850 to 1913. It offers a comprehensive view of sanitary investments with a newly digitized dataset on water supply infrastructure construction dates for almost three hundred urban settlements. The diffusion of these investments was rather slow until the 1870s and then accelerated in subsequent decades, mostly because of financial constraints and then increasing demand for water. Regressing water supply infrastructure with mortality indicators shows that water supply improvements are associated with declines in mortality, but that their effect is small. In the absence of efficient systems of sewage disposal, water supply improvements had a limited impact on mortality rates.
Lack of access to clean water is still the norm in many communities around the world. The United Nations estimates that 2.2 billion people remained without safe drinking water in 2022, and 3.5 billion do not have safely managed sanitation. 1 The consequences of water scarcity for food consumption and hygiene are so significant that universal access to this basic resource is a key priority in international development, as stated in Goal 6 of the Sustainable Development Goals.
Countries in Europe score highest in measures of safe drinking water services, although this was not the case less than two centuries ago when most people lacked the conveniences of modern large-scale supply systems. As late as the third quarter of the nineteenth century, the majority of large urban settlements were not served by waterworks, with the exception of England and Wales. 2 The situation in Germany was particularly bad, with over two-thirds of municipalities with more than ten thousand inhabitants not having this infrastructure in 1876. Within twenty years, however, substantial sanitary investments brought modern water facilities to almost 90 percent of cities and set Germany on a path to achieve universal access to safe water. 3
This article examines the causes and consequences of this major transformation in the provision of urban water. Three inter-related aspects of waterworks construction will be considered. 4 First, I analyze the regional and temporal diffusion patterns of water supply infrastructure using a new dataset on construction dates covering almost three hundred urban settlements. 5 This complements the national and regional averages provided in other studies by offering a dynamic and detailed picture of investments in central water supply across regions and time. 6 Second, I review the literature on waterworks diffusion to identify the factors that determined the growing role of local authorities in public goods provision during the nineteenth century. I complement this with an analysis of the relationship between mortality crises during the 1866 cholera epidemic and subsequent sanitary investments. This complements related work on Berlin by Kappner (this issue, p. 545). 7 Third, I examine the correlation of clean water with mortality for the period 1877-1913 using a large sample of cities drawn from the dataset. This complements earlier studies that attempted to quantify the mortality impact of piped water in Germany with less comprehensive city coverage and a slightly different focus. 8
The following section discusses the construction of the dataset on water supply infrastructure and the diffusion of this networked infrastructure throughout Germany in the second half of the nineteenth century. This is followed by an examination of various hypothesis previously suggested to explain this investment, and a quantitative analysis of the relationship between public health crises and subsequent investments in urban infrastructures in the context of the 1866 cholera epidemic. An analysis of the link between clean water and mortality is achieved by matching the dataset and mortality information for a large number of cities for the period 1877-1913.
The Beginnings of Modern Water Provision in Germany
Traditional systems of water supply have a long history. At its peak, the city of Rome had more than ten aqueducts and a network of pipes bringing water to public fountains and some private properties. 9 Systems using waterwheels and wooden pipes supplied citizens in some cities during the thirteenth and fourteenth centuries, although their carrying capacity was quite limited. 10
The water demanded from these traditional systems radically changed in Europe by the mid-nineteenth century, as the population almost doubled in the preceding hundred years. 11 This demographic change was particularly intense in industrializing England and was accompanied by rapid urbanization. During the first four decades of the nineteenth century, the share of the English population living in towns of at least ten thousand inhabitants rose from 25 to 47 percent. 12 This added unprecedented pressure to traditional systems of water provision that proved obsolete by the mid-nineteenth century as water shortages became more common and the inadequate storage and disposal of waste polluted water sources, including wells, rivers, and reservoirs. Public hygiene worsened significantly. 13
Other countries underwent similar experiences, and Germany was no exception. 14 Institutional change and improved transport infrastructure during the first half of the nineteenth century created favorable conditions for economic development and population growth, which accelerated after the Napoleonic wars. 15 The German population increased from around 10 million to 30 million people between 1700 and 1850. 16 This demographic change put mounting pressure on existing water systems that mostly relied on direct access to watercourses, wells, fountains, or rainwater. Even in places with more complex systems, delivering a sufficient and constant water flow became increasingly more challenging during the nineteenth century. This prompted local governments to invest in new water technologies with a much greater carrying capacity as were being developed in England. 17
The first German city that built a complex system of water distribution was Hamburg, after a catastrophic fire in 1842. The English engineer in charge of reconstruction, William Lindley, supported the establishment of centralized water and sewerage systems following the recommendations of Edwin Chadwick, who published his well-known work on the sanitary condition of England in July that year. 18 Chadwick argued that proper environmental sanitation required an integrated network of pipes and sewers that could bring large amounts of potable water into the city and then efficiently dispose wastewater in neighboring agricultural fields. 19 Such a system represented an engineering challenge given the available technologies at the time and was very costly, but Hamburg was a prosperous harbor city, and accepted these sanitary expenses, finishing construction in 1849. 20
The experience of Hamburg marks the beginning of the sanitary revolution in Germany, and the starting point of my analysis. To examine the subsequent geographic diffusion of waterworks, I have compiled data on the construction dates of centralized systems of water provision in the German Empire between 1849 and the early 1900s, drawing on several sources. 21 Virtually, all medium- and large-sized cities had constructed water infrastructure by then. 22 The sample consists of 291 cities with at least fifteen thousand inhabitants that were surveyed in 1904 by the Imperial Health Office. 23
Secondary sources provide information on the year in which centralized water systems were built. 24 As these systems consisted of many intertwined elements, it can be challenging to pinpoint their exact construction date. Waterworks were not homogeneous across cities. For example, some places relied on water- or steam-powered pumping stations to lift water from underground sources, while others relied on gravity systems. 25 The reported completion dates often indicates when it was possible for dwellings to be connected to the pipe network to receive running water, but not when all citizens had access. 26 Berlin completed its waterworks in 1856, but only 40 percent of lots were serviced a decade later. 27 In other municipalities, the process was much faster. Görlitz built modern waterworks in 1878 and most houses were connected by the end of the nineteenth century. 28 The majority of citizens in Bremen consumed filtered water by 1890, although its water pumping system opened less than two decades before, in 1873. 29
Nonetheless, the reported construction dates capture a fundamental and positive transformation in the centralized provision of local water supply. The records often provide a comprehensive description of each project and identify its completion as a watershed in the history of a city. They refer to the construction of networks of main and secondary pipes leading to distribution points (houses, hydrants, or flowing wells), or the connection of water sources with reservoirs, including pumping facilities. To appreciate the urban transformation that the data capture, consider Hamburg, where in the sixteenth century cooperatives supplied a few houses directly using wooden pipes and piston pump waterworks, and householders fetched water directly from canals as well as the rivers Elbe and Alster. The scale of mid-nineteenth century investments transformed city infrastructures from decentralized, labor-intensive, and low-capacity systems to homogeneous, large-scale, and capital-intensive networks that could deliver water to thousands of households simultaneously. 30 The same was true in smaller towns, such as Küstrin or Emden, which in the 1890s installed steam-powered machines to replace rainwater cisterns and fountains, increasing both the quantity and quality of supplied water, through the use of sand filters. 31
Figure 1 shows the percentage of cities with waterworks during the period 1849-1904. “Cities with over 15,000 inhabitants in 1904” refers to the 291 places listed in the 1904 sanitary survey and represents information for a fixed number of municipalities without requiring a set population threshold, as is sometimes done in the literature. 32 This has the advantage of avoiding compositional changes stemming from population growth. For comparison purposes, Figure 1 also presents a series referring to cities of at least fifteen thousand inhabitants listed in statistical reports of the Imperial Health Office between 1877 and 1904; the sample size increases from 146 to 288 cities in this period. 33 As expected, the fixed sample lies slightly below the unconstrained series, because it contains smaller settlements that tended to construct waterworks later than did larger towns. Overall, the differences are not large and tend to disappear as the twentieth century draws nearer.
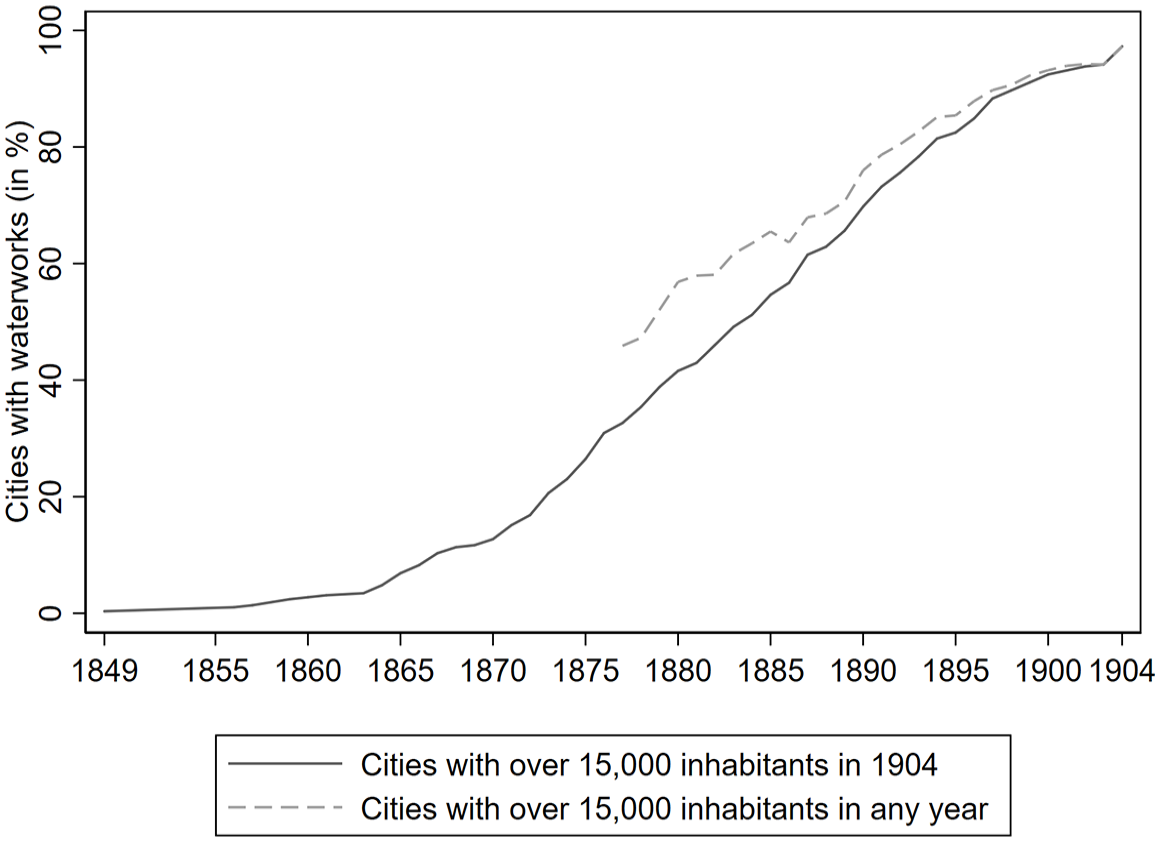
Percentage of cities of at least fifteen thousand inhabitants with water supply infrastructure works in the German Empire, 1849-1904.
The expansion of waterworks proceeded slowly during the 1850s. Although Hamburg’s system was installed in 1849, Berlin did not have one until 1856. This was the Stralauer Tor waterworks, which drew on the expertise of an English chief engineer, John Moore. The lag between the two cities in part reflected the unwillingness of the Berlin City Council to invest in expensive waterworks. A municipal supervisory agency subordinated to the Prussian state, and not Berlin’s public officials, signed a contract with a private consortium that led to the creation of the Berlin Waterworks Company. 34 By the end of the 1850s, only four other German cities—Würzburg, Altona, Magdeburg, and Mühlhausen (Alsace-Lorraine)—had installed waterworks. 35 This situation changed after 1870, as the share of cities supplying piped water steadily increased by 2.5 percentage points per annum (seven projects). By 1904, water supply systems were present in almost all medium- and large-sized urban settlements.
Figure 2 illustrates the spatial diffusion of centralized water supply systems throughout the German Empire. By 1870, such infrastructure was present in just a few regions of Prussia, Bavaria, Württemberg, and Alsace-Lorraine. The Kingdom of Saxony was somewhat ahead of the rest because all of its districts had at least one city with modern facilities. A decade later, most regions had added between one and three water systems in their urban landscape. Consequently, the majority of districts of the German Empire had at least one municipality with a piped network before 1880. The districts of Düsseldorf and Arnsberg stand out in this respect, since the number of waterworks increased by eight in the preceding decade. By 1890, virtually all regions throughout the German Empire had invested in water infrastructure, except for Oldenburg, Marienwerder, and Reuß. Westphalia and the Rhineland experienced the largest increases in the number of finished waterworks. By 1904, all regions had entered the new sanitary era. Unsurprisingly, the most populous districts—without considering Berlin—had the highest concentration of sanitary facilities: Düsseldorf, Arnsberg, Potsdam, and Oppeln.
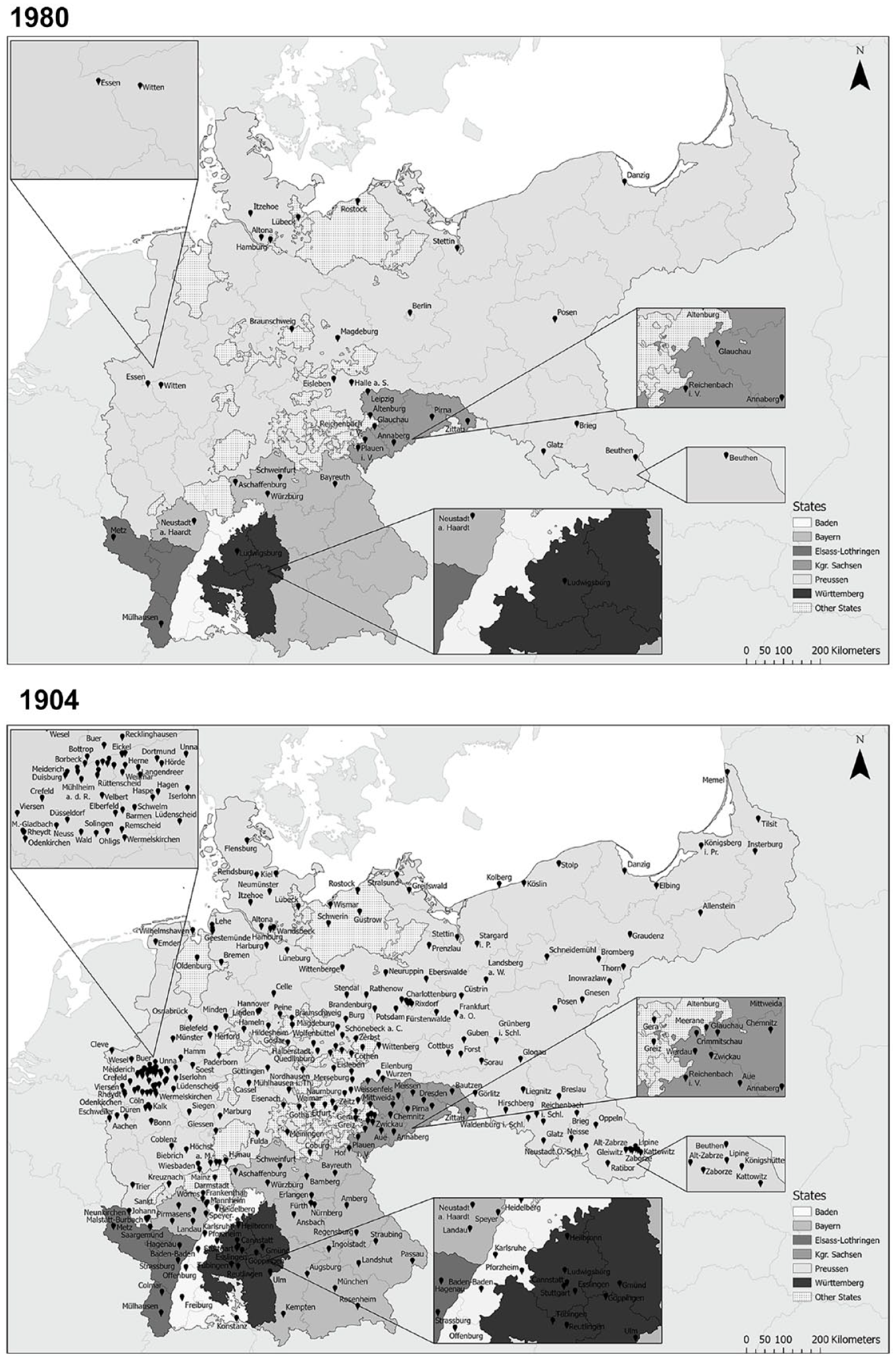
Spatial diffusion of water supply infrastructure in German cities, 1870 and 1904.
The water systems constructed by 1904 shared some similarities: 249 (86 percent) relied exclusively on underground sources; of the remainder, seventeen used a combination of surface and underground water, seventeen drew on surface water exclusively with (mostly) some sort of purification and filtration, and eight relied on wells and other traditional methods. The methods used to power waterworks also varied between cities. Distribution capacity ranged between 10 and 339 liters (2.6 to 89.6 U.S. gallons) per person a day. 36 As this does not account for inequalities within cities or the type of water used (domestic, industrial, or municipal), the wide variation in potential individual consumption suggests that urban infrastructure investment still had a long way to go before the typical resident was properly served. Nonetheless, the municipal efforts undertaken during this period laid the foundation to achieving universal access to clean water during the twentieth century. 37
Determinants of Investment in Water Supply Infrastructure
Investment in water infrastructure was related to increased demand, as population growth reached unprecedented levels during the nineteenth century. Consider the experience of Bremen, which grew more than fourfold; from thirty-five thousand inhabitants in 1815 to eighty-three thousand in 1871, and one hundred sixty-one thousand in 1900. At the national level, Germany’s population grew by around 15 million between 1870 and 1900, compared with 8 million in the three decades preceding 1870. 38 With overcrowding and poor construction standards, cities were vulnerable to major fires, as in Hamburg in 1842. This disaster made clear that firefighters needed reliable access to water. 39 City officials decided to invest in a system of hydrants that could provide plentiful and rapid access to water. Although the case of Hamburg is often considered unique in Germany, similar explanations for infrastructure investment are advanced in other cities. 40
Rising population density also increased the risk of epidemics, such as cholera. With the spread of this disease in the nineteenth century, numerous outbreaks wreaked havoc among populations throughout the world. While acknowledging the high toll in terms of mortality and social disruption, some scholars have argued that episodes of cholera had positive long-term consequences because they provided extra impetus for investments in sanitary infrastructure. 41 In Germany, the 1866 epidemic was identified as a catalyst for sanitary investments because it led Max von Pettenkofer—a renowned sanitarian—to organize a cholera conference and advocate ideas of sanitation and cleanliness. 42 This provided further momentum for the organization of associations and periodicals giving voice to the German sanitary movement, which in turn prompted the liberal urban middle class to invest in waterworks. These reform organizations included members and officials from city councils, thus linking them with institutions in charge of local policy making. 43
Some of the contemporary arguments in support of infrastructure were grounded in economic efficiency and morality. Chadwick argued that investing in sanitary infrastructure was desirable because more breadwinners would not die prematurely, which would in turn reduce the number of supported widows and orphans. Higher standards of hygiene also would improve morality among those at the bottom of the income distribution. 44 Pettenkofer provided an economic rationale. Using the example of Munich, he argued that the prevalence of disease imposed a large economic burden on the city that could be avoided with an efficient water and sewerage system. 45 Public health organizations argued along the same lines in the 1860s to seek the support of liberal businessmen and industrialists. 46
While compelling from a humanitarian point of view, it is also possible to test whether public health considerations were the prime driver of investments in centralized water provision. Faulty knowledge about disease transmission mechanisms impeded the design of effective public health policies. The long intellectual battle between proponents of the miasmatic and germ theories led to sharp policy disagreements that sometimes halted progress in improving health conditions (see Kappner, this issue, p. 545). 47
Unlike other municipalities at the time, Hamburg did not provide filtered water, yet plans to do so dated back to 1852. 48 Local elites with vested interests in preventing trade disruptions led them to embrace a miasmatic mindset that precluded quarantines and other isolation measures during epidemic outbreaks. 49 This proved disastrous when cholera hit Hamburg in 1892 and unfiltered water piped from the Elbe magnified the impact of the epidemic. In contrast, neighboring cities with filtration facilities only recorded a few cases. Another reason why construction works were delayed related to the complexity of community decision-making. Even if a city council was convinced that piped water was a necessary public good, disputes emerged about the technologies to be used (such as filtration, and the use of steam- or water-powered pumping stations), water sources (underground water, lakes, or waterways), and funding strategy (public or private). The processes of deliberation differed across cities along with geographic conditions and political dynamics. 50
Another factor complicating understanding of the link between cholera epidemics and sanitary investment is that both occurred during a period of rapid industrialization that raised water demand. Some of the emerging industries, such as steel production or textile finishing, required large amounts of water that required a reliable and plentiful water flow. The occurrence of epidemics was more common in relatively large, fast-growing, and prosperous cities experiencing rising incomes. If public health is considered to be a normal good, higher water demand would be expected as community income increased. These considerations call for caution in highlighting a particular element, as it is hard to disentangle multiple factors that were operating simultaneously. To deal with this, John Brown considers a sample of Rhenish Prussian towns during the late nineteenth century and finds that measured public health problems accounted for a small fraction of water demand, with industrial demands and the median voter’s tax payments emerging as key drivers of sanitary investment. 51
Recent empirical studies also find no direct link between mortality levels and water supply infrastructure construction dates. A study of thirty-four German cities shows that mortality levels five years before the establishment of waterworks were not statistically different from the rest of urban Germany. 52 I explore this idea further, by matching information for a sample of seventy-seven Prussian cities on the year in which water supply infrastructure was completed with data on excess mortality during the 1866 cholera epidemic (Figure 3). 53 Excess mortality is defined as the percentage difference of total deaths in 1866 relative to 1865. 54 Cities above (below) the horizontal line experienced higher (lower) mortality in 1866 than in 1865. Cholera episodes were catastrophic for most cities in the sample, with deaths much higher than in the preceding year. Following the “cholera-forcing” hypothesis, one would expect that cities with higher mortality to have invested in water infrastructure earlier than places with lower relative mortality in 1866. Figure 3 shows mixed evidence. Some cities with excess mortality rates above 75 percent did invest in sanitary infrastructures during the late 1860s and early 1870s, but so did places with much lower death numbers. In addition, a group of municipalities with high relative mortality in 1866 did not build their waterworks until the 1890s. To be sure, the pattern depicted in Figure 3 reflects a simple, correlational relationship, based on a sample of the German urban landscape—additional research is required to investigate the cholera hypothesis more systematically, with a sample covering municipal settlements with varying economic, social and demographic backgrounds.
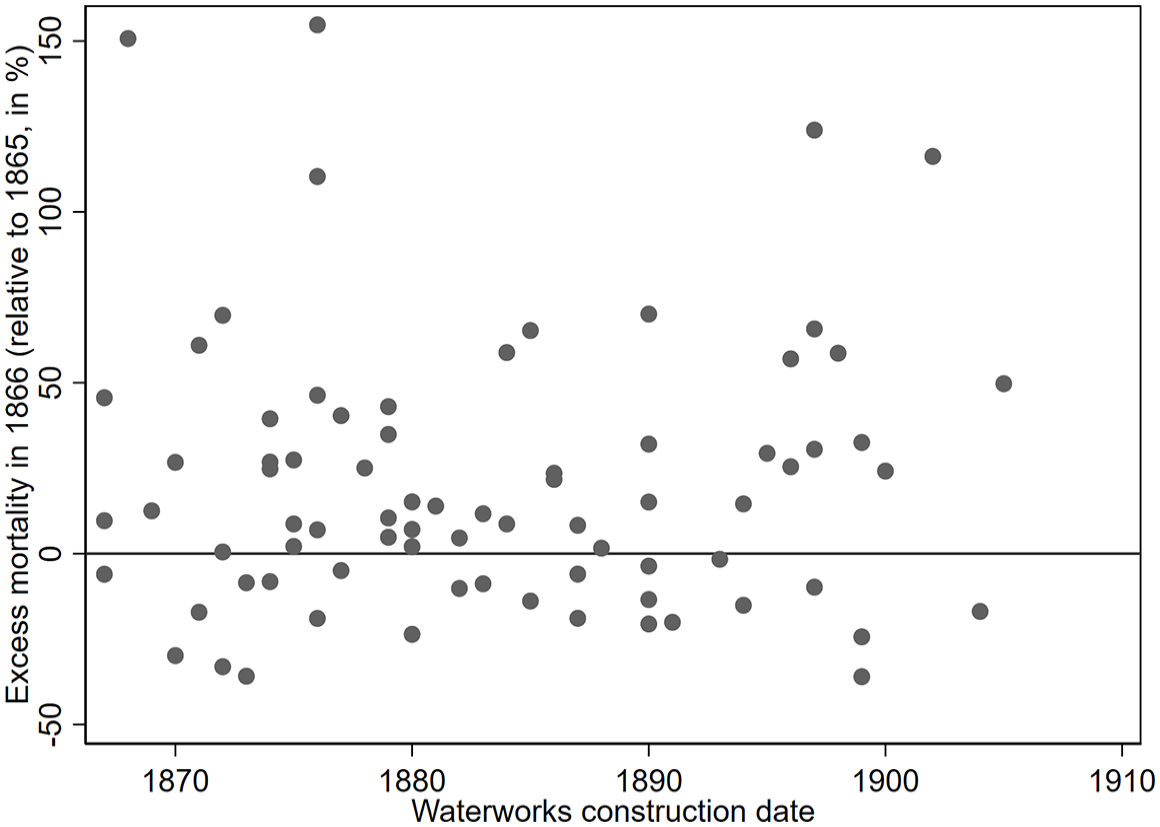
Excess mortality in 1866 and years of water supply infrastructure construction in seventy-seven Prussian cities.
Financial considerations are typically considered an important factor impacting investment decisions, because sanitary investment requires large amounts of capital. It is not surprising that Hamburg had the first and most advanced water supply system in Germany given its prosperous economy; or that Frankfurt, another wealthy city, undertook major sanitary works with apparently little concern about going into debt. 55 Municipalities with less buoyant public finances or unwilling to incur debt, such as Berlin, Altona, and Magdeburg, resorted to private initiatives during the first decades of the sanitary revolution. These proved unsatisfactory and most waterworks were publicly managed by the first decade of the twentieth century. 56
While funding ownership could influence the timing and type of sanitary infrastructures constructed, population or market size was critical in determining their viability. The high fixed costs associated with operating a centralized water supply system meant that per unit costs fell as the number of households connections increased. This can be tested by comparing water infrastructure construction dates and population for 128 cities (see Figure 4). As expected, there is a clear correlation between these variables, indicating that smaller cities built centralized water systems later than larger cities. At the same time, cities adopting piped-water systems earlier were probably larger at the turn of the twentieth century than those that lagged because access to good sanitary services reduced mortality and were more attractive to immigrants and investors. The correlation between population and infrastructure timing, therefore, may be affected by the choice of using population figures in 1900 instead of when construction works started or finished. If city populations are referred to the year in which their piped-water systems started operating, compared to a sample of cities that built systems after 1877, the correlation coefficient in both cases is virtually the same: −0.32. This suggests that bigger cities invested earlier and had advantages over smaller ones, regardless of the funding model. This was most likely due to their larger tax base and customer base. 57 Indeed, the costs associated with the new sanitary infrastructures were substantial and they represented an important part of the municipal budget. 58
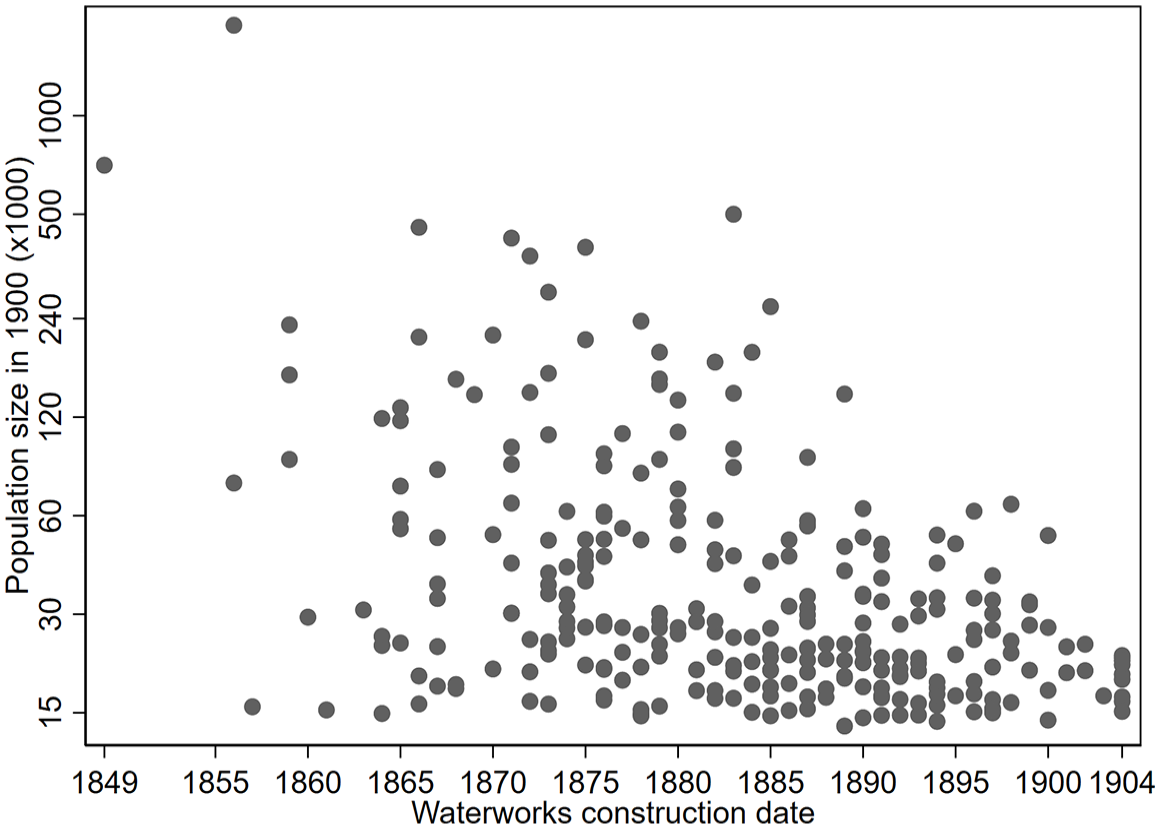
City population size (thousands) and dates of water supply infrastructure construction, 1849-1904.
Figure 4 also shows that the negative correlation between population size and waterworks construction dates exhibits a significant degree of variation. Dresden had almost eight times the population of Bonn in 1900, but both completed their water infrastructure works in 1875 (when the population ratio of the two cities was also similar). This variation suggests that other factors deserve consideration, such as institutional arrangements influencing politics and community decision-making. In England, investment in local public goods was associated with the removal of political constraints imposed by a widespread laissez-fare ideology and an expanding franchise, as political elites opposed taxation and thus the public provision of public goods. 59 This was not the case in Germany, where substantial sanitary investment took place while local political power was restricted for the majority of the (low-income) population. Municipal elections in many regions were organized using a three-class voting system, with voting strength dependent on the proportion of taxes paid by local individuals. The first class consisted of the wealthiest citizens who together paid a third of the taxes and had the right to elect a third of the city council. The individuals paying the next third of the taxes formed the second class and so on. In a period of high economic inequality, the system resulted in a high degree of political inequality. As an extreme example, the head of the Krupp family elected a third of the city council in Essen between 1886 and 1894. Other regions with less a priori restrictive systems, such as Frankfurt, which granted equal voting, restricted the franchise by setting income thresholds to become an eligible voter. 60
These electoral systems, contrary to what democratization theories predict (that franchise extension grants political voice to low-income citizens who are likely to demand public goods and redistribution), nonetheless seem to have boosted sanitary expenditures. 61 The city-state of Bremen completed its water system in 1873, despite civic life being quite undemocratic—senators were elected for life and the voting system gave preference to rich lawyers, merchants, and (later) property-owning male citizens. 62 The rising industrial elite stood to profit from a less hazardous disease environment that reduced sickness and had positive implications for productivity. Lower mortality rates also prevented human capital losses and ensured a plentiful workforce in a period of declining urban fertility and rural-to-urban migration. Negative externalities associated with disease outbreaks in poor neighborhoods affected well-off districts. This too may have been a motivation for supporting investment. 63 In late-nineteenth-century Germany, income distributions that were skewed toward high-income groups are associated with an increased probability of the construction of water infrastructure. 64
The case of Germany highlights the importance of politics and economic incentives in the centralized provision of piped water. Arguments appealing to the benefits for the whole population had limited impact, since the large sums needed to establish and maintain sanitary infrastructure required financial commitments that many would not pay without receiving something in return. Local elites demanded plentiful, reliable supplies of water to ensure a healthy workforce and their nascent industries. Rising incomes also prompted the affluent to seek the convenience of piped water for domestic consumption. Financial considerations and the demands of a rising liberal industrial elite were crucial determinants in achieving a political equilibrium that could sustain substantial sanitary investment over the long term.
The Mortality Consequences of Clean Water
During the second half of the nineteenth century, one factor influencing water supply infrastructure’s potential to reduce mortality was access to clean and germ-free water sources. Some sanitary infrastructures would have been relatively safe in municipalities with plentiful underground water that was less prone to contamination. In Posen, water was brought from a nearby mountain range using wooden pipes before a central water supply system was built in the 1860s. 65 Most cities were not so fortunate. Evidence from urban Prussian communities suggests that water pollution was a serious threat, since mortality due to waterborne diseases, such as typhoid fever or diarrhea, were the most important causes of death in the late 1870s. 66 These diseases took many fewer lives in England and Wales where citizens were provided with piped water. 67 In subsequent decades, German deaths declined as waterborne ailments were reduced substantially. Did clean water provision cause this decline?
Evidence from other countries suggests that waterworks removed disease-spreading microorganisms from distribution networks. Various studies estimate that water purification technologies account for a large part of the mortality decline in American cities during the first decades of the twentieth century. 68 Similarly, the modernization of water supply systems has been found to reduce mortality substantially in various parts of Europe and Asia. 69 In addition to the direct impact of fewer deaths caused by waterborne disease, mortality was also reduced indirectly, as water supply systems lowered the general disease burden from gastrointestinal ailments, such as typhoid. These types of diseases had a low fatality rate, but they scarred the immune systems of survivors, weakening them against later disease insults. 70
While it appears logical that water technologies had a substantial impact on mortality, there are several reasons to reconsider this link. First, recent studies from the United States suggest water purification technology accounted for a lower fraction of mortality reduction. 71 Second, diseases arising from fecal-oral contamination can occur via mechanisms other than drinking water—by poor transport of waste or personal habits in the household itself. Inadequate waste disposal and storage systems increase the potential of exposure to diarrheal ailments, through the misuse and poor maintenance of toilets, or inappropriate storage of human excrement. 72
Recent evidence for a sample of German cities shows that although piped water contributed to reduced mortality, its effects were limited in places with inefficient systems of waste removal. 73 Jointly, water and sewerage improvements account for at least 21 percent of the decrease in crude death rates (CDRs) between 1877 and 1913, and 25 percent of the fall in infant mortality. 74 The effects of sanitary infrastructures were not homogeneous through the urban landscape, however, with the largest declines in mortality in cities with a significant textile sector. Female employment may have diverted time away from infant care or breastfeeding, and in these circumstances, access to cleaner water may have had a particularly beneficial effect. Alternatively, a large textile sector may have created a more polluted environment, triggering water infrastructures that helped improve the disease environment. Cities with unequal income distribution experienced lower mortality declines after the construction of centralized water facilities. 75 One possible reason for this is that high inequality in situations of widespread deprivation means that a large fraction of the population live close to subsistence levels. With little or no savings, these groups could not contribute to government expenditure on public goods and would have little interest in paying for relatively expensive access to piped network. 76
The new database on water supply infrastructure construction allows us to explore the impact of sanitary investments on mortality. The data are linked with CDRs, infant mortality rates (IMRs), and various control variables for the period 1877-1913. The sample is restricted to the ninety-nine cities with information on mortality at least five years prior to waterworks construction to ensure sufficient measured variation in the results before and after centralized water provision begins. The model is estimated as follows: 77

where i and t indicate the index city and time period;
Table 1 presents the results, using both using CDRs (Panel A) and IMRs (Panel B) as dependent variables. The first column of each panel presents the outcome of regressing the dependent variable on waterworks and a set of city-fixed effects, year-fixed effects, and city-specific linear trends. The subsequent columns introduce demographic and other controls. For both panels, the coefficients are stable and robust. Their sizes imply that the (log) of CDR and IMR declined by 0.03 points after waterworks were constructed. Considering that the overall decline of CDR and IMR was 0.47 and 0.39 logarithmic points, water infrastructure is associated with a 6 percent (0.028/0.47) and 8 percent (0.033/0.39) reduction in mortality. These reductions are relatively low, suggesting that for the period 1877-1913, the construction of water infrastructure had a limited impact on mortality compared with the five years prior to construction. 80 One reason may be related to within-city patterns of poverty and wealth inequality, a factor shown to be of importance, for example in the case of Paris. 81 More generally, the effectiveness of waterworks interact with a large number of factors, such as the demographic composition of a city, the economy and structure of the labor force, or geographic endowments. While beyond the scope of this article, Gallardo-Albarrán has laid out a framework to understand such complex interactions. 82
Waterworks Construction and Mortality in 99 German Cities, 1877-1913.
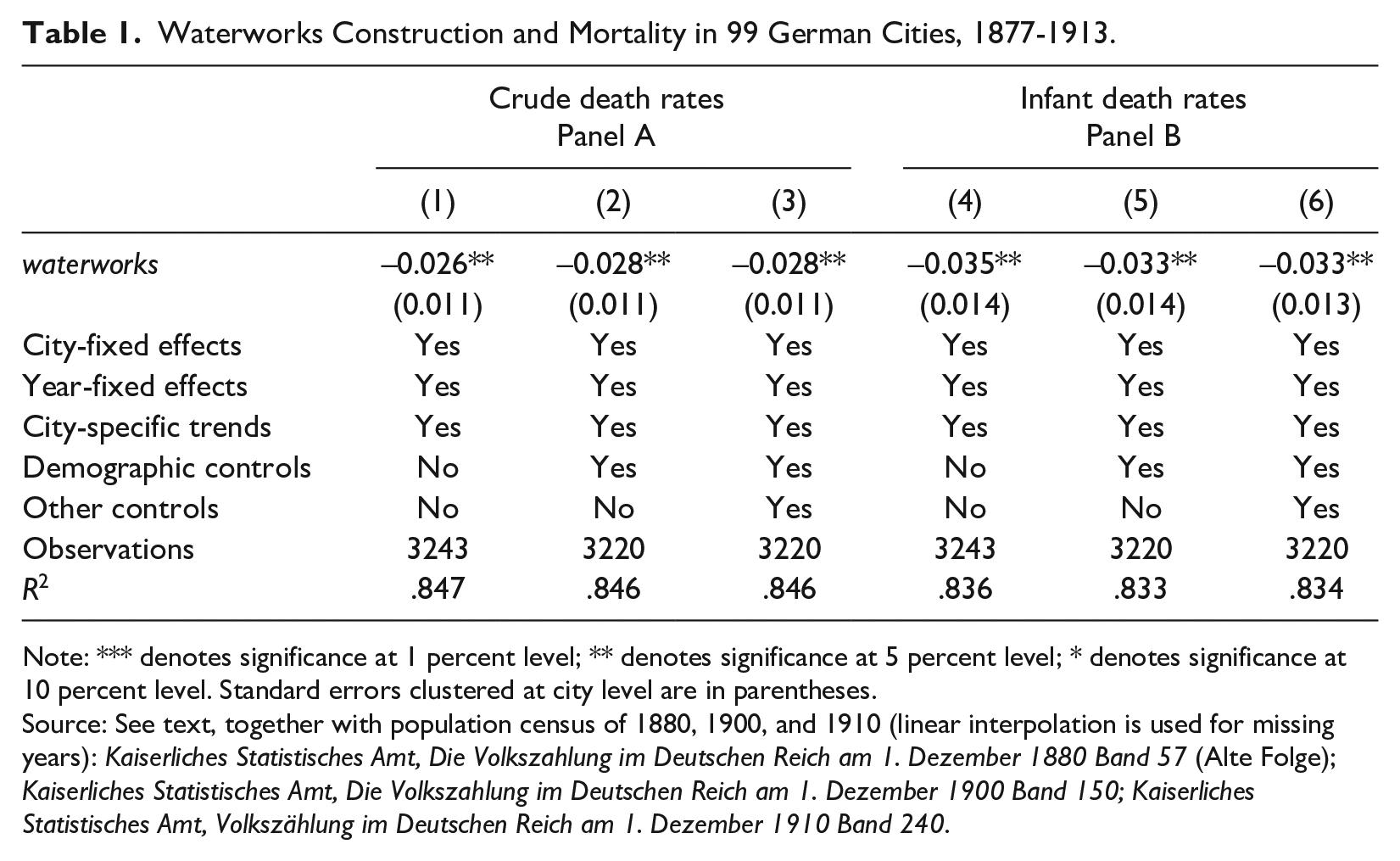
Note: *** denotes significance at 1 percent level; ** denotes significance at 5 percent level; * denotes significance at 10 percent level. Standard errors clustered at city level are in parentheses.
Source: See text, together with population census of 1880, 1900, and 1910 (linear interpolation is used for missing years): Kaiserliches Statistisches Amt, Die Volkszahlung im Deutschen Reich am 1. Dezember 1880 Band 57 (Alte Folge); Kaiserliches Statistisches Amt, Die Volkszahlung im Deutschen Reich am 1. Dezember 1900 Band 150; Kaiserliches Statistisches Amt, Volkszählung im Deutschen Reich am 1. Dezember 1910 Band 240.
Conclusion
This article has examined the causes and consequences of a major transformation in the German urban landscape during the second half of the nineteenth century—the transition to a modern system of water provision. It provides a comprehensive view of sanitary investments across regions and time with a newly digitized dataset on water supply infrastructure construction dates between 1850 and 1900 for almost three hundred urban settlements. The diffusion of this infrastructure was rather slow until the 1870s and accelerated in subsequent decades. By 1904, almost all cities with at least fifteen thousand inhabitants had constructed waterworks.
The literature on the determinants of sanitary infrastructures suggests that financial constraints combined with increasing demand may explain this variation in construction. Testing the argument that cholera triggered sanitary investments by considering the 1866 cholera epidemic suggests mixed results. Some cities affected by this scourge did build piped water supplies right after the outbreak, while others did not. More evidence is needed to assess this hypothesis more systematically.
Finally, the article examines the link between mortality and investments in urban water supply systems. Regression analysis combining the new dataset on waterworks construction with two measures of mortality examined ninety-nine cities for the period 1877-1913. The results suggest that water supply improvements are associated with relatively small declines in mortality. These findings support recent research that water supply improvements alone had a limited impact in the absence of efficient sewage disposal systems.
The experience of Germany during the period when universal access to clean water was becoming established suggests that other factors, such as financial considerations and the increasing water demands of a rising liberal industrial elite, were important in achieving a political equilibrium that could sustain sanitary investments over the long term. As the quality of such services improved over time through enhanced filtration technologies and higher network pressures, subsequent investments may have produced larger marginal benefits. Further research could provide a more detailed analysis of such subsequent investments.
Footnotes
Acknowledgements
I am grateful to the guest editors of this issue, Lionel Frost and Martin Shanahan, for their constructive feedback. I also received useful comments from Pim de Zwart.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Netherlands Organization for Scientific Research: “Global health inequality and the diffusion of sanitation since 1850” (NWO; grant number VI.Veni.201H.048).