
Abstract
Literature on the consequences of managerial reform for professionals in public services has often taken the professions as universal phenomenon, unaffected by sectoral heterogeneity. However, focusing on professionals’ own perspectives, this study notes important similarities and variations between professionals from two domains—GPs and teachers. The findings are attributed to professional identity values of excellence, ethics, and engagement, against which reforms were directed, and to the capacity of different professional groups to develop strategies based on these values. Suggesting that the professional identity of specific professions is key creates different conditions and consequences for introducing new management practices.
Introduction
Despite increasing attention for professional roles in collaborative governance approaches (Aschhoff & Vogel, 2019; Steen & Tuurnas, 2018), over three decades of public management reforms leading to managerial changes have left a clear mark on public services in most western countries (Hendrikx & Van Gestel, 2017; Pollitt & Bouckaert, 2017). “Managerialism” refers to “governmental public policy diffusing managerial thinking into public organizations to measurably improve organizational efficiency” (McGivern et al., 2015). Even new collaborative forms like network governance and co-production of public services with citizens (Aschhoff & Vogel, 2019; Osborne et al., 2016; Sørensen & Torfing, 2011; Tuurnas, 2015) are often still steered by managerial means, for example, by encouraging collaboration through financial incentives, by protocolizing professional practices and by measuring performance for transparency purposes.
Although literature provides us with many overviews of these managerial reforms, few systematically compare what the consequences are for the professionals who are responsible for public service delivery within those managerialized contexts (Adams, 2015; Mauri & Muccio, 2012). Professions can be described as institutionalized occupations (Abbott, 1988; Evetts, 2013), whose members are granted a certain amount of autonomy and prestige to deliver services that are key to society (Gardner & Shulman, 2005; Noordegraaf, 2015). Although its exact characteristics are up for scholarly debate, professionalism is commonly associated with high-skilled exclusive expertise, objectivity, and altruism often captured in (implicit) ethical codes, and workers’ commitment to clients and profession (Abbott, 1988; Gardner & Shulman, 2005; Leicht, 2016). Most scholars have studied the consequences of managerialism for a single profession (Brodkin, 2011; McGivern et al., 2015; Shams, 2019), or infer general (inter)national trends (Dent et al., 2016; Faulconbridge & Muzio, 2011; Leicht et al., 2009) without sectoral specificities. This does leave us with the question whether results of single-case studies or of the more abstract and generalized trends are relevant to all domains, or may need further specification. Therefore, despite few exceptions (see Klenk & Pavolini, 2015; Turner et al., 2016), more comparative analyses of the impact of managerialism on professionals across various professional domains are necessary (Adams, 2015; Hendrikx & Van Gestel, 2017).
This is particularly true for the perspectives of professionals themselves (Denis et al., 2015), whereas managerialism has implied changes at public sector level (macro-level) and at the level of individual public services organizations or policy networks (meso-level). However, much remains unknown about how this has affected the development of professionals’ role expectations and identities at micro-level (Aschhoff & Vogel, 2019; Van Gestel et al., 2019). Such insight is important though, because awareness is growing that professional identity is a key mechanism through which professionals make sense of, and enact upon, what they come across in their workaday practice (Bévort & Suddaby, 2016; Spyridonidis et al., 2015). Literature also shows that professional identity change can be triggered by developments in professionals’ macro- and meso-level contexts (Chreim et al., 2007; Denis et al., 2015). As such, managerialism has the potential not just to change the roles of professionals, but also their “hearts and minds” (Ball, 2003), leading to different interpretations and ultimately different professional practices in public service delivery. Connecting macro-/meso-level managerial change to micro-level professional identity is therefore crucial to improve our insight into the role of professional values in implementing managerial reform (Denis et al., 2015; Zacka, 2017).
This study aims to acquire such better understanding by systematically comparing the consequences of managerial reforms on professionals in two different domains within one national context from a professional identity perspective: general practitioners (GPs) in primary health care and teachers in secondary education in the Netherlands. Although not as substantial as in Anglo-Saxon countries, public sectors in the Netherlands have been confronted with managerial reforms comparable to other countries in the western world (Kickert, 2008; Pollitt & Bouckaert, 2017). Despite differences, for both GPs and teachers, these changes imply among others an increasing standardization of their professional practice and a growing measurement of their performance (Pavolini, 2015; Schimank, 2015). Although GPs and secondary school teachers are often characterized as “full professionals” and “semi-professionals” respectively (Etzioni, 1969), with teachers inevitably having less autonomy due to the fact that they are part of a school organization, it should not be underestimated how much in fact they have in common: like general practice, teaching has considerable professionalism traits, including specific teacher training, objectivity and altruism, and dedication to student development (Schimank, 2015; Van Veen, 2008). Moreover, both professionals fulfill key roles in the lives of ordinary citizens and therefore the way they deal with these changes in their daily practice determines to great extent the perceived quality of crucial public services (Zacka, 2017). Hence, comparing GPs and teachers within these two policy areas offers a unique way to study what managerial reforms ultimately imply for professionals, enriching our understanding of professional identity and its micro-level (re)construction.
Going beyond the well-described managerial pressures on professionalism (Freidson, 2001), the comparative analysis of the consequences of managerial reform for professionals in the two domains suggests first of all a mismatch between public managers’ and professionals’ perceptions of professional work. While the former often focus on “hard” and “technical” quality (Klenk & Pavolini, 2015; Newman, 2013), professionals themselves define softer aspects like the relational or social side as the core of their professional work. Leaving interactions with clients—patients and students—largely ignored in managerial reform, this creates professional identity conflicts. Second, the analysis shows important differences in the timing, approach, and outcomes of the reform itself (Hendrikx & Van Gestel, 2017; cf., Ackroyd et al., 2007). As this study argues, these variable outcomes of managerialism in two sectors can be attributed in large part to the professional values against which reforms were directed and the strength of professionals’ identity determining the extent to which different professional groups were able to develop strategies for promoting professional aims.
The analysis of the consequences of managerial reform on the professionals across two services is presented in four parts. First, the origins of management restructuring and the nature of change in the context of the literature on managerial reform and professional identity are considered. Then, the research methods are described, including interviews with 52 GPs and secondary school teachers. The third and main section of the paper holds the presentation of the comparative analysis of the managerial reforms in both policy domains under study and their differing consequences on the two professions, as perceived by GPs and teachers. Finally, this article discusses how the observed variations across the two domains can be explained in the light of current academic debates.
The Consequences of Managerial Reform on Professional Identity
One of the consequences of the new public management (NPM) as a steering paradigm that came into fashion in the late 1980s throughout the western world has been the focus on improving efficiency and effectiveness of public service delivery using private sector managerial techniques and principles (Ackroyd et al., 2007; Pollitt & Bouckaert, 2017). Despite national variations (Kickert, 2008; Pollitt & Bouckaert, 2017), the resulting managerial reforms often implied for public sector professionals that they became profiled as accountable service providers rather than autonomous experts with considerable discretion from public and political accountability (Aschhoff & Vogel, 2019; Hendrikx & Van Gestel, 2017; Evetts, 2013). A growing focus on their (measurable) output led to a shift toward more top–down knowledge and performance measurement, thereby protocolizing and regulating professional practice and enhancing accountability procedures to control professionals’ performance (Dent, 2006; Newman, 2013; Waring & Currie, 2009), empowering management over professionalism (Bryson et al., 2014; Leicht et al., 2009). Although professionals’ community and collaboration with their peers as basis for their legitimacy remained highly relevant, competition among professionals in many sectors has simultaneously been encouraged, creating a layered and complex environment of expectations in which professionals need to ensure the continuity of public service delivery (Hendrikx & Van Gestel, 2017; Leicht, 2016).
Most studies on managerialism in relation to professional work focus on how the practices of professionals are impacted in specific domains (Brodkin, 2011; McGivern et al., 2015; Shams, 2019), often highlighting the problematic reconciliation between professional and managerial modes of working (Freidson, 2001; Leicht, 2016; Noordegraaf & Steijn, 2013). However, more scholarly attention is needed into how professionals themselves experience, weigh, and ultimately enact upon managerial reform, adding a bottom–up perspective to public administration literature (Hupe & Hill, 2016). This is in line with growing awareness that policy reforms designed by policymakers never offer blueprints that professionals merely execute; professionals always need to interpret and apply them to concrete cases (Brodkin, 2011; Hupe & Hill, 2016; Zacka, 2017). Therefore, whether the goals and ambitions of managerial reforms are met, depends on their outcome in public service delivery and hence their success lies for an important part in the hands of professionals (Brodkin, 2011; Hupe & Hill, 2016). However, despite literature on policy implementation emphasizing the importance of taking a bottom–up perspective, the daily realities of frontline professionals are still easily lost out of sight by policy makers (Hupe & Hill, 2016; Matland, 1995; Zacka, 2017). This may be problematic for professionals themselves, as becomes apparent in the discontent and struggle among frontline professionals of all stripes who have trouble reconciling their professional norms and values with those of the modern day policies they have to implement (Jansen et al., 2010; Tummers et al., 2009). However most importantly, this will ultimately be problematic for society and its citizens whereas they are the end-users of professional services (Zacka, 2017).
Literature suggests that professional identity is a key mechanism through which professionals make sense of, and enact upon, what they come across in their workaday practice (Ashcraft, 2007; Pratt et al., 2006). It provides the language, values, and meanings through which professionals perceive and interpret not just the contact with their clients but also the dealings with their institutional and organizational environment (Chreim et al., 2007). In case professionals are expected to execute new roles due to managerial reforms, they interpret these changes through the lens of their professional identity (Pratt et al., 2006; Spyridonidis et al., 2015). Professional identity can be defined “as the relatively stable and enduring constellation of attributes, beliefs, values, motives, and experiences in terms of which people define themselves in a professional role” (Ibarra, 1999, p. 765). In case of the professions, the institutionalized collectives provide these constellations for their members. The social interaction between individual and collective is shaped by elaborate socialization processes through professional training and membership of professional associations. Consequently, professional socialization leads to the development of “a sense of common experiences, understandings and expertise, shared ways of perceiving problems and their possible solutions” (Evetts, 2013, p. 780). Despite some typical individual variation between members of the same profession (Bévort & Suddaby, 2016), this creates a strong shared sense of professional identity (Barbour & Lammers, 2015).
Since professional identities are not fixed but are “relatively stable” (Ibarra, 1999), they gradually change over time. Such change can among others be triggered by developments in professionals’ organizational and institutional environments, including the managerial reforms that professionals need to implement (Chreim et al., 2007; Denis et al., 2015). In this sense, managerial reforms have the potential to fundamentally alter professionalism, not just by changing their roles but also by changing professionals “hearts and minds” (Ball, 2003). After all, in literature on professional identity, it is argued that professional identity has two sides that evolve interactively: self-image and role (Ashcraft, 2007; Barley, 1989; Chreim et al., 2007; Reay et al., 2017). Self-image refers to the normative beliefs individual professionals hold about the collective purpose, goals, values, norms, and interaction patterns associated with being a member of their profession (Ahuja et al., 2017; Ibarra, 1999; Reay et al., 2017). These beliefs are the relative stable ways of how professionals think they should be (Hendrikx, 2018, 2020). Role refers to the real-life actions and experiences of enacting a job (Ashcraft, 2007; Ibarra, 1999). Role is thus about what professionals perceive they do, which is determined by workaday practice throughout their career (Hendrikx, 2018, 2020). Changes in roles have the potential to change self-images, leading to new processes of sensemaking and enacting by professionals and hence new practices in public service delivery. Therefore, professional identity is a crucial link in our understanding of the interactions between professionals and the managerial changes in their respective fields (Barbour & Lammers, 2015; Denis et al., 2015; Reay et al., 2017; Shams, 2019).
To study the consequences of managerial reform for professionals in two domains, in this article, professional identity is operationalized with the values from the so-called “Good Work framework” (Barendsen & Gardner, 2009; Gardner et al., 2001). This framework has been developed to comprehend three main values of professional work—excellence, ethics, and engagement—and thereby includes the most important traits of professionalism (see also Hendrikx, 2018, 2020). Excellence refers to the standards of skills and expertise, which allures to the most prominent facet of professionalism and that is high-skilled exclusive expertise. Ethics is about the social responsibility a worker has toward others, which resonates with professional objectivity and altruism often captured in (implicit) ethical codes. Engagement taps into a worker’s dedication to his or her work, which captures professionals’ commitment to clients and profession. For each value, this study examines how professionals define their self-image followed by their perception of how they enact upon it in the lived reality of their workaday roles. In this vein, professional identity offers a unique way to study how professionals think they should act in close relation to what they perceive doing in daily reality, in a context of managerial reform.
In terms of the self-image and role dynamic, managerial changes have led to an accumulation of role expectations requiring professionals to change their practices (Aschhoff & Vogel, 2019; Hendrikx & Van Gestel, 2017). Hence leading to concrete role changes, the consequences of managerial reform have therefore primarily been on the role side of the professional identity coin. However, considering the close link between the two, this study aims to find out how this affects professionals’ self-image as well by examining how professionals of two domains perceive these role changes in relation to their self-image for each of the three values of the Good Work framework (Figure 1).
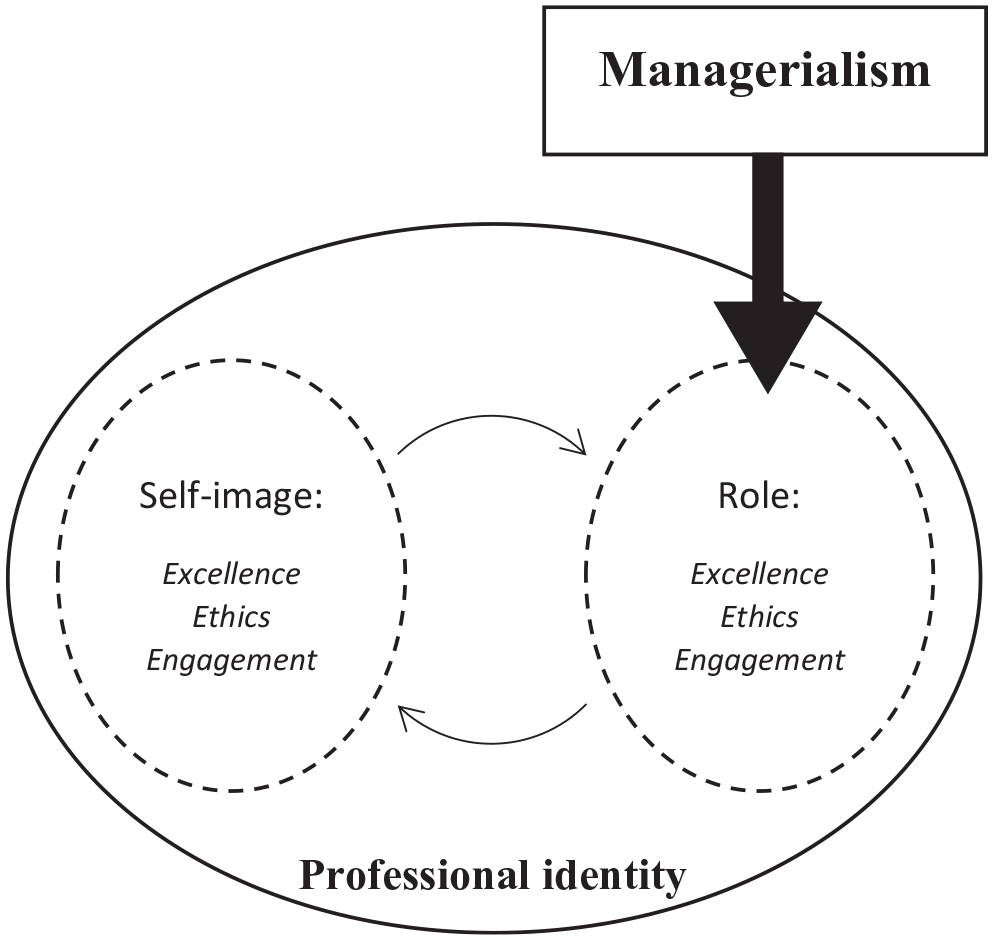
Managerialism impacting professional identity.
Managerialism in Dutch General Practice and Secondary School Teaching
In line with broader international trends, managerial mechanisms have been introduced in Dutch health care and education sectors (Saltman et al., 2012; Snoek, 2017). International literature often describes how both modern day GPs and teachers are increasingly confronted with a standardization of their professional work, and how this standardization is subsequently used to measure and evaluate professional performance (Pavolini, 2015; Schimank, 2015). Nevertheless, despite these overall similarities, a closer look into what managerialism exactly means for both professional domains in the Netherlands learns that important differences exist in their timing, approach, and outcomes even within one national context (Hendrikx & Van Gestel, 2017; cf., Ackroyd et al., 2007).
For GPs in the Netherlands, the most influential managerial change was due to the transformation of the Dutch health care system with the Health Insurance Act [2006], aiming to improve health care quality while cutting costs (see Van de Ven & Schut, 2008 for an overview). However, this market-oriented health care reform not only changed GPs’ remuneration system toward an output orientation, adding a fee-for-service component next to a capitation fee—an annual ‘registration fee’—(Schut et al., 2013); it also established an “audit culture” (see also Shore & Wright, 2015) pressuring GP practice to become more transparent (Schäfer et al., 2010). As a consequence, GP practice has been cut into predefined standardized services—or “products” (Van de Ven & Schut, 2008)—turning them into measurable, priced, and hence manageable blocks. Using the International Classification of Primary Care (ICPC) codes, GPs must label each patient contact for reimbursement purposes. At the same time, this coding provides health insurers insight into GP performance (Hendrikx, 2018; Schut et al., 2013).
For teachers, managerial changes were rather gradual. Being positioned within a school, teachers slowly but steadily became even more so encapsulated by this organizational setting. Since the 1980s, managerial reforms fostered school merging, and strengthened the position of school management by introducing a system of lump sum financing while delegating many tasks including staff management to school boards (Karsten, 1999; Waslander et al., 2016). The increase of school autonomy has been accompanied by high-stakes accountability mechanisms to control educational quality and content to enhance the performances of students, teachers, and school organization (Hooge, 2017). As a result, educational practice has been substantially standardized and quantified using “centrally determined and monitored measures of pupil achievement” (Day, 2007, p. 677), putting teachers in an ever more executive role vis-à-vis their school management.
So although both professional domains are affected by managerialism, for GPs it took up until mid-2000s before managerial reform changed their practice considerably (Van de Ven & Schut, 2008), while for teachers this started at least 15 years prior to that. Moreover, while GP performance is made visible by health insurers, their direct relationship is not a hierarchical one, leaving them at least some room to maneuver (Hendrikx, 2018). For teachers on the contrary, their school boards directly use their educational scores as a proxy for teacher performance (Hendrikx, 2020). Hence, although both sectors have been confronted by substantial managerial reform, it appears that secondary school teaching in the Netherlands has been impacted earlier and stronger than Dutch general practice. Against the background of these differences, this study’s results will be presented and discussed, but first its methodology will be explained.
Methods
Focusing on the scale and organization of their professional groups, data show that in 2016 approximately 11,834 GPs worked in the Dutch primary care sector (Van der Velden et al., 2017) and that in the same year, Dutch secondary schools employed a total of 75,700 teachers. This study focusses on teachers holding a postgraduate degree in their subject field, whereas their identity is expected to be most strongly developed. Although the exact numbers are not registered, based on the amount of hours taught, 44.616 persons are calculated to be postgraduate degree teachers (DUO, 2018). In addition, the formal organization of the two sectors shows that health care professionals, especially GPs, have a background of local individual entrepreneurs with strong informal networks. Since the 2000s, they are increasingly organized in primary health groups, with the GPs and multiple practitioners such as physiotherapists in a collaborative setting (Boot, 2013). Teachers, by contrast, have traditionally been located in more bureaucratic and “managed” settings (Bronneman-Helmers, 2011).
Building on earlier studies drawing on a variety of (secondary) data sources (Ackroyd et al., 2007; Turner et al., 2016), we use comparable interview data as main source, which allows taking into account professionals’ views on their professional values of expertise, ethics and engagement across two domains related to managerial reforms in their respective fields. In total, 22 GPs were interviewed in 2012, and 30 secondary school teachers with a postgraduate degree in 2017 (Table 1). All professionals were interviewed using Rubin and Rubin’s (2005) procedure for conversational partnership which allowed to win trust and to encourage professionals to reflect deeply upon their self-image and role, first for excellence, then for ethics and finally by engagement. For each of these three elements of the Good Work framework, professionals were asked to describe what they believed this element should be, appealing to their self-image. Then, participants were asked to describe how they believed what this element actually looked like in their workaday practice, appealing to their role. This exploration of their own definitions of their self-image and role for each of the three elements of Good Work was crucial to define their professional identity in their own terms. All interviews lasted an hour on average and were audio recorded and transcribed.
Overview of Interviewees.
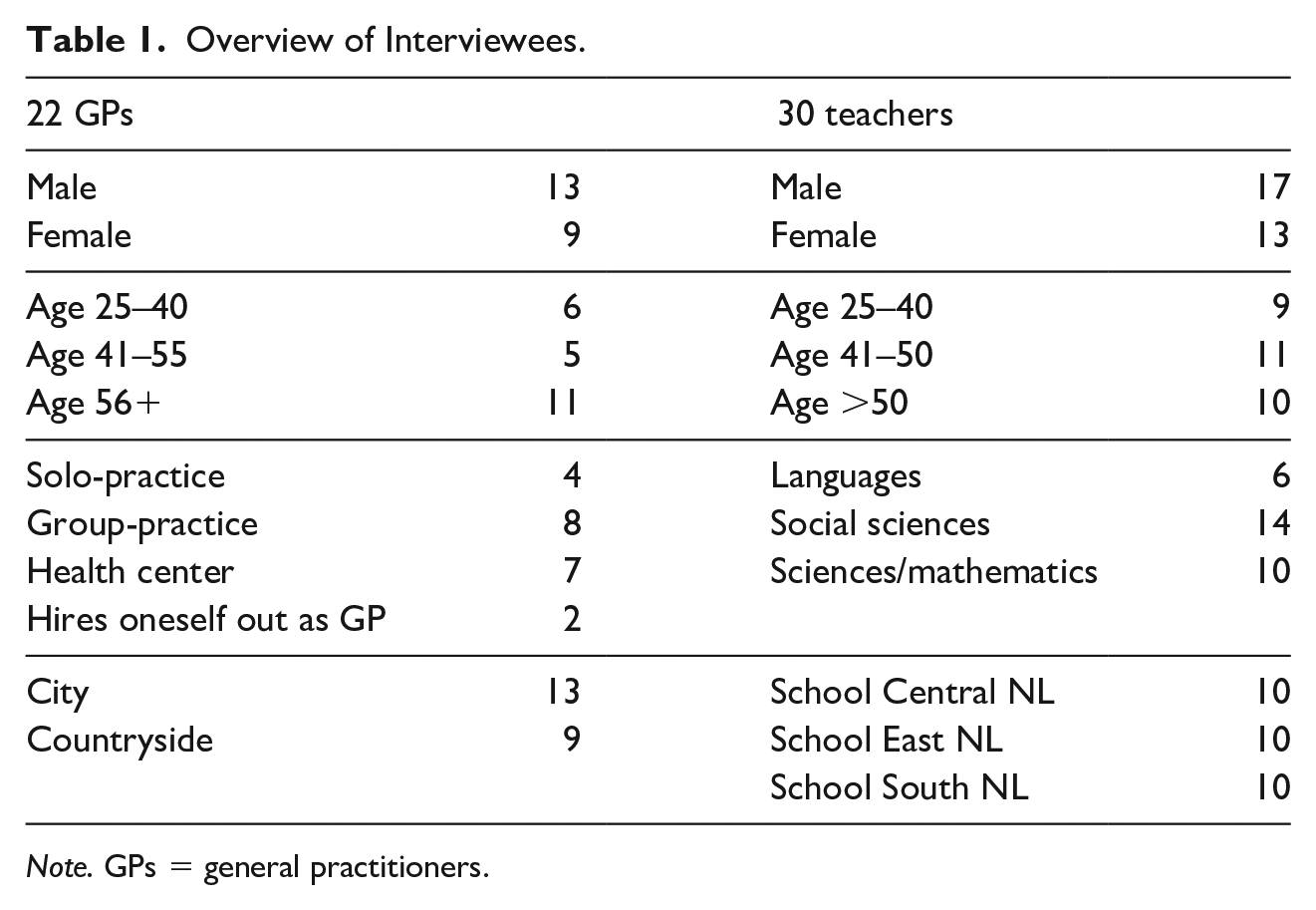
Note. GPs = general practitioners.
Using the coding procedure as described by Robson and McCartan (2016), the data were analyzed in two phases. First, for excellence, ethics, and engagement separately, all statements were labeled with an initial summarizing code. For this, the qualitative data analysis program NVivo was used. Subsequently, these codes were categorized in themes, which was done so in relation to the original data to make sure that these themes kept making sense. Second, the themes were ordered among themselves. Here, the elements of the Good Work framework were related to all the data again to see if statements on excellence also contained notions on ethics for example. Doing so, allowed for a “dialogue” between theory and empirics (Alvesson & Kärreman, 2007). This allowed to gain a deep understanding of GPs’ and teachers’ professional identity in relation to managerial reform, upon which in the following section is reported.
Results
The perspectives of GPs and secondary school teachers on the consequences of managerial reform on their profession are described along the lines of the three values of the Good Work framework—that is, excellence: high-skilled expertise; ethics: the ethical code of providing service in the interest of the client; and engagement: commitment to the profession and the clients. For each element, the most prominent similarity is given, followed by defining differences. These defining differences include the extent to which a professional identity is shared among professionals and underline the importance of professional identity for understanding how managerialism affects professions.
Excellence
When it comes to professionals’ expert knowledge and skills, GPs and secondary school teachers both argue that the core of their expertise has two sides and that managerial role expectations place a unilateral emphasis on one of them. The two sides involve a “technical” side comprising medical knowledge for GPs and subject knowledge and didactics for teachers, and a relational side that is perceived a prerequisite for good professional practice. GPs and teachers alike perceive they must be “socially sensitive” for the personality, mood, context, and history of their patients, respectively their students, to establish constructive relationships in which proper curing or learning can take place. They thus emphasize that the “technical” or “substantial” part of their role and the relational element are closely intertwined. As a teacher explains: “The teaching profession has two components I value equally: being knowledgeable and passionate for a specific subject on the one hand, and pedagogy, flexibility and the social on the other.” (T30). In a similar vein, a GP views both sides equally important for being an excellent professional: “When patients are satisfied about your medical practice as well as your communication and trust, I believe you are doing a good job as a GP.” (G18).
Respondents of both professions however argue that current role expectations—based on managerial reforms—solely focus on the more technical sides of their professions. The consequence of managerialism for their profession is illustrated by a teacher: “Government constantly tries to steer education as if it were a company: managing for results, benchmarking central exam results, all those things that come over us from the ministry.” (T19) In parallel, GPs emphasize that the consequences of managerialism on their profession do not correspond with their self-image. As a GP says: “When you measure whether a GP performs well, you should not only look at medical practice. There are so many factors in GP work that are valuable, but unmeasurable!” (G1).
Both GPs and teachers argue they feel deeply involved with the well-being of patients, respectively, the personal development of students but emphasize that managerial reform led to a strong result-oriented practice. Within this reality, respondents experience the delicate process of carefully crafting personal relationships that serve as prerequisite for patient curing and student learning to be marginalized. For example, while it might be efficient to transfer more simple tasks to lower-ranked assistants, it does undermine the effectiveness of professional care. A GP illustrates the opposite effect, saying: In a business-like way it is being decided that simple tasks can be done by someone else so you can do the difficult things. However, you can only do difficult things when people trust you. I think this [transfer] is very dangerous because it jeopardizes the relationship with the patient. (G8)
The emphasis in managerial reforms on “results” often goes along with increased time pressure. Despite the obvious differences between GPs and teachers with regard to the nature of their respective professional services, both kind of professionals express their concern for not being able to invest as much time as they should—based on their self-image—in building individual relationships with patients and students. A teacher illustrates this concern, saying: When I teach to 11 classes, so more or less 300 students, I will signal something problematic that needs my attention with 10 percent of them. Well, that implies 30 students spread over those classes with whom I should have a little chat or for whom I should make extra materials and that’s hardly possible. (T1)
Managerialism and the related focus on results and time pressure thus leads to lowering professional excellence, in the perception of both groups of professionals.
A defining difference between respondents from both professions with regard to excellence lies in the degree of homogeneity of professional knowledge. For GPs, the medical guidelines formulated by their own scientific association offer a shared knowledge base and define their expertise in shared norms of what to do when faced with a specific medical complaint. A GP proudly explains: “We have medical guidelines defining best practices on how to deal with specific problems written by the profession itself. Now that is professional!” (G1). For teachers, their professional knowledge base is much more fragmented. They teach different subjects, ranging from languages to sciences, which leads to different didactics that come along with each subject. Moreover, already in the 1990s Dutch government has started to determine specific educational goals for each subject. One teacher’s remarks are illustrative for this diversity and the consequences for educational innovation this brings along: We [mathematics teachers] cannot vary endlessly. For languages, you have oral, reading and writing skills, but we don’t have that. It’s frustrating because we try to come up with innovative work forms, like group work, presentations, and papers. But while these are very normal work forms for other subjects, they are not for mathematics. (T25)
In our study, GPs thus seem to have a much more shared self-image of their professional knowledge compared to teachers, also having a stronger ownership of what counts as excellent.
Ethics
With regard to ethics, the data show that both GPs and teachers attach great value to deliver public services in the best possible interest of their clients. Yet, they argue that with measures for treatment and accountability based on managerialism, serving these needs has become a challenge. They believe that patients and students often simply do not “fit” the standardized boxes used for treatment and teaching, leading to unequal cases being treated equally. A teacher explains how students with similar grades cannot be treated as if they are on the same level without taking the differences in assistance—for example outside school trainings—into account (T5). Grades therefore do not tell the whole story in the perception of teachers, implying that without context information, teachers feel they cannot fulfill their professional role in correspondence with their self-image. Managerialism also requires GPs and teachers to act as prudent followers of predefined procedures to improve the output of their services, measured in standardized ways. Both groups of professionals in our study emphasize there is little room and time left for tailor made processes, as requested by the needs of their patients or pupils. The pressures for more standardized treatment therefore also affect professionals’ perception of the degree of ethics in their role. As a GP points out in reference to a lack of context information in interpreting lab results: “It is not taken into consideration whether someone is 19 or 89 [years old], but just whether a certain value in the lab is below 2.5. It makes me wonder: what the hell are we doing?!” (G11).
Ethical codes are however not similar to GPs and teachers; each group has a different way to explain what “good” means for serving their patients’ or students’ interests. Unlike the teachers, the GPs in this study have a shared idea of how to serve their clients’ interests, based on a reference to their professional ethical code and professional association. In other words, they seem to have a relative strong self-image for ethics, and their professional community plays a key role in articulating professional values and facilitating collective sharing. As a GP illustrates: “Ethics is conscientiously delivering decent work. (. . .) Working in good faith with your patient and our Hippocratic Oath puts that to words nicely.” (G2). Secondary school teachers on the contrary are less confident about professional ethics. When being asked for their ethical standards as a professional, they mention the mission and vision formulated at school board level or their own gut feeling. They make almost no reference to their professional community. One teacher illustrates the difference with GPs with regard to ethics and displays a relatively “weak” professional self-image that seems to hamper professional role execution: GPs have had to study that much more. For us, it’s much more intuitively knowing what is right and what is wrong. I have colleagues who give penalties to kids constantly for misbehaving, while others never do that. (. . .) I have very little to hold on to. Our principal is too little involved. (. . .) I sometimes miss direction and clarity. (T2)
GPs thus seem to have stronger shared and established ethical codes than teachers do in our study.
Engagement
Turning to engagement, both GPs and teachers in this study unanimously argue that managerial reform has posed challenges for their professional engagement with their clients and with their profession. With regard to engagement with their clients, GPs and teachers argue that it is part of their professionalism to actually “see” a patient or a student. This means that they feel they need to know the ins and outs of a person and follow their development, whether it be in health or education. A teacher emphasizes: “You need to have a sincere interest in those kids. You need to really like those kids. And you need to keep seeing them as individuals and not as a group.” (T27). Similarly, a GP explains that engagement means knowing your patients: “You need to have a caring feeling for your patients in a professional way. So you need to feel that responsibility.” (G12). Both professional groups thus have a self-image that they need to be engaged with patients or pupils. Moreover, both professional groups share that this self-image is under pressure due to time constraints, whereas all respondents argue that there is little time to build this kind of relationship with their students respectively their patients.
With regard to engagement with their profession, GPs and teachers argue professionals have a responsibility to invest time in keeping up to date with the state-of-the-art knowledge in their respective fields. They also think they should contribute to their professional community and be opinionated about the new developments for their profession. As a teacher describes her feeling of engagement: “Engagement in education means that you follow the discussions, that you read about it, that you know what is going on.” (T4) Comparably, a GP says: “Everybody stands for our profession—whatever that may mean, we stand for it. (. . .) There is a big feeling of solidarity.” (G17) In this way, both emphasize the responsibility you have as a professional to be involved.
However, for engagement with their profession we also find an important difference between the two professions. While GPs claim they are strongly involved in advocating and serving their profession’s interests, teachers complain that they are “too passive” in this. They argue they should stand up for themselves on a collective level and serving their professional community, but in reality, most teachers admit they do not. One teacher criticizes this attitude: “When we are granted more professional leeway, even then I see many teachers saying ‘we have more leeway,” period. But they don’t actually take it! (. . .) People do not claim that ownership. If a board member says “we all turn left,” then 95 percent will turn left while 80 percent of them thinks “I don’t want to turn left, but I’ll just do it.” (T24)
Teachers thus seem less inclined to organize themselves and to stand up for their own profession compared to GPs.
In sum, against the background that both professional domains are impacted by managerialism, this study finds many similarities demonstrating the consequences of managerial reform on professional identity, where both professions seem to lose grip on keeping up traditional professional values of excellence, ethics, and engagement. However, simultaneously this study’s findings highlight important variations between GPs’ and teachers’ professional identity that helps to explain this the observation that managerial reforms have impacted secondary school teaching in the Netherlands earlier and stronger than Dutch general practice. In particular, these variations revolve around the degree to which their self-image is shared among peers and the importance of their professional community for this collective sharing. The next section discusses these findings in relation to literature on managerial reform and professional identity.
Discussion
Based on a qualitative research strategy including semistructured interviews with professionals across two sectors, this article sought to answer the following research question: What are the consequences of managerial reform across two domains within one national context and how can we explain similarities and variation from a professional identity perspective? The case is comparing the reforms and their relevance for the professions of GPs and secondary teachers in the Netherlands. Using a theoretical framework combining literature on managerial reform and professional identity, it systematically compares both domains and professions, unraveling the consequences that have contributed to sectoral variation and offering leads for more effective policy design and implementation by improving the fit between reform and professionalism. This article’s contribution to literature on professionalism in relation to managerial reforms is twofold.
First, going beyond the in literature well-described pressures on professionalism by managerial reform (Freidson, 2001), by focusing on professional identity, the analysis of this study reveals that a specific aspect of professionalism is key here: the necessity to establish a personal relationship between professional and client. Although the nature of their professional services differs, both GPs and teachers often fulfill important roles in the lives of their patients and students. Not just by curing and teaching but by providing moral and social guidance in situations where their clients are vulnerable, for example, in situations of serious illness, or deeply problematic situations at home. Where policy makers and public managers often focus on the “hard” and “technical” quality of professional work (Klenk & Pavolini, 2015; Newman, 2013), this study shows that professionals have a different take on what the quality of their work actually is—or at least should be. It shows that professionals prominently value the social side of professional work as crucial precondition for professional service delivery. Therefore, while managerialism aims to increase the quality of professional work, it seems to fall short in recognizing what this quality actually entails, with professionals themselves arguing that the results of their services will be better in case they can pay more attention to the social sides of their professional work.
Second, this study contributes to our understanding of exactly how and why the consequences of managerial reform vary across professions. Where secondary school teaching has been much more prone to external meddling, allowing successive Dutch governments to decentralize responsibilities to school managers—thereby encapsulating teachers ever more strongly in an organizational setting—and define educational goals, GPs have mitigated processes of managerial reform much stronger and longer. By moving beyond the common focus on a single profession or explanations derived from different national contexts (Adams, 2015; Mauri & Muccio, 2012), this study explains this sectoral variation based on a systematic analysis of how professionals themselves define the main values of professionalism—that is, high-skilled expertise, ethical codes, and engagement to the profession. Compared to GPs, secondary school teachers turn out to have a more heterogeneous understanding of what “good teaching” entails: not only their knowledgebase is more fragmented and controversial, also their ethical standards are less clearly established and their engagement with their professional group is less activist by default. Being more and more “managed” by their school organization seems to intensify this heterogeneity among teachers.
The analysis thereby reveals that how professions are affected by managerialism is related to having a “stronger” or a “weaker” professional identity. This “strength” of professional identity depends on one hand on how clearly professionals are able to define what these main values mean for their profession, and on the other hand on the extent to which these definitions are shared on a collective level. Professional communities play a key role in articulating professional values and facilitating this collective sharing (Barbour & Lammers, 2015; Pratt et al., 2006). The more professionals are subsequently able to articulate a shared identity, the less prone they are to external influences defining the output of their professional service delivery. Therefore, when studying policy design and implementation processes, one needs to go beyond focusing on professional practices and roles (Hendrikx & Van Gestel, 2017; Brodkin, 2011) but needs to reach into the realm of professional values and identity.
When reaching into this realm, this study’s main implication for policy makers and scholars interested in the field of public administration and implementation by professionals is that more empirical and theoretical attention needs to be devoted to professionals’ own definitions of good professional work. Although they are seldom recognized as such (Meyer & Hammerschmid, 2006), public management reforms are inevitably “identity projects,” whereas they affect professional roles and require professionals to re-relate their self-images to these new roles. Literature on professional identity shows that successful identity change requires a careful process of identity reconstruction, in which professionals are slowly but steadily guided toward internalizing new role expectations into their self-images (Reay et al., 2017). However, this study’s usage of the Good Work framework to explore professionals’ identity has made clear that in the eyes of professionals themselves managerial reforms have fallen short in recognizing what professionalism for GPs and teachers is all about: the combination of high-quality work and social relationships. Taking into account professionals’ identity in processes of policy-making, for example, by reflecting together with professionals on what they believe public policies mean for their professional work, holds potential to ensure a stronger “fit” between public management reform and professionalism.
Limitations and Future Research
It should be noted that based on its qualitative data set, strong generalizing claims about professionals in general cannot be made. However, aiming for transferability and comparability rather than statistical generalizations (Robson & McCartan, 2016), the setup of this study and its 52 semistructured interviews allowed for an insightful and systematic comparison across professions within one national context. Rather than “measuring” professionals’ identity with fully predefined categories, using the Good Work framework allowed for professionals themselves to define what the professional values of their identity are all about, making visible the difficult struggle between managerial role demands and professionals’ self-image. It hence revealed that while managerial reforms do lead to important role changes, these changes are not automatically incorporated into professionals’ identity, putting professionals in a complex situation in which they need to deal with multiple and often competing demands. Building on Reay et al. (2017), for future research, this brings up questions, for example, about how public management reforms can make sure professionals’ identities change along with the role changes they aim for. However, also questions that are more fundamental are relevant. Instead of just adding new role expectations, on a societal level, we need to answer what roles we want our professionals to fulfill, what kind of people they need to be, and what capacities they need to have? Are they for example moral agents (Zacka, 2017)? Or do we want to limit their professional leeway to keep a firm grip on professional service delivery?
Moreover, with regard to the professionals in this study, additional research is recommended to see if its findings translate to professionals from other levels and professions, for example, teachers in primary school or university, or medical specialists. Literature gives strong grounds to expect this to be the case (Reay et al., 2017; Shams, 2019; Van Hulst et al., 2016), but since sectoral variation is one of the main claims of this study, additional comparisons are recommendable. Furthermore, this study opens up the research possibility for international comparison (Adams, 2015). Literature shows that the managerial reforms share many similarities across countries for medicine (Cloutier et al., 2016) as well as for teaching (Day, 2007; Schimank, 2015). However, the question remains whether managerialism affects the professional identities of GPs and teachers elsewhere in a similar vein as described in this study, or whether new mechanisms can be discovered. This could provide insight into the influence of institutional characteristics like administrative culture (Pollitt & Bouckaert, 2017) and institutions in the field on the content and shape of managerial reforms.
Conclusion
This study reveals that managerial reform has affected two professional domains in one single national context in both similar and different ways. Both professional domains went through managerial reforms aimed to strengthen efficiency and effectiveness. Looking at the perspectives of professionals themselves on the three values we distinguished in professional identity—excellence, ethics, and engagement—we can conclude that professionals experience a discrepancy for each of them between the new managerial role expectations and their professional self-images. Where managerialism only stresses the importance of the technical sides of professionalism, professionals themselves argue that the relational side of their professional service delivery is at least equally important and even a prerequisite. Nevertheless, besides these differences, managerial reforms in the two domains differed in timing and consequences. Where teaching was prone to more constant change from the mid-1980s onwards, putting them in an ever more executive role; for GPs it took up until mid-2000s before managerial reform changed their practice considerably with the introduction of a market-oriented system in Dutch health care. This appears to be partly due to the degree to which professionals were able to articulate their self-image for each of the three values and subsequently the degree to which these definitions where shared on a collective level for which the organization of the professional community is crucial. Although more empirical work into other professions is recommendable, this study’s findings suggest that this “strength” of professional identity mediates the consequences managerial reforms have on professions, allowing professions whose members have a “strong” professional identity to retain more control over the output of their professional services than those with a “weak” professional identity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.