
Abstract
Black men remain severely underrepresented in the mental health workforce. This study explored how sociocultural and racialized barriers influence their motivations to pursue mental health careers and the challenges they encounter. Using purposive sampling, we conducted in-depth, semi-structured interviews with 34 self-identified Black men working in counseling, social work, or psychology. They represented various stages of professional training and licensure across these mental health fields. Guided by critical race theory and social cognitive career theory, data were analyzed using reflexive thematic analysis; two core categories and four themes were identified. Within the Motivation category, Purpose and Support emerged as key motivators, reflecting personal fulfillment, community responsibility, and mentorship. The second category, Barriers, included the themes of Stigma and Systemic Inequalities, encompassing cultural norms around masculinity, financial hardship, biased licensure, and limited early exposure to the field. Despite these challenges, participants expressed a strong commitment to improving access and representation. The findings support the need for targeted recruitment strategies, structural reforms, and culturally grounded career pathways.
Despite longstanding diversity efforts, Black men remain one of the most underrepresented groups in the mental health profession. As of 2022, they comprise just 3% of psychologists, a 2% increase from 2011 (American Psychological Association, 2022). This underrepresentation extends across related fields: Black men account for only 8% of Black social workers with a master’s degree and 1.6% of psychology doctoral students (American Psychological Association, 2023; George Washington University Health Workforce Institute, 2019; Salsberg et al., 2020). Furthermore, they represent just 5.1% of enrollees in counselor education programs (Council for Accreditation of Counseling and Related Educational Programs, 2023).
These disparities reflect deeper structural inequities that limit access to culturally responsive care in Black communities. The shortage of Black male mental health professionals creates a disconnect between client needs and available services. Historical racism, unethical medical practices, and exclusion from research have fueled mistrust toward mental health systems among Black individuals (Boulware et al., 2003; Gaston et al., 2016). Clients often prefer therapists who share their racial background, as this builds trust and cultural understanding (Goode-Cross & Grim, 2016). However, the shortage of Black providers, particularly men, limits the likelihood of these connections and contributes to gaps in service utilization and outcomes.
Although recent diversity and equity initiatives have gained traction, many have failed to adequately address the specific challenges faced by Black men entering the mental health profession. These efforts are often overly generalized, treating racial and gender diversity as interchangeable categories and overlooking the intersectional barriers faced by Black men (Bell, 2018; Bonner et al., 2021). Consequently, Black men remain significantly underrepresented in both the mental health workforce and in the institutional and scholarly efforts aimed at addressing workforce inequities. Broad diversity initiatives without intentional and targeted strategies risk reinforcing existing disparities rather than correcting them (Beasley et al., 2015; Bonner et al., 2021).
Research on Black men’s experiences in the mental health field remains limited. Existing studies often generalize across race or gender or center women’s experiences, overlooking how Black men navigate educational and professional pathways (Beasley et al., 2015). Few studies have explored the influence of their intersecting identities, cultural values, and histories on career decisions and persistence in psychology, social work, and related fields (Beasley et al., 2024). The dearth of research limits the development of culturally informed recruitment and retention strategies.
To address this gap, we explore how Black men perceive and respond to the barriers they encounter in entering the mental health profession. Using a qualitative approach, grounded in critical race theory (CRT) and social cognitive career theory (SCCT), we aim to center the voices of Black men and provide insight into their experiences, motivations, and challenges.
Literature Review
Understanding representation in the mental health workforce is essential to addressing disparities in access, quality of care, and culturally responsive practice. Within this broader conversation, Black men remain uniquely underrepresented across psychology, counseling, and social work (Beasley & Hernandez, 2025). This underrepresentation cannot be viewed in isolation; rather, their experiences are shaped by intersecting challenges related to race, gender, and systemic exclusion, impacting both entry into and advancement within the field (Beasley et al., 2015).
Theoretical Framework
CRT and SCCT offer complementary frameworks to examine the career development of Black men in the mental health profession. CRT highlights how racism is embedded in institutions, creating structural barriers that limit access and advancement (Delgado & Stefancic, 2001; McGee & Stovall, 2015). SCCT emphasizes how self-efficacy, outcome expectations, and personal goals are shaped by sociocultural context and external barriers such as limited mentorship (Lent et al., 1994). CRT’s focus on counter-storytelling also foregrounds lived experiences, revealing how racialized realities influence perceptions of opportunity and exclusion.
Historical Context and Systematic Mistrust
To ground these theoretical perspectives in lived realities, it is important to examine the historical and systemic forces that have shaped Black men’s exclusion from the mental health profession. Racism in medicine and psychology has long pathologized Black experience, as seen in the 19th-century diagnosis of drapetomania, which framed enslaved Africans’ desire for freedom as mental illness (Willoughby, 2018). The Tuskegee Syphilis Study further fueled cultural mistrust by intentionally denying treatment to Black men (Toldson & Toldson, 2001). These historical harms continue to shape perceptions of the mental health field today. While institutions such as the American Psychological Association have acknowledged past injustices, recent rollbacks of diversity initiatives raise doubts regarding the profession’s sustained commitment to racial equity (American Psychological Association, 2021; Riddle, 2025). Cultural mistrust remains high, driven by concerns about misdiagnosis, lack of cultural competence, and the lingering impact of exploitative care (Boulware et al., 2003).
In the face of these systemic barriers, Black men often rely on high-effort coping mechanisms to navigate exclusion. John Henryism, a coping strategy characterized by relentless perseverance in the face of adversity, offers insight into how Black men persist in fields like mental health. While it may reflect strength and resilience, it is also associated with increased psychological strain, depressive symptoms, and reduced help-seeking owing to internalized stigma and masculine role expectations (Cadaret & Speight, 2018; Hudson et al., 2016; James et al., 1983). Thus, the decision to enter and remain in the mental health profession may come at a significant cost to well-being.
Stereotypes, Masculinity, and Stigma
In addition to historical and systemic factors, cultural beliefs about masculinity and mental health shape the underrepresentation of Black men in the field. Mental illness is often stigmatized in Black communities, with help-seeking seen as a weakness or spiritual failure (Coleman-Kirumba et al., 2023; Taylor & Kuo, 2019). These beliefs clash with dominant ideals of masculinity, which emphasize stoicism and emotional restraint. As a result, mental health work rooted in empathy and vulnerability can feel incompatible with cultural expectations of manhood (Donaldson, 1993).
Additionally, Black men must navigate harmful societal stereotypes that compound these internalized beliefs. Hines et al. (2021) found that Black boys are often subjected to early adultification and criminalization, experiences that strip them of emotional innocence and reinforce the need to be hypermasculine as a means of protection. Racial microaggressions and implicit bias, such as assumptions of aggression or intellectual inferiority, are common experiences that reinforce this dynamic (Sue et al., 2007). These experiences create both internal and external barriers to entering a field where emotional expression and vulnerability are central.
Educational and Structural Barriers
While cultural stigma plays a role in Black men’s underrepresentation, structural barriers within the education system are equally significant. Early challenges in K–12, such as disproportionate discipline and a lack of Black male educators, hinder engagement and access to role models (Bell, 2020; Jeter & Melendez, 2022). These barriers persist in higher education, where they face underrepresentation in graduate programs, limited mentorship, and weak institutional support (Brooks et al., 2024). Disparities in licensure exam pass rates further reflect systemic inequities, driven by unequal preparation resources, cultural bias in testing, and broader educational disadvantages (Association of Social Work Boards, 2022). These barriers delay licensure, restrict career mobility, and reinforce racial gaps in the mental health workforce.
Economic factors compound academic and institutional obstacles. Financial challenges, including student debt and limited intergenerational wealth, further influence career decision-making, particularly for professions requiring advanced education but offering delayed financial return (Houle & Addo, 2018). The intersection of educational disparities and financial burden creates a systemic disadvantage, reinforcing the structural exclusion of Black men from the mental health profession (Houle & Addo, 2018). Taken together, these factors emphasize the need to examine how educational and economic structures shape access to and representation within the mental health workforce.
Motivations for Pursuing Mental Health Careers
Despite systemic and educational barriers, many Black men are motivated to pursue mental health careers because of their personal experiences, cultural identity, and a commitment to community. Their decisions are often shaped by trauma, loss, or exposure to therapy, which inspire a desire to help others access the support they once needed. This motivation reflects what Beasley and Hernandez (2025) call a “gendered racial equity ethic,” where professional goals are tied to racial uplift and social justice.
Cultural representation and visibility are equally important within the profession, providing both inspiration and affirmation. The absence of culturally responsive care often compels Black men to serve as the representation they once lacked (Byars-Winston, 2010). For many, this profession is not just a career choice but a calling rooted in purpose, resilience, and a legacy of service to their communities (Beasley et al., 2015).
The Role of Mentorship
While intrinsic motivation often sparks interest in mental health careers, mentorship provides the external support to sustain it. Mentorship helps Black men navigate systemic barriers, affirm their identities, and build professional confidence, especially in predominantly White settings (Beasley et al., 2021; Chandler, 2011). Positive relationships with culturally similar mentors foster a sense of belonging and motivate entry into the field. Research shows that mentorship mitigates the effects of racial discrimination, supports identity development, and enhances academic and professional readiness (Hannon et al., 2024). By offering guidance and modeling success, mentorship plays a critical role in empowering Black men in the mental health profession.
Purpose of the Study
Despite growing literature on diversity in counseling and psychology, a significant gap remains in research specifically examining Black men’s pathways into the mental health profession. Although some studies have explored the experiences of Black individuals in the counseling profession (Hannon et al., 2024) and doctoral psychology programs (Beasley & Hernandez, 2025), few have examined why Black men pursue mental health careers more broadly. This lack of specificity limits understanding of the racialized and gendered experiences shaping their decisions. Addressing this gap, we explore the motivations and challenges that influence Black men’s entry into the mental health field. Guided by CRT and SCCT, we examine how structural inequities, self-efficacy, and identity formation impact access and persistence. Accordingly, this study is guided by the following research question: • How do sociocultural and racialized barriers shape Black men’s motivations to pursue mental health careers, and what factors deter them from entering or advancing in the field?
Method
Study Design
To address this research question, the study employed a qualitative phenomenological design to explore the lived experiences of Black men pursuing careers in the mental health field. A phenomenological framework was used to capture participants’ subjective meanings and the essence of their experiences as they navigated educational, professional, and sociocultural barriers (Moustakas, 1994). Data were analyzed using reflexive thematic analysis, which facilitated an iterative and interpretive process of identifying patterns across narratives while maintaining fidelity to participants’ lived realities (Braun & Clarke, 2021).
Participants
Guided by this design, participants were recruited to capture a diverse range of perspectives from Black men working or training in the mental health field. The sample comprised 34 self-identified Black men with backgrounds in social work, counseling, psychology, or related mental health fields. Participants ranged in age from 26 to 66 years, with an average age of 43.5 years. The majority of the sample (n = 26) held a master’s degree in social work, counseling, or clinical mental health counseling. A smaller subset had obtained doctoral-level training, including five participants with PhDs in Rehabilitation Counseling, Community Psychology, or Counselor Education. One participant had a Doctorate in Social Work and another held a PsyD in Clinical Psychology.
With regard to licensure, six participants were Licensed Clinical Social Workers (LCSWs), six were Licensed Professional Counselors (LPCs), and six were Licensed Social Workers (LSWs). Additionally, there was one Licensed Clinical Psychologist and one Licensed School Counselor. Two participants were pursuing a Master’s in Social Work at the time of the study. Fourteen participants did not hold any professional licensure.
Participants’ Education, Licensure, and Age (N = 34)
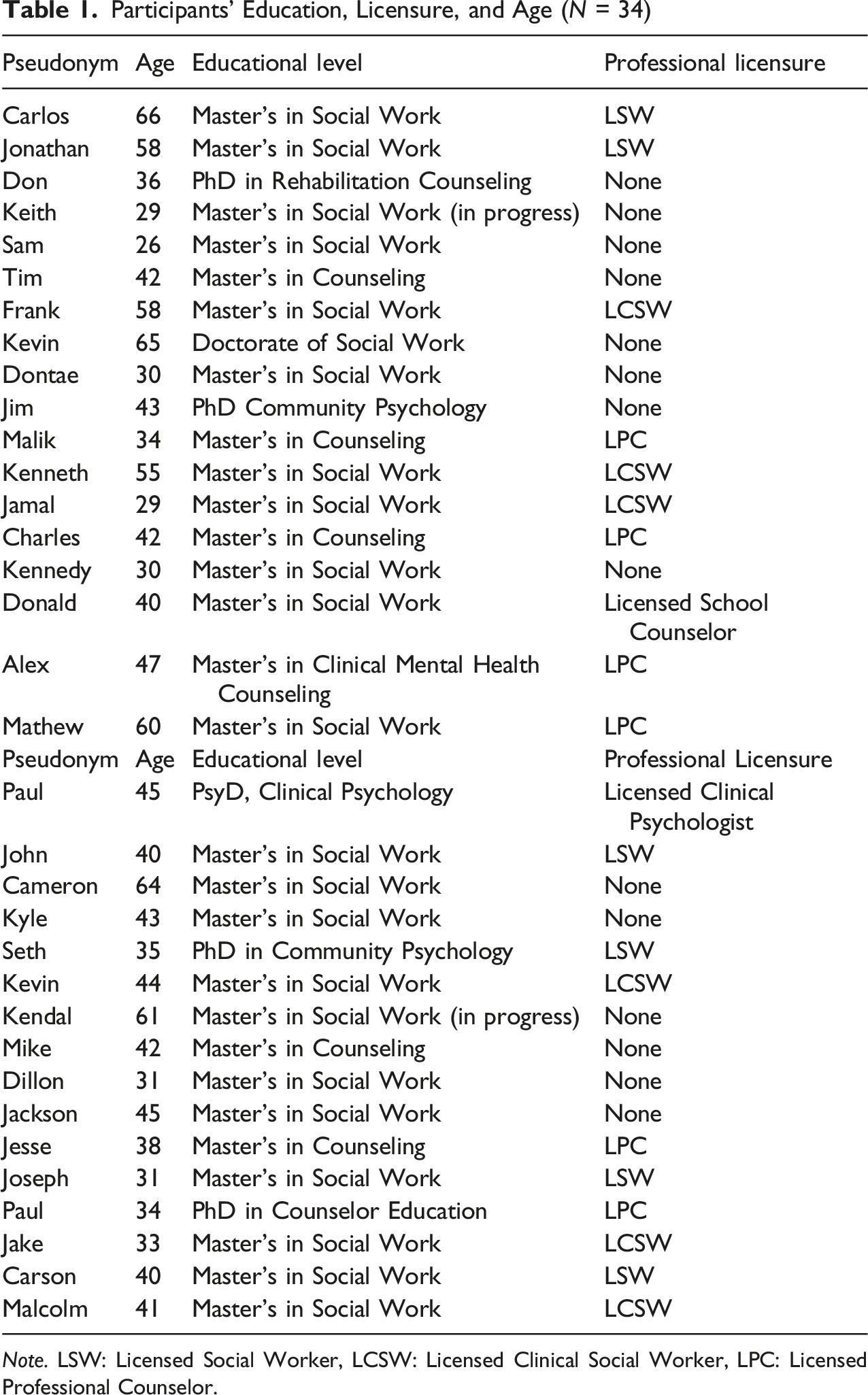
Note. LSW: Licensed Social Worker, LCSW: Licensed Clinical Social Worker, LPC: Licensed Professional Counselor.
Positionality
In addition to considering participants’ diverse experiences, it was also important to reflect on the researchers’ identities and how they may have influenced data collection and interpretation. Following qualitative research practices (Grzanka & Moradi, 2021), the authors reflected on how their identities shaped the research process. The first author is a Black male, LCSW, and PhD student in Criminology with over a decade of experience counseling Black boys and men. The second author is a Nigerian female Master of Social Work student, whose cross-cultural perspective informed understandings of equity and representation. The third author is a Black male LPCC and PhD student in Counselor Education. To manage bias, the team used analytic memos, met weekly to discuss coding, and engaged in investigator triangulation to ensure findings reflected participants’ perspectives (Fusch et al., 2018).
Procedure
Building on this reflexive awareness, the following procedures were implemented to ensure methodological rigor and transparency throughout data collection. Before initiating any recruitment activities, approval was obtained from the Institutional Review Board (IRB) of the first author’s university. Once IRB approval was granted, targeted marketing was conducted on LinkedIn to recruit Black male mental health professionals for the study. Additionally, participants were recruited directly from local community mental health centers in the Midwest region.
The study employed semi-structured interviews guided by a 20-question protocol grounded in CRT and SCCT. Interviews, lasting approximately 50 minutes, were conducted virtually via Zoom, audio-recorded with participant consent, transcribed verbatim, and coded using NVivo software. To protect confidentiality, all participants were assigned pseudonyms in the documentation and reporting. All data were stored on a secure server within the first author’s university network, which is protected by institutional firewalls and access controls to ensure data confidentiality and integrity.
The interview protocol addressed the central research question, focusing on career entry, training experiences, and long-term goals. Sample questions included: (1) “Why did you choose the mental health field?” (2) “Did school prepare you to work with diverse groups?” and (3) “How do your race and gender influence your career goals?”
The interview guide was piloted with a small group of participants to ensure clarity and thematic relevance. All participants were asked the same key questions, in a varied order to accommodate conversational flow. The codebook used for analysis was developed by the first author and closely aligned with the interview protocol and theoretical framework.
Purposive sampling was employed to intentionally recruit participants who could provide relevant insights regarding the study’s research question (Tongco, 2007). This method involves selecting participants based on the researcher’s judgment of who can best contribute to the study (Tongco, 2007). Eligibility criteria required participants to identify as Black men, be employed within a mental health setting, and hold a master’s degree in a relevant mental health discipline (e.g., counseling, social work, and psychology) or be currently enrolled in such a program. Data collection continued until thematic saturation was achieved, a point at which no new themes or insights emerged (Gill, 2020). Saturation was assessed iteratively through ongoing evaluation of the redundancy and depth of participant responses, consistent with qualitative research best practices (Gill, 2020).
Data Analysis
Following data collection, a systematic analytic process was undertaken to interpret participants’ narratives and identify recurring patterns of meaning. Reflexive thematic analysis (Braun & Clarke, 2021) was used to examine Black men’s motivations, barriers, and career pathways in mental health. This approach supported critical engagement with the data, honored participants’ lived experiences, and accounted for researcher positionality, particularly that of the first and third authors as scholars and practitioners of color (Byrne, 2022). It also enabled the interpretation of key patterns in how Black men navigate structural and personal challenges in pursuing mental health careers.
Data analysis followed the six phases of reflexive thematic analysis as outlined by Braun and Clarke (2021): (1) data familiarization, (2) initial coding, (3) generating preliminary themes, (4) developing and reviewing themes, (5) refining and defining themes, and (6) producing the report. The authors began by immersing themselves in the transcripts through repeated readings. During initial coding, each author independently identified patterns related to participants’ lived experiences, such as financial barriers, mentorship, and cultural stigma. These codes informed the generation of preliminary themes. The team met regularly over three weeks to review, consolidate, and refine themes. They also reflected on how the study’s theoretical frameworks shaped the interpretation and meaning assigned to each theme during analysis and reporting.
Early in the analysis, participants consistently framed their motivations and challenges through the lens of racialized experience and community responsibility. While guided by CRT (Delgado & Stefancic, 2017) and SCCT (Lent et al., 1994), coding revealed how intersecting identities as Black men influenced participants’ desire to counter systemic exclusion in mental health. Rather than isolating individual goals, participants linked their career paths to broader issues such as underrepresentation, cultural mistrust, and the need for healing in their communities. These insights informed the refinement of themes and highlighted the impact of systemic barriers and cultural purpose on their vocational decisions.
Thematic analysis was conducted using an inductive approach, allowing patterns and meanings to emerge directly from the data (Braun & Clarke, 2021; Braun et al., 2022). The team developed and refined a codebook based on recurring concepts identified through repeated transcript reviews. Multiple rounds of coding and discussion helped ensure consistency and depth, while attention to contradictions preserved the complexity of participant experiences. Final themes were confirmed collaboratively to ensure they accurately reflected the data.
Results
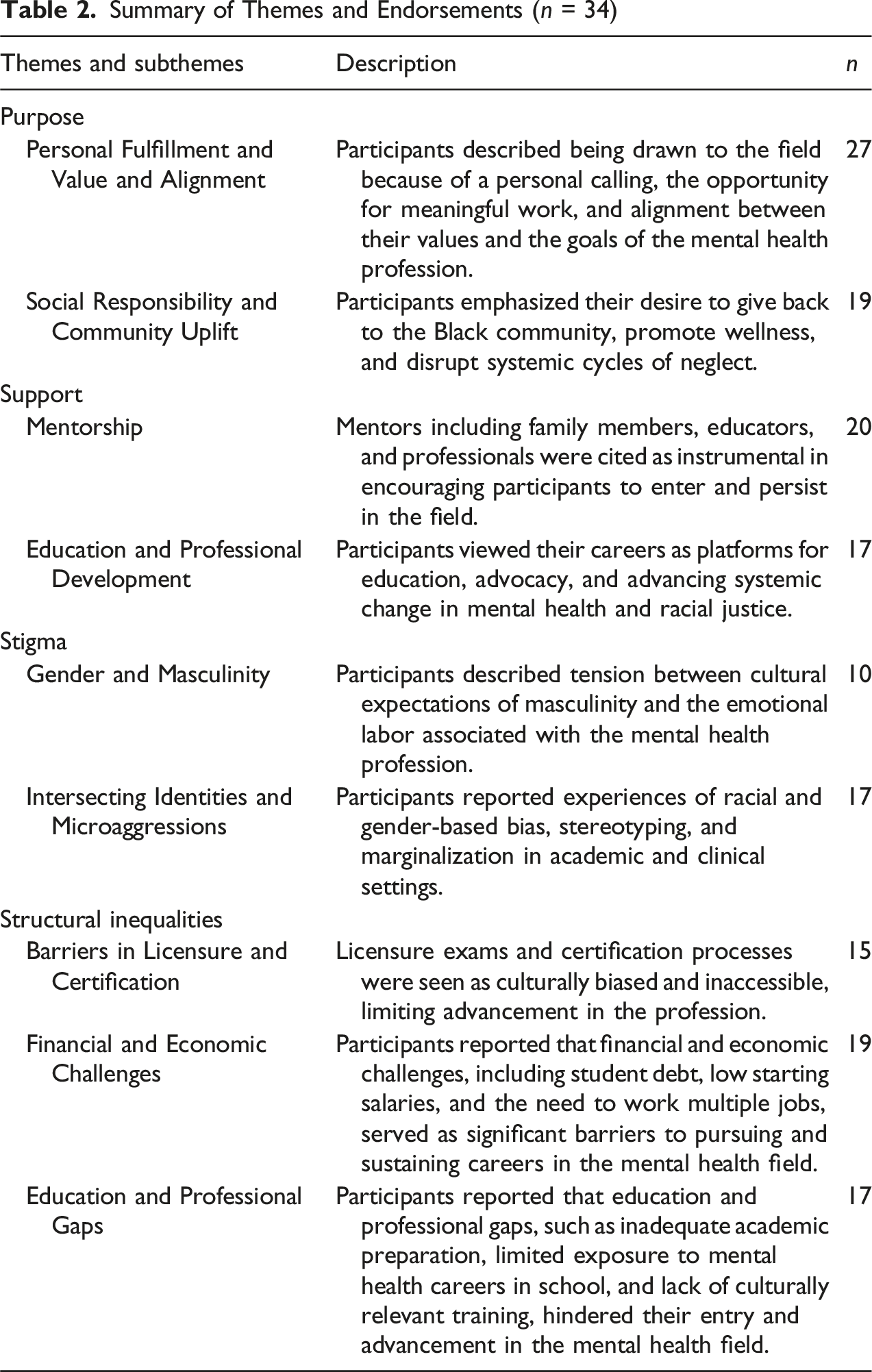
Summary of Themes and Endorsements (n = 34)
Motivation to Pursue Careers in Mental Health
The first analytic category, Motivations, captures the factors that inspired participants to enter the mental health profession. Two central themes emerged: Purpose and Support. Purpose reflected internal motivations such as personal fulfillment and a sense of social responsibility. Support encompassed external influences such as mentorship and access to educational and professional development. These themes illustrate how individual purpose and structural support intersect to motivate Black men to pursue careers in a field where they are underrepresented.
Purpose
Building on this broader understanding of motivation, Purpose emerged as a driving force that connected participants’ personal fulfillment with their commitment to social change through mental health work. The participants’ responses revealed a deep sense of alignment among their personal values and the mission of mental health work, as well as a commitment to serve their communities. This theme had two subthemes: (1) Personal Fulfillment and Value Alignment, reflecting participants’ internal motivations and desire for meaningful and identity-affirming work and (2) Social Responsibility and Community Uplift, highlighting their intention to address intergenerational trauma, promote healing, and give back to underserved communities.
Personal Fulfillment and Value Alignment
Many participants (n = 27) described a strong internal calling to engage in meaningful and emotionally rewarding work. Their decision to pursue a career in mental health was generally influenced by lived experiences with adversity, personal healing, or the mental health struggles of loved ones. For instance, Carlos described the gratification he felt from helping others: The fulfillment of working for a purpose outside of yourself it has a gratification to it, a unique gratification to it. It allows you to interact with so many others . . . to see wellness and the process from where they’ve started to where they are.
Carlos’s account reflects how outcome expectations, specifically the emotional reward of helping others, fueled his professional interest. His narrative aligns with SCCT as it illustrates how self-efficacy and meaningful work reinforce long-term career persistence (Lent et al., 1994).
Kevin shared how personal loss became a turning point in his career path: My older brother ended up taking his own life. So that kind of just really made me want to like, you know, actually, let me just focus and study, learn this stuff, and reach out and support people that are going through it.
This reflection reveals the interplay between personal trauma and professional transformation. Kevin’s decision to turn grief into purposeful action exemplifies SCCT’s emphasis on self-efficacy rooted in lived experience. His quote also engages CRT, highlighting how Black men navigate individual and collective trauma in the face of systemic failures in mental health care (Delgado & Stefancic, 2017; Gaston et al., 2016; Lent et al., 1994). Similarly, Jonathan emphasized a desire to leave a lasting impact: I want to make a difference in people's lives. That's the reason why I feel that if I could make an impact on one person's life on this earth before I leave. I know I did my duty.
Jonathan’s reflection underscores the existential drive many participants exhibited, viewing their work as more than a job, but a purpose. His narrative highlights the SCCT construct of personal goals and legacy, while also reflecting the CRT focus on counter-storytelling using lived experience to resist dehumanizing structures and to redefine what success means for Black men in historically exclusionary professions (Delgado & Stefancic, 2017; Lent et al., 1994).
Social Responsibility and Community Uplift
Beyond personal alignment, many participants (n = 19) described a collective ethic of care that guided their decision to enter the field. They viewed mental health work as a way to confront systemic racism, break generational cycles of trauma, and expand culturally competent care. Mathew, for example, grounded his career decision in shared experience and cultural empathy: I understand what these people go through because, growing up in Chicago, I saw similar struggles. It made me want to help in a way that resonates with their experiences.
Mathew’s words highlight how lived experience functions as a motivator for service, reinforcing SCCT’s emphasis on person–environment fit and demonstrating how identity alignment can shape career goals (Lent et al., 1994). Kyle described the broader social needs that drive his work: Living in high-poverty areas showed me how much mental health support is needed for healing and resilience.
Kyle’s reflection illustrates how systemic neglect inspires counteraction. His motivation reflects CRT’s focus on structural inequality and SCCT’s concept of outcome expectations, where exposure to community conditions directly informs a commitment to transformative practice.
Similarly, Alex, a licensed therapist and school counselor, framed his work as a response to stigma and a source of inspiration for others: So, for me, it was really about breaking that stigma. You know, Black men can open up. We can talk about our feelings, and there's benefits to doing that. I just saw within myself the need to play my role in society. That was one of the main reasons I wanted to get into mental health. I'm seeing the benefits, and I want to continue to spread that word and help Black men in particular. I think we need to do it more in our community. So I'm playing my role and hoping that others are inspired by what I do.
Alex’s statement embodies both the SCCT model of social learning and self-efficacy as he uses his own example to shape behavior and expectations and CRT’s critique of internalized racial narratives, particularly the stigma surrounding emotional vulnerability among Black men. His focus on community modeling and generational impact situates his work within a framework of resistance and healing (Delgado & Stefancic, 2017; Lent et al., 1994).
Across these responses, participants framed their professional paths not only as personally meaningful but also as part of a larger struggle for equity, healing, and visibility. Their decision to enter the field reflects a purposeful disruption of racialized barriers and a strategic effort to create culturally responsive mental health systems from within.
Support
While personal purpose provided the foundation for participants’ pursuit of mental health careers, their journeys were equally shaped by the social and structural supports that helped transform motivation into opportunity. Social support plays a crucial role in ensuring participants’ entry into the mental health field. Supportive relationships with mentors, educators, and role models provided both encouragement and direction, especially in the face of structural and cultural barriers. Two subthemes emerged: Mentorship, highlighting the impact of individuals who guided participants and provided affirmation, and Education and Professional Development, reflecting how academic and training environments supported access and growth. Collectively, these forms of support helped participants navigate underrepresentation and systemic inequities.
Mentorship
Mentorship, identified by 20 participants, played a critical role in shaping career paths. Mentors ranging from family members to professionals offered encouragement, validation, and access to opportunities, helping participants navigate a field where Black men remain underrepresented.
For many, mentorship began at home. Jesse reflected on how encouragement from his father and a trusted professional helped shape his path: I talked to my dad about it. He was like, maybe you should go into social work. So I talked to my social worker mentor about it, and he expressed that it would be a good fit for me.
This example illustrates how familial and community-based mentorship provided early clarity and reassurance, reinforcing self-efficacy, a key component of SCCT Theory (Lent et al., 1994).
Others described mentorship as a turning point in overcoming doubt and envisioning success. Paul shared: Mentors made me believe that I could do something, and see the good impact I would make.
His experience highlights the role of mentors as affirming agents who dismantle internalized barriers and help Black men recognize their own potential. Through a CRT lens, this support can be seen as a counterforce to institutionalized doubt and systemic exclusion (Delgado & Stefancic, 2017).
Beyond affirmation, mentorship often provided tangible access to career opportunities and advanced training. Malcolm explained: My mentor was the director of counseling at my university, and he pushed me to consider graduate school in psychology. He opened doors for me and gave me confidence to believe I could succeed in this field.
Mentorship in this context acted as a structural intervention, bridging opportunity gaps and counteracting racialized underrepresentation in the profession. Moreover, it modeled what was possible, frequently through same-race role models who embodied the success participants aspired to achieve.
Mentors were not only instrumental in offering practical advice and career navigation strategies but were also seen as emotional anchors during challenging circumstances. Many participants emphasized the importance of mentors, who validated their struggles, normalized their experiences as Black men in predominantly White academic spaces, and encouraged persistence.
Taken together, participants viewed mentorship as essential, not incidental. It was a form of culturally responsive support that expanded their access, deepened their sense of belonging, and helped solidify their professional identity.
Education and Professional Development
Academic and professional training shaped participants’ entry into the mental health field. Participants (n = 17) described how coursework and field experiences revealed community needs and career opportunities, while many also navigated predominantly White institutions with limited cultural support. These experiences influenced both their development and commitment to the profession.
Keith described how his undergraduate coursework in sociology helped him make sense of structural inequities and sparked a desire to support others: As I was going through undergrad, I was studying sociology, and I was like, you know, this gives me explanations on why certain communities go through certain stuff and others don't. Seeing Black students drop out of college due to mental health issues really pushed me to figure out how to support them and myself. That journey led me to pursue a master’s in social work.
Keith’s account illustrates how educational content can deepen awareness of social issues and motivate career decisions rooted in community care. It reflects SCCT’s focus on outcome expectations and person–environment fit as factors in career development (Lent et al., 1994).
Sam recalled a formative moment when he encountered a visual display about social work during high school: I believe 70% of social workers are wounded healers. So they've been through experiences that have wanted them to give back and to help others who are going through those experiences. I was in my junior year of high school. I had about four internships under my belt, all in social service, but I had no idea which way I wanted to go. Then I saw this pie chart at the school of social work showing 50 different categories of what you could do with social work. That was my defining moment.
This moment of discovery reflects how exposure to diverse career possibilities can ignite vocational clarity. For Sam, this realization marked a turning point in identity formation, where awareness of opportunity intersected with internal motivation, a dynamic consistent with SCCT’s focus on self-efficacy and career exploration (Lent et al., 1994).
These responses show how education shaped participants’ sense of purpose and direction. Academic exposure and early experiences clarified career paths, strengthened self-efficacy, and deepened their commitment to service.
Barriers Deterring Black Men From Entering the Field
While the overarching theme of Motivation, encompassing both personal purpose and social support, illustrates the factors that encourage Black men to pursue mental health careers, participants also identified a set of barriers that impede entry and advancement within the field. The second analytic category, Barriers, captures the sociocultural and structural challenges that hinder Black men’s entry and advancement in the mental health field. The first theme, Stigma, included subthemes of Gender and Masculinity and Intersecting Identities and Microaggressions, highlighting how cultural norms and racialized experiences created feelings of exclusion. The second theme, Structural Inequalities, encompassed barriers in licensure, finances, and education, including biased exams, student debt, lack of early exposure, and limited representation. These themes reveal how racialized and gendered systems continue to restrict access and progress in this profession.
Stigma
Among the barriers identified, Stigma stood out as a deeply rooted obstacle that discouraged Black men from entering the mental health field and shaped their perceptions of belonging within it. Participants described how cultural expectations and societal narratives shaped their perceptions of emotional expression and professional identity. Two subthemes captured these experiences: Gender and Masculinity, which highlighted how norms around toughness and emotional restraint conflict with the nature of mental health work; Intersecting Identities and Microaggressions reflected the bias and exclusion participants encountered as Black men in predominantly White academic and clinical spaces.
Gender and Masculinity
Traditional views of masculinity discouraged emotional expression and framed mental health work as incompatible with male identity. Participants (n = 10) recalled being taught to “be tough” and avoid vulnerability, making caregiving roles feel misaligned with expectations of manhood. Carson reflected on how traditional views of masculinity shaped his perception of the field: Growing up, we were always told, ‘Men don’t cry,’ or ‘Be tough.’ So, the idea of working in a field where you’re helping people process emotions doesn’t fit the image of what a man is supposed to be.
Carson’s experience reflects the impact of gendered cultural conditioning, where emotional labor is perceived as incompatible with dominant notions of Black masculinity. This reinforces internalized stigma that shapes career interest and confidence. His narrative aligns with SCCT, as restrictive gender norms can limit perceived self-efficacy and outcome expectations. From a CRT lens, it highlights how racialized constructions of masculinity further marginalize emotional expression and discourage entry into care-based professions. Jake highlighted the gendered perceptions of the profession: Social work in itself is a female-dominated industry, right? And, you know, if you watch any movie or when you think of a social worker, you don’t think of men. You think of women who are trying to help, not men.
Jake’s reflection illustrates how public narratives and media representations reinforce the association of helping professions with femininity, implicitly excluding men, especially Black men. This lack of visibility impacts both identity formation and the perceived legitimacy of pursuing such roles.
Intersecting Identities and Microaggressions
Participants reported experiencing racial and gender-based bias in academic and clinical settings. Some participants (n = 17) described how microaggressions created exclusion and reinforced stereotypes, undermining their confidence and sense of belonging in the profession. Don reflected on the pressure of being one of the few Black men in professional settings: I always felt like I had to prove I belonged, especially being one of the only Black men in the room. It’s like you’re constantly navigating how others see you.
This reflection reveals the psychological strain of being racially hyper-visible in predominantly White spaces. Constantly managing how one is perceived involves emotional labor and reinforces a sense of otherness. Through the lens of CRT (Delgado & Stefancic, 2017), Don’s experience illustrates how institutional environments maintain racialized exclusion even when Black men are present. From an SCCT perspective (Lent et al., 1994), such experiences negatively impact self-efficacy and contribute to internalized doubts about one’s place in the profession. Kyle described feeling isolated and unsupported in a predominantly White school setting: My supervisors didn’t really know how to work with the Black community. It was hard being the only Black clinician in a school full of white staff. Black and Brown youth would seek me out, but I didn’t have the institutional support to meet their needs.
Kyle’s reflection underscores how underrepresentation, coupled with a lack of institutional support, leads to isolation and burnout. This reinforces CRT’s view that diversity without structural change fails to support marginalized professionals. These accounts reveal how race, gender, and professional identity intersect to create systemic barriers, leaving Black men unsupported in the very spaces where they are most needed (Delgado & Stefancic, 2017).
Structural Inequalities
While Stigma highlighted the cultural and interpersonal forces that shape Black men’s perceptions of the mental health field, participants also emphasized the Structural Inequalities that restrict tangible access and advancement within it. Structural Inequalities, such as biased licensure processes, financial hardship, and inadequate educational preparation, shaped participants’ access to and persistence in the mental health field. These experiences are captured in three subthemes: Barriers in Licensure and Certification, Financial and Economic Challenges, and Education and Professional Gaps. Collectively, they reflect the cumulative effects of disinvestment, policy bias, and exclusion, which are core concerns of CRT (Delgado & Stefancic, 2017) and SCCT (Lent et al., 1994).
Barriers in Licensure and Certification
Licensure emerged as a major structural barrier to entry and advancement in the mental health field. Participants (n = 15) described the licensing exam process as culturally biased, inaccessible, and misaligned with their lived experiences. Jamal’s reflection underscores the perceived cultural disconnect embedded in standardized testing practices, particularly licensure exams in mental health fields: I was told you had to think like a White woman, or you had to think like a cop to pass this test. And this is what you have to think like to pass.
His comment illustrates how passing the exam is perceived to require a mindset that diverges from one’s own identity. This reinforces CRT’s assertion that professional systems frequently prioritize dominant cultural norms, marginalizing the perspectives and strengths of people of color (Delgado & Stefancic, 2017). Malcolm shared a similar experience: When I was studying for the LCSW exam, somebody gave me a tip, and the tip was: Don’t study like you have the mindset of a 40-year-old Black male.
This advice reveals how deeply embedded racial and age-based assumptions are within the licensure process. Through the lens of SCCT (Lent et al., 1994), this may erode outcome expectations and reduce self-efficacy, signaling that success in the field may require abandoning one’s cultural identity.
Collectively, these reflections highlight how structural barriers in certification not only hinder access and advancement but also reproduce exclusion by requiring assimilation into dominant cultural norms.
Financial and Economic Challenges
Financial hardship was frequently described as a deterrent to entering or remaining in the mental health field. Participants (n = 19) shared how the cost of graduate education, low compensation in the profession, and the need to support themselves or their families created unsustainable pressure. These economic barriers influenced both their initial career decisions and long-term professional trajectories. Donald reflected on the strain of balancing educational debt with low wages: It’s hard to justify going into a field where you’re accumulating so much debt for a degree, and the pay doesn’t match the effort or cost. You’re making sacrifices every day to stay in this work.
His statement captures the tension between professional commitment and financial survival, highlighting how compensation in the field fails to reflect the demands placed on clinicians. From an SCCT perspective (Lent et al., 1994), low outcome expectations regarding financial return significantly discourage career pursuit or persistence. Jackson described how economic struggles were compounded by early academic disadvantages: It’s tough being able to fund school. In many cases, you forego an income unless you’re working while attending school, which is extremely difficult. I think, naturally, there are more educational barriers for Black men. Additionally, when financial struggles exist and you’ve faced challenges in K-12, those deficits can make you believe it’s not possible.
His reflection highlights the cumulative impact of financial and educational inequity. CRT helps contextualize this within broader patterns of systemic disinvestment in Black communities, wherein historical and structural disadvantages limit access to the profession (Delgado & Stefancic, 2017).
Despite these challenges, some participants maintained a sense of purpose and possibility. Kevin explained how targeted financial support could reshape access: Yeah, I just think if they had the financial support to do so if scholarships were available, if while you're in high school, you could identify a kid with potential, put them on a social work track, and connect them to an agency upon graduation, that would be the best plan.”
Kevin’s suggestion reflects a proactive vision for enhancing equity in the profession. His comment underscores how system-level interventions, such as scholarship programs and career pathways, can address disparities and support retention.
Collectively, these reflections illustrate how financial and economic constraints serve as structural barriers that disproportionately affect Black men’s access and success in the mental health field. Without intentional reforms to reduce the debt burden, increase compensation, and provide early financial support, the struggle for equity and representation will continue.
Education and Professional Gaps
Limited access to quality education, lack of representation in academic content, and cultural messaging shaped early barriers to entering the mental health field. Participants (n = 17) described how these systemic inequities undermined their confidence, delayed career discovery, and reinforced the belief that this profession was not meant for them. Jim described how limited representation and inequitable schooling environments during K–12 contributed to a sense that higher education was unattainable: Some black men in K through 12 have educational deficits, and by like not seeing other black men with degrees or obtaining a masters it doesn’t seem attainable to them.
This reflection illustrates how early educational inequities and limited representation converge to shape academic aspiration and self-efficacy among Black men. When young Black boys experience under-resourced schools and lack exposure to educators or professionals who look like them, educational deficits compound over time, reinforcing the perception that higher education is inaccessible. These early experiences can erode confidence, discourage persistence, and delay or deter entry into professional fields such as mental health. Viewed through the lens of CRT, this underscores how systemic disinvestment and racial underrepresentation within education perpetuate a cycle of exclusion, limiting access to culturally affirming role models and sustaining structural barriers to advancement (Delgado & Stefancic, 2017). For those who did persist, encountering a curriculum dominated by White theorists contributed to feelings of cultural disconnection. As Malik shared: We were looking over all the theories and all the practitioners. They’re all older white males. And so I was thinking to myself, oh, well, this field probably isn’t for me. Because why don’t people like me do this, right? We didn’t see... no Black theorist or anyone in those books.
Malik’s reflection illustrates how the lack of Black representation in academic content can erode a sense of belonging and reinforce systemic exclusion, a dynamic central to CRT (Delgado & Stefancic, 2017). It also aligns with SCCT, which posits that limited representation weakens self-efficacy, outcome expectations, and access to role models (Lent et al., 1994).
Mathew also recalled how the media further narrowed his understanding of what a mental health professional looked like: I grew up watching Frasier, and I didn't even put two and two together that Frasier was a therapist because he was a talk show host, right? So for me, that was a whole other thing. But that's what I thought a therapist was: an older white guy who had you sit on a couch and talk to you about your problems.
His quote illustrates how early cultural representations, particularly those that exclude people of color, shape the professional identities that youth internalize. It reinforces CRT’s assertion that racialized invisibility operates not only in education but also in the broader cultural narratives young people absorb (Delgado & Stefancic, 2017).
Collectively, these reflections demonstrate how educational and cultural gaps delay access to the mental health field and shape a deep sense of exclusion from it. Reforms in early education environments and the representation and portrayal of mental health careers across systems are required to address these barriers.
Discussion
The purpose of this study was to explore how sociocultural and racialized barriers shape Black men’s motivations to pursue mental health careers and the factors that deter them from entering or advancing in the field. Guided by CRT and SCCT, the study sought to understand how structural inequities, self-efficacy, and identity formation influence career pathways among Black men in the mental health profession.
Participants frequently described a strong sense of personal purpose and community responsibility as central to their decision to pursue careers in mental health. Many cited lived experiences with trauma, grief, and exposure to community violence, paired with a lack of culturally responsive providers, as powerful motivators. The desire to offer identity-affirming care, break generational cycles, and heal their communities echoed the Gendered Racial Equity Ethic described by Beasley and Hernandez (2025), which emphasizes ethical and community-rooted motivations among Black men in psychology doctoral programs.
This sense of purpose was often nurtured and reinforced through meaningful relationships, with mentorship emerging as a critical influence on participants’ career trajectories. Encouragement from family members, educators, and community figures reinforced their belief in their ability to succeed and contributed to a sense of purpose. This finding aligns with SCCT, which highlights that self-efficacy, social support, and expected outcomes influence career development. Similarly, Hannon et al. (2024) found that mentorship plays a critical role in guiding Black students through academic institutions and into counseling professions. Their study reinforces the idea that having relatable, trusted mentors not only supports academic persistence but also affirms cultural identity and belonging, key elements echoed in participants’ responses.
The role of educational experiences was also emphasized by the participants in shaping their professional development. Coursework, early exposure to mental health careers, and supportive learning environments deepened their sense of purpose and clarified their career direction. These findings align with SCCT, which highlights the influence of self-efficacy and outcome expectations on career choice (Lent et al., 1994). Similarly, Chandler (2011) found that Black psychology students thrive when academic programs provide early exposure, culturally relevant training, and strong support systems. Their study underscores the role of institutions in affirming students’ identities and equipping them to navigate predominantly White academic spaces—factors that also emerged as critical in the present study.
While many participants were motivated to pursue mental health careers, several identified Black masculinity norms as a barrier. Emotional vulnerability, a key element of mental health work, conflicted with cultural expectations of stoicism, leading to hesitation and external judgment. This aligns with SCCT, which highlights how negative outcome expectations can reduce interest in certain fields (Lent et al., 1994). Consistent with these findings, Beasley et al. (2015) found that Black men in psychology often struggle with societal messages that discourage emotional expression and reinforce the perception that mental health work is misaligned with masculine identity. Their study, like the present one, points to the need for more affirming spaces that challenge rigid norms of masculinity and support Black men in pursuing emotionally engaged professions.
Structural barriers, including financial hardship, low pay, and student debt, which limited access to graduate training, shaped participants’ pathways. Licensure exams were seen as culturally biased and structurally exclusionary. These findings mirror existing research; Beasley et al. (2021) documented how men of color in psychology navigate exclusion and the perception of counseling as a low-status field. Beasley and Hernandez (2025) highlighted institutional isolation and gatekeeping in doctoral programs. Apgar and Nienow (2024) found disproportionately low pass rates for Black and Brown graduates on the Association of Social Work Boards exams, rooted in structural racism. Collectively, these studies affirm that the barriers described by participants in the present study reflect broader, systemic patterns in mental health credentialing.
The findings reveal that Black men pursuing mental health careers are driven by a desire to create change and counter harmful community narratives. CRT (Delgado & Stefancic, 2017) illuminates how they navigate underrepresentation shaped by racial and gendered stereotypes, aligning with Wingfield and Alston’s (2012) work on Black professional men. Masculinity norms also posed barriers, echoing Forsman and Barth’s (2017) findings on male participation in female-dominated fields. These dynamics reflect SCCT’s focus on outcome expectations and self-efficacy (Lent et al., 1994). Despite these challenges, the participants remained committed to service, underscoring the need for pathways that promote equity and culturally grounded care.
Limitations and Future Directions
Several limitations should be considered. While the study offers valuable insights, it may not reflect experiences across all geographic or professional contexts. Self-selection may have introduced recruitment bias, as those with strong views on race, gender, or professional barriers may have been more likely to participate. Researcher positionality may also have shaped interpretation, as shared identity can both build trust and influence analysis. Finally, the cross-sectional design captures a single point in time, limiting understanding of how motivations and barriers may evolve. These limitations highlight the need for longitudinal, multi-site research on Black men’s pathways into mental health.
Implications
An urgent need exists to establish structured entry pathways into the mental health field for Black men, starting as early as high school. Peer-led mental health groups in schools can facilitate early exposure, affirm identity, and cultivate leadership in spaces where Black males are often underrepresented. These initiatives help counteract social and structural barriers that discourage the pursuit of communal careers such as psychology and social work (Beasley et al., 2015, 2024). Clear clinical pathways, including internships, group facilitation, and targeted messaging, can build confidence and sustained interest. Promoting mental health careers on social media platforms such as TikTok and Instagram may also reframe the field as culturally relevant and purposeful (Zhang et al., 2021).
To build on these early interventions, national Black professional organizations can serve as key partners in formulating and sustaining these pathways. Organizations such as the Association of Black Psychologists, the National Association of Black Social Workers, and the National Association of Black Counselors could play a meaningful role in creating targeted initiatives that support Black males’ entry into the mental health field. This might include launching national programs implemented by local chapters to introduce high school-aged Black boys to mental health careers. Over time, these efforts could expand to include mentorship programs, dedicated scholarships, and summer camps. Through these initiatives, Black boys could learn from Black scholars, develop mental health knowledge and skills, participate in rites of passage, and explore the full range of opportunities the field offers.
At the postsecondary level, initiatives such as the We Are Men program at the University of Illinois Chicago’s Jane Addams College of Social Work offer a powerful model. This program provides scholarships, mentorship, and professional development opportunities to Black male graduate students pursuing mental health careers, addressing both financial and structural barriers while fostering community and identity (University of Illinois Chicago, 2021). Institutions should replicate such efforts while also uplifting the legacies and theories of scholars such as Dr Joseph White, Dr Amos Wilson, Dr Bobby E. Wright, and Dr Frantz Fanon, to cultivate a culturally grounded pipeline of practitioners.
Finally, licensing reforms are critical to ensure equitable access to the profession. States such as Illinois, Rhode Island, and Connecticut have implemented alternatives to traditional clinical social work licensure exams by allowing additional supervised hours to substitute for standardized testing (Apgar & Nienow, 2024). These shifts offer equitable pathways for qualified Black men, many of whom face systemic disadvantages in the licensure process. Collectively, these educational and policy strategies provide a more inclusive foundation for a mental health workforce that reflects and serves diverse communities.
Conclusion
This study shows that Black men’s pursuit of mental health careers is influenced by both systemic barriers and culturally rooted motivations. Despite educational, financial, and structural challenges, their commitment reflects a deep sense of social responsibility and community uplift. Grounded in CRT, the findings highlight how racism and underrepresentation shape career pathways, while SCCT emphasizes the role of self-efficacy, mentorship, and representation (Delgado & Stefancic, 2017; Lent et al., 1994). These insights affirm the importance of culturally grounded pathways, racial identity, and healing in advancing the goals of Black psychology. Increasing representation requires both dismantling structural barriers and amplifying the strengths Black men bring to the field.
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board at the University of Cincinnati (Protocol #2024-0257). All procedures were conducted in accordance with ethical standards for research involving human participants.
Consent to Participate
Verbal informed consent was obtained from all participants, with documentation of consent procedures approved by the Institutional Review Board.
Author Contributions
The authors would like to acknowledge the following contributions to the development of this manuscript. Aaron Mallory facilitated and conducted the interviews and led the drafting of the data analysis section. Toluwanimi Arogundade assisted in data analysis and contributed to writing the literature review. Lauren White contributed to the development of the discussion and conclusion sections and provided critical revisions throughout the writing process.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The qualitative data from this study are not available for sharing owing to confidentiality and ethical restrictions.