
Abstract
While a number of studies have argued for a relationship between military morale and military effectiveness, analyses of the sources of morale have overlooked the possible role of military medicine. We suggest that military medicine may be an important predictor of morale. We assess this claim via an observational survey of U.S. military veterans and a survey experiment of active-duty U.S. military personnel. We find a statistically significant relationship between confidence in military medicine on one hand and morale on the other, especially for respondents who have seen combat.
Morale is frequently discussed as a key component of military effectiveness. In the early months of Russia’s 2022 invasion of Ukraine, for example, poor performance by Russian troops was attributed in part to low morale (Dickinson, 2022). Famously, Xenophon attributed battlefield victory to whichever army was “stronger in soul.” Reflecting on his service in World War II, U.S. General George C. Marshall wrote, “You can have all of the material in the world, but without morale it is largely ineffective” (Office of the Chief of Military History, Department of the Army, 1964, p. 38). But what, exactly, contributes to military morale remains somewhat murky. 1
We identify combat medicine as a key predictor of military morale. Good medical care increases the odds of survival. Therefore, soldiers who believe they will receive good medical care if they sustain an injury should, in theory, exhibit higher levels of morale than soldiers who do not believe they will receive good medical care. Related, military personnel who believe that good medical care is accessible to their unit should exhibit higher levels of morale because they care about the health and well-being of their fellow soldiers. More indirectly, better medical care is likely to improve the odds that a unit can stay together; unit cohesion also has been shown to correlate with higher morale (Gal, 1986; Vaitkus & Griffith, 1990).
We assess the relationship between military medicine and military morale using two related strategies. First, we surveyed U.S. military veterans. Second, we conducted a survey experiment of active-duty U.S. military personnel, prompting respondents with various scenarios regarding the quality of military medicine before asking them about their morale. To our knowledge, ours is among the first systematic examinations of the relationship between military medicine and military morale.
While somewhat mixed, our findings suggest an overall positive relationship between military medicine and morale. Among veterans, respondents who rated accessibility and quality of medical care in their unit highly consistently demonstrated significantly higher morale than respondents who gave poorer ratings to military medicine. Our full sample of active-duty military personnel did not generate responses that suggest a treatment effect of additional information on the quality of military medicine. When focusing on active-duty service members who have seen combat, however, we again observe a positive relationship between military medicine and military morale, an effect replicated in the survey of veterans. The relationship between medicine and morale is clearly conditional upon combat, likely because combat exposure heightens an understanding of the importance of medicine. Being in harm’s way, in other words, makes people realize how important it is to mitigate those harms.
The remainder of this article proceeds in five parts. First, we provide a brief literature review of military morale as a foundation for our main argument on the relationship between military medicine and military morale. Second, we discuss our two-part research design, including details of the two surveys underlying this article. Third, we present our results on the veterans and active-duty surveys. Our discussion and conclusions follow.
Morale and Medicine: Theory and Overview
Investigating the relationship between military medicine and morale requires a definition of morale, as well as understanding prior scholarship of the causes and consequences of morale. The inherent intangibility of morale makes definition challenging. As Gal (1986) noted in a seminal paper, morale is often conflated with “motivation” at the individual level. Along these lines, a 2008 U.S. Army report borrows from Britt et al. (2006) to define morale as “A soldier’s level of desire, commitment, and enthusiasm for completing a unit mission under stressful circumstances” (p. 162; Department of the Army, 2008, p. 60. Inderjit et al. (2021) also adopt this definition).
Individual morale is sometimes conceived of as a sense of well-being. A 1989 U.S. Army Report on the subject defined morale as: “a person’s mood or state that may be influenced by a host of factors, from caring leaders to dry socks to hot food” (Bartone, 1989, p. 2). Similarly, Ewell (1982) argues that morale is the individual soldier’s sense that “he will be taken care of through thick and thin” (p. 20). More recently, an Army Field manual on Human Resources Support views a soldier’s quality of life as crucial to morale (Department of the Army, 2021).
We view morale as a combination of these two factors. A sense of well-being contributes to motivation. Our conception of mo active-duty women acknowledging experiencing such an erale hews closest to that articulated by Manning (1994): “enthusiasm and persistence with which a member of a group engages in the prescribed activities of that group” (p. 4).
Identifying the sources of military morale is a similarly vexing task. We argue that better military medicine should improve morale and motivation through three key mechanisms. First, better military medicine lowers an individual soldier’s risk of death or even long-term injury and illness, which should improve morale. In this way, medicine contributes to a sense of well-being.
Second, knowing that one’s comrades will be well taken care of if injured or sick also should improve morale. Here, the notion that unit cohesion improves morale (and vice versa, in a sort of feedback loop), is crucial. Knowing they will be well-cared for in case of injury should improve morale and the will of soldiers to follow orders and fight. In their assessment of wartime medicine, a group of World War II U.S. military doctors wrote: It means a great deal to find that within the combat team with which [a soldier] is so deeply identified, there are members [doctors] whose job is care and protection. At a moment which his identification with his unit is in jeopardy, this is of great importance, and helps to maintain his sense of unity with his group. All of this has a significance to the soldier on every psychological level (Bartemeier et al., 1946, p. 491).
Conversely, soldiers who suffer disease and untreated injury often experience a loss of morale and motivation. Journalist A. J. Venter (2013) describes how Portugal’s poor medical capabilities in its wars in Guinea, Angola, and Mozambique in the 1960s and 1970s may have degraded the morale of Portuguese troops (p. 399). Sagala (2006) discusses the British expedition in Italy in WWI, when desertion was an issue because illness and other frustrations lowered morale (Oram, 2002). Harrison (2004) affirms that “the campaigns in North Africa and Italy demonstrate clearly the connection between health, discipline, and morale” (p. 129). Note, here, that there is mutual causality—undisciplined soldiers are less likely to follow hygiene and health guidelines, which increases the rates of diseases (Harrison, 2004, pp. 193–194). In this sense, medicine and morale are mutually reinforcing.
Third, existing studies have demonstrated a positive relationship between unit cohesion and morale (Vaitkus & Griffith, 1990); by keeping more soldiers in the fight, military medicine contributes to the maintenance of unit cohesion and, by extension, to military morale. A large body of research argues that group cohesion increases the effectiveness of troops and that soldiers fight primarily for their “buddies” (Ambrose, 1995, 1997, 2001; Chaco, 2001; Ellis & Hastings, 1980; Little, 1964; Marshall, 1947; Stouffer, 1949; Wong et al., 2014. For a contrasting view, see Kier, 1998). Shils and Janowitz (1948) argue that the key to why one fights or surrenders is the social cohesion of the primary group. Cohesion is affected by the existence of an ideological “hard core” of soldiers who are models to others, a community of shared experience among soldiers, constant spatial and interpersonal contact among soldiers, thoughts about one’s family, the maintenance of basic physiological needs, and the relationship with superiors.
Military medicine can affect group cohesion in several ways. First, because better military medicine increases survivability, it preserves military units, ensuring prolonged contact and shared experiences. Second, military medicine prevents erosion of soldiers’ morale as a result of the death of close friends. Third, military medicine ensures physical survival; according to Shils and Janowitz, fear of death can sorely undermine the importance of the primary group. As they note, Concern about food and about health always reduces the solidarity of a group. Throughout the war, and until the period just before the end, German Army medical services were maintained at a high level of efficiency; the decline in their efficiency coincides with the deterioration in the morale of the men (Shils & Janowitz, 1948, p. 291).
This final point follows Chaco’s (2001) claim that “analysts overlook the importance of survival when examining soldier motivation” (p. 62). This logic echoes Maslow’s (1998) hierarchy of needs: people attempt to fulfill basic physiological needs first before addressing other requirements.
Based on this logic, our primary hypothesis is:
Research Design
Morale is a challenging variable to analyze systematically. Because it has such a strong emotional aspect, the most logical approach is to survey those whose morale is being assessed. We focus on two populations: U.S. military veterans and U.S. active-duty military personnel. While veterans are an easier to reach population for survey purposes, surveys of veterans will necessarily be retrospective. Surveying active-duty military personnel, on the other hand, provides important opportunities for improving causal inference via survey experiments; however, active-duty military personnel are a challenging population to survey. Below, we discuss our measures of military morale, survey design, and recruitment strategy.
Measuring Morale
We use the Combat Readiness Morale Questionnaire (CRMQ) to measure morale. First used in studies of the Israeli Defense Force (IDF) in the 1980s, the CRMQ has since been used in several studies involving U.S. forces (Bartone, 1989; Gal & Manning, 1987; Vaitkus & Griffith, 1990). The CRMQ includes questions that address morale both directly and indirectly. For example, respondents are asked about their personal level of morale and the level of morale in their unit. They are also asked about their confidence in various aspects of leadership, such as the decisions of those higher in the chain of command, and unit cohesion.
Based on the CRMQ, our survey includes questions that facilitate measurement of six components of morale: cohesion, deployment willingness, confidence in leadership, confidence in training, discipline, and motivation. In addition, we ask survey respondents to assess their own morale and the morale of their units directly. These questions are constructed using Likert-type scales that range from 4 to 7 points with possible response values ranging from low or very low to high or very high. Responses pertaining to the components of morale and the direct self- and unit-morale assessments are then combined into an overall measure of respondent morale, which serves as our primary dependent variable. 2 This morale index is constructed by summing responses to questions that measure each of the six components of morale and questions related to direct morale assessments:

The additive Morale Index ranges from 0 to 115, with these values reflecting the lowest and highest possible values of morale. By constructing a measure of respondent morale that incorporates distinct elements that contribute to individual morale, we can better capture variation in different experiences of military personnel during their time in service. For example, this approach allows us to capture differences in morale that would result between a soldier who expressed a high degree of confidence in their training but felt their unit lacked a high level of morale overall.
Measuring Military Medicine
We use the CRMQ as part of two surveys underlying this study. Each survey focuses on a different population. The first survey, focusing on U.S. military veterans, asks veterans about their combat experience and their experience with military medicine before administering the CRMQ morale questionnaire. Our main military medicine-related questions presented to military veterans are:
How would you rate the quality of medical care in your unit?
How accessible was medical care in your unit?
How confident were you in the medical care you would have received if you were wounded on deployment?
Veterans were asked to answer with respect to a combat unit if they had deployed, and to answer regarding the unit where they had served the longest if they had not deployed. Results from this survey are necessarily retrospective and observational, as veterans are reflecting on their past experiences. They are especially helpful in understanding the relationship between military medicine and military morale in past conflicts. Similar to our overall respondent morale index, here we combine responses to these military medicine questions into a single overall measure that reflects veteran confidence in military medicine during their time of service. Therefore, our primary explanatory variable in the veteran analysis is reported confidence in military medicine:

The veterans Medical Index ranges from 0 to 12, reflecting situations where the respondent expressed no confidence in the medical care they could access or receive in their unit or where the respondent felt a high degree of confidence in medical care.
The second, larger, survey focuses on active-duty U.S. military personnel. Here, we use a survey experiment based on the possibility of a North Korean attack on U.S. military bases in South Korea to improve causal identification. The survey experiment includes four arms that vary military medical conditions in an unordered fashion. For example, one arm includes the sentence “Of particular concern is the stress on the military’s medical capabilities, given limited resupply and air evacuation capabilities in the event of an attack.” Another arm states that “the U.S. military has taken important steps to ensure high-quality medical care for any U.S. military personnel injured in such an attack.” The CRMQ is administered after the experimental condition, such that it should measure a participant’s morale conditional upon having read the description, permitting us to compare average outcomes per group to determine treatment effects. Using the two manipulations above as examples, we expect that respondents who are told that the military “has taken important steps to ensure high-quality medical care” will score higher on the morale questionnaire than respondents who are told that the military’s medical capabilities will be stressed due to limited resupply and air evacuation capabilities.
The experimental conditions are based on a wargame held at Air University in October 2017 (Curtis E. LeMay Center for Doctrine Development and Education & LeMay Center Wargaming Directorate, 2018). This tabletop exercise was organized by Air Force medical personnel who were especially interested in how compromised air evacuation could affect medical care in a mass casualty situation. While the United States had air superiority in Afghanistan and Iraq such that policies such as the “golden hour” rule—where wounded military personnel were mandated to be evacuated to a higher-level medical facility within one hour of injury—could be implemented, the likelihood is that future conflicts the United States is involved in may see contested airspace. Thus, casualties would not be easily evacuated. Lingering questions following the exercise referred precisely to issues of morale around understandings of the quality of medical care and the possible use of Chemical, Biological, Radiological, or Nuclear weapons (CBRN). The four arms of our survey experiment thus vary on these dimensions: whether the military medical community is prepared to handle a mass casualty situation absent robust air evacuation and in the presence of CBRN.
As depicted in Table 1, we expect these conditions to yield varying increases and decreases of military morale vis-à-vis the controls and each other.
Active-Duty Survey: Experimental Design.
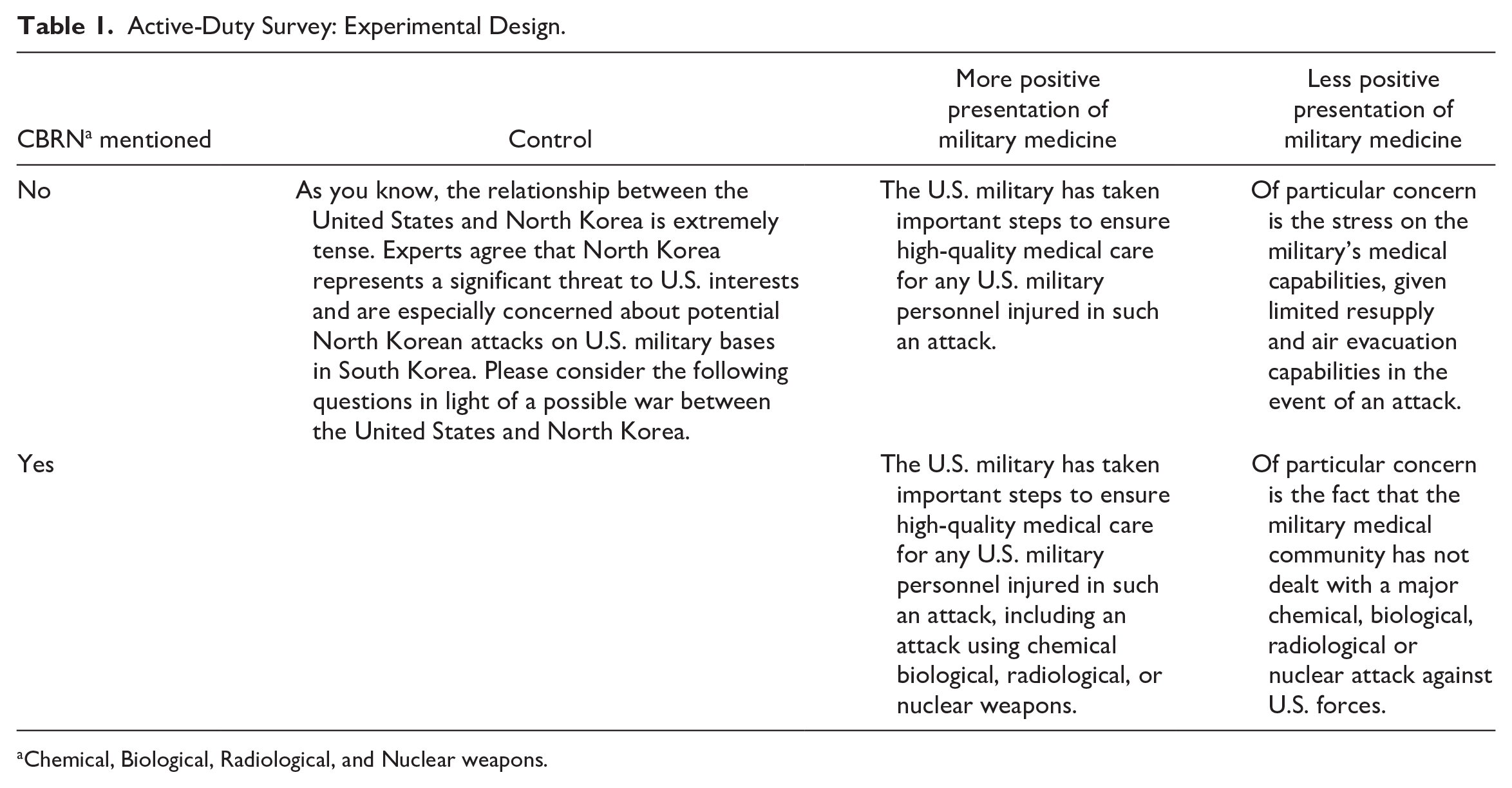
Chemical, Biological, Radiological, and Nuclear weapons.
Recruitment Strategy
Recruitment of military personnel into surveys is notoriously challenging. Both veterans’ organizations and the Department of Defense are understandably reluctant to share contact information for their members. To access these populations, we employed a mixed social media strategy.
Following Neundorf and Öztürk (2021), we recruited subjects for the veterans’ survey primarily via Facebook. Before the start of the survey, we put out a call for focus group participants—both veterans and active-duty personnel—on Twitter; the purpose of the focus groups was to pilot the survey and the Facebook ads. After making revisions in response to the focus groups, we ran the veterans’ portion of the survey from February 10, 2022 until March 2, 2022. Specifically, we published ads on Facebook aimed at the U.S. military veteran population (see Figure 1). We continued the ad campaign until we had achieved a sample of 452 veterans who completed the survey and were representative of the U.S. veteran population. 3
Facebook Advertisements.
We employed a similar strategy to recruit active-duty military personnel into our survey. Initially, we adopted the same strategy as used for veterans, except that we directed ads to Instagram as well as Facebook on the Meta platform, given that active-duty military personnel skew younger than the veteran population and younger people are more likely to use Instagram than Facebook. We therefore also turned to two other social media platforms: Twitter and Reddit. The authors tweeted out a call for respondents on Twitter using the #miltwitter hashtag. On Reddit, the authors posted the survey with a call for respondents on the r/marines forum. 4 Note that we did not use a paid advertising campaign on Twitter or Reddit the way we did on the Meta platform. 5 The active-duty survey began on July 23, 2022, and concluded on July 2, 2023, ultimately yielding 1,808 usable responses.
We took several steps to ensure the validity of samples recruited using social media. First, Meta’s advertisement platform offers a variety of highly precise demographic targeting variables that we calibrated to maximize advertisement delivery to users identified as likely members of the military or armed forces residing within the United States. In addition, we invited respondents to share their preferred duty stations during their time of service as a validation check that survey respondents represented actual veterans or military personnel. Finally, for the active-duty portion of the survey we implemented an attention check to screen respondents who failed to identify North Korea as the adversary country in the hypothetical conflict prompt.
Data and Analysis
Given the observational and experimental research designs employed in this study we approach the analysis of morale using two different strategies. For our veterans sample we investigate how a veteran respondent’s confidence in military medicine during their service accounts for variation in their overall total morale using linear regression with controls, including key demographic characteristics and combat experiences.
With our active-duty survey results, we leverage randomization of experimental conditions to avoid issues of confounding, endogeneity, and selection. Because experimental conditions are randomly assigned, they are, by construction, independent of other variables, including the dependent variable. First, we look at the simple morale index in each group, by experimental condition. Second, we run statistical models (ordinary least squares [OLS] regressions) as although confounding will be limited due to randomization of assignment into experimental conditions, demographic variables could influence whether and how someone “takes” the experimental condition, meaning whether they read it, if they understand it, and how they interpret or process it.
Military Veterans
The key independent variable in our analyses of military veterans is the Medical Index. The medical index for veterans ranges from 0 to 12, with a median of 9. Almost 20% of respondents (19.89%) answered 9, making it the mode as well as the median; nearly as many (19.50%) answered 12, the highest possible value. Overall, the data suggest the veteran respondents in the survey had, on average, high opinions of the medical care available to them, with few outliers who express displeasure.
The veterans’ morale index tells a somewhat similar story in that most of our respondents have high morale. The morale index ranges from 21 to 111 with a median of 84. Half of respondents gave scores between 74 and 92. As with the medical index, a small proportion of people give very negative assessments overall, but they are a minority—only 10% of respondents gave an answer below 60.
Table 2 shows the results of linear regressions with complete controls, 6 for the full sample (1), the full sample controlling for which conflict(s) the veteran was in (2), 7 a subsample of only those in combat (3), and a subsample of only participants who were not in combat (4). 8 Regardless of the model specification, the coefficient on the medical index remains positive, statistically significant, and of a similar magnitude. 9 Figure 2 illustrates the relationship between military medicine and morale for a typical respondent 10 using the results of the model with the full sample (Model 1). As the upward slope indicates, increases in the medical index are strongly associated with increases in morale. Substantively, for the sample as a whole, the results indicate that a one standard-deviation increase in the medical index should translate to approximately an 8-unit increase in morale (just over half a standard deviation in morale).
Linear Regression Results for Veterans’ Survey.
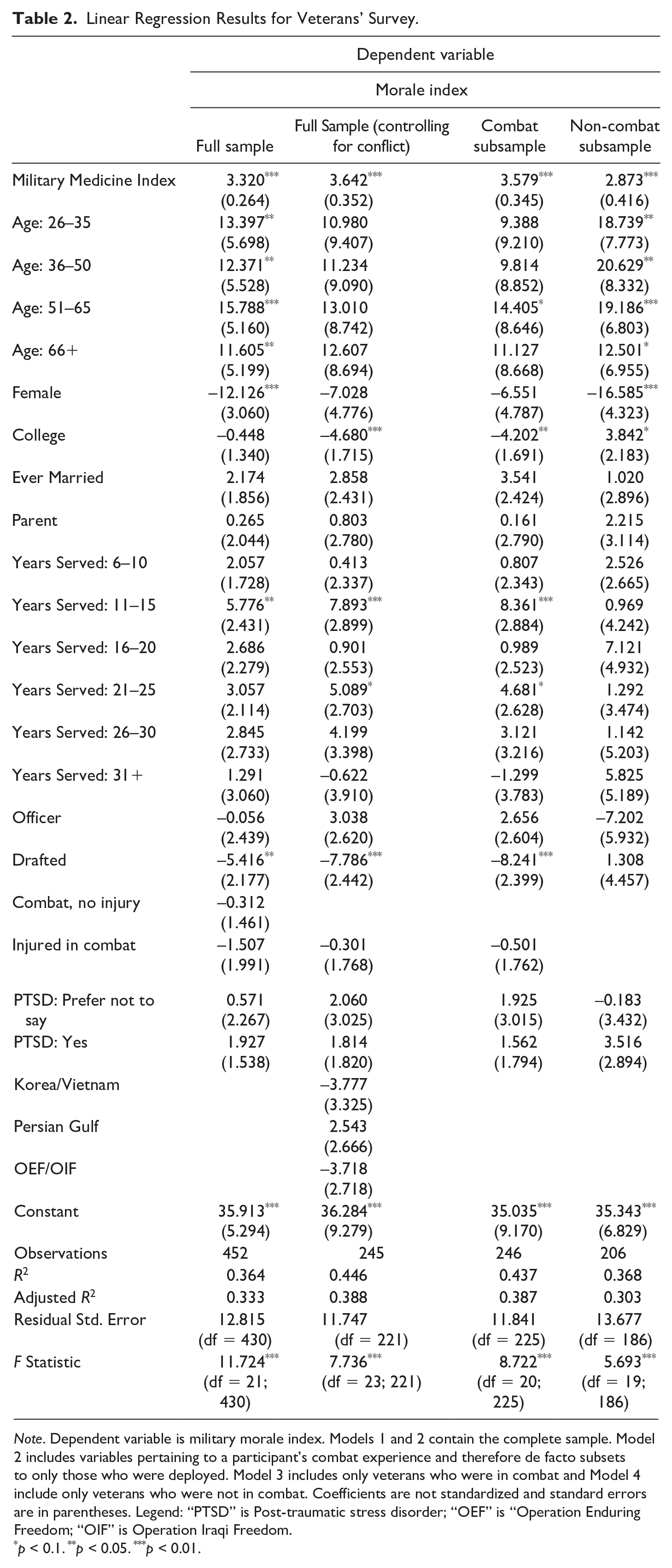
Note. Dependent variable is military morale index. Models 1 and 2 contain the complete sample. Model 2 includes variables pertaining to a participant’s combat experience and therefore de facto subsets to only those who were deployed. Model 3 includes only veterans who were in combat and Model 4 include only veterans who were not in combat. Coefficients are not standardized and standard errors are in parentheses. Legend: “PTSD” is Post-traumatic stress disorder; “OEF” is “Operation Enduring Freedom; “OIF” is Operation Iraqi Freedom.
p < 0.1. **p < 0.05. ***p < 0.01.
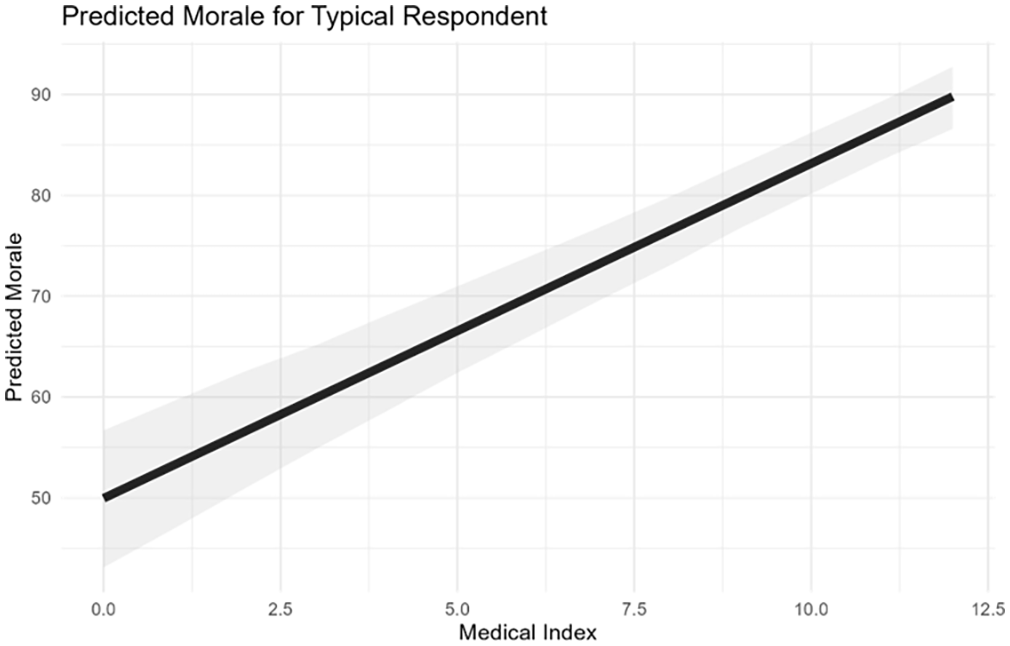
Predicted Morale Index Based on Table 2, Model 1, for the Modal Veteran Respondent.
In addition to consistent evidence of a positive association between military medicine and morale, we find strong patterns among the demographic variables. Older veterans and those who served longer usually have higher morale, on average, although the coefficients are not always statistically significant, and female veterans and those who were drafted have lower morale. When we split the sample into those who were in combat (Model 3) and those who were not in combat (Model 4), under the intuition that those who were in combat may have systematically different experiences in the military, and therefore may have experienced military medicine differently or have systematically different morale drivers, we still find a positive and statistically significant association between military medicine and morale in both groups. The only difference we see when we split the sample is that college education is associated with lower morale among those who were in combat, but higher morale among those who were not in combat, which results in a canceling effect in the aggregate sample.
Active-Duty Personnel
The advertisement campaign successfully recruited 1,808 active-duty military personnel who completed all relevant questions and passed our attention check. 11 Overall, active-duty personnel scored considerably lower than veterans on the morale index, with a mean morale index of 68.43. This difference may stem in part from the veteran population’s being older and longer removed from their time of military service; this distance might result in higher assessment of their time in service. Our analysis of veteran morale suggests a non-linear relationship between age and morale with morale increasing with age up to a point.
Recall that active-duty military personnel were asked to consider a hypothetical scenario about a conflict between the United States and North Korea. As described in Table 1 above, some personnel were given prompts which suggested that the military medical community would be well prepared to deliver care absent air evacuation or in the presence of CBRN, whereas others were told that the military medical community would be ill-prepared to deliver care in these circumstances.
Figure 3 is a boxplot reporting the median and quantiles of the morale score by experimental condition group. Remarkably, the medians of all five groups are all within a 1-point range on a 115-point scale (69, 69, 69.5, 70, and 70, respectively). This finding is affirmed by the results of linear regressions (Table 3), which show no identifiable association between the experiment arms and morale in the complete sample (Model 1). 12 We also see differences between the veterans and active-duty samples in the effects of demographic variables. Whereas among veterans, older veterans typically report higher morale, older active-duty participants report somewhat lower morale, although the age distributions are different, with most veterans being 66+ and most active-duty service members being 25 or younger. Female service members, like female veterans, report lower morale on average than their male peers. Married service members report lower morale on average, and time in unit is also associated with lower morale. Having been in combat is associated with higher morale.
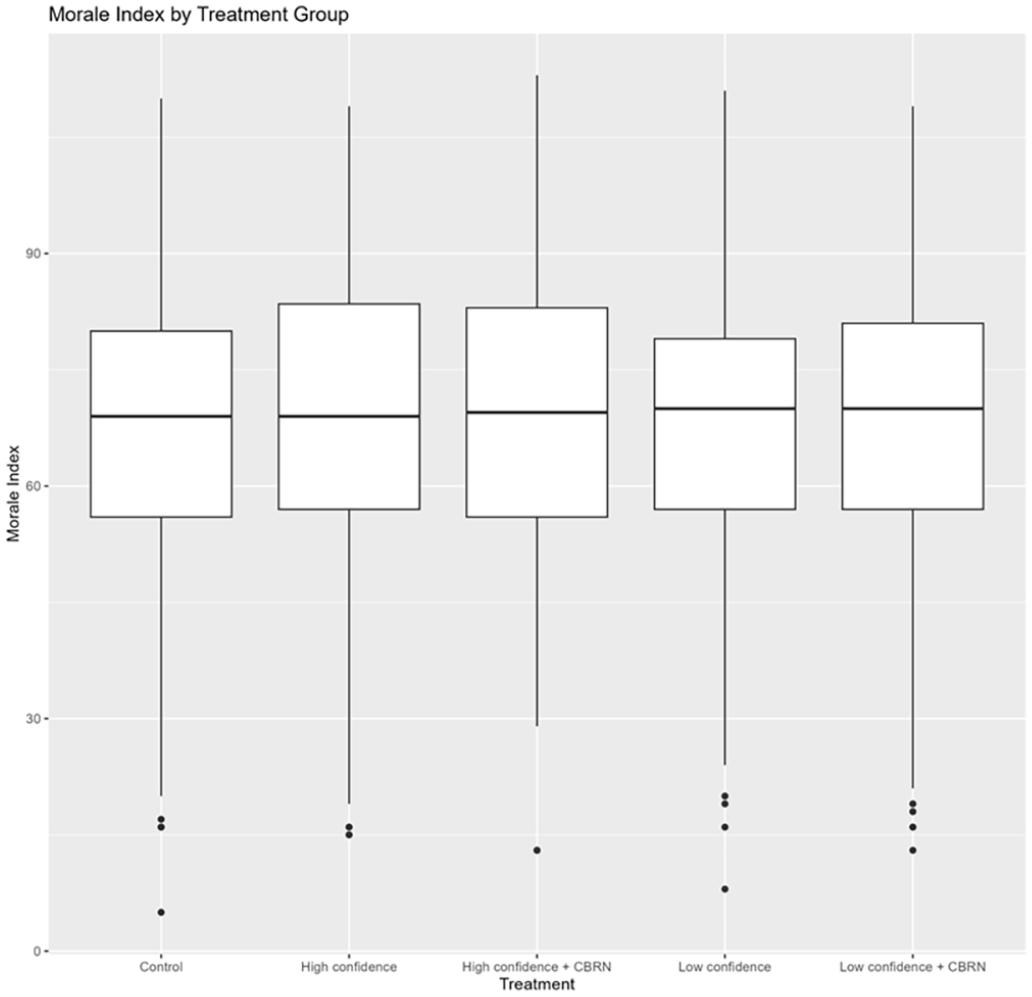
Boxplot Illustrating the Distribution of Morale by Experimental Condition.
Results of Linear Regressions for Active-Duty Survey.
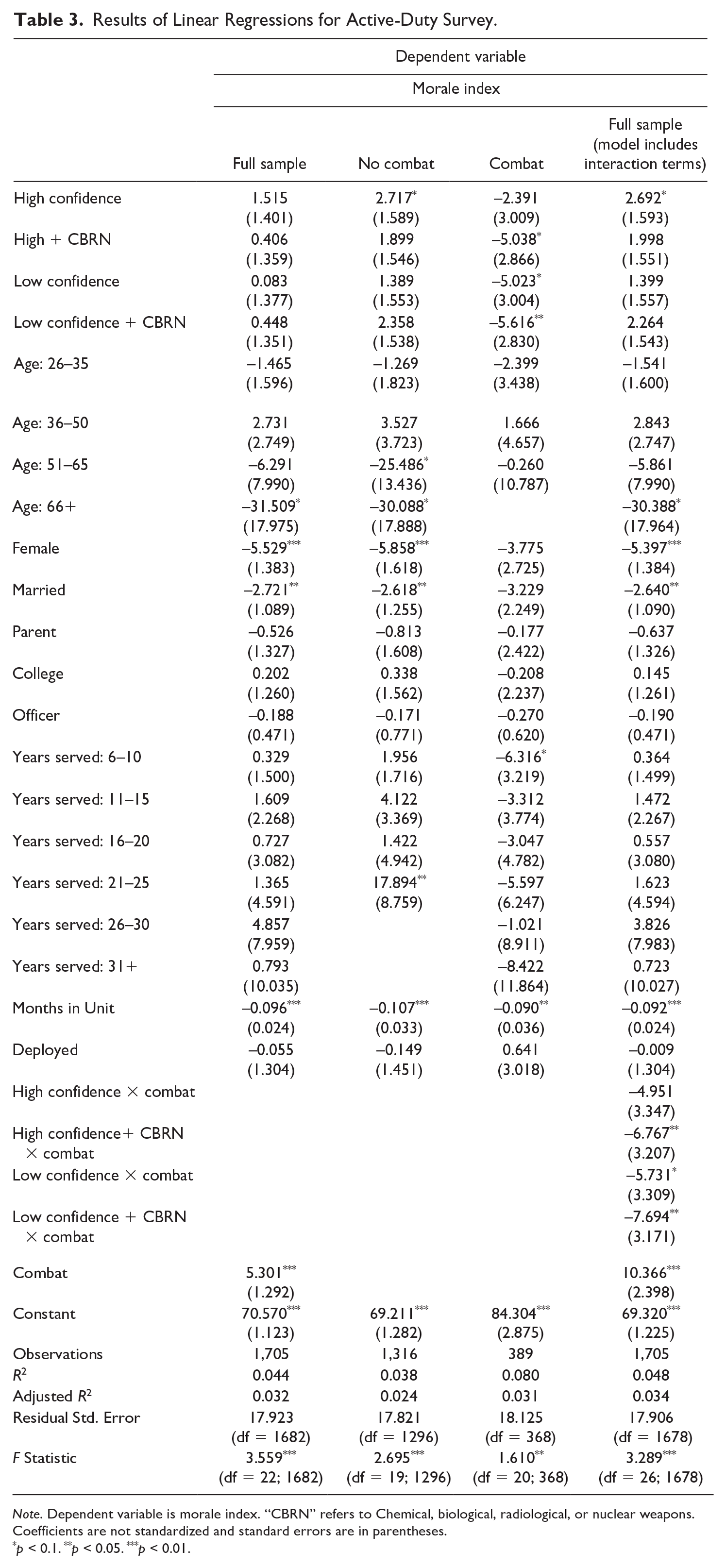
Note. Dependent variable is morale index. “CBRN” refers to Chemical, biological, radiological, or nuclear weapons. Coefficients are not standardized and standard errors are in parentheses.
p < 0.1. **p < 0.05. ***p < 0.01.
While these overall results are inconsistent both with our analysis of military veterans and our overarching hypothesis, further investigation helps explain why. The differences in morale among those who have and have not been in combat is more consequential for the active-duty service members than for veterans. As illustrated by Figure 4, treatment effects are only observed in the combat subsample. Disaggregating our models into combat and no combat subsamples, as in Table 3 (Models 2 and 3) or interacting the experimental condition with a combat dummy (Model 4), demonstrates that, with controls, our null effects in the full sample reflect null effects among most respondents, who have not been in combat. 13 Among those who have been in combat, however, we see effects consistent with our primary hypothesis: experimental conditions that suggest inferior medical care generate statistically significant decreases in morale, at p <.10 for high confidence + CBRN and low confidence, and at p <.05 for low confidence + CBRN. In the interaction model, this gap is illustrated by the negative and statistically significant coefficients on the interaction terms. Because these negative coefficients are larger than the positive coefficients for non-combat participants, this result demonstrates a negative and statistically significant effect within these three experimental conditions. The relationship between military medicine and morale in our active-duty survey is as predicted, but it is limited to those who have been in combat.
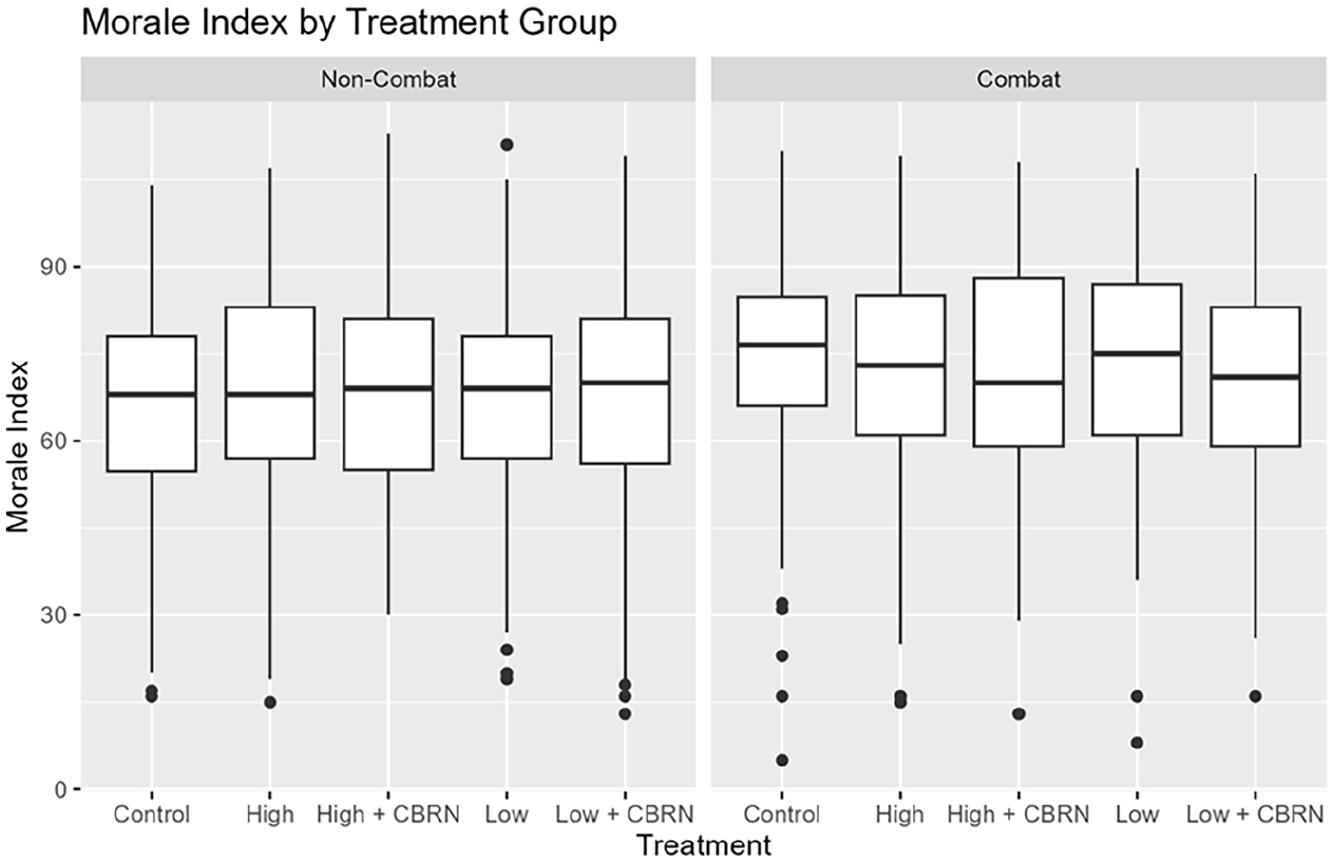
Distribution of Morale by Experimental Condition for Non-Combat (Left) and Combat (Right) Participants.
Discussion
These results raise two main questions. First, why is there a much clearer relationship between military medicine and morale among veterans compared with active-duty military personnel? And second, why does combat experience generate pronounced differences in the relationship between military medicine and morale in both samples?
Two key differences between veteran and active-duty populations can help answer the first question. First, although the survey specifically asked veterans to reflect upon their medical experiences while in service, veterans’ attitudes toward military medicine may be colored by their experiences with medicine as veterans. As Suzanne Gordon (2018) demonstrates, the U.S. veterans’ health care system is significantly more robust and holistic than the broader civilian health care system, which is plagued by insurance paperwork, disconnected service providers, and a constant need for referrals. Second, veterans exhibit higher morale generally than active-duty military personnel. This contrast is likely due in part to the changing composition of veterans. Women, for example, comprise 11% of the veteran population but 17% of the active-duty population. In both the veteran and active-duty analysis, women reported significantly lower morale than men but, again, there are more women in active-duty (proportionately) than in the veteran population. The average time in service has also increased greatly and likely is another depressor of morale. Not only is morale lower for active-duty personnel compared with veterans but, among veterans, morale is lower for those who served in Operation Enduring Freedom (OEF) or Operation Iraqi Freedom (OIF), wars notable for extensive and frequent redeployments.
Second, while there was no effect of our military medicine experimental conditions on morale in the overall active-duty sample, we observed an effect when we split the sample into those who had and had not seen combat. Treatment effects were clearly visible among active-duty military personnel who had been in combat; similarly, the positive relationship between military medicine and morale was more pronounced among veterans who had seen combat. Knowing you might be killed or wounded makes the importance of good medical care more immediate. Those respondents who had not seen combat—perhaps because they were assigned roles farther from danger or served when the United States was not engaged in a major military action—may have been less focused on immediate threats to survival, and the tools available to address them. While our experimental conditions may not have been strong enough to affect morale in the non-combat sample, our results suggest that further research on military personnel who have seen combat is warranted in future explorations of military morale.
Conclusion
Morale is a notoriously challenging component of military effectiveness to understand, measure, and manipulate. Our results show that military medicine is a critical component of morale, especially when it matters most—when troops are in combat. Both among military veterans and active-duty military personnel who have seen combat, there are clear and statistically significant positive relationships between confidence in military medicine on one hand and morale on the other.
These findings suggest pathways for future research. For example, our understandings of military morale often suggest a relationship among individual morale, unit morale, and unit cohesion. Additional research that surveys combat veterans and members of specific military units could help disentangle these threads. 14 Our findings are restricted to current and former U.S. military personnel; replications of this study in other countries could tell us to what extent the positive relationship between military medicine and morale holds outside the U.S. Time series data could also be very informative. This research is limited by the fact that both samples are cross-sections; they capture a particular point in time but do not permit us to understand or evaluate how these attitudes may change over time or how individual respondents may react to changes in their own circumstances.
We also find, in both the veterans and active-duty samples, a strong negative relationship between sex and morale. That women reported levels of morale that were 12 points lower than men in the veterans data and five points lower among active service members is cause for concern and strongly suggests differences in the experiences of men and women in the military that significantly shape their morale. We did not ask respondents about their experiences with sexual trauma. But one possible explanation for lower morale among women in our sample may stem from the persistence of sexual assault within the U.S. military. A recent systematic analysis of active-duty military personnel found that women were more than five times as likely as men to have experienced a sexual assault during the preceding year with approximately 4.8% of active-duty women acknowledging experiencing such an event (Research and Development [RAND], 2015, p. 11). Additional work has attempted to identify reasons for such persistent sexual assault within the military. Wood and Toppelberg (2017), for example, identify socialization processes among recruits and officers as normalizing sexual harassment as a punishment mechanism, which further disincentivizes reporting. Beyond the clear ethical and legal implications of widespread sexual assault in the military, the findings presented here are consistent with the possibility that sexual assault compromises military capacity by undermining morale among servicemembers who experience sexual assault directly, or indirectly such as when an assault happens to a fellow squad member or other servicemember. More generally, it is also possible that women feel they receive inferior health care to men. Both points speak to recent research demonstrating a negative relationship between inequities within militaries and military performance writ large (Lyall, 2020).
In addition to questions around women’s health in the military, this study could have implications for our understanding of the evolving relationship between military personnel’s mental health and morale, as well as the morale of military medical practitioners themselves. With the increasing acceptance of diagnoses like posttraumatic stress disorder, knowing that long-term mental health care is available to them and, further, reducing the stigma associated with receiving such care, could improve morale. This possibility is especially important given the longer-term and different types of deployments U.S. and NATO troops have experienced in recent years (Duel & Reijnen, 2024; Kline et al., 2011). Furthermore, collaboration between the U.S. Military Health System and civilian health agencies during the COVID-19 pandemic through the standup of field hospitals and deployment of naval ships for civilian health care as well as participation in Operation Warp Speed to produce a vaccine in under a year showcased the strength of U.S. military medicine and was a morale booster for those serving and providing care (Koehlmoos et al., 2022).
Policy makers and military leadership desire to maximize the effectiveness of military forces while contending with resource limitations. Military personnel need to know they will receive medical support if injured or harmed while carrying out their duties. Our results suggest that these goals are not mutually exclusive. Rather, to the extent that morale improves combat effectiveness, the results of this study suggest that investments in military medical capacity may serve as a cost-effective force multiplier. In fiscal year 2022, the U.S. Department of Defense (DOD, 2022) allocated approximately 7.3% of its annual budget toward health-related programs for service members through its Defense Health Program (pp. 4–27). As important as the money spent is the distribution of those funds; Congressional reforms enacted in 2016 were meant to reduce spending on military health and outsource to civilian health facilities, an outcome that could greatly undermine the overall quality of military medicine (Zogg et al., 2022). More recently, the U.S. military appeared to have revived its commitment to health care, partly because of the COVID-19 pandemic (Mincher, 2024). To maintain morale, continued investment in military medicine and outreach is warranted. Perhaps most important, military personnel must be informed of, and believe in, the quality of medical care they will receive if they fall ill or become injured in combat. So, in addition to preventive care such as addressing the spread of infectious diseases like COVID-19, the military medical community should publicize its remarkable successes in combat operations in Afghanistan and Iraq. But for the relationship between military medicine and morale to continue to hold, the military medical community should also publicly invest in updating practices for peer/near-peer competition where airspace could be contested, resulting in longer evacuation times. Explaining how the military medical community will address the provision of care in a peer/near-peer competition could have a significant impact on morale. Given the importance of combat experience, however, the strongest effects will likely emerge after operations have begun. Our findings suggest that, to the extent these DOD health care commitments translate to improved military unit health outcomes, military health investments contribute to the U.S. military’s overarching mission by improving military morale and, therefore, military effectiveness.
Footnotes
Appendix A
Appendix B
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors report no conflict of interest. The contents, views or opinions expressed in this manuscript are those of the author(s) and do not necessarily reflect official policy or position of Uniformed Services University of the Health Sciences, the Department of Defense, the Departments of the Army, Navy, or Air Force, the Veterans Health Administration, or the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is pre-registered at OSF, ![]() and funded by the U.S. Army Research and Development Command (Award# W81XWH-20-C-0127). Earlier versions were presented at the 2022 Medical Health System Research Symposium and Annual Meeting of the American Political Science Association.
and funded by the U.S. Army Research and Development Command (Award# W81XWH-20-C-0127). Earlier versions were presented at the 2022 Medical Health System Research Symposium and Annual Meeting of the American Political Science Association.