
Abstract
The high prevalence of military veteran substance use (SU) when compared to their nonveteran counterparts has been described as an urgent public health issue. The commonality of severe mental and physical health comorbidities in this population affects their ability to recover and relates to the onset and maintenance of homelessness. While veteran-targeted housing and SU interventions exist, they are being underutilized. This scoping review synthesizes published peer-reviewed articles from 1990 to 2021 at the intersections of housing, substance abuse, and service utilization by homeless veterans. Qualitative thematic analysis of 119 retained peer-reviewed articles revealed five key themes: (1) the association between SU and housing stability, (2) gendered comparisons with service needs and provision, (3) consideration for comorbidities, (4) social support and relationship-centered interventions, and (5) barriers to health care services. This review offers a series of concerns, outcomes, and recommendations that might be valuable for practitioners, health care providers, and community stakeholders when implementing or re-evaluating new or existing homeless veteran treatment programs.
Keywords
Introduction
Across their lifetime, up to 52.5% of veterans meet the DSM-5 criteria for various substance use disorders (SUDs; Boden & Hoggatt, 2018; Teeters et al., 2017). At any point in time, about 11% of veterans meet the criteria for SUD, which is comparably higher than their nonveteran counterparts (Boden & Hoggatt, 2018). As such, the commonality military veteran’s with SUD has been described as an urgent public health issue (Blakey et al., 2022). Unfortunately, mental health difficulties are also common among veterans and can precede the onset of SUD, maintain them, and hinder their recovery. In a general sample of more than 4 million veterans, 25.7% of them encountered posttraumatic stress disorder (PTSD), a depressive disorder, an anxiety disorder, another serious mental health illness (psychotic disorders and bipolar spectrum disorders), or a combination of these across the last year (Trivedi et al., 2015). Beyond the general population of veterans, in those seeking mental health treatment, almost 80% experience a combination of PTSD, major depressive disorder, or generalized anxiety disorder (Lan et al., 2016; Richardson et al., 2017). The high prevalence of mental health difficulties in veterans is attributed to unique risk factors related to their service duties (i.e., physical combat, traumatic event exposure, geographic dislocation; Tsai & Rosenheck, 2013).
Compared to their nonveteran counterparts, veterans experience a higher incidence of homelessness despite faring better on sociodemographic factors typically associated with homelessness, such as unemployment, poverty, and access to health care and housing services (Collin et al., 2015). In both populations, homelessness seems to be determined by SUD, mental illness, poverty, and adverse childhood experiences (Metraux et al., 2017; Nichter et al., 2023). However, veterans who report homelessness are more likely to have received an “other-than honorable”/dishonorable discharge or served a short period in the military (Metrau et al., 2017; Tsai et al., 2016). In addition, those exposed to combat are at greater risk of homelessness potentially due to consequences related to combat including trauma, PTSD, and SUD (Metraux et al., 2017; Nichter et al., 2023). Indeed, the combination of mental illness and SUD is the most common and consistent risk factor in veterans becoming homeless (Bowe & Rosenheck, 2015; Dunne et al., 2015; Tsai & Rosenheck, 2013). The insidious combination of factors results in 10% of veterans experiencing homelessness 5.5 to 9 years following their discharge from service (Nichter et al., 2023). The average veteran who experiences homelessness is a 50-year-old male who is single/divorced, unemployed, and has less education (Nichter et al., 2023; O’Connell et al., 2008; Simpson et al., 2019; Tsai et al., 2014). Unsurprisingly, homeless veterans commonly report PTSD, depressive disorders, SUD, as well as serious mental health illnesses (psychotic disorders and bipolar spectrum disorders) (Brenner et al., 2017; Metraux et al., 2017). Sadly, veterans experiencing homelessness have elevated odds of attempting to end their lives across their lifetime (Nichter et al., 2023).
The United States has observed an overall decrease in veteran homelessness since 2010, although recent trends are increasing (U.S. Department of Veteran Affairs, 2024). SUD’s and their related health concerns hinder veteran’s ability to gain and maintain stable housing, making it a primary concern (Dunne et al., 2015; Montgomery et al., 2013). Indeed, these ailments commonly go untreated impeding the successful transition out of homelessness (Creech et al., 2015; Iheanacho et al., 2018). While veteran-focused and addiction-targeted services exist, homeless veterans are more likely to utilize emergency departments (EDs) for assistance (Dunne et al., 2015). Furthermore, housing is seen as essential for addiction recovery, although SUD themselves are a barrier to gaining housing, creating a bidirectional relationship (Betancourt et al., 2023). Together, these compounding factors highlight service gaps for homeless veterans encountering SUD and a complicated landscape for interventions. While individual studies exist to evaluate challenges in providing SUD intervention for homeless veterans, current initiatives would benefit from a synthesis of published research to identify emerging trends and inform new initiatives (Betancourt et al., 2023; Iheanacho et al., 2018; Tsai et al., 2014). This study aimed to conduct a synthesis of peer-reviewed published data over 30 years that discuss the intersection of veteran homelessness, SUD, and service utilization.
Methods
PRISMA-ScR (Tricco et al., 2018) and PRISMA-S (Rethlefsen et al., 2021) were followed for this scoping review. A protocol was not used in preparation for this review. Select published reviews were consulted for overlap but deemed to be sufficiently different, out-of-date, or too niche compared to the intention of this review (Byrne et al., 2013; Lowe & Dybicz, 2019; Mejia, 2020; Weber et al., 2017).
Eligibility Criteria
The criteria used to determine eligibility were as follows and were implemented through search terms as well as limiters (when available) in the databases:
Peer-reviewed primary research journal articles in English—secondary research, such as reviews, were excluded.
Theses and dissertations were included during abstract screening, although they were removed during full-text screening as the review shifted focus to peer-reviewed articles.
Published between 1990 and 2021 (data pulled May 2021)
Geographic focus on Canada, the United States, the United Kingdom, Australia, and New Zealand.
The abstract screening included articles that contained veteran and homelessness terminology in the Abstract and/or Title.
Full-text screening focused on articles that discussed substance use or barriers to health services.
Literature Search and Screening
In early 2021, preliminary work was completed by a social work librarian (A.L.) to assess the necessary scope of search terms and databases for this review, following consultation with the rest of the research team and drawing from other published methodologies (Aubry et al., 2020; Munthe-Kaas et al., 2018). The search terms and configuration were kept intentionally broad in order to attempt to locate all resources on this topic. The same approach was employed in selecting the databases, with the team settling on the Sociology Collection (databases: Applied Social Sciences Index & Abstracts [ASSIA], Sociology Database, Sociological Abstracts, Social Services Abstracts), PTSDPubs, PAIS Index, ProQuest Dissertations and Theses Global, Medline, APA PsycInfo, ERIC, Education Source, CINAHL, Social Work Abstracts, Academic Search Premier, Military & Government Collection, Embase, and Web of Science (Social Sciences Citation Index, Science Citation Index Expanded, Arts and Humanities Citation Index, Emerging Source Citation Index). The complete electronic search strategies for each database can be found in the supplemental material.
Furthermore, search terms centered around housing programs were not imposed in the search but instead used as a screening parameter to ensure that author-specific differences in terminology were not missed. Comprehensive testing of search terms around veterans and the military was also conducted to ensure that the final two search terms caught all related terminology; a complete list of considered terminology is available. Please see Appendix C for a definition of homelessness, and refer to our search terms in the supplemental file. The date range was selected to capture a broad assortment of articles, especially since this topic area has been neglected in scoping reviews, leaving a lot of ground to cover. This review focused on the ABCANZ military alliance, which includes Canada, the United States, the United Kingdom, Australia, and New Zealand, due to the similarities between these nations (Government of Canada, 2022). This geographical focus provides a cohesive analysis among militaries that operate within a partnership and common standards. In addition, the review focused solely on peer-reviewed articles to help narrow the number of articles screened. Finally, this review did not omit studies based on methodology or research design.
All 6088 articles were exported into Covidence, with one article dropped during import and 3338 removed through de-duplication (completed by A.L.). Two independent screeners (D.Q. and S.L.) reviewed the titles and abstracts for the 2749 results in Covidence, screening for peer-reviewed articles that mentioned veterans and homelessness. Conflicts were resolved by a third reviewer (J.B.). A total of 467 articles were sought for full-text retrieval with 11 being unretrievable. The full-text review of the retained 456 articles was conducted independently by two screeners (J.L. and N.L.) in Covidence, who further isolated the resources based on eligibility/screening criteria. Following two rounds of screening, 119 articles were included in this review. Please see Appendix A for the inclusion/exclusion criteria table. Quality appraisal of the included resources was not completed for this review. The PRISMA flow diagram in Appendix B breaks down the entire screening process.
Data Extraction
This review followed qualitative thematic analysis methods to extract and synthesize primary information (Vaismoradi et al., 2013). Initial article data were generated using Covidence’s data extraction generator, which provided an Excel file containing article information, including author names, publication dates, journal titles, and abstract text. All articles were reviewed independently by each research team member to identify relevant themes surrounding SU and use and/or barriers to health services. The research team then met to discuss the most prominent themes until a consensus was reached. Two researchers (J.L. and N.L.) were tasked to independently extract and chart article information into an Excel file according to the identified themes (Please see supplementary file). The same two researchers used the charted information to synthesize thematic results, which were then reviewed by the rest of the research team to ensure consensus and accuracy. In addition, quantitative findings were completed independently by a single member of the research team (J.B.), who conducted an online search of each first author’s affiliation and country of origin and charted the information into an Excel file, including the documentation of research design for each article.
Results
Quantitative Findings
While qualitative thematic analysis was primarily used for this review, three notable quantitative findings are presented. First, all retained articles for this review were scanned to determine the affiliated country of the first author for each publication. While we anticipated that the United States would represent the bulk of all retained publications, we had not expected such a lack of diversity of publications from ABCANZ military alliance countries nor the extent of publications coming from American authors. First authors from the United States (N = 116) account for almost all publications retained in this review, except for three from Canadian authors (N = 3).
Second, we examined the number of published articles across 30 years (1990–2021) and compared them among 5-year groupings (See Figure 1). This review reveals that the number of publications associated with veteran homelessness, addiction, and SU barriers and services has increased relatively significantly over the past 10 years.
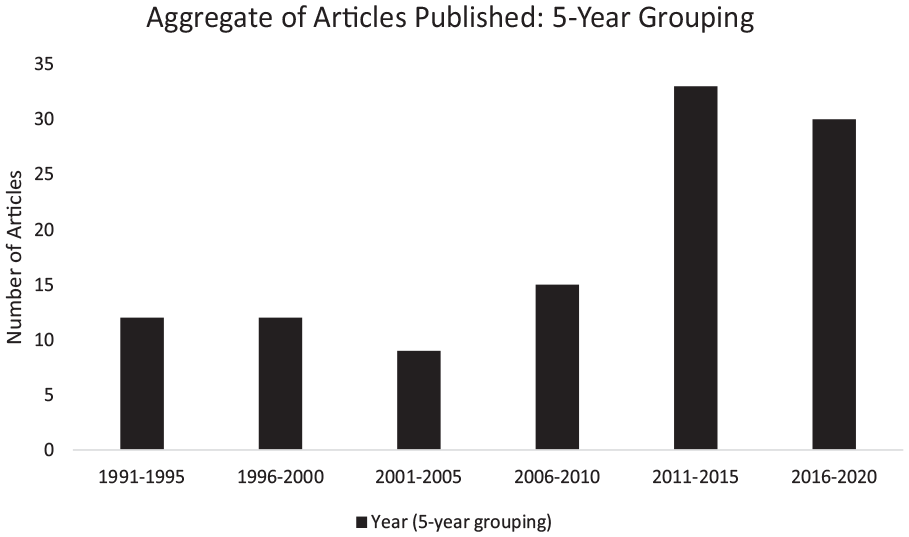
Aggregate of Articles Published: 2-Year Grouping.
Third, the characteristics of the 119 retained articles were assessed. Most articles (41.2%) used quantitative analysis, while an ample proportion were observational (26.9%). Qualitative methods (13.4%) and experimental design (13.4%) were equally represented. Most studies (40.3%) had females as a subgroup and typically represented less than 5% of a study’s sample. Other articles had no mention of gender (23.5%) or focused on males (22.7%), while only a few offered gendered comparisons (10.9%) or focused on females (2.5%). Figure 2 below offers more detail.
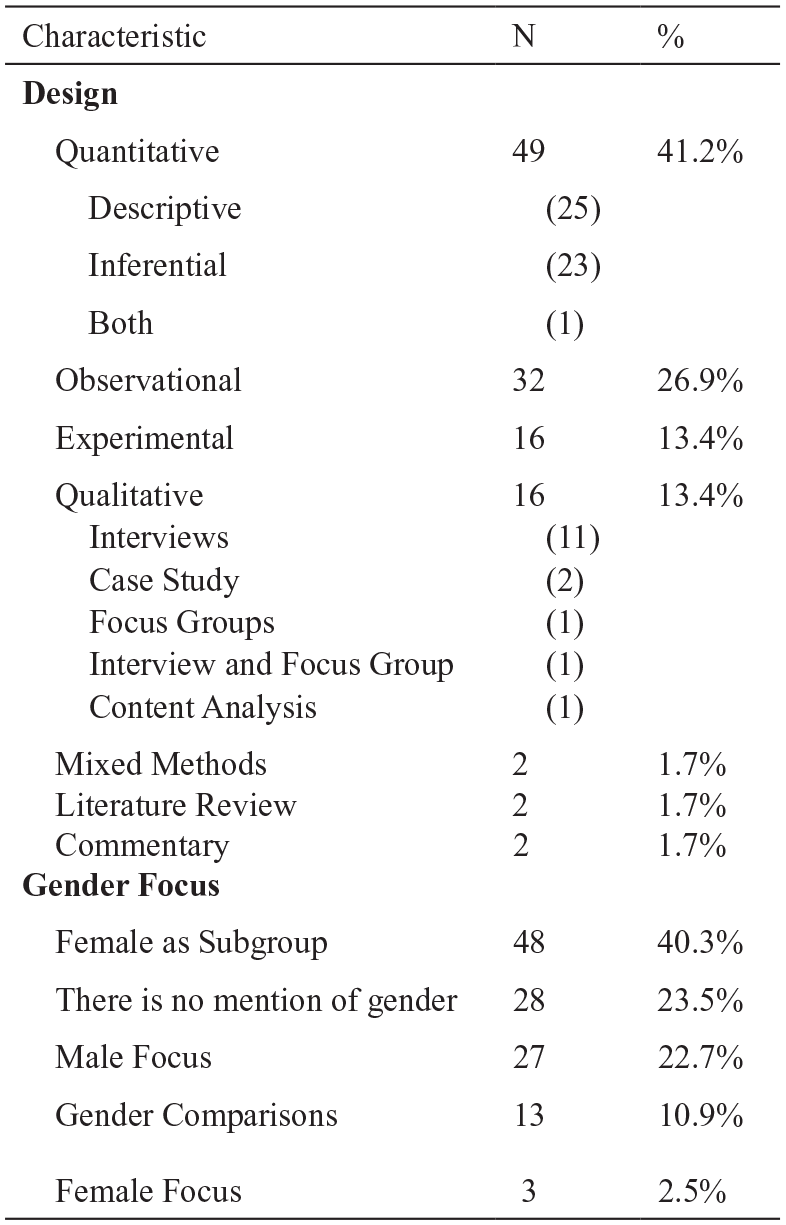
Research Designs Included in the Review (N = 119).
Qualitative Findings
Five key themes were generated through thematic analysis of all articles included in this review. These themes were as follows (1) the association between SU and housing stability, (2) gendered comparisons with service needs and provision, (3) consideration for comorbidities, (4) social support and relationship-centered interventions, and (5) barriers to health care services.
The Association Between SU and Housing Stability
The research included in this review spans three decades, throughout which an association between SU and housing stability is repeatedly confirmed. Specifically, we observed a pattern of SU impacting veterans’ ability to maintain safe and stable housing as well as the inverse of homelessness inhibiting veterans’ access to services to address their SUDs and other health concerns (Bachhuber et al., 2015; Tsai & Rosenheck, 2013; Winer et al., 2021). Veterans who lacked stable housing frequently turned to EDs to meet their health needs, given that they lacked access to regular preventive care for SUDs and other comorbidities (Byrne et al., 2017; LePage et al., 2014; O’Toole et al., 2013). Active use of substances also inhibits service/housing access, given that some programs require sobriety/abstinence to enroll and/or remain in the program (Hutt et al., 2018; Petrovich et al., 2014; Schinka et al., 2018). Transitional and supportive housing programs implementing Housing First principles attempt to address the complexities of this bidirectional association. Housing First programs were commonly discussed across the articles in this review (Montgomery et al., 2013; O’Connell et al., 2009, 2012; Tsai et al., 2014; Tsai & Rosenheck, 2013). Please see Appendix C for a definition of housing first.
One widely assessed Housing First program in the United States is Housing First U.S. Department of Housing and Urban Development-Veterans Affairs Supportive Housing (HUD-VASH). Homeless veterans enrolled in HUD-VASH were more likely to be stably housed 12 months after enrolment compared to the treatment-as-usual group—those receiving existing veteran affairs services (Montgomery et al., 2013). Both the HUD-VASH and treatment-as-usual groups saw a decrease in ED visits and in-patient mental health treatment. However, between-program differences were not significant in this study, likely due to the plethora of overlapping services available to both groups, such as case management, outreach, and housing search assistance (Montgomery et al., 2013). Furthermore, the HUD-VASH group remained significantly longer in in-patient mental health (Montgomery et al., 2013). Alternatively, homeless veterans staying in housing under the Milwaukee Continuum of Care illustrated how recovery work could only start once in stable housing (Nelson et al., 2019). Gruenewald et al. (2018) further noted the importance of Housing First and the lack of flexibility of abstinence-based housing programs as a barrier to care.
Gendered Comparisons With Service Needs and Provision
Earlier studies of US homeless veterans opted not to recruit samples of female veterans due to their low representation in the population (Conrad et al., 1998). More literature has been released in recent years, with the increase in females enlisting in the US military and serving in combat. No studies in the review discussed transgendered or intersex veterans. The retained literature presents several characteristics of female veterans and comparisons with male counterparts. The literature indicates that female veterans are less likely to be homeless than male veterans (Bachhuber et al., 2015; Byrne et al., 2016; Tsai et al., 2012), yet simultaneously are at greater risk of homelessness (Bachhuber et al., 2015; Byrne et al., 2013) and are overrepresented in adult female homeless populations (Byrne et al., 2013).
Compared to homeless male veterans, homeless female veterans were more likely to be younger (Byrne et al., 2013; Montgomery & Byrne, 2014; Tsai et al., 2012, 2014), be married (Benda & Belcher, 2006), have children (Benda & Belcher, 2006), and have greater social connectedness and social supports (Benda, 2006). In a sample of 1634 homeless female veterans with SUDs, 289 (16.79%) were accompanied by dependent children (Tsai et al., 2014). Female veterans experiencing homelessness generally had lower rates of substance dependence or use (Byrne et al., 2013; Tsai et al., 2014; Tsai et al., 2014). However, homeless female veterans were also less likely to be employed (Byrne et al., 2013; Tsai et al., 2012), have greater rates of mood disorders (Benda, 2006; Byrne et al., 2013; Tsai et al., 2014; Tsai et al., 2014), and have higher rates of PTSD (Tsai et al., 2012, 2014). Homeless male veterans, on the other hand, were more likely to have cognitive impairments (Benda, 2006), had previous stays in SU treatment programs (Benda & Belcher, 2006), been exposed to combat (Tsai et al., 2012), been arrested for a felony in the previous 5 years, and comorbidities of chemical use and psychiatric disorders (Benda & Belcher, 2006). Most significantly, save for childhood physical abuse, homeless female veterans had been demonstrated as more likely than homeless male veterans to have survived sexual and/or physical abuse throughout their lives, in the military, or over the past 2 years (Benda & Belcher, 2006; Benda, 2006). Female homeless veterans were found to be significantly more likely than male homeless veterans to access outpatient medical and mental health supports, whereas male homeless veterans were more likely to use SU outpatient treatments and ED services (M. M. Desai et al., 2003; Montgomery & Byrne, 2014; Schutt et al., 2019). In a set of focus groups with 29 female homeless veterans, participants reported that there were fewer homeless services or housing programs for female veterans than for male veterans (Hamilton et al., 2012).
Several studies reveal similar treatment program outcomes, although with some nuanced differences that should be considered (Benda, 2004, 2005, 2006; R. A. Desai et al., 2008; Justus et al., 2006; Tsai et al., 2012). Participation in a veteran domiciliary treatment program was shown to reduce the effects of age, childhood abuse, SU, combat exposure, and suicidal thoughts for both genders on risk for readmission (Benda, 2006). Furthermore, male (70%) and female (66%) homeless veterans in a dual-diagnosis in-patient program were similarly readmitted to MHSUD facilities during the 2-year follow-up period (Benda, 2004). Although SUDs, childhood abuse, and depression predicted readmission for both genders, male homeless veterans were readmitted with higher scores on SU measures, combat exposure, aggression, cognitive impairments, confused thinking, and memory loss (Benda, 2004, 2006). Similarly, 1 year following a transitional housing program, controlling for gender differences at intake, male and female veterans displayed no differences in housing, employment, SU, physical or mental health, or quality-of-life outcomes (Tsai et a., 2012). There were also generally no differences in housing outcomes between males and females in HUD-VASH (Tsai et al., 2014). Nevertheless, case managers assigned to the program were found to focus more on employment-related activities, spend more time in in-person sessions, and have better working relationships with female veterans. While the study did not reveal the reason for the better relationship between caseworkers and female veterans, this might be due to the reported increase in face-to-face time compared to males. R. A. Desai et al. (2008) charted the effectiveness of a 6-month Seeking Safety treatment program with female homeless veterans suffering from SU and trauma histories. It was found to produce moderate improvements in employment, social support, general symptoms of distress, and symptoms of PTSD.
Consideration for Comorbidities
Nearly half (43.7%) of the articles in this review included discussions that centered around the influence of comorbidities on health care access and service utilization among veterans experiencing homelessness (O’Toole et al., 2013; Tsai et al., 2021; Wenzel et al., 1996). The presence of physical and mental health disorders was the most commonly reported condition occurring in conjunction with SU in this population (Gamache et al., 2000; Kasprow, Rosenheck, et al., 1999; Tsai et al., 2021). Dual diagnoses or self-reports of SU and mental health disorders, including depression, anxiety, PTSD, schizophrenia, and bipolar disorder, were frequently observed in the literature (Applewhite, 1997; Carpenter et al., 2015; Kuehn, 2013; McGuire et al., 2011; Wenzel et al., 1996). Similarly, co-occurring physical health concerns reported consistently across multiple articles in this review included diabetes, hypertension, arthritis, hepatitis, and HIV (LePage et al., 2014; McGuire et al., 2011; Norbeck et al., 2020; O’Toole et al., 2010).
Existing research in this review demonstrates that while veterans experiencing homelessness came into contact with the health care system at higher rates than non-veterans experiencing homelessness due to the aforementioned comorbidities (O’Toole et al., 2010, 2013; Tsai et al., 2021), this did not guarantee that they would receive appropriate services to address all competing health issues (Iheanacho et al., 2018). Iheanacho et al. (2018) found that health care providers—particularly those who encounter homeless veterans in EDs—were faced with the challenging task of identifying and responding to all competing health concerns within the short window of time that they see these patients who are part of a highly transient population. Providers may, therefore, prioritize, overlook, or even misdiagnose specific health concerns, leaving veterans experiencing homelessness with unmet needs even after seeking care (Iheanacho et al., 2018; O’Toole et al., 2013; Petrovich et al., 2016). Veterans experiencing homelessness who accessed primary care were also found to be 1.5 to 10 times more likely to have no ED use compared to non-homeless veterans, depending on the type of care accessed (O’Toole et al., 2013). Again, this reinforces the importance of assessing comorbidities among veterans experiencing homelessness to connect them to appropriate health care services. The relevance of comorbidities in treatment options was observed in a handful of studies included in this review that were explicitly designed to evaluate treatment programs for dually diagnosed veterans experiencing homelessness (Ellison et al., 2016, 2020; Kasprow, Frisman et al., 1999; Leda & Rosenheck, 1992; Smelson et al., 2018, 2013).
Social Support and Relationship-Centered Interventions
This review identified relationship-centered interventions for SU as a commonly used type of SU intervention for veterans experiencing homelessness (Burling et al., 1992; Ellison et al., 2020; LePage & Garcia-Rea, 2008, 2012; Yoon et al., 2017). Based on the available literature, this group of interventions holds the potential to decrease the use of substances and increase adherence to treatment for this population. For example, homeless veterans who participated on a softball team within a residential treatment program recorded higher abstinent rates from drugs and alcohol and stayed in treatment longer compared to patients in the same residential treatment not participating on the softball team (Burling et al., 1992). Similarly, LePage et al. (2006) evaluated using a contingency management intervention to enhance altruistic and lifestyle behaviors and improve the treatment program environment. Patients were rewarded for each recorded recreational, social, and spiritual activity and the supportive acts done by other patients. The authors concluded that this intervention significantly enhanced motivation and engagement in the primary treatment program (LePage et al., 2006). Increasing healthy lifestyle behaviors (e.g., social support, recreation, and spiritual practices) was also found to decrease SU relapse and re-entry into homelessness for domiciliary rehabilitation residents (LePage & Garcia-Rea, 2008).
A series of articles by Benda (2004, 2005, 2006; Benda & Belcher, 2006) broadly examined the impact that social supports, or lack thereof, can have on homeless veterans’ SU. Among homeless female veterans with SU and psychiatric disorders, augmented social support and enriched relationships with friends and family were associated with a lower risk of readmission to a VA in-patient program (Benda, 2004). Furthermore, Benda and Belcher (2006) modeled the impacts of forgiveness on veterans’ alcohol and drug use. Through statistical modeling, these authors concluded that forgiveness, when sought later in life by veterans experiencing homelessness, can improve relationships with family and friends and decrease feelings of distress and depression, which contribute to the use of drugs and alcohol. Therefore, Benda and Belcher (2006) argued that VA services should include interventions that seek to mitigate veterans’ social disconnectedness. The two streams of literature captured in this theme provide support for this group of relationship-centered interventions for SU among veterans experiencing homelessness.
Barriers to Health care Service
Barriers to health care service intersect with the other four themes discussed above. However, many studies in this review specifically investigated factors that helped and hindered access to health care services. Researchers have demonstrated that homeless veterans with psychiatric or SUDs more frequently accessed medical care, EDs, smoking prevention services, SU in-patient and outpatient programs, and residential treatments (M. M. Desai et al., 2003; Iheanacho et al., 2018; McGuire & Rosenheck, 2005; Norbeck et al., 2020). However, despite general increases in service use, homelessness has been demonstrated to decrease access to certain preventive medical services such as tobacco cessation, immunization, cancer screening, and counseling (McGuire & Rosenheck, 2005).
Common barriers to service use discussed across multiple unrelated qualitative studies included dehumanizing or insensitive service providers; lack of information about services; lack of trust in the system; geographic location; poor service organization; restrictive policies; struggles with mental health issues and substances, and transportation (Applewhite, 1997; Marsella et al., 2020; Weber et al., 2017; Winer et al., 2021). In later research, homeless veterans cited a preference for accessing EDs due to difficulties and time constraints in navigating the health care system or accessing other resources (Weber et al., 2017). Quantitative research supports the barriers to access identified within qualitative studies. In an evaluation of primary care experiences among veterans with mental health and/or SUDs, homeless veterans more often reported negative experiences than housed veterans for service provider communication, comprehensiveness, care coordination, medical decision-making, and self-management support (Jones et al., 2017). Using logistic regression models to predict access to SU services, preference for VA-provided services, geographic availability, and referral through other providers were all enabling factors of access (Petrovich et al., 2016).
One standard system approach to reducing access barriers, such as geographic location and poor service organization, has been integrating primary care, homeless services, and mental health and SU services. Such an approach was championed in a case study of the Veteran Affairs Greater Los Angeles Health care System (Blue-Howells et al., 2008), where, beyond service integration, the clinic also organized more walk-in appointments and on-call psychiatric assessments. Jones et al. (2018) demonstrate positive outcomes of similar changes made by VA Homeless Patient Aligned Care Teams (HPACT), such as more offerings of walk-in appointments, flexible scheduling, extended hours, community outreach, and service integration. Geographic co-location and integration of services results in more rapid receipt of appointments, more visits, more preventive services, and lower levels of ER access (McGuire et al., 2009).
Discussion
This scoping review provided a synthesis of peer-reviewed published data over 30 years that discuss the intersection of veteran homelessness, SUD, and service utilization. Overall, homeless veterans are overrepresented in health service use compared to non-homeless veterans (Manhapra et al., 2021; Rosenheck et al., 2021).
The evidence of this review maintains that homeless veterans with SUDs disproportionately access health care (i.e., emergency room) and SUD treatment services (i.e., in-patient and out-patient SU treatments). To reduce widespread and recurrent use of services, it may be beneficial for first-line SUD interventions to attend to homeless veterans’ unique and complex needs. Tailored mental health and SUD treatments that consider a biopsychosocial model are unequivocally beneficial to treatment outcomes regardless of disorder or population (Afuseh et al., 2020; Dixon et al., 2016; Engel, 1977; Marchand et al., 2019; Välimäki & Lantta, 2019). Moreover, patients prefer and encourage individually tailored treatment and find it superior to a “one size fits all” approach (Li et al., 2024). Indeed, within our results, gendered differences, mental and physical comorbidities, and housing stability were shown to be factors that are predictive of success in the treatment of SUD.
Previous studies have indicated that male and female homeless veterans are equally subject to readmission for SU treatment (Benda, 2006; R. A. Desai et al., 2008; Justus et al., 2006; Tsai et al., 2012). However, gender differences were shown to be a key factor in successful treatment and increased the likelihood of successful housing. It has been proposed that “to provide the best care to women veterans, it may be important to address their unique health, mental health, and psychosocial needs through specialized programs” (R. A. Desai et al., 2008, p. 996). Indeed, there are gendered differences that should be considered in SUD treatment programs to improve female veterans’ outcomes and increase the chance of stable housing. For instance, homeless female veterans are more likely to be responsible for children and have higher rates of sexual abuse (particularly during service), mood disorders, and PTSD (Byrne et al., 2013). Veteran’s Affairs in the United States is a leading organization in caring for veterans (including those experiencing homelessness), offering health care programs such as Residential Rehabilitation Treatment Programs and Psychosocial Residential Rehabilitation Treatment Programs, and highlighting a person-centered nature. However, there seems to be less focus on women-specific programming (Lowman & Sheetz, 2021). Outside of the United States, it could be helpful to develop programs targeting homeless women with SUD and co-occurring mental health difficulties. Programs such as Seeking Safety (R. A. Desai et al., 2008) could be consulted as starting points for tailoring programs for homeless veteran women (Johnstone et al., 2023).
Beyond gender, the success of SUD programs for homeless veterans is significantly impacted by their mental and physical health comorbidities. SUD often co-occurs with physical conditions such as diabetes, hypertension, arthritis, hepatitis, and HIV, as well as mental health disorders like depression, anxiety, PTSD, schizophrenia, and bipolar disorder (LePage et al., 2014; McGuire et al., 2011; Norbeck et al., 2020; O’Toole et al., 2010). These psychological and physical health issues are frequently the primary reasons veterans seek health services, particularly in EDs or from physicians (Iheanacho et al., 2018; O’Toole et al., 2013; Petrovich et al., 2016). However, primary care settings typically do not provide the continuity of care necessary to manage the complex comorbidities that veterans often present with (Cucciare et al., 2015). Despite the multitude of services offered by Veteran Affairs, less than half of the U.S. veteran population uses these services (Meffert et al., 2019; Tsai et al., 2015). Furthermore, many other countries lack similar integrated care systems for veterans. This underscores the ongoing need for primary care services and tailored interventions alike to be adequately equipped to address the complex needs of veterans experiencing homelessness and their associated comorbidities (Canavan et al., 2012).
Service providers are encouraged to take their time in identifying and treating their complex needs (Iheanacho et al., 2018). It may be beneficial for primary care settings to receive additional training about specialized resources targeting homeless veterans with SUD, who may be better equipped to address their needs (Armstrong et al., 2005; Vest et al., 2019). Moreover, SUD treatment centers and housing interventions, regardless of the overseeing organization, should maintain a standard of continuity of care that addresses mental and physical health issues holistically. This care could focus on addressing difficulties hierarchically, prioritizing life-threatening conditions, treatment-inhibiting factors, and quality-of-life concerns (Lynch et al., 2006).
Finally, evidence continually supports a housing-first model and the positive impact housing stability has on SUD treatment programs for homeless veterans (Bachhuber et al., 2015; Tsai et al., 2013; Winer et al., 2021). The increased focus on housing stability could decrease the overutilization of general health care services such as ED and in-patient mental health services. However, housing programs should strongly consider more flexibility with abstinence-based housing programs because these programs contribute to homeless veterans being stuck in a perpetual state of addiction (Hutt et al., 2018; Petrovich et al., 2014; Schinka et al., 2018).
This scoping review only considered peer-reviewed academic sources. Therefore, including gray literature and sources outside peer review might provide significant evidence and information not considered in our review’s findings. In addition, our research team only gained access to Scopus after this work was completed, so a further search of that extensive database could be included in the future. Despite looking at the ABCANZ military alliance countries, the vast majority of publications came from United States authors, which has led to evidence and recommendations that are geographically biased and might not easily translate to other countries. More research on homeless veteran SUDs needs to be completed outside the United States to account for geographical differences in demographics, lived experiences, and service delivery. Future research could identify reasons for the gendered differences in service utilization, which might further illuminate comorbidities and barriers to accessing services. We acknowledge that qualitative thematic analysis is subjective and leaves room for bias and differences in interpretation. Finally, depending on the scope and direction, a broader or narrower range of databases or publication timeframe may be considered for future scoping or systematic reviews, including the addition of Scopus, which was added to the university’s access after this review was underway.
Conclusion
This scoping review illustrates how homeless veterans experiencing SUDs have complex needs and face additional service barriers compared to nonhomeless veterans. The findings offer service providers, frontline service workers, and community stakeholders essential considerations and recommendations for delivering SUD services to homeless veterans. Each thematic section of this review can undoubtedly warrant a systematic review, and we encourage future researchers to do so. We hope this review encourages non-American researchers to contribute to this important topic and that it contributes to positive change.
Supplemental Material
sj-docx-1-afs-10.1177_0095327X241297650 – Supplemental material for Substance Use Service Utilization and Barriers to Access Among Homeless Veterans: A Scoping Review
Supplemental material, sj-docx-1-afs-10.1177_0095327X241297650 for Substance Use Service Utilization and Barriers to Access Among Homeless Veterans: A Scoping Review by Jordan Babando, Justine Levesque, Danika A. Quesnel, Stephanie Laing, Nathaniel Loranger, Arielle Lomness and Philip McCristall in Armed Forces & Society
Footnotes
Appendix A
Inclusion/Exclusion Criteria.
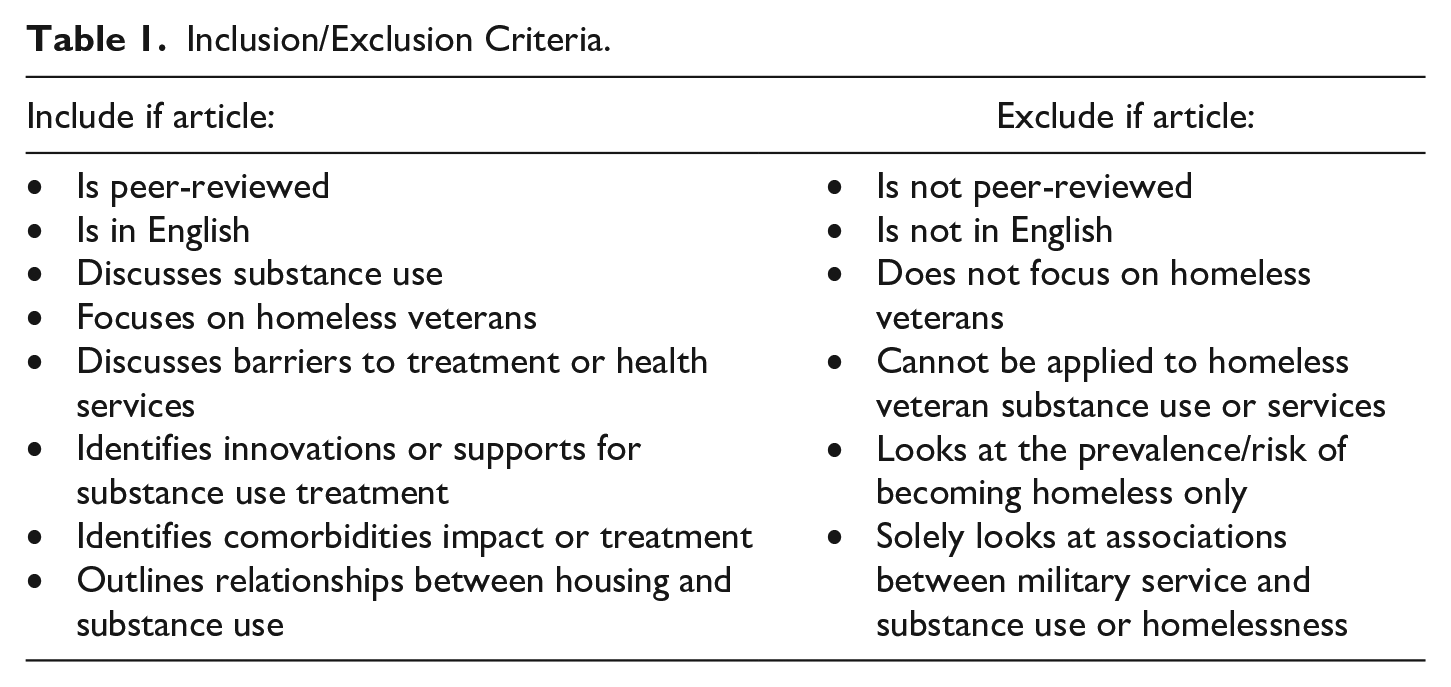
| Include if article: | Exclude if article: |
|---|---|
| • Is peer-reviewed • Is in English • Discusses substance use • Focuses on homeless veterans • Discusses barriers to treatment or health services • Identifies innovations or supports for substance use treatment • Identifies comorbidities impact or treatment • Outlines relationships between housing and substance use |
• Is not peer-reviewed • Is not in English • Does not focus on homeless veterans • Cannot be applied to homeless veteran substance use or services • Looks at the prevalence/risk of becoming homeless only • Solely looks at associations between military service and substance use or homelessness |
Appendix B
Appendix C
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.