
Abstract
The purpose of this article is to analyze the ecosystem of a military family, focusing on the risk factors that influence their health and well-being on various socioecological levels (individual, micro, meso, and macro). We develop a theoretical model of health outcomes and risk factors and test it empirically using quota sampling of 460 respondents from military families in Slovenia. Thirty-three regression models were calculated to measure the impact of theoretically defined risk factors on the health outcomes of military families. Surprisingly, a long daily commute, one of the most military-specific factors in Slovenian society, is viewed more positively than negatively. Moreover, risk factors related to the family on the micro and individual levels, such as poor financial situation or parental stress, are responsible for the greatest impact on military family health. Meanwhile, spouses report that military work-related stress affects the servicemembers’ overall health and increases the possibility of intimate partner violence.
Keywords
Like any civilian family, a military family 1 has its own ecosystem that defines it within the broader context of society. Ecosystems are made up of intricately linked social networks that create the basis for interactions outside the family (Everson & Camp, 2011). In Slovenia, military families are an integral part of wider society, in close proximity with their extended family, and interact in the community as part of various nonmilitary social networks. On macro level, military families are open to civil society agents of socialization like the preschool care system and obligatory public primary school.
Following the war for independence in 1991, the Slovenian Armed Forces (SAF) has slowly moved from the institutional to occupational model, 2 passing through various phases of professionalization and the transition from a compulsory to all-volunteer armed forces. The latter was achieved in 2002, while 2 years later Slovenia became a full member of both North Atlantic Treaty Organization (NATO) and the European Union (EU). Today, approximately 16% of SAF servicemembers are female with the SAF having been the first NATO member to appoint a female major general to the position of Chief of the General Staff. 3 Nowadays, the security environment requires the military to be engaged in a variety of tasks, leading to increased workplace demands (e.g., military exercises, international operations and missions, tasks related to management of illegal migrations, a long daily commute to work). All of this places a heavy burden not only on the life of servicemembers but also on that of the military family.
Although servicemembers generally encounter similar challenges to other professions in balancing between the family, work, and personal time, certain of their challenges are quite specific. For instance, they are often away from home for shorter (e.g., trainings) or longer periods (e.g., deployments of varying levels of risk), which disrupt family routines and affect the whole family and the parenting (Wojda et al., 2017). Military demands also often cause various negative health outcomes among servicemembers whose problems often spill over into their families (e.g., Foran et al., 2017; Rentz et al., 2007; Skomorovsky et al., 2015). As explained later in the article, the health outcomes of the whole family might be a result of combat stress, frequent long-term absences, adaptations to a new social environment when deployed, changes in family routines in times of absence and reintegration into the family following deployment, and other stressors.
Several studies in the fields of military sociology, psychology, social psychology, and defense studies in different countries have identified a range of health problems among servicemembers and within military families. The following health outcomes specific to either servicemembers or military families (as a unit) have been recognized (see Figure 1): misuse of psychoactive substances (e.g., alcohol, drugs, medications; Foran et al., 2011; Wright et al., 2012); depression and posttraumatic stress disorder (PTSD; e.g., Campbell & Renshaw, 2016; Foa et al., 2009; Hoge et al., 2004); intimate partner violence (IPV; Aronson et al., 2014; Forgey & Badger, 2006; Newby et al., 2005); intimate partner (dis)satisfaction (e.g., Carvalho & Chambel, 2017; Juvan & Jelušič, 2007; Keeling et al., 2015); poor child–parent relationships and compromised child well-being (e.g., Andres & Moelker, 2011; Bóia et al., 2017; Skomorovsky & Bullock, 2017; Vuga Beršnak, 2016); and general health (e.g., Baker et al., 2009; Sauvet et al., 2009; Williamson et al., 2019).
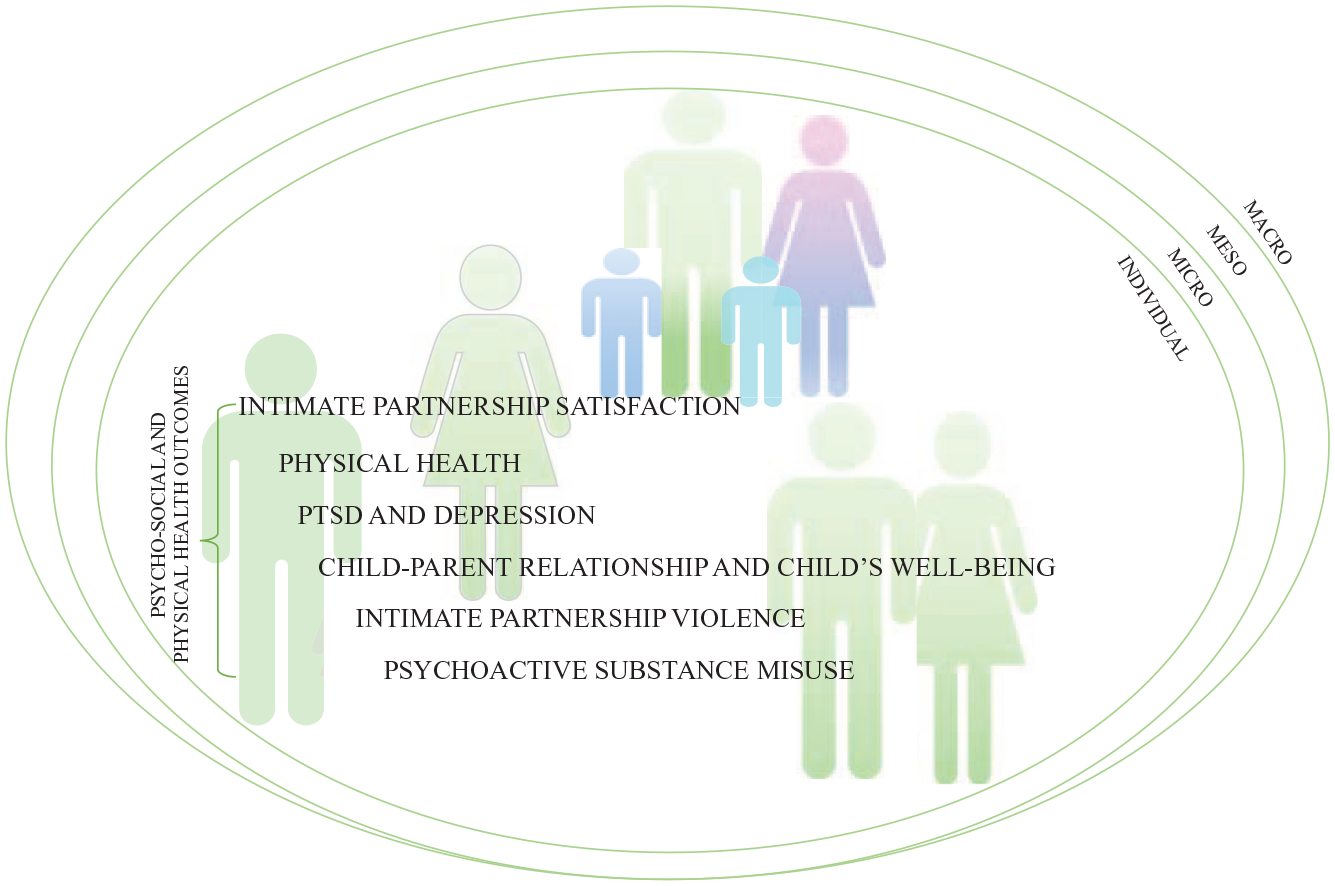
Psychosocial and Physical Health Outcomes of a Military Family
The majority of these studies were carried out in Western countries (e.g., the United States, Canada, the United Kingdom, certain European countries). Yet, these countries have completely different national interests, international aspirations, and global roles, which means the military organization involved has a comparatively different nature and purpose. Among others, a small European country like Slovenia differs with respect to the following: (1) noncombat deployments dominate; (2) the position held by military families within the military organization (private civilian housing, not a military housing system); (3) the welfare state (e.g., a publicly available child care system and primary school, public health care system, various family and social support measures); (4) the full-time employment of civilian spouses; and (5) the proximity of the extended family, and the important supportive role played by the grandparents.
Taking such differences into account, we developed a theoretical model 4 containing recognized health outcomes of a military family and defined military-specific risk factors on various levels within the family’s ecosystem. 5 The model anticipates that each psychosocial or physical health outcome that is identified is affected by risk factors on one or more levels. To understand the military family’s health, we observed the interactions between various risk factors within the family’s ecosystem (from the individual to the macro level) and statistically measured the strength and direction of their impact on military families’ health by applying regression models for each health outcome listed above.
The purpose of this article is to analyze the strength of selected risk factors for the health of the Slovenian military family by testing the theoretical model.
Risk Factors for a Military Family’s Health
The selected theoretically supported risk factors (see Table 1) stem from various socioecological levels: individual, micro, meso, and macro. The individual level refers to individual characteristics of servicemembers and their spouses. The microsystem is composed of the military family level, the military organizational level, and the extended family. The mesosystem, where separate stakeholders from the microsystem start to interrelate with each other, is in our case the community (e.g., school, military, spouse’s employer, extended family). The macrosystem comprises the national and institutional policy level and the position held by the military organization in a given society. The specifics of the Slovenian environment were identified through a process of conducting qualitative expert interviews in military and civilian environments (Vuga Beršnak, Živoder et al., 2020). Some health outcomes are simultaneously risk factors for another health outcome.
Measuring the Risk Factors on Various Socioecological Levels.
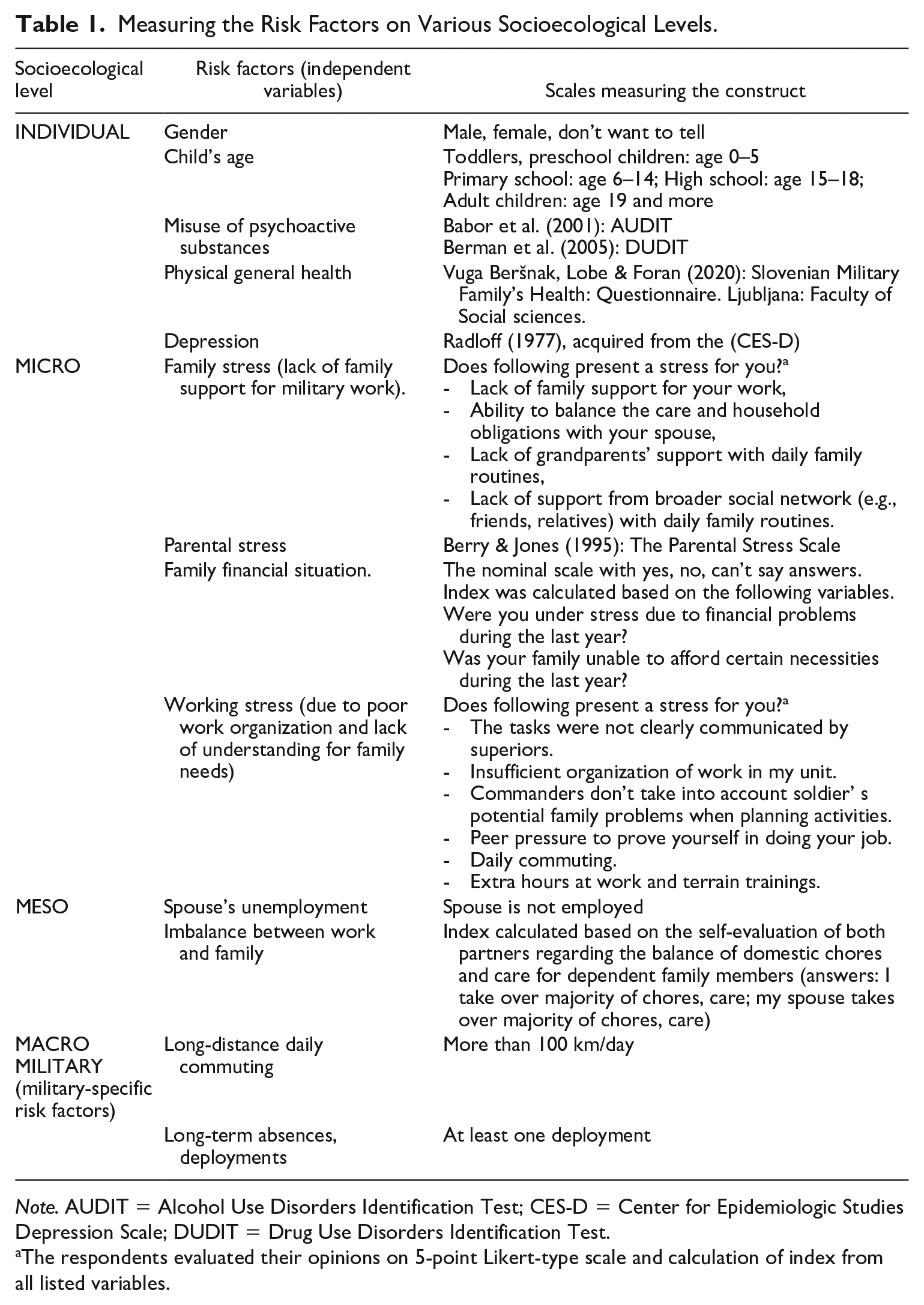
Note. AUDIT = Alcohol Use Disorders Identification Test; CES-D = Center for Epidemiologic Studies Depression Scale; DUDIT = Drug Use Disorders Identification Test.
The respondents evaluated their opinions on 5-point Likert-type scale and calculation of index from all listed variables.
Later in this article, the risk factors arising from various socioecological levels are considered in the context of how they affect the health outcomes of a military family.
On the individual level, gender is an important predictor for certain health outcomes.
Among the general population, men are more inclined to misuse psychoactive substances, alcohol, and/or drugs (Bloor, 2006; Degenhardt et al., 2008; European Monitoring Centre for Drugs and Drug Addiction [EMCDDA], 2014; Jeriček Klanšček et al., 2015; UNODC, 2014). Alcohol misuse increases the risk of relationship problems, violence, or child maltreatment (Foran et al., 2017). Risk factors for alcohol misuse also include depression, which at the same time is a health outcome (e.g., Foran et al., 2011; Pierce et al., 2000). On the contrary, intimate partner satisfaction may be important for preventing depression (Asbury & Martin, 2012).
Heavy drinking can be linked to IPV. Adams (2000) discovered that while women initiate violence slightly more often (hit first), men are responsible for more serious sexual and physical violence (Aronson et al., 2014). Bradley (2007) established that male military veterans are less likely to cause IPV than their civilian counterparts. On the contrary, Aronson et al. (2014) found that more violence is detected in military families than in civilian ones. It is clear that the data for different countries, societal groups, and time periods vary, allowing the conclusion that gender’s impact on IPV is inconclusive for either civilian or military families.
On the micro level, we defined four groups of risk factors: (1) the family problems, (2) the work environment, (3) parental stress, and (4) a poor family financial situation. Furthermore, we predicted that, like parental stress, the age of children can also be a risk factor.
Stress, regardless of its origin, influences various aspects of one’s life, health, and well-being. Stress is associated with the misuse of psychoactive substances, including alcohol with its ability to reduce stress (Cappell & Greeley, 1987; Sayette, 1999). It might trigger alcohol addiction (Becker, 2017). Moreover, the work environment could be a source of stress affecting the misuse of psychoactive substances, IPV, and certain other negative health outcomes (Bray et al., 1999). It seems that servicemembers often perceive their working environment as more stressful compared with home (Bray et al., 1999). Stress can also be attributed to the triggering of depression, together with other environmental factors (Tafet & Nemeroff, 2016).
Another important source of stress responsible for negative health outcomes is a family’s financial situation (Wan et al., 2019; Wang & Pullman, 2019). Previous analysis of the SAF’s servicemembers indicates the family’s satisfaction with the income of the member employed in the military is a predictor of overall satisfaction with an intimate partnership (Vuga & Juvan, 2013). Bullock and Williams’s (2019) findings for Canada’s armed forces reveal a similar impact of financial stability on overall family satisfaction. One may thus assume that dissatisfaction with the military income and the family’s related financial problems might be a risk factor for intimate partner satisfaction.
The latter is also influenced by military demands such as deployments and other absences. Rentz et al. (2007) established that frequent deployments can increase the level of family stress, which is related to violence. The anguish caused by a deployment can manifest in the stay-at-home spouse and indirectly in preschool children (Osofsky & Chartrand, 2013). Deployments can affect the relationship between child and parent as well as the child’s well-being. Stay-at-home parental stress often grows during a deployment, but not necessarily only then.
On the meso level, we observed the impact of the following risk factors: work–family conflict and spouse’s unemployment.
The additional burden of a lack of balance between the parents regarding the care and other household obligations can cause physical and emotional exhaustion and trigger negative health outcomes. Military working demands are often the reason for stress and the lack of a balance between family and work (Skomorovsky et al., 2015). The family is often subordinated to the demands of the military (Hannola, 2019; Vuga & Juvan, 2013). The latter is generally expected from a supportive and caring institution, which a family definitely is (Švab, 2001). Furthermore, support and care are primarily expected from women (i.e., spouses in military families are typically female). When placing the work–family balance into the broader societal context, we may say that in Slovenia the dominant model is fatherhood whereby fathers participate and assist their female partners with the child care, while women are expected to be the dominant parental figure (Švab, 2020). In addition, since Slovenia has not followed the re-traditionalization tendency to the extent seen in certain other postsocialist countries, Slovenian women remain fully employed (the same applies to servicemembers’ spouses; Švab, 2020).
The employment of the civilian spouse is an important factor for a military family. Demands made by the military (e.g., frequent absences, longer deployments) put extra pressure on the nonmilitary parent, who must take over the care and household obligations (Gribble & Fear, 2019; Vuga Beršnak, 2016). On the contrary, this spouse’s unemployment can bring negative financial and psychological effects. Especially during the deployment, an unemployed spouse with a poor social network will more likely focus on the risks of the deployment, which leads to feelings of stress, worry, and depression (Bailey, 2019). The latter often spills over into the children and negatively affects their coping ability (e.g., Drummet et al., 2003; Pincus et al., 2004). On top of that, the unemployment of a male spouse is an additional trigger for IPV against female servicemembers (Aronson et al., 2014).
On the macro level, military support mechanisms and national family and social policies hold an important place in a military family’s ecosystem (e.g., Jelušič et al., 2020; Švab, 2020; Vuga Beršnak et al., 2021). 6 However, in our model we concentrate on two risk factors specific to the SAF, namely, ones that occur in a military sample more often than in a civilian one and define a military lifestyle. More is explained about both military-specific risk factors below as part of the argumentation concerning Hypothesis 1.
Research Question and Hypotheses
In line with the aims of the article, namely, (1) to identify the risk factors in a military family’s ecosystem and (2) to observe the interlacing of risk factors on various socioecological levels, our research question is, “Which of the theoretically and empirically recognized risk factors significantly influences the health outcomes of a Slovenian military family?”
Based on the expert interviews in the qualitative phase of this study (Vuga Beršnak, Živoder et al., 2020) and the preliminary results of the quantitative survey, we identified two risk factors that are military-specific (they did not emerge in the civilian sample): (1) a long-term absence, deployment to an international operation or mission; and (2) a long daily work commute (over 100 km per day). While both of these risk factors interfere in the family’s day-to-day routine, deployment also causes intensity and stress in the family for several reasons.
Based on these findings, we also formulated the following hypothesis:
Although every family encounters various risk factors for their health, the demands of the military add to the general risks that civilian families face in their day-to-day lives. Previous findings concerning Slovenian society and the military (Vuga Beršnak, 2021b; Vuga Beršnak, Lobe & Foran, et al., 2020) show that deployments and a long daily work commute are two factors specific to the military organization and play out differently than in a civilian environment.
Deployment is typically known for negatively affecting the child (e.g., Drummet et al., 2003; Skomorovsky & Bullock, 2017; Tomforde, 2005; Watanabe & Jensen, 2000), the child’s well-being (Skomorovsky, 2018), and disturbs the relationship between the child and the military parent. Naturally, the consequences of deployment vary depending on the child’s age and the stay-at-home parent’s ability to cope with the new situation and establish a functioning family routine. Moreover, deployments affect intimate partner relations and can lead to the stress and dissatisfaction of the stay-at-home spouse (e.g., Andres, 2014; Keeling et al., 2015).
Furthermore, Wheatley (2012) states that a long daily commute (over 100 km/day) negatively affects the family dynamics by making the work–life balance more difficult. Our own survey (Vuga Beršnak et al., 2021) among the SAF during the lockdown revealed that daily commuting to a certain extent influences the sharing of burdens within the family. When spouses had to take over the majority of the care and household obligations, the balance was destroyed and the servicemembers felt less successful (Vuga Beršnak et al., 2021). Military spouses are more often exposed to stressors than civilians, but are also more resilient in terms of coping with various situations (Moelker & van Der Kloet, 2003).
Based on the matters discussed above, we assume that both military-specific risk factors affect the health and well-being of a military family; however, the focus thus far has been on the child’s well-being:
In Slovenian society, alcohol consumption exceeds the European average, with Slovenia being one of the countries with prevalent heavy drinking patterns (among Germany, Czechia, Luxembourg, the Baltic countries; World Health Organization [WHO], 2019). The SAF forms an integral part of civilian society and is therefore affected by its agents of socialization (Vuga Beršnak, 2021a). Servicemembers also develop their networks outside the military and their identities are not chiefly related to the military (Juvan & Jelušič, 2007; Vuga & Juvan, 2013). This may lead one to assume a strong impact of the health characteristics of society on servicemembers and their families. Still, the military organization is very selective and holds high expectations in terms of the health of its servicemembers. It has procedures in place for recognizing alcohol misuse and servicemembers are periodically tested (Vuga Beršnak, 2020). In addition, Slovenia has adopted a “non-combat policy” for international operations and missions, resulting in zero casualties thus far (Vuga Beršnak, 2021a). This means servicemembers are rarely exposed to combat situations and are hence less likely to suffer from physical or psychological combat injuries or PTSD (for more, see Jacobson et al., 2008; Wright et al., 2012). Psychological problems that follow a combat experience often spill over into the family, which is, namely, not expected to be the case with the SAF.
Considering the facts mentioned above, as supported by expert interviews within the SAF, we assume that military-specific risk factors do not significantly affect alcohol misuse in the SAF:
The family demands the emotional and physical devotion of its members. On the contrary, the military organization is a greedy institution when making demands on servicemembers and their families (Coser, 1974; M.W. Segal, 1986). The military strives for success with the socialization, comradeship, and identification among servicemembers. Furthermore, military demands encroach on servicemembers’ family time and often indirectly interfere in family daily routines by extending hours spent in the field, prolonging deployments, or carrying out multiple-day or -week trainings. The comprehensiveness of a military lifestyle in combination with the traditional division of gender roles in Slovenian society (i.e., despite the full-time employment of civilian spouses) was confirmed during the lockdown in 2020 when civilian spouses were left alone and took on the majority of the domestic work, child care, and home schooling (Vuga Beršnak et al., 2021).
Accordingly, while servicemembers might not feel the risk of military work (and associated stress) for the family’s health, we may expect that their spouses do. The military working environment is hence a risk factor on the family level.
Method
The results presented here were collected in the broader mixed-methods study “Military-Specific Risk and Protective Factors for Military Family Health Outcomes” (MilFam), using a sequential exploratory design. After a thorough literature review of research findings, we have developed the theoretical model, and afterward, the qualitative part of the study was conducted. Expert interviews with relevant military and civilian experts were performed to increase understanding of the model, ascertain how its components work in the Slovenian cultural and social contexts, and, finally, make any necessary modifications to it. To empirically test the theoretical model, a suitable measurement tool was constructed (Vuga Beršnak, Lobe & Foran, 2020) and used in the quantitative survey to explain the relationships between the risk factors and health outcomes in military families. The findings presented in this article are based on the results of the quantitative part of the study.
Sample and Data Collection
We performed the survey between November 2020 and March 2021 during a time of strict pandemic-linked lockdown in Slovenia. The related restrictions meant the original plan to rely on face-to-face data collection with self-completion survey questionnaires in the barracks was impossible. Instead, the questionnaires were administered and filled in electronically through the online surveying service 1KA.
A sampling strategy thus had to be adopted and it aimed to proportionally reflect the key characteristics of the military population important for our research purpose. We decided on nonprobability quota sampling, with the quotas defined based on our research focuses: (1) gender structure of the observed population and (2) number of children per servicemember (i.e., size of the family) in the observed population. An invitation to participate and a link to the survey were disseminated via formal military and informal personal channels. We sought to include as many servicemembers exposed to the highest military demands (i.e., mostly combat units) as possible. Among their spouses, we applied nonprobability purposive sampling. Each servicemember who participated in the survey part of the research received a request to invite their spouse.
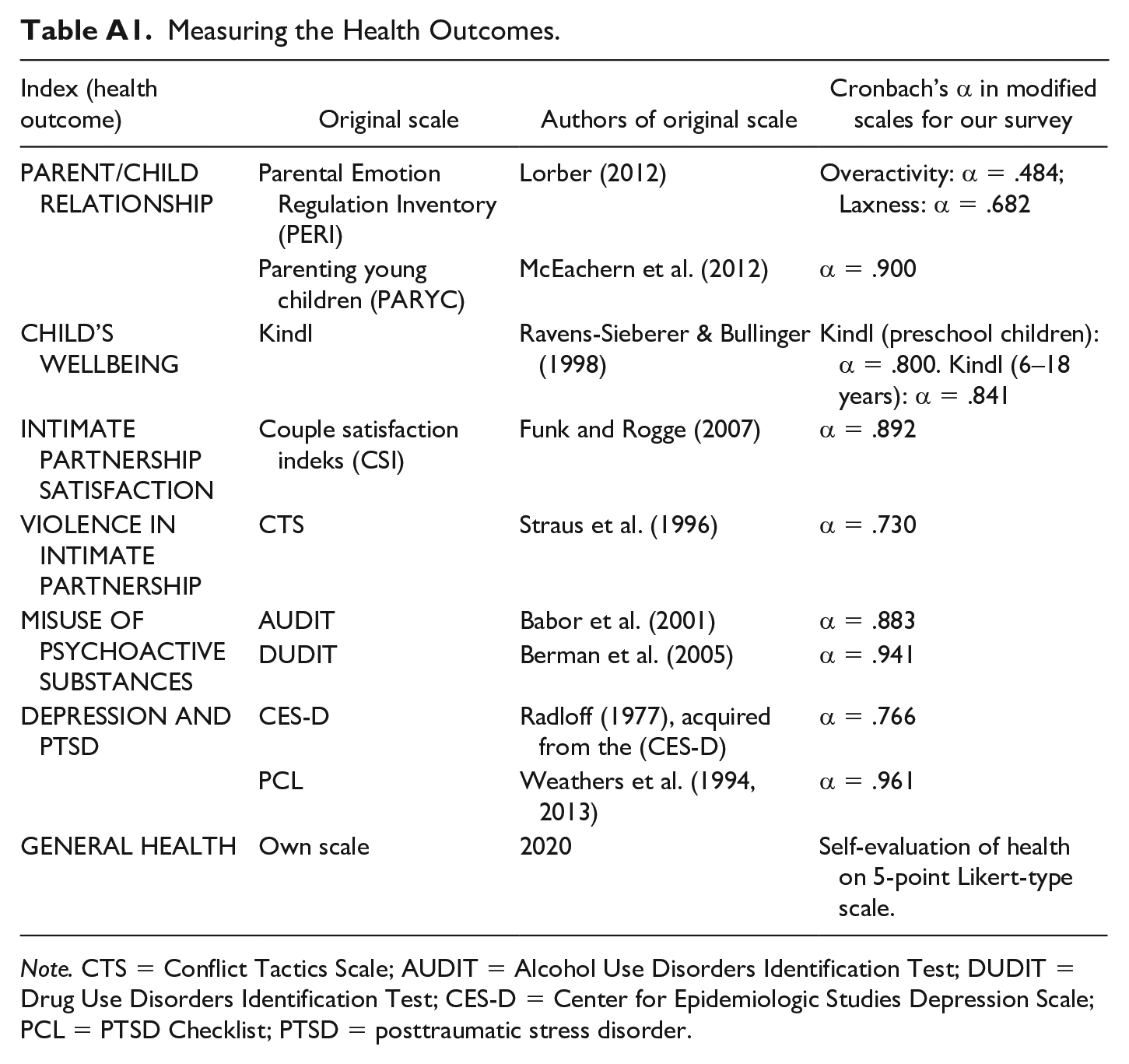
Measurement Instrument
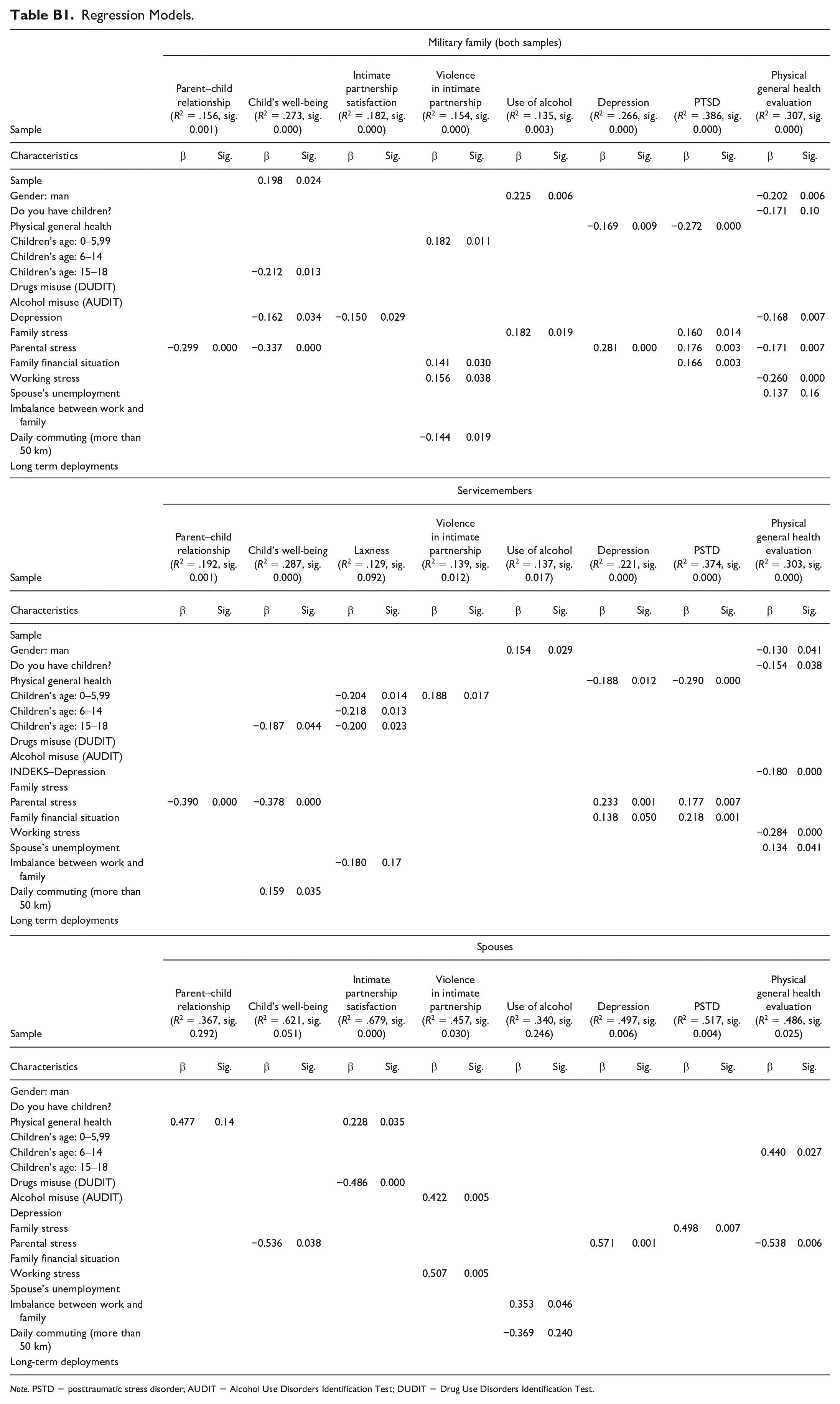
We applied the scales available in the appendix (see Table A1). Indexes representing the health outcomes were then calculated based on the originally measured scales and tested in several regression models (see Table B1: Regression models).
Linear regression analysis (enter method) was used to test which risk factors influence the individual health outcome within the observed military family unit as well as separately between the servicemembers and their spouses. 7 Authors performed analysis for 11 regression models for the military family, followed by 11 more models for the spouse data only and another 11 for the servicemember data only. The presented analysis for hypothesis testing is hence based on 33 regression models examining the impact of the selected risk factors (at various socioecological levels) on health outcomes within military families as a whole, and separately using data for the servicemembers and their spouses to detect any differences in these three groups.
Results
Sample Characteristics
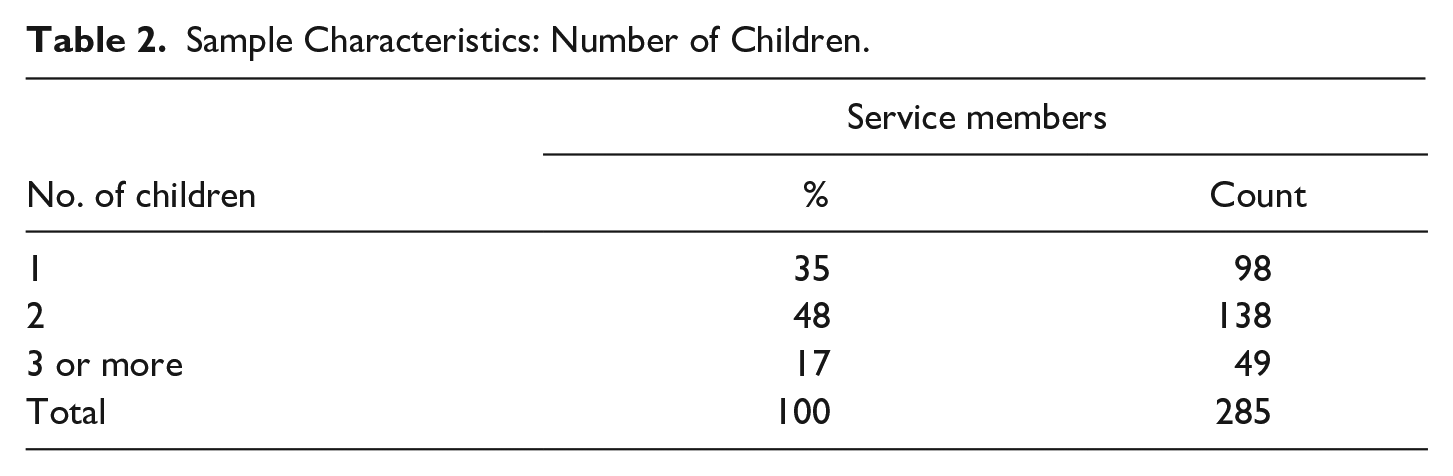
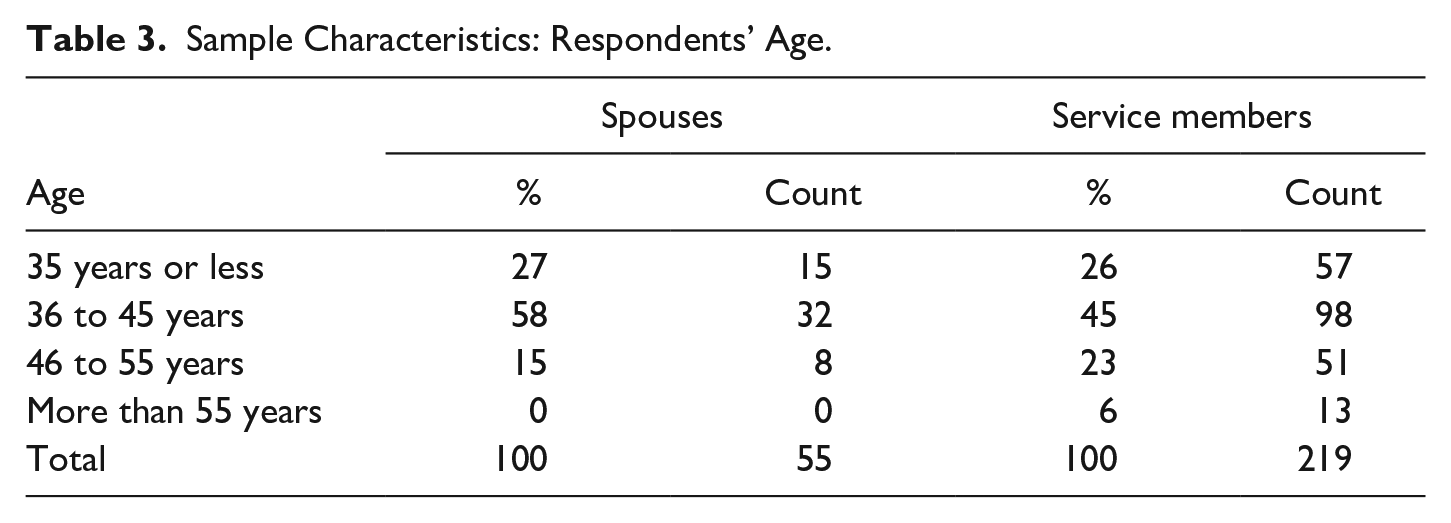
The questionnaire was answered by 368 respondents from the military population and 92 of their spouses. Altogether, the sample size is 460 respondents. Only servicemembers with at least one child were included in the research. The MilFam survey respondents included 84% of male and 13% of female 8 servicemembers, although a few of did not wish to reveal their gender. In the sample of spouses, 82% of the respondents were female and 18% were male (Tables 2 and 3).
Sample Characteristics: Number of Children.
Sample Characteristics: Respondents’ Age.
We focused on the tactical level (70% of servicemembers), noting that 25% of SAF servicemembers at the time of participating in the survey were working on the operational level and 5% on the strategic level.
The respondents’ age (41 years) is a little lower than the average (42 years) for the military population. We were specifically concentrating on families with underaged children (below 18 years), which is reflected in the age structure of our sample.
Analysis
The regression analysis for each health outcome of a military family shows the military-specific factors do not have any significant effect on the vast majority of health outcomes. However, there are a few exceptions to this. When looking at IPV within the military families (joint analysis of the data for both servicemembers and their spouses), we see that a long daily commute (β = −0.144, sig. = 0.019), together with preschool-aged children (β = 0.182, sig. = 0.011), a poor family financial situation (β = 0.141, sig. = 0.030), and stress that arises from the specific features of the work (β = 0.156, sig. = 0.038), has a weak, yet statistically significant effect. The total variance explained in IPV is 15% (R2 = .154, sig. = 0.000). Interestingly, a long daily commute works in the opposite direction: For those commuting less on a daily basis, IPV is increasing.
Furthermore, analysis of the spouse data shows that a long daily commute also has a significant effect on the consumption of alcoholic beverages (β = −0.396, sig. = 0.024), indicating that more alcoholic beverages are consumed by those whose military spouses (servicemembers) commute less than 100 km a day. Another statistically significant factor in explaining alcohol consumption is the inconsistency of sharing family obligations (β = 0.353, sig. = 0.046), indicating that alcohol misuse grows along with greater inconsistency with family obligations. However, the regression model (R2 = .340, sig. = 0.246) is not statistically significant for this health outcome.
Looking only at the servicemember data, we observe another family health outcome affected by a long daily commute—the children’s well-being. Daily commuting over a long distance has a slightly positive statistical effect (β = 0.159, sig. = 0.035) on the children’s well-being together with the child’s age (β = −0.187, sig. = 0.044). Younger-age children and less stress on the side of both parents (β = −0.378, sig. = 0.000) and aforementioned daily commuting contribute to the better well-being of children. Overall, this statistical model (R2 = .287, sig. = 0.000) is statistically significant, explaining approximately 29% of the variance in children’s well-being with respect to the risk factors included.
To conclude the analysis related to Hypothesis 1, we note that a long daily commute yields some surprising results: IPV tends to decrease the longer the distance of the commute, whereas children’s well-being tends to increase with a long commute. The latter also contributes to the lower level of alcohol misuse among nonmilitary spouses. Surprisingly, in quantitative part of our survey military deployments were not shown to have a significant effect on a military family’s health:
The linear regression analysis for all three samples—family, servicemembers and spouses—reveals that the military-specific risk factor long-term deployment indeed does not significantly affect alcohol misuse in either a military family or among servicemembers. Still, the joint data regression model (R2 = .135, sig. = 0.003) shows two factors with a slightly significantly affect on alcohol misuse, namely, gender (β = 0.225, sig. = 0.006) and stress (β = 0.182, sig. = 0.019), with stress being the main source. The data show that men in military families, either servicemembers or spouses, are more prone to misuse alcohol. Furthermore, as family-related stress increases, alcohol misuse also increases. The data set for the servicemembers produces similar regression results for alcohol misuse (R2 = .137, sig. = 0.017), with the only statistically significant factor being gender (β = 0.154, sig. = 0.029).
In the spouse sample, the data regression model (R2 = .34, sig. = 0.246) is not statistically significant with respect to alcohol misuse. However, two predictors have a significant impact on this health outcome. First, the lack of a balance in sharing domestic obligations (i.e., child care function and daily chores) between the parents affects the alcohol misuse (β = 0.353, sig. = 0.046). Second, servicemembers’ long daily commute (β = −0.396, sig. = 0.024) is negatively associated with alcohol misuse:
Linear regression models show that among the micro-level risk factors working environment proves not to be the risk factor with the greatest impact.
We now consider the modeled health outcomes that shed light on this finding. First, the model using the spouse data (R2 = .457, sig. = 0.030) shows that for IPV military working environment is indeed the strongest predictor (β = 0.507, sig. = 0.005). Another, also moderately strong, predictor is alcohol misuse (β = 0.422, sig. = 0.005), meaning that according to the spouses, the military working environment, as the biggest source of stress, along with increased alcohol misuse leads to greater IPV.
Working environment is also an explanatory factor in the military family model (R2 = .154, sig. = 0.000), although it is not the strongest one. In fact, the factors that are statistically significant—having preschool-aged children (β = 0.182, sig. = 0.011), having financial difficulties in the last year (β = 0.141, sig. = 0.030), and working-environment-related stress (β = 0.156, sig. = 0.038)—have a relatively moderate effect on IPV. In addition, short-distance daily commuting (less than 50 km per day; β = −0.144, sig. = 0.019) also adds to IPV.
Another health outcome in a military family with a military working environment (β = −0.260, sig. = 0.016) as the strongest predictor is the self-evaluation of general health (R2 = .307, sig. = 0.000). Servicemembers feel the negative impact of work-related stress on their health. The nonmilitary spouses self-evaluated their health better than the servicemembers did with regard to experiencing stress related to the military working environment.
Women in military families evaluate their health better (β = −0.202, sig. = 0.006). In addition, having fewer children (β = −0.171, sig. = 0.010), not experiencing depression or only less frequently (β = −0.168, sig. = 0.007), facing less parental stress (β = −0.171, sig. = 0.007), and the nonmilitary spouse’s unemployment (β = 0.137, sig. = 0.016) add to a better general health self-evaluation. However, it is necessary to emphasize that, although they are statistically significant, all the predictors have quite a moderate impact.
In the model using the servicemember data (R2 = .303, sig. = 0.000), a similar trend emerges as for military families—working environment is the strongest predictor (β = −0.284, sig. = 0.000) of positive self-evaluation of general health. Furthermore, being a female, having fewer kids, being less depressed, and having an unemployed nonmilitary spouse lead to a better self-evaluation of general health of a servicemember.
For all other health outcomes, working environment is not a game changer. Typically, parental stress, financial-situation challenges, and the stress emerging within the family environment affect the observed health outcomes.
Discussion
The comprehensive analysis allowed us to confirm the second hypothesis, whereas the first and third ones were rejected.
Before explaining each hypothesis, we will answer the research question. We sought to answer which risk factors on various socioecological levels most affect the family. The analysis reveals that the strongest one is parental stress on the micro level. This risk factor stands out when explaining child well-being and quality of relationship between parents and children (better relationships with their children if they experience less stress in their parenting practices). Furthermore, it is the leading predictor for depression among servicemembers and even more their spouses. Likewise, persistent PTSD can be predicted in families with increased parental stress.
The analysis indicates that financial difficulties have a negative impact on depression and PTSD and they add to the increase in psychoactive substance misuse among spouses but, interestingly, not among servicemembers. Gender plays a slight role in alcohol misuse for servicemembers because male servicemembers are prone to consume more alcohol, whereas for their spouses alcohol misuse increases with an imbalance in sharing family obligations.
The health outcome with the highest number of significant risk factors is the self-evaluation of general health. When considering the military family as a whole, being a woman, having fewer children, having less parental stress, being less exposed to military-related work stress, and being less depressed contribute to a better self-evaluation of general health (Table 4).
Empirically Testing the Models: Risk Factors With the Significant Impact on Military Family’s Health.
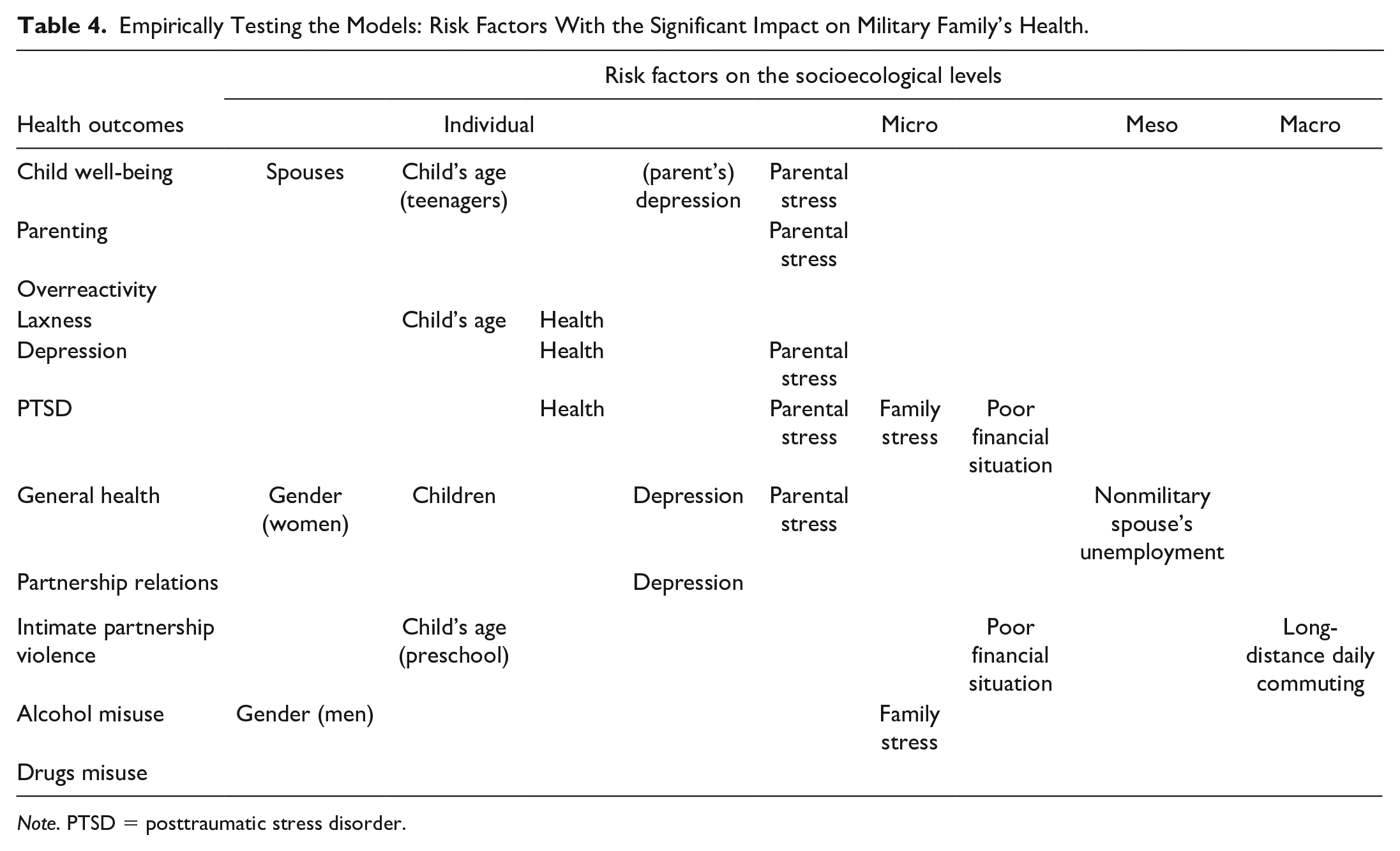
Note. PTSD = posttraumatic stress disorder.
As regard the first hypothesis, “Military-specific risk factors (i.e., deployments and long-distance daily commuting) on the macro level significantly negatively affect the health outcomes of a military family,” we may conclude that there is no support for it.
The most surprising finding after examining several regression models is the inability to detect the impact and strength of deployment on the observed health outcomes, which is even more surprising when we analyze the research data holistically. When asked directly in interviews, both the servicemembers and their nonmilitary spouses recognized the negative impact held by deployments on children of different ages (see Vuga Beršnak, 2021b), as did adult children from military families when thinking about their youth. 9
This confirms the findings of various authors mentioned above with respect to a deployment’s negative impact on children.
Still, the regression model was unable to reveal the direct impact of deployment on either child well-being or the parenting. Our regression models thus do not provide support for the first hypothesis.
Further analysis of a long daily commute, surprisingly, reveals several positive impacts. IPV tends to go down as the distance of the commute increases. The less time a violent intimate partner spends with their spouse, the less likely it is that an act of violence will occur in the relationship. Therefore, for all types of IPV, the distance of commuting helps the nonviolent spouse and the whole family avoid that violence. The analysis also shows that a servicemember’s long daily commute contributes to decreased level of alcohol misuse among nonmilitary spouses, as spouse, who spends most of the day alone with the children, must act as a responsible parent and cannot consume excessive amounts of alcohol.
The last impact of daily commuting relates to child well-being. We expected that a distant workplace reduces the opportunity for parents to spend quality time with their children, namely, that a long daily commute affects child well-being negatively. Surprisingly, our analysis does not support this assumption. On the contrary, child well-being increases with a long daily commute. This needs to be placed in the wider Slovenian social context. In our research, 70% of respondents came from the tactical level and almost two thirds were soldiers or noncommissioned officers, whose earnings are much lower than for officers. The financial reimbursement received for daily commuting could reach one third or more of one’s monthly income (depending on the home–workplace distance). Accordingly, a positive aspect of daily commuting for child well-being may be attributed to the financial benefits of having a higher monthly income. The latter contributes to the better material well-being of the whole family.
The data analysis lends support for the second hypothesis, “The macro-level military-specific risk factor ‘long-term deployment’ does not significantly affect alcohol misuse in either the military family or among servicemembers,” which may then be confirmed.
Furthermore, we had expected alcohol to be detected as a major health issue because the military is part of broader Slovenian society in which alcohol is consumed excessively. Based on the misuse of alcohol in wider society, we hypothesized that the military-specific risk factor of long-term deployment is not an important risk factor for excessive alcohol consumption within a military family, nor among the servicemembers.
In addition, there are well-established procedures for detecting alcohol misuse in the military that are regularly performed by the military police. As alcohol misuse might lead to losing one’s employment in the military, servicemembers are probably reserved when it comes to consuming alcohol. While on deployment, the misuse of alcohol might affect the performance of military tasks and result in an accident or even death, which is an extra argument against alcohol misuse during deployment.
Still, while discussing alcohol, we emphasize that on the individual level gender is a predictor for alcohol misuse. Men are prone to consume more alcohol than women. Furthermore, as family-related stress on the micro level increases, so does alcohol misuse.
Finally, we move from the macro military to the micro military and family risk factors. We hypothesized (H3) that, among risk factors on the micro level, the military working environment has the strongest negative impact. The data analysis showed the spouses reporting a higher possibility of IPV if the servicemember is subjected to stress arising from their work, when combined with excessive alcohol use. We also detected the impact of workplace stress on the self-evaluation of general health, namely, servicemembers feel that work stress negatively affects their general health. In this respect, in a military family, namely, in both samples (spouse and servicemember), women feel healthier than men. Having fewer kids and experiencing less parental stress contributes to the perception of better health, which is also related to the work–family balance and the care obligations. The data reveal that servicemembers’ perception of health is positively influenced by their nonmilitary spouses not being employed. This may be interpreted in the context of the aforementioned care obligations within the family. If the nonmilitary spouse is unemployed, they can offer full support to the servicemember and, indirectly, to the military. In Slovenia, the majority of men and women are fully employed, regardless of family size (number of children), which brings an additional burden to both parents. Traditionally, as discussed in the theoretical part of this article, a greater burden is taken on by women. We also see that the impact of parental and family stress is stronger than that of work stress. Thus, if the nonmilitary spouse is unemployed and the servicemember earns enough to support the whole family, there is less pressure on the family and the parenting, leading to the family feeling healthier.
Based on the analysis, we are unable to confirm the third hypothesis: Among the risk factors recognized on the micro level (i.e., family, working environment, parental stress, financial situation), the military working environment is the biggest risk factor for health outcomes. Although working environment is an important risk factor on the micro level, we cannot claim that it is the strongest or most frequent one. On the contrary, the obligations and potential stress rooted in the family and child care are more frequent risk factors when it comes to the health of military families in Slovenia.
Conclusion
To summarize, the model best explains the following health outcomes (with R2 higher than .200): PTSD, the self-evaluation of general health, child well-being, and depression. The least explained health outcome is substance abuse. Assumingly, the latter topic is highly sensitive and, although all ethical standards were followed while collecting the data, we may of course expect a higher degree of socially acceptable answers compared with other areas.
As discussed, some risk factors included in the regression model hold better explanatory potential than others (see Figure 2): (1) on the individual level, these are gender and the perception of general health; (2) on the micro level, we find parental stress, family-related stress, and a poor financial situation; (3) on the meso level, an imbalance in sharing family obligations and the nonmilitary spouse’s unemployment; and (4) on the macro level, the servicemember’s long daily commute.
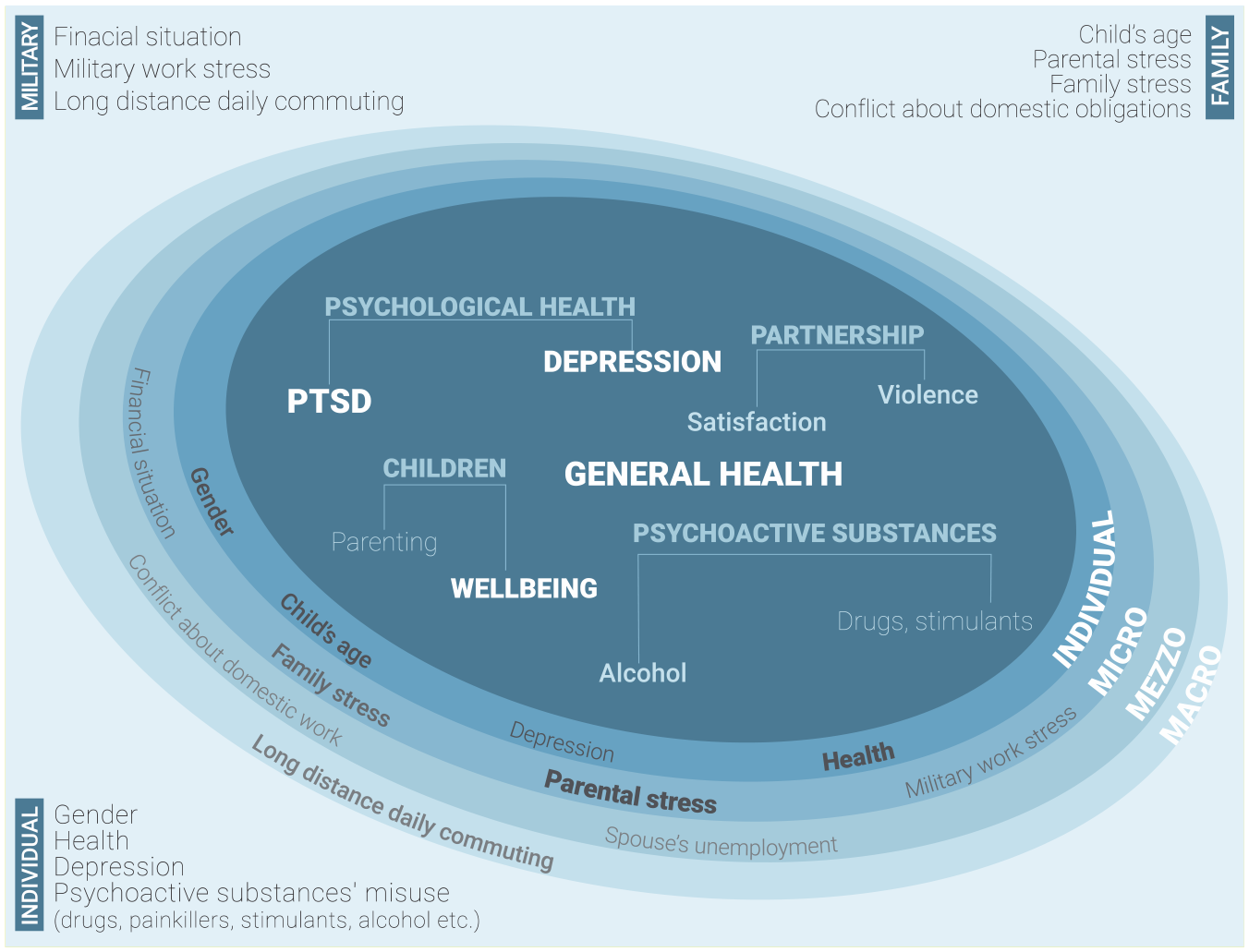
Empirically Tested Model of Risk Factors for a Military Family’s Health
The risk factors identified on various levels show that in the SAF, the military-specific risk factors on different socioecological levels are not crucial predictors for the health of a military family. One of the most surprising findings is that daily commuting, as one of the military-specific factors, was seen as being more positive than negative. A poor financial situation and work-related stress are also important risk factors.
However, we see that the most significant are in fact the family-related risk factors such as parental and family stress or an imbalance in sharing family obligations. The analysis also reveals the desire of servicemembers to have an unemployed nonmilitary spouse, who would take on the “burden” of family obligations and reduce the impact of the demands of both the family and the military. The latter corresponds to the Slovenian traditional perception of gender roles in the family. However, the spouses do not confirm the basis for such desires as our analysis does not offer any indication that nonmilitary spouses are willing to stay home and offer full support to their military spouses (and, indirectly, to the SAF).
In the end, we must emphasize that the study was performed during the pandemic years and the research team had to carry out the research in several lockdown periods, entailing working from home, home schooling, and more intensive tasks among the servicemembers that left them with less time and energy to participate in the survey and in other unexpected and extraordinary circumstances. This is undoubtedly a limitation of our survey as it was not conducted in an optimal environment using a face-to-face approach, but instead through the use of e-tools. Despite that, the results are clear-cut and we believe that in further analysis it will be necessary to upgrade our regression models with the protective factors. We will observe changes in military families’ health caused by the protective factors, namely, whether and how strong they alleviate the role played by the risk factors in a military family’s health.
Footnotes
Appendix A
Measuring the Health Outcomes.
| Index (health outcome) | Original scale | Authors of original scale | Cronbach’s α in modified scales for our survey |
|---|---|---|---|
| PARENT/CHILD RELATIONSHIP | Parental Emotion Regulation Inventory (PERI) | Lorber (2012) | Overactivity: α = .484; Laxness: α = .682 |
| Parenting young children (PARYC) | McEachern et al. (2012) | α = .900 | |
| CHILD’S WELLBEING | Kindl | Ravens-Sieberer & Bullinger (1998) | Kindl (preschool children): α = .800. Kindl (6–18 years): α = .841 |
| INTIMATE PARTNERSHIP SATISFACTION | Couple satisfaction indeks (CSI) | Funk and Rogge (2007) | α = .892 |
| VIOLENCE IN INTIMATE PARTNERSHIP | CTS | Straus et al. (1996) | α = .730 |
| MISUSE OF PSYCHOACTIVE SUBSTANCES | AUDIT | Babor et al. (2001) | α = .883 |
| DUDIT | Berman et al. (2005) | α = .941 | |
| DEPRESSION AND PTSD | CES-D | Radloff (1977), acquired from the (CES-D) | α = .766 |
| PCL | Weathers et al. (1994, 2013) | α = .961 | |
| GENERAL HEALTH | Own scale | 2020 | Self-evaluation of health on 5-point Likert-type scale. |
Note. CTS = Conflict Tactics Scale; AUDIT = Alcohol Use Disorders Identification Test; DUDIT = Drug Use Disorders Identification Test; CES-D = Center for Epidemiologic Studies Depression Scale; PCL = PTSD Checklist; PTSD = posttraumatic stress disorder.
Appendix B
Regression Models.
| Military family (both samples) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample | Parent–child relationship |
Child’s well-being |
Intimate partnership satisfaction |
Violence in intimate partnership |
Use of alcohol |
Depression |
PTSD |
Physical general health evaluation |
||||||||
| Characteristics | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. |
| Sample | 0.198 | 0.024 | ||||||||||||||
| Gender: man | 0.225 | 0.006 | −0.202 | 0.006 | ||||||||||||
| Do you have children? | −0.171 | 0.10 | ||||||||||||||
| Physical general health | −0.169 | 0.009 | −0.272 | 0.000 | ||||||||||||
| Children’s age: 0–5,99 | 0.182 | 0.011 | ||||||||||||||
| Children’s age: 6–14 | ||||||||||||||||
| Children’s age: 15–18 | −0.212 | 0.013 | ||||||||||||||
| Drugs misuse (DUDIT) | ||||||||||||||||
| Alcohol misuse (AUDIT) | ||||||||||||||||
| Depression | −0.162 | 0.034 | −0.150 | 0.029 | −0.168 | 0.007 | ||||||||||
| Family stress | 0.182 | 0.019 | 0.160 | 0.014 | ||||||||||||
| Parental stress | −0.299 | 0.000 | −0.337 | 0.000 | 0.281 | 0.000 | 0.176 | 0.003 | −0.171 | 0.007 | ||||||
| Family financial situation | 0.141 | 0.030 | 0.166 | 0.003 | ||||||||||||
| Working stress | 0.156 | 0.038 | −0.260 | 0.000 | ||||||||||||
| Spouse’s unemployment | 0.137 | 0.16 | ||||||||||||||
| Imbalance between work and family | ||||||||||||||||
| Daily commuting (more than 50 km) | −0.144 | 0.019 | ||||||||||||||
| Long term deployments | ||||||||||||||||
| Servicemembers | ||||||||||||||||
| Sample | Parent–child relationship |
Child’s well-being |
Laxness |
Violence in intimate partnership |
Use of alcohol |
Depression |
PSTD |
Physical general health evaluation |
||||||||
| Characteristics | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. |
| Sample | ||||||||||||||||
| Gender: man | 0.154 | 0.029 | −0.130 | 0.041 | ||||||||||||
| Do you have children? | −0.154 | 0.038 | ||||||||||||||
| Physical general health | −0.188 | 0.012 | −0.290 | 0.000 | ||||||||||||
| Children’s age: 0–5,99 | −0.204 | 0.014 | 0.188 | 0.017 | ||||||||||||
| Children’s age: 6–14 | −0.218 | 0.013 | ||||||||||||||
| Children’s age: 15–18 | −0.187 | 0.044 | −0.200 | 0.023 | ||||||||||||
| Drugs misuse (DUDIT) | ||||||||||||||||
| Alcohol misuse (AUDIT) | ||||||||||||||||
| INDEKS–Depression | −0.180 | 0.000 | ||||||||||||||
| Family stress | ||||||||||||||||
| Parental stress | −0.390 | 0.000 | −0.378 | 0.000 | 0.233 | 0.001 | 0.177 | 0.007 | ||||||||
| Family financial situation | 0.138 | 0.050 | 0.218 | 0.001 | ||||||||||||
| Working stress | −0.284 | 0.000 | ||||||||||||||
| Spouse’s unemployment | 0.134 | 0.041 | ||||||||||||||
| Imbalance between work and family | −0.180 | 0.17 | ||||||||||||||
| Daily commuting (more than 50 km) | 0.159 | 0.035 | ||||||||||||||
| Long term deployments | ||||||||||||||||
| Spouses | ||||||||||||||||
| Sample | Parent–child relationship |
Child’s well-being |
Intimate partnership satisfaction |
Violence in intimate partnership |
Use of alcohol |
Depression |
PSTD |
Physical general health evaluation |
||||||||
| Characteristics | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. | β | Sig. |
| Gender: man | ||||||||||||||||
| Do you have children? | ||||||||||||||||
| Physical general health | 0.477 | 0.14 | 0.228 | 0.035 | ||||||||||||
| Children’s age: 0–5,99 | ||||||||||||||||
| Children’s age: 6–14 | 0.440 | 0.027 | ||||||||||||||
| Children’s age: 15–18 | ||||||||||||||||
| Drugs misuse (DUDIT) | −0.486 | 0.000 | ||||||||||||||
| Alcohol misuse (AUDIT) | 0.422 | 0.005 | ||||||||||||||
| Depression | ||||||||||||||||
| Family stress | 0.498 | 0.007 | ||||||||||||||
| Parental stress | −0.536 | 0.038 | 0.571 | 0.001 | −0.538 | 0.006 | ||||||||||
| Family financial situation | ||||||||||||||||
| Working stress | 0.507 | 0.005 | ||||||||||||||
| Spouse’s unemployment | ||||||||||||||||
| Imbalance between work and family | 0.353 | 0.046 | ||||||||||||||
| Daily commuting (more than 50 km) | −0.369 | 0.240 | ||||||||||||||
| Long-term deployments | ||||||||||||||||
Note. PSTD = posttraumatic stress disorder; AUDIT = Alcohol Use Disorders Identification Test; DUDIT = Drug Use Disorders Identification Test.
Acknowledgements
We would like to thank the members of the Slovenian Armed Forces and their spouses who participated in our survey. Special thanks also go to the entire MilFam research team as well as external experts who supported us in various stages of the research process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Slovenian Research Agency (research project J5-1786) and conducted within the framework of the Defence Research Center (program P5-0206).