
Abstract
In 1912, the Lancet published an article titled “The City of Madras and its immunity from epidemic plague.” The Lancet’s article was part of a spate of investigations by sanitary officials, bacteriologists, and epidemiologists into the reasons as to why the city remained largely free from the plague pandemic, which hit colonial India especially hard in the latter half of the 1890s. The absent epidemic in Madras suggests new ways to understand plague in colonial India and the relationship between the etiology of epidemics and cities more broadly. Colonial officials assumed that the plague would affect Madras in a similar fashion to the deadly outbreaks in Bombay and Hong Kong. The article follows varied explanations for the absence of the plague, showing how tropical environments were hardly inherently vulnerable to disease. Rather, the disease was constituted in specific urban environments, which had implications on understanding of disease vulnerability and immunity.
Introduction
In 1912, the Lancet published an article titled “The City of Madras and its immunity from epidemic plague.” 1 The Lancet’s article was part of a short spate of investigations by sanitary officials, bacteriologists, and epidemiologists into the reasons as to why this city, and the province of Madras presidency at large, especially the coastal districts, remained largely free from the plague pandemic, which hit India especially hard in the latter half of the 1890s. While colonial India, particularly Western India (and particularly Bombay) was severely affected by the third plague pandemic, Madras, located in southeast India, remained relatively less affected. Sanitary officials, the British colonial government and epidemiologists were all interested in why a city so similar to Bombay and Calcutta remained unaffected. To better understand the diverse trajectories of the plague in colonial India, the article investigates the various explanatory frameworks offered for the city remaining free of the bubonic plague. 2
The article reconstructs the years of the third plague pandemic in Madras city for two ends. 3 First, exploring the history of the Madras plague allows for a rethink of linear narratives of the plague in colonial India, which treat India as the epicenter of plague, and in turn focus on the epicenter of plague, namely, cities like Bombay, within India. Like Dora Vargha and others have suggested, epidemic beginnings, course, and endings are diverse. In other words, there is no straightforward trajectory of an upward curve of infections, followed by acquired immunity through vaccination or infection. 4 Scholarly attention follows the grain of the epidemic, focusing on its epicenter, origins, and climax. 5 This is especially relevant in the British Indian context. British India, as scholars have established, was deeply affected by the plague. However, British India was a deeply varying geography, with no singular trajectory of disease. While for the Indian subcontinent as a whole, the plague was no doubt devastating in terms of mortality, there remained regions that varied from this standard narrative. 6
Colonial narratives associated the plague with poverty, insanitary habitats, stench, and humans living in close quarters to one another alongside non-humans. 7 Mary Sutphen in her work on Calcutta and Hong Kong writes that “The houses occupied by artisans and laborers who were afflicted with plague were small and badly ventilated with damp earthen floors.” 8 Prashant Kidambi argues that colonial narratives characterized the plague as an “infection of locality,” or invited by the habits and living conditions of the urban poor. 9 Madras city then presented a challenge to this characterization of colonial cities as inherently vulnerable to the plague. 10 Rather, the city’s immunity from plague presented a puzzle to the colonial government and epidemiologists and therefore challenged conceptions that tropical or colonial cities were inherently vulnerable to plague and disease more widely. 11
Second, following the plague in Madras city reveals the importance of the “urban” as field—the infrastructures, climactic conditions, and non-humans, all differing radically from other cities that the plague did indeed affect severely. When the plague was recorded to enter Madras in a severe manner, it was in 1916, and it was a less visible variant known as pneumonic plague. 12 More specifically, the article shows how Madras city’s climate, infrastructures, including housing and the harbor, the nature and behavior of its non-humans, sanitary structures, and the city’s social geographies were uncovered as explanatory frameworks for immunity from the plague. This follows work by several medical historians who have long argued for particularizing the history of tropical environments. 13 Taking this further in the context of urban environments, Christos Lynteris’ work on the plague in Hong Kong and Bombay shows how soil and urban housing become objects and sites of investigation for bacteriologists and epidemiologists. 14 Here, I examine how an investigation of the plague within the urban, that is, Madras’ climate, sanitary regimes (particularly a “passporting” system), non-humans, harbor and housing, and social geographies constituted the city’s immunity to the plague.
In revealing the particular histories of Madras city and its experience of the plague, this article also engages and challenges the centrality of the plague in the Bombay Presidency, and indeed the scholarship surrounding the plague, which focuses on cities that were deeply affected by the plague. The plague in the Bombay Presidency, in both contemporary medical reports and scholarship, has come to dominate versions of the epidemic in colonial India. Whether creating nationalist and anti-colonial sentiment, producing labor bondage, a cartographic sensibility, presenting evidence for British colonial subjectification, and providing lessons for the present, the Bombay plague has been central. 15 In settler colonial cities, such as Cape Town, the plague prompted violent removals of Africans, undergirding and accentuating a paradigm of racially segregated settlements. 16 While these perspectives are no doubt important, looking closely only at cities that have been deeply affected curtails our understanding of the varied trajectories of plague in the city. Sonali Dhanpal, for instance, writing on the plague in Bangalore city, has uncovered a history of encampments, and “temporary” residences. Dhanpal argues that while the plague is often seen as momentary in terms of urban planning, the kinds of temporary, and precarious conditions it created in terms of encampments are often overlooked. 17 Nevertheless, Bangalore was a city that was clearly deeply affected by the plague. 18 These studies echo Myron Echenberg’s framework of following the plague across cities that were deeply affected by it, albeit in diverse ways. 19
This article therefore brings together city and pathogen within a singular framework. In the specific case of urban environments, studying city and pathogen together provokes a series of questions. Christos Lynteris, for instance, asks: what environments were conducive to the rise of plague; what forms of housing gave refuge to the disease; and what urban structures harbored the bacillus? 20 The plague in Madras city provokes the very opposite question. What made the city immune from plague? The urban and social geography of Madras, according to medical studies and the official archive, were the reason as to why this city was susceptible to plague and yet somehow immune to it. The layout of the city, its infrastructure, specific sanitary regime, the structure of caste, the behavior of the Madras rat and bandicoot in the city, and its climatic conditions, all had a role in explaining the plague’s relative absence from Madras. This explicitly varied from other cities, such as Bombay and Calcutta, where the plague caused substantial death and social disturbance. Following the trajectory of the plague in a city, which was on paper susceptible to the plague, but surprisingly escaped its worst effects allows then for a “place based” understanding of diseases, such as plague, and also a pathology-based understanding of urban space. 21 The epidemic’s behavior in Madras also contradicts wider understandings of plague in colonial India that framed colonial subjects, especially the urban poor, as putatively diseased. The spread, or lack thereof in Madras city, was therefore implicated in the making of the ways in which an epidemic behaved and the space of the city.
Tracking Plague in Madras City
While bubonic plague was spreading rapidly in Bombay and other parts of colonial India by 1898, “indigenous plague,” or plague cases that spread from carriers inside Madras were first sporadically detected only as late as 1905. Yet, plague lingered in the city, in fits and starts, but never really causing panic, for a lengthy period after. Indeed, after a lull in cases, 1916 was one of the worst years for the plague epidemic, with a severe outbreak of multiple kinds of plague. 22 The plague, however, loomed large in the imagination and writing of medical and sanitary officials during the years the pandemic raged across other British colonial cities. Like other colonial cities, therefore, Madras had to prepare for life amidst a pandemic, and various rules, laws, and regulations were passed to attempt to shield it from the plague. Its relative lack of cases earned it the tag of an “immune city,” and epidemiologists and bacteriologists attempted to understand why this was indeed the case. A narrative of the plague is useful in understanding how the plague archetype manifested in Madras, with less intensity and geographical spread. It also introduces the various dimensions of the city-space, of control, and containment.
The relative lack of plague cases in the city meant that the sanitary regime was far less antagonistic than in cities like Bombay and Poona. However, the early outbreak of plague does not explain entire phenomenon of rebellion. Cities in the Madras presidency, such as Bellary and Coimbatore suffered early from the plague, and yet did not see uprisings. Nevertheless, the rates of infections in these cities were nevertheless markedly higher than in Madras city. 23 In other parts of India, particularly in Western India, plague measures led to strong public disturbances. In Poona, a virulent outbreak of the epidemic led the British to think about a “strong” sanitary commissioner. W.C. Rand, who was chosen for the job in Poona, decided to employ the military to search houses for infected cases and police the streets. As Rajnarayan Chandavarkar shows, it was largely in Bombay and Poona that plague riots and plague panic took hold, due to these heavy-handed measures. The climax was when the Chapekar brothers shot Rand, who was in charge of implementing such measures on June 22, 1897. 24 More broadly, David Arnold had labeled the plague measures enacted by the colonial government as an assault on the Indian body. 25
In contrast, possibly as a result of the plague not entering Madras city as an unknown disease, there was no substantial protests against plague measures. 26 The rules for plague management within the Madras city stated:
As far as circumstances permit, Hindus should be employed in those parts . . . where Hindus predominate, and Muhammadans where Muhammadans are in a majority. Officers of all grades should use the greatest courtesy and consideration to the people, and should interfere as little as possible with their habits, feelings and religious prejudices. 27
At the outset of the plague when it hit Bombay in 1898, the medical administration in Madras was unsure on how to approach it. The municipality report in 1898 stated that The outlook cannot be considered to be very bright. Plague is indigenous within 80 miles of Madras though the number of cases has not been very great, yet there is good reason for fearing that they will become more numerous in course of time.
It mentioned that “many” seemed to think that plague could naturally not flourish on the East coast, as which the municipality was suspicious off. Furthermore, the municipality argued that containment measures could not be relied upon, as there were too many “loop-holes of space.” 28 The report warned that despite the vigilance of the Moffusil (district and town) officers, plague could arrive by rail or road, and that rats and other kinds of “infected merchandise” could bring the plague into the city, without the knowledge of the municipality. Urging caution, the municipality report stated that “Fortune has so far favoured us, and he is bold who would dare to say how Madras would fare” 29 (Figure 1).
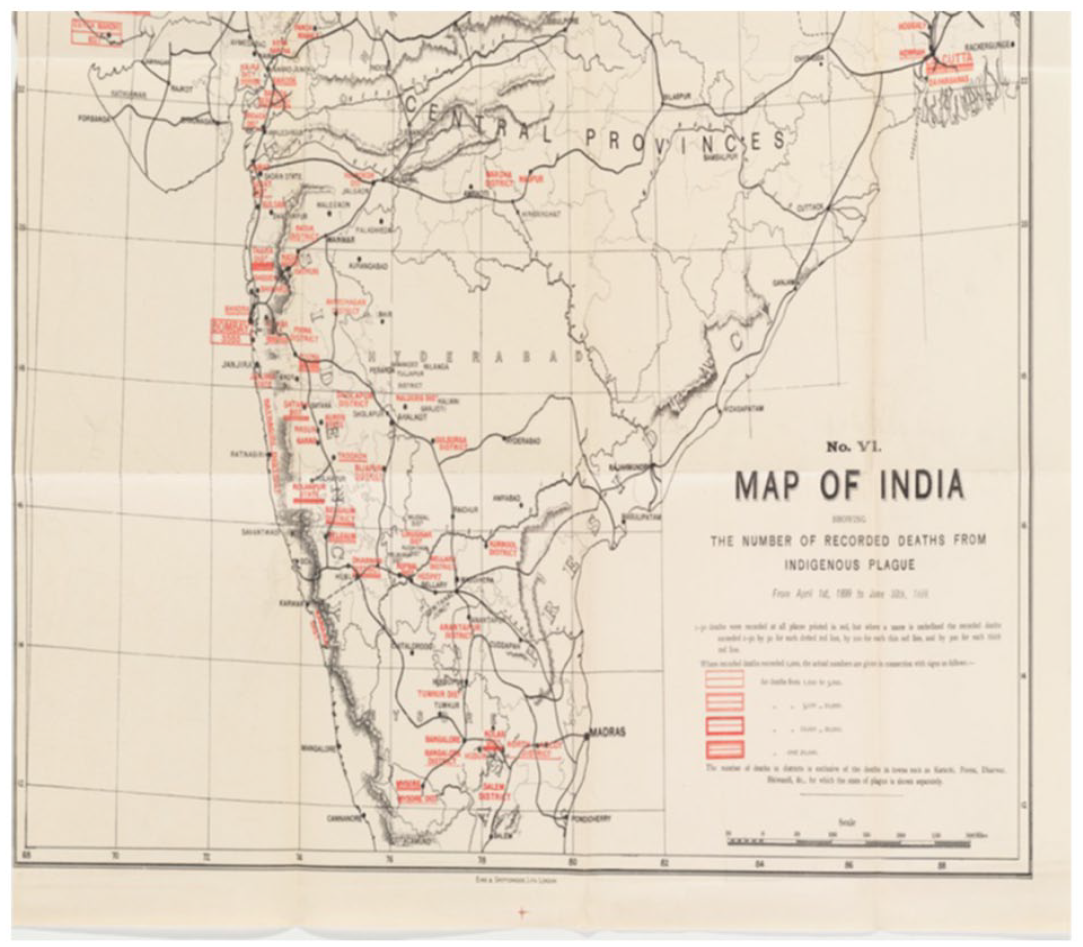
Map of India showing plague deaths. Madras here is not highlighted in red like many other urban regions.
The story of indigenous plague in Madras city began from January 1905, rather late compared with other British port cities. The seven-year delay, after the plague had first come into Bombay, meant that the colonial government had developed a particular blueprint of plague management through medical science, urban policing, and legal regimes. A fishing village near the city had experienced an “unusual number of deaths,” and the sanitary establishment came to investigate. Three women were found suffering from ulcers, and the Madras doctors were certain that this was plague. No rats were found in the village itself, which composed of 613 persons and 118 huts. However, immediately to the rear of the village, was a Mauritius-Fiji emigration depot. Upon questioning, the superintendent of the depot admitted that rats were seen dying in the depot, and the superintendent was unaware of how they were disposed. Investigation revealed that the rats were thrown across the depot walls, onto a road that led to the village. Immediately, the rats were sent for bacteriological examination at the Guindy laboratory, and found to have been infected with plague. The depot was evacuated immediately. The events left the sanitary establishment puzzled. The immigration depot was a crowded space. Whether in case of the depot, “with its hundreds of coolies from plague infested areas” or “the fishing village with its harbour working population,” where the precise origin of the plague proved “impossible” to prove. Furthermore, it was of enormous surprise to the investigating officials that the plague had not spread. 30
There was no uniform in which villages around Madras city responded to the plague measures. On April 21, 1905, a case of plague was discovered in a village named Hancock Paracherry. This was a large fishing village, and very soon, three more cases of the plague occurred. According to municipal reports, residents cooperated with the evacuation measures. The inhabitants of the plague affected houses were evacuated, and a rat exterminator was laid in each of the huts. Two more cases of plague were discovered in June of the same year, but these were detected in visitors who had come into the village. Once again, no further cases were detected in the following months. 31 In Cassimode Kuppam, again a coastal village, a different story prevailed. The municipality referred to the inhabitants of the village as “a particularly illiterate and ignorant lot.” This village, officials argued, attempted to conceal every illness from the authorities, prevent rat-catching, and were opposed to evacuations. On May 20, a woman suffering from fever and pneumonia was removed to a health camp and plague bacilli was detected in her sputa in abundance. By August 18, eight cases of the bubonic plague were reported. Although no other cases were detected for the next four months, in December of the year, the threat of plague re-surfaced once again. After a single infection in December, 20 infections were detected in 1906. The rat catching and extermination staff, who had almost been disbanded, were re-engaged. Every single rat caught was sent for bacteriological examination, and there was a clear correlation between the infected rat and the region where the plague cases in humans occurred. 32
Similarly, the city was threatened with an outbreak of plague in 1907. The corporation report commented that while the threat of plague remained, the city remained “plague-free.” The only community to suffer a serious outbreak was the Marwaris, “a money lending class.” Around fifty members of the community had absconded from Madras without the knowledge of the Poonamallee authorities (a locality where a plague observation center had been setup), the area they resided in. What followed was a large-scale search of Marwari residences, and arrangements were made to keep the houses and colonies they lived in under close observation. The Poonamallee area of the city was largely cordoned off, with plague passports demanded from anyone entering Madras wishing to visit or reside in the region. Policemen were also deployed to man the toll-gates, to prevent anyone running. Once again, the city as a whole, survived, with the Poonamallee outbreak not escaping to other parts of Madras. 33
The years following 1907 were of relative freedom from plague. The official reports follow a standard format, and only imported cases were found in the city. 34 Plague cases were minimal, and rules were relaxed. Indeed, in mid-1908, the post of the superintendent of passports, a nodal officer who dictated the passporting system, was disbanded. 35 In 1910, an inquiry was commissioned led by Captain Norman White, as part of the Plague Research Commission, on the “comparative freedom of Madras from the plague.” The Madras government and corporation awaited these details eagerly and described the problem as one of “great complexity.” The Madras government was particularly surprised because: (1) the Mus rattus, which was identified as the most common agent of transmission, was abundantly present in Madras houses and (2) that Madras rats were in fact more susceptible to plague, and equally infected with fleas like those in Bombay. 36
The plague, however, stayed with Madras city over the decades to come, with 1916 perhaps one of the worst years the city faced. Several towns outside Madras city, including Ambur, Gudiyattam, Salem, and Coimbatore, were all affected by the plague in 1916.
37
As plague restrictions had loosened, many infected persons traveled from these towns into Madras city, expecting heavy plague measures in them. The chances of outbreak, a health report argued, were much greater in large cities like Madras, where once an infected person had entered into a “large and busy railway station” like the central railway station, it was difficult to track them. Furthermore, the important passporting station at Basin Bridge had shut down by 1912.
38
In 1915, there were no cases reported; in 1914, three cases reported; and in 1912 and 1911, there was just the one case. The city had assumed that plague had passed it.
39
When it came back in 1916, the complexity of the plague was recognized. The city health officer commented Madras city offers every facility for an outbreak of plague, in case infection is once introduced. Bubonic plague is not communicated from man-to man without the transmission of the rat, in the case of pneumonic plague, the infection could be contracted with coming into proximity to the sick.
40
Following the 1916 outbreak, reflections from the corporation report suggested that the passporting system the authorities had instituted had been “instrumental in keeping plague” away from Madras, and the abolition of the inspection station at Basin Bridge had a lot to do with its return, through the smuggling of cases into the city. Evidently, plague had now become an annual occurrence within 100 miles of the city, and yet the report observed that it was only “luck,” which had stopped the plague from entering the city. In 1916, a rapid succession of plague cases had occurred between the months of September and October. A particular case that was closely surveyed was a pilgrim party of 45, who had come in from the temple town of Rameswaram. Three people in the party were found to have plague. The party also had a lorry load of luggage, in which wheat flour, sugar, and other materials which, according to the sanitary commissioner, were spaces in which fleas or even infected rats could seek refuge. As the health officer for the city put it, “it looked for a time as if madras has been be visited for the first time with an actual and not merely threatened epidemic of plague.” 41
The narrative of plague shows how the colonial urban in Madras attempted to track, trace, and map the plague and prevent it. However, colonial rhetoric on associating the plague with particular communities, whether it is coastal fishing villages or Marwari merchants also persisted. This led in turn, to a generalizable nature of different communities and the city as the plague emerged as a medically standardized disease. However, at every turn, the corporation and the sanitary administration were fearful that the plague would arrive in Madras. As they continued waiting for the attack, particularly as conditions in other colonial cities, such as Calcutta and Bombay worsened, the colonial government started investigating why Madras particularly was not affected. The next section turns to the diverse explanations offered for the making of Madras as a city “immune” to the plague.
What Constituted Plague Immunity
Both contemporary reports and recent scholarship have commented on the remarkable fact that as the plague raged across India, Madras remained relatively unaffected. The Indian Plague Commission report, which has published in 1901, had sections on the Madras presidency that were fairly short. Typically, the write up occupied a maximum of a page and a half of the report 42 In it, the districts identified as infected through “indigenous plague” were Bellary, Anantapur, and Salem. Later in 1899, larger towns, such as Vellore and Kuppam were affected, with the report identifying the source of infection from Mysore. 43 On the town of Madras itself, the report commented that “the town of Madras has not been infected so far, though a number of imported cases have occurred in it.” 44 In other words, the plague commission, and the local sanitary establishment had found no evidence of the epidemic spreading. In 1927, a city mortality committee, which was appointed to investigate the reasons and causes of death in the city and recommend measures to improve life expectancy from disease stated that “Plague has never been a menace to the health of Madras city and needs no consideration in any review of health conditions . . .” 45 By the late 1920s, the mortality committee did not even efficaciousness in putting out case rates. Rather, the low death rates implied that the city definitively had avoided the plague epidemic that had circulated across colonial India since the 1890s. 46
Natasha Sarkar calls the plague in Madras “the epidemic that never was.” 47 In tracing the anxieties of the Madras sanitary administration caused by plague, Sarkar showed how a session of the Indian National Congress, to be held in the town of Amaravati sparked off fears. Amaravati was not far from Punjab and Bombay, where the plague was spreading rapidly. 48 There were forty delegates from the city of Madras who were penciled in to attend the session in Amaravati. The Madras government was apprehensive, and fearful that these delegates would come into contact with others attending the session from the plague affected parts of India, including Punjab and Bombay. The government therefore monitored delegates closely. On their return, all forty were quarantined in either Ooty or Arakonam, for a period of ten days, after which they could enter the city. Sarkar argues, “These initial fears were unwarranted because plague never really made its presence felt in this region.” 49
In the years of the plague, there was research within Madras, in the field and lab, to explore why the city had not suffered the plague. In what follows, I explore in detail how epidemiologists and sanitary officials arrived at this conclusion. The explanatory logic encompassed (1) the framework of sanitary governance, including plague passports, plague rules, quarantine, and disinfection; (2) the social geography of Madras city and the possibility of caste rules (an idea that upper castes are “pure” and lowered castes are “polluted”) and plague rules co-existing; (3) the behavior of non-human forms (rat, bandicoot, and flea) of transmission in Madras; and (4) the climatic conditions of Madras city. 50 Each logic posited a different explanation of plague immunity. Taken together, these varied explanations show how tropical environments were hardly inherently vulnerable to disease. Rather, disease was constituted and in specific urban environments, which had implications on how disease vulnerability and immunity were understood.
Some early investigations were entirely unsure why the Madras presidency as a whole remained unaffected. Writing in 1899, Spencer Low, who served as medical officer of the plague camp and railway inspection station at the busy railway station of Jolarpet stated: “The Presidency of Madras, whether from its geographical position or as a result of the preventive measures adopted by its government, has not suffered so severely from epidemics of plague as have some other parts of India.” 51 Low’s observations were backed by the statistics he produced. While the nearby Mysore and Hyderabad province, with a combined population of 17 million, had 20,000 deaths by June 30, 1899, while Madras with a population of 36 million only suffered 2,092 deaths. Particularly, Madras city itself suffered only 11 deaths, and all were imported cases. 52 As Low noted, there were “ninety-nine ways” of accessing a district in the presidency, for “every one that could be guarded.” Low did not believe that sanitary conditions of the towns in the presidency, or Madras city, were sufficient to explain immunity from plague. Low was left puzzled as so what created the conditions for immunity. 53
Under Lt. W.G. King, the Madras sanitary administration, several officials argued, was remarkably efficient in preventing the plague from entering the city. King, who is even today celebrated as the “Englishman who banished plague from Madras,” was viewed as an uncompromising and commanding official. 54 The logic of sanitary administration, like in other cities was multi-pronged. Madras was positioned, like other busy port cities, at the intersection of sea, rail, and road routes. 55 The most frequent passenger trade was between Madras and Rangoon, a city the Madras officials believed that plague was fairly prevalent. 56 The harbor in Madras, however, was not fully built till 1905. The lack of a harbor meant that larger boats had to disembark quite far from the shore and quay. The cargo was then put on to small boats, and taken ashore. The method, one study argued “diminished” if not “obliterated” the risk of bringing in plague-infected rats, who in the case of other cities easily made their way from the ship to the harbor and then the shore. Rice, which was the commodity most imported from Rangoon, was tied in gunny bags and stored in large go-downs, before importers sold them into the Indian market. It was here that the risk of rat infestation was at its greatest. 57
The process of surveillance of ships and the harbor was, of a corporeal nature. 58 Ship crews had to be inspected morning and evening. Typically, coolies were employed by ships to lift loads on to the shore. The shore coolies’ addresses were taken down, and any coolie who did not return to work the following day would have their houses inspected. There was a registration system for coolies, and the police were to enforce the system, preventing any but registered coolies from boarding ships. Policemen further had to prevent ship crews from landing, and compel all coolies and crew to use the bathing stations every time. 59 Passengers, especially those traveling in third-class compartments were forced to have their luggage disinfected by heat. 60 More generally, enormous importance was placed on pilgrimage and commercial maritime routes, quarantine, and attempts to control disease. 61
Rail was a more severe threat. Madras was connected to two main railway systems, including the “Madras and Southern Mahratta” system and the “South Indian railway” system. A line north linked Madras with Calcutta, and a southern line with Tuticorin, a north-west line with Bombay and a south-west line that linked to the Mysore. 62 The railway from Mysore was repeatedly identified, in contemporary reports and studies shortly after, as the chief danger to Madras city. Mysore, a nearby princely state, was severely affected by the plague. J.P. Bedford, in a report on the Madras presidency’s plague measures, was caustic in his assessment, calling Mysore “without policy.” Qualifying his comment, Bedford claimed that in Mysore, no measures were forced on the people—just advice given, and people left to follow it if they saw fit. 63 Bedford compared plague with a commodity, labeling Mysore a free-trade state and Madras a controlled one, whereby the commodity trade flourished in the former, and was limited in the latter. Bedford’s assessment of the plague measures across the presidency were overwhelmingly positive, and although they did not entirely prevent infection from crossing over, it was also extremely difficult for plague-infected persons to come into the state. 64
To move through Madras city’s railway station, a passenger required a “plague passport” (see Figure 2). The passporting system was implemented strictly within the city. Under the Epidemic Diseases Act of 1897, the city had established its own set of rules. 65 Anyone entering the city from a region that the Governor of Madras had declared a plague affected region had to obtain a passport. A series of eight rules governed the life of the plague passport in Madras. They applied to any passenger who arrived from a plague affected district. The officer at the passporting station noted down details of their residence, and the passenger was required to report any medical occurrence up to ten days after their arrival . 66 When a passenger arrived via rail from a plague affected district, they were stopped and issued a passport at the Perambur railway station. The city was divided into circles, and passported passengers would have to meet a designated passport at each circle each day, to declare themselves free of symptoms. 67 They also had to furnish details, such as their home address. The passport focused on the household of the passenger (assumed to be a male), specifically, women and the children, and stated that any “occurrence of abortion amongst women . . .” in a passport holders household, “of convulsions amongst children and of sudden death in the aged should not be ascribed to ordinary causes without medical advice.” 68 The passporting system in Madras city therefore sought to carefully monitor entrants from any plague affected district across colonial India (Figure 2).
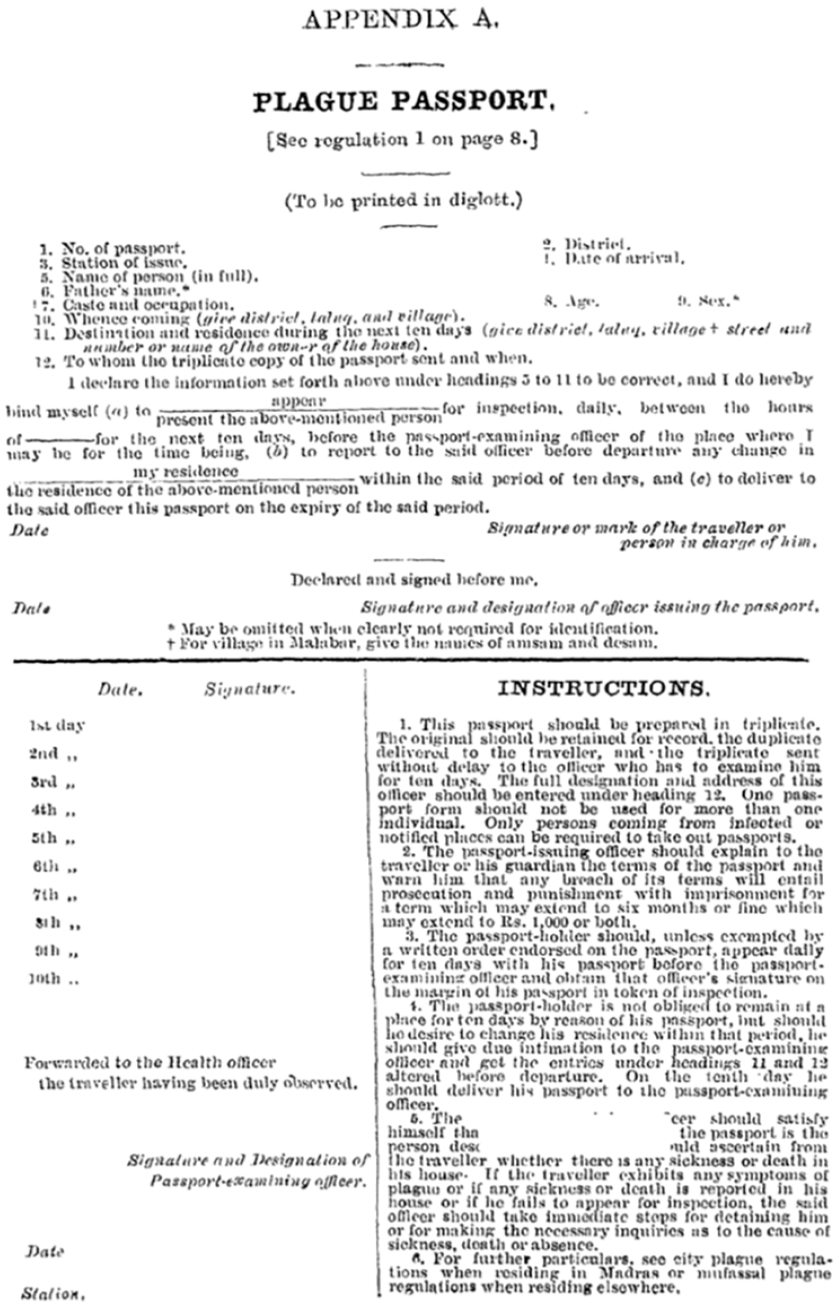
Example of the plague passport.
The Madras Chamber of Commerce, a body representing major industrialists in the city, was among the fierce advocates of the stringent plague regulations and the protection they provided accounted for the “remarkable immunity” that Madras had enjoyed. It vigorously backed the measures and argued that the expenditure on them was justified and necessary. For the Madras Chamber of Commerce, the circulation of money and the continuing of trade had been possible due to the stringent measures that the city government had imposed. For J. P. Bedford, the author a report on the plague administration of Madras, the Chamber’s approval proved the “sagacity” and “success of Plague Policy,” and no higher praise could be sought. 69 For Bedford, explanations that foregrounded the city’s “natural immunity” were misplaced. He suggested that in his long tour around the Presidency and Madras city, there was no verbal support for the explanation that climatic factors had saved Madras city from the plague. 70 The sanitarian framework received anecdotal support. One K. R. G. Aiyar, who lived for a lengthy time in Madras, wrote in 1920 that in comparison, the town of Belgaum was filthy. During the years of the plague, he never saw a sanitary inspector in sight, whereas in Madras, sanitary staff were working “all day” to eliminate plague cases. 71
In addition to the strong preventive measures that the sanitary commissioner King and others argued were responsible for prevention of plague, King identified the social geography and hierarchy of society in Madras city as an important reason as to why the plague did not affect the city. King argued that the plague rules he had set out for Madras were fully compatible with “caste rules.” 72 For King, the inhabitants of Bombay had not fully understood this confluence between plague rules and caste rules. In a convocation lecture delivered at Madras University (the longest recorded one), King set out the aim of the rules. King argued that the plague rules were not to disrupt caste rules, but secure “the complete union of all castes and creeds in aid of the strenuous efforts to prevent mortality and the destruction of trade.” There was huge confidence in the corporation, according to King, that the sanitary measures set out by government, and the cooperation of population, would together get the better of the plague. In proving his point, King read from Shasthras, showing how Hindus in ancient India supposedly dealt with the plague. The rapid evacuation of houses and subsequent segregation of the infected population was the precise way in which the Madras government and the Ancient Hindus both had intervened to prevent the plague. Commenting on an extract from the Bhagavatha Purana, King said:
the recognition (in this extract) of the dying rats as a sign of the danger of infection disposes of any possibility of the disease referred to being other than plague. The term Mahamari is used to this day as designating the disease in Gharwal, where, as you are doubtless aware, plague has from time immemorial been endemic. This injection to evacuate the ordinary houses of residence so completely as to involve removal of relations, friends, and servants and to resort to clean ground that has never been lived upon by human beings and not to return to the infected house till lapse of time and special processes for its purification have rendered it safe, represents literally the whole policy of the various regulations issued by each local government in reference to plague-infected villages. Even the modern modes of disinfection in this disease are strictly in accordance with the Shastras for inanimate objects, viz., for the flooring of houses, scraping and burning; for disinfection of buildings, free exposure to sun and win; and other objects, dry heat or hot water and chemicals, which are alkalis and acids. 73
Here, King was posing caste as an alibi and ally for plague rules. The Shastras, which explicate rules for ritual purity, embedded in a caste hierarchy, according to King, were ideal to repel the plague from homes. 74 In the lecture, he argued that the Shastras were compatible with purity and purification. In other words, particularly in a lecture hall that was predominantly Brahmin, King attempted to credit Brahminical exclusionary and regulatory frameworks (e.g., not allowing people from lowered castes to enter homes or use the same vessel to consume food) as the reason why plague did not spread.
The compatibility of ancient texts, such as the Shastras with plague rules was in direct opposition to what nationalists in cities, such as Bombay suggested. In Bombay, plague rules were an infringement of the “inner,” or the colonial state quarantining individuals and entering the space of the native home that led to the plague’s association with nationalistic sentiment. 75 This speaks more broadly to why King’s idea that Madras was adhering to caste rules as plague rules was a key reason as to why the city was not affected. First, King was attempting to use the plague to re-read colonial modernity through upper-caste Hindu traditions. Second, King was playing to the audience he was addressing. The university audience was largely upper caste, and the plague was perhaps a way to consolidate power among his audiences. Here, King was able to mobilize rhetoric around the successful prevention of plague to consolidate his position among the caste elites in the city. The rhetoric around the absence of diseases, such as plague in effect, consolidated caste as a category and power, whether through upper-caste rebellion or governmental rules supposedly coinciding with appropriate behavior.
Alongside, epidemiologists conducted investigations into the city’s so-called immunity. T.S. Ross, writing in the Indian Medical Gazette in 1906, argued that “The real solution of the question of our immunity from plague is, I believe, intimately bound up with the habits of our rat population.” 76 In Latin terms, the house rat in Madras was the Mus Rattus, and the street rat was the Nescocia Banch’cota, or in lay parlance the Bandicoot. The Madras rat, argued Ross, is a non-burrowing rat. In other words, it lived in the human house, unable to survive effectively on the streets. The Mus Rattus made its home behind furniture, in roofs, behind large bags, and “stays as a rule in the house to which he belongs.” According to Ross, the house rat lived in “mortal terror” of the bandicoot, which was a large and “ferocious beast.” Therefore, rats of each house could be treated as separate communities who did not necessarily interact with rats in the next house. For Ross, this was the underlying explanation of why the plague did not spread from house to house, and rather remained confined to a single house. 77
Ross’ evidence was from the way in which plague had spread in Madras. Largely, the rats had remained confined to a single area, and had not moved about. Furthermore, it was only in huts that rats had moved from one house to another. This too, it was only when the rats were chased by exterminators, or houses evacuated and disinfected, that rats ran from one abode to another. 78 For Ross, had the Madras rat, like those in Bombay, been living extensively in sewers and pipes across the city, the plague outbreak would have been similar to that in other cities. Ross pointed to newspapers reports about the Madras bandicoot. One report suggested that Madras owed more to the bandicoot than all the plague measures (the Rules and Regulations) put together, and this to Ross was hardly a “frivolous” explanation. 79 On the other hand, the bandicoot remained free of plague. Those bandicoots that were caught in proximity to the plague-infected rats were tested, and they had so far remained plague-free. Again, Ross suggested that this was due to the behavior of the bandicoot, rather than its innate immunity against plague. Each bandicoot family had its separate burrow, often in large gardens, which minimized their chances of being infected. 80 Despite his theory surrounding the bandicoot, Ross reverted to rat extermination as the ideal way of keeping plague cases low in the city. 81
However, investigations from the Plague Research Committee, published in the Journal of Hygiene suggested otherwise.
82
The authors suggested that The presence of the bandicoot in such large numbers has been offered as an explanation of this [absence of plague] fact. It is difficult to believe that people who have propounded Such a theory can have made a study of the habits of the bandicoot.
83
Studying the bandicoot in the lab, made all the difference for this investigation. The Bandicoot, described as “ferocious” by Ross in the field, was seen as an innocent animal in the lab. The Mus Rattus was living in cages with the bandicoots for a long period of time, and not in a single instance, the study argued, had the bandicoot attacked the rat. 84 There was further complexity in the bandicoot theory. In the investigations of the epidemiologists, inhabitants of the native parts of the city stated that bandicoots frequently came into the house, especially at night, and that people were disturbed by their clumsiness. However, the traps laid out in the houses failed to capture many bandicoots. The study thereby concluded that “the invasion of dwelling houses with bandicoots (at any rate young ones) is an uncommon event.” 85 In other words, there was a question as to whether the bandicoot could have been the carrier of plague, and indeed if it was, did it actually enter dwellings. What emerges, therefore, is differences in how the bandicoot was conceived was a carrier of plague between the lab, field, and public narrative.
Colonial reports and newspaper commentary continually remarked that the conditions for plague were rife in Madras city, and yet it did not catch on. Not many were convinced with the explanation that Madras during the early years of the plague in India was “naturally” immune. However, a later detailed investigation published in 1912 in the Journal of Hygiene grounded the most likely explanation as to why the city did not suffer from plague in the urban environment. More specifically, the article argued that the rat flea could not survive in the cooler climactic conditions of Madras city, as well as it did in large parts of colonial India. The environmental explanation has been accepted even in contemporary studies. Chinmay Tumbe, in a comprehensive survey of the plague across India, writes In the south, the Madras Presidency was left relatively unscathed by the plague, though the districts of Bellary, Coimbatore and Salem did occasionally see outbreaks, predominantly in urban areas . . . The prevalence and behaviour of the rat flea, as later research confirmed, saved the bulk of south and east India from plague.
86
The rat-flea theory, or the explanation of plague immunity through climate emerged post 1910. 87 Even the housing and layout of Madras city was linked with the relative low prevalence of plague. As the article in the Journal of Hygiene argued “It [Madras] is quite unlike the other presidency towns of India and can best be described as a collection of small towns and villages separated one from the other by considerable tracts of open country.” What didn’t fully fit this narrative was that certain parts of the city, such as Chintadripetta, Triplicane, and Georgetown (the seat of British government), were densely populated with housing settlements closely situated near one another, very similar to cities, such as Bombay and Calcutta. 88 From the viewpoint of rats, the article argued that the “poorer houses” afforded them “unlimited shelter.” Rats were everywhere during the investigation, and indeed, as the article concluded, they could thrive in large portions of the town. The city’s immunity from plague could therefore not be put down to an unfriendliness to rats. 89
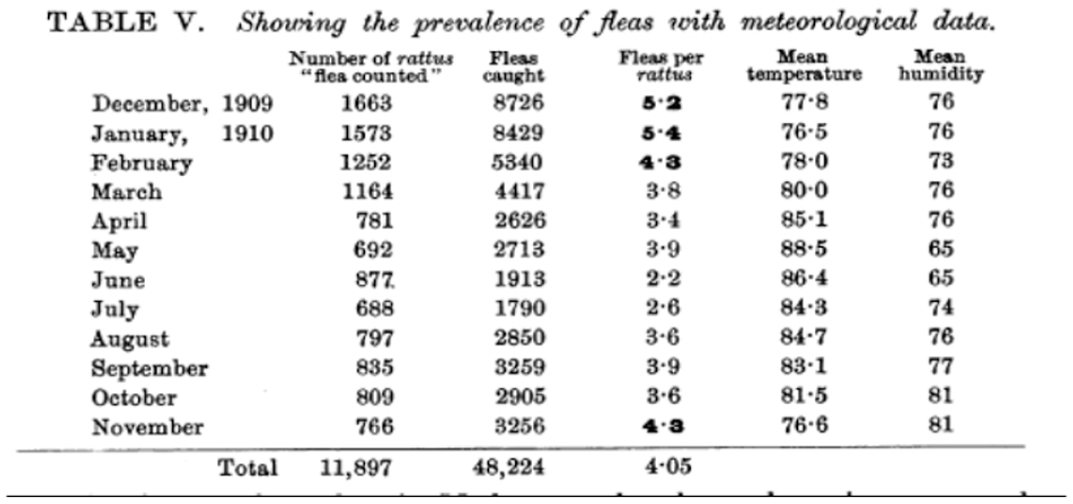
The government investigation on the Madras plague, conducted between 1905 and 1912, examined the relationship between the climatic condition of Madras city and the rat flea in detail. While the rat was a disease reservoir, the flea, it was by now established, was the main disease vector.
The figures show that in Madras as elsewhere there is a seasonal variation in the abundance of rat fleas. X cheopis was most abundant in December and January while only about half as many were found in the hot dry weather in June and July.
This range was not uncommon in most cities affected by the plague. What was different about Madras in case of the number of fleas, was that while the minimum figure was very much the same (around fleas per two to three rats), the maximum figure differed. There were a maximum of only five fleas per rat during the height of the plague season in Madras city, in November and December. In other cities, the number was far higher. For instance, it was nineteen fleas in Belgaum, twelve in Dhand, nine in Poona, thirteen in Lucknow, eighteen in Cawnpore, and up to fourteen in Bombay. 90 Even for the commission, the rat-flea theory did not fully add up. Experiments had shown that the flea survived far better in cool moist conditions as opposed to hot dry air. However, in the colder months of November and December, the flea could live for a considerable time. 91 The commission, which also found that rats in Madras were extremely susceptible to the plague, only offered tentative conclusions. They stopped short of putting forth a scientifically proven claim of climatic conditions, and instead resorted to stating that Madras has escaped the plague “because infection has been unable to reach there or has met with some obstruction immediately after its arrival.” 92 J. Taylor, who was part of the plague research commission appointed by the Madras government, finished a thesis on the plague in Madras for an MD at Glasgow University in 1913. For Taylor similarly, temperature and climatic conditions was a key correlation to plague rates (Figure 3). But even as Taylor admitted, this did not explain why Rangoon and Bombay had suffered the plague, while Madras escaped it. 93
Map showing temperature and climactic conditions in relation to plague case density.
A subsequent paper published from the Plague Research Commission’s investigations in 1915, repeated this uncertainty. The paper, published in the Journal of Hygiene, again pointed out that Rangoon, where the plague did settle in, had a similar climate to Madras. Bombay, while cooler from in February and March, had a very similar temperature in the months of November and December. 94 Therefore, there was no question of the city possessing “natural” immunity. Furthermore, considering the susceptibility of the rat to plague, even the low number of fleas would have been sufficient for an outbreak. 95 In reviewing the evidence, this paper suggested that it had to be concluded that the plague had “failed to reach Madras city,” despite its road and rail links to nearby Bangalore, which was badly affected. 96
In 1916, far after the worst effects of the plague had passed colonial India, as detailed in the first section of this article, Madras city suffered its worst plague outbreak. The narrative of the outbreak is detailed, but produces further questions. There is subsequently a detailed narrative about every arrival: Kannapan, for instance, arrived with his mother and two brothers from Poona, on September 24. He had an enlarged gland in the left axilla, described as “very tender and painful.” A young girl, ten years old, Ram Bai, who arrived from Raichur, developed bubo in the right axilla—the plague bacilli was found in the bubos.
97
There were other cases—one deceased Thyagarajan came down from Secunderabad with his mother Kuppamal and brother Damodaram on Wednesday via the Bezwada express. Fever was extremely high, but there was absence of cough, septum, diarrhea, and buboes. His mother said they were inoculated at Secunderabad a month ago, but no certificate could be produced.
98
This could have even been the first onset of the influenza pandemic, which ranged from 1916 to 1918, but passed off as the plague. The corporation report for 1916 commented that Madras city offers every facility for an outbreak of plague, in case infection is once introduced. Bubonic plague is not communicated from man-to man without the transmission of the rat, in the case of pneumonic plague, the infection could be contracted with coming into proximity to the sick.
99
Yet, for a city that had suffered its worst outbreak in 1916, no further investigation was conducted and indeed the 1916 outbreak did not find mention in a major report published on mortality statistics and diseases that affected the city most in 1927. The lack of interest can, at least partially, be ascribed to the decline of the plague as an epidemic at the scale of the colony and indeed the empire (Figures 3 and 4).
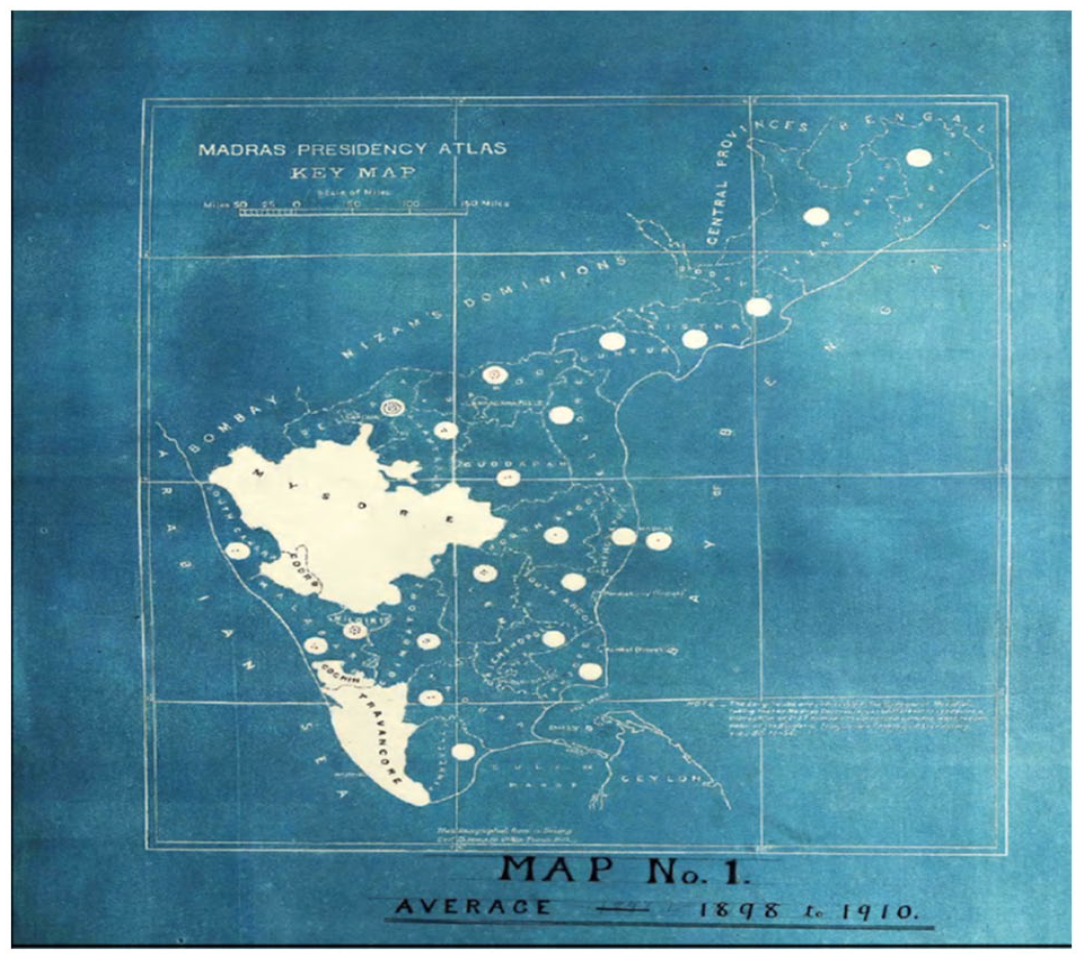
Table showing the prevalence of fleas alongside meteorological data in Madras city.
Conclusion
This article argues that the plague brought into view Madras city’s particular range of environments, government structures, physical infrastructures, and non-humans as a result of the plague’s absence, rather than the devastation it caused in other colonial cities and tropical environments. In the case of Bombay and Calcutta, insanitary environments, dirt, and poor housing were routinely blamed for the spread of the plague, associating tropics with disease in a singular frame. 100 Yet what puzzled colonial medics and sanitary officials was that a city, in this case, Madras with similar kinds of perceived insanitary environments, hardly felt such effects. Ultimately, the immune city of Madras challenged constructions of colonial urban environments as inherently diseased. Simultaneously, the absence of the plague allowed for reification of urban caste geographies.
Subsequently, as a result of the plague, cities, such as Bombay, Calcutta, and Bangalore were planned afresh following the epidemic. 101 Entire neighborhoods were razed and the provincial government setup improvement trusts in each of these cities. In Madras, however, no such response was forthcoming. Rather, the plague, while present in fits and starts, did not accumulate the currency in influencing urban planning as it did in other contexts. While the urban planning trajectories of cities, such as Bombay, Bangalore, and Calcutta were deeply influenced by the plague, with improvement trusts and extensions introduced, the plague was not the mover of urban planning in Madras. 102 For instance, Bombay created an improvement trust in 1899 and Calcutta soon after in 1911. 103 Rather, alongside water supply and drainage, town-planning in Madras was introduced only in the 1920s, as a province wide intervention, rather than a monumental urban upheaval following the plague.
Furthermore, there was a clear difference between lab and field, in investigating and thereby constituting the various aspects of Madras city’s vulnerability and immunity to the plague. The lab suggested, quite clearly, that Madras was ripe, as a well-connected port city, with a similar climate to Bombay, for a plague outbreak. Yet the actual happenings, and field investigations and observations in the urban suggested differently. This dissonance between lab and field persisted in various explanatory theories on the plague. On climatic conditions, for instance, lab investigations that compared the temperature, humidity, and rainfall in various cities, concluded that Madras, like Bombay and Rangoon, was ripe for affliction with the plague. Similarly, in the case of the Madras rat, investigations in the lab showed that the bandicoot and the rat could co-exist, and indeed the rat was hardly fearful of bandicoots. Yet, in the field, observers reported otherwise. This struggle, to reconcile the lab and field, was then supplanted on to explanations that favored the sanitary framework. Either the plague could not reach Madras, or was stopped in its tracks. As Lynteris argues, “Not precisely knowing what one did not know about the . . . plague became both a significant driver of scientific research and, as the case of India makes particularly clear, a fertile field for applied experiments . . ..” 104 In Lynteris’ case, the “field” was soil, and it resulted in direct outcomes on the urban environment due to its urgency. In the case of this article, the “field” was the city, its infrastructures, social geographies, climatic conditions, behavior of non-humans and specific sanitary frameworks.
Footnotes
Acknowledgements
The author is grateful to Pratik Chakrabarti and Christos Lynteris for reading drafts of this article, especially with their expertise on medical history. Audiences at various seminars, including at Shiv Nadar University and the University of Manchester sharpened arguments the author has made here.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author is also grateful for funding from the British Academy (grant no. SG2122\210708) for travel to archives.