
Abstract
Volitional impairment is central to the civil commitment of sexually violent persons (SVPs), yet little is known about how forensic professionals define and assess this construct. This study surveyed 29 experienced SVP evaluators (mean experience > 20 years) to examine their conceptualizations and assessment practices. Participants completed open-ended questions, rated 31 potential indicators on Likert-type scales, and evaluated two hypothetical cases. While some consensus emerged on key indicators—including repeated treatment failure, lack of insight, persistent deviant urges, verbalized loss of control, self-regulation deficits, and disregard for consequences—case analyses revealed substantial, often contradictory, variability in expert conclusions. Agreement on hypothetical cases was only 79% and 72% per vignette, with critical discrepancies even within the same legal jurisdictions. These findings demonstrate that statutory language alone does not account for differences, leading to inconsistent evaluations. The study highlights an urgent need for clearer operational definitions and structured tools to enhance assessment reliability.
Keywords
The civil commitment of sexually violent persons (SVPs) represents one of the most complex intersections of law, psychology, and public policy. Such commitments hinge on the contentious construct of volitional impairment—a notion central to distinguishing individuals with a history of sexual offense convictions who are unable to control their behavior from those who choose to commit crimes despite adverse consequences (Morse, 1998; Schopp, 2001). Forensic professionals must navigate a fragmented landscape of statutory definitions, judicial interpretations, and empirical research to make determinations that significantly impact individual liberties and public safety (Mercado et al., 2005).
The seminal cases of Kansas v. Hendricks (1997) and Kansas v. Crane (2002) have framed much of the legal discourse on SVP commitments. In Hendricks, the U.S. Supreme Court upheld the Kansas SVP Act, authorizing the civil confinement of individuals deemed unable to control their behavior due to a “mental abnormality or personality disorder.” This decision introduced the concept of volitional impairment as a constitutional threshold for commitment but failed to define it, prompting widespread criticism for its ambiguity (Schopp, 2001). The Court opined, “. . . admitted lack of volitional control, coupled with future dangerousness, adequately distinguishes Hendricks from other dangerous persons who are perhaps more properly dealt with exclusively through criminal proceedings” (Hendricks, p. 360). Five years later, in Crane, the Court revisited the volitional impairment issue, clarifying that a “complete lack of control” was not required for commitment but that the state must demonstrate “serious difficulty in controlling behavior.” While this ruling added nuance, it did little to provide specific guidance for assessing behavioral control, leaving lower courts and forensic professionals to wrestle with its practical application.
The Crane decision has since catalyzed a wide array of state-level interpretations. These interpretations generally fall into three broad categories (Pierson, 2012): implicit lack-of-control theory, nested lack-of-control theory, and treating control as a separate element.
Implicit Lack-of-Control Theory
States following the implicit lack-of-control theory assume that proving a mental abnormality and future dangerousness establishes lack of control, thus negating the need for a separate finding on the issue. For example, in Wisconsin’s In re Laxton (2002), the court held that lack of control was inherently established by the nexus between mental abnormality and dangerousness, making a separate finding unnecessary. Similarly, Florida’s State v. White (2004) adopted this reasoning, concluding that the presence of a mental abnormality and predisposition to sexual violence implied a lack of control. Texas courts (e.g., In re Commitment of Taylor, 2010) have also upheld commitments without requiring separate proof of lack of control, arguing that a predisposition to sexual violence is sufficient. However, critics argue that this approach disregards the constitutional safeguard outlined in Crane, as it risks conflating predisposition with an inability to control. As Justices Scalia and Thomas noted in Crane, referencing the majority opinion in Hendricks,
it could not be clearer that, in the Court’s estimation [in Hendricks], the very existence of a mental abnormality or personality disorder that causes the likelihood of repeated sexual violence in itself establishes the requisite “difficulty if not impossibility” of control. (Crane, p. 419)
Nested Lack-of-Control Theory
The nested lack-of-control theory embeds the requirement of lack of control within the statutory definition of mental abnormality, linking the two concepts more explicitly. Arizona’s In re Leon G. (2002) exemplifies this approach, interpreting the statutory language requiring proof of a mental disorder that makes an individual likely to engage in sexual violence as inherently including a lack-of-control component. Similarly, Illinois’s People v. Masterson (2003) and Massachusetts’s In re Dutil (2002) have held that a mental abnormality causing serious difficulty in controlling behavior satisfies the Crane requirement. While this approach offers a closer causal connection between the mental disorder and the individual’s dangerous behavior, it risks conflating mental abnormality with volitional impairment. Critics warn that this analytical conflation weakens Crane’s constitutional safeguard by allowing jurors to assume that a mental abnormality automatically implies impaired volitional capacity, even though these concepts are intended as distinct.
Control as a Separate Element
Some states take a stricter approach by requiring a separate finding on lack of control, treating it as an independent component of the state’s burden of proof. Missouri’s Thomas v. State (2002) reversed a SVP commitment due to inadequate jury instructions that failed to include lack of control as a distinct requirement. Similarly, Kansas’s In re Care & Treatment of Ward (2006) explicitly required a finding of lack of control as a separate element and relied on testimony regarding the defendant’s resistance to treatment and compulsive behaviors. In New Jersey’s In re W.Z. (2002), the court remanded the case due to the absence of specific findings on volitional impairment but did not provide guidelines for evaluating volitional impairment. While this approach adheres more closely to Crane’s mandate, states following this interpretation often lack operational clarity on what constitutes serious difficulty in controlling behavior. Consequently, these jurisdictions rely heavily on case-specific factors and expert testimony, which can introduce variability and subjectivity into the process.
The divergent state-level interpretations of Crane reveal the challenges in aligning legal standards with scientific assessments of control. States following the implicit theory risk eliminating the constitutional safeguard by failing to separately address volitional impairment, while those employing the nested theory often conflate mental abnormality with control. In contrast, states requiring separate findings preserve the procedural protections of Crane but face the challenge of defining volitional impairment in a consistent and operationally clear manner.
Across all approaches, courts frequently depend on expert testimony to assess volitional impairment. This type of testimony is controversial because clear guidelines for these assessments do not exist. Some effort has been made to provide guidance for assessing volitional impairment in the context of the insanity defense (Rogers & Shuman, 2000), but there is no analog for SVPs. The absence of standardized guidelines results in purely subjective expert testimony that is likely to vary across examiners, both between and within jurisdictions and hearings. Indeed, the lack of a specific definition and operationalization of volitional impairment led to criticisms that it “lacks substance” (Janus, 2001), lacks a normative basis (Schopp, 2001), and is “untenable,” “meaningless,” and “unworkable” (Association for the Treatment of Sexual Abusers [ATSA], 2001). Although these critiques emerged over two decades ago, SVP laws persist in 20 states, the District of Columbia, and at the federal level (Sreenivasan, Rokop, et al., 2020). Thus, clarifying the meaning of volitional impairment as it relates to SVP civil commitment is necessary to adequately structure opinions offered to legal decision-makers, explain why certain individuals are suitable for commitment and differentiate between them in a non-arbitrary manner.
Defining Volitional Impairment and Related Constructs
The concept of volitional impairment has been described in myriad ways and using several terms, including impulsiveness, recklessness, deficits in self-control, poor self-regulation, and disinhibition (e.g., McCann & Garcia, 1999; Tangney et al., 2004). There are wide differences in how volitional impairment has been conceptualized in the literature. These variations reflect differing theoretical frameworks, methodological approaches, and definitions. Some perspectives emphasize the inability to control one’s actions despite awareness of their consequences, while others focus on deficits in decision-making, impulse regulation, or situational constraints.
Factors Potentially Relevant to Volitional Impairment Opinions
Despite the elusiveness of a widely accepted definition of volitional impairment, several factors have been identified as potentially relevant for their presumed association with volitional impairment generally and when applied to an SVP candidate. A summary of various resources on this topic is provided below, which underscores the importance of considering the interplay of person and situational forces in its assessment.
Hall (1985) suggests that “massive stress” and “certain organic conditions” may compromise behavioral controls, emphasizing the significance of situational factors, transient emotional states, and substance use in assessing loss of control. Notably, efforts to resist or evade specific behaviors may reflect a lack of volitional capacity, whereas engaging in alternative actions to avert anticipated responses may indicate intact volitional control.
Morse (1994) explored the complexities of “control” with regard to excuses for wrongdoing and identified several self-protective variables that contribute to an individual’s ability to exercise control over their actions. These include self-awareness and self-monitoring, fear of consequences, rationality (encompassing accurate perception and appropriate reasoning), a desire for moral behavior, emotional control, empathy, the ability to suppress desires, and good judgment or practical wisdom.
Burton et al. (1998) operationalized the construct of self-control by identifying several key components. These include limited frustration tolerance, desire for immediate gratification, inadequate patience, preference for risk, tendency to engage in physical rather than mental contemplation, and self-reported instances of crime and other reckless behaviors.
Doren (2002) proposed two key dimensions for evaluating volitional impairment. The first relates to an impaired ability to learn from negative consequences, which may be observed in individuals who repeatedly engage in harmful behaviors despite previous punishment. The second relates to a constrained view of choices. For example, individuals with paraphilic disorders may exhibit a limited set of sexual behaviors that override their ability to consider alternative actions or consequences.
Rogers and Shuman (2005) identified several factors hypothesized to be indicative of volitional impairment in those with a history of sexual offending. These include a lack of capacity for meaningful choice, which is reflected in an impaired ability to make rational decisions after carefully considering options; a disregard for personal consequences, such as evidenced by the continuation of certain behaviors despite negative repercussions; an incapacity for delay, particularly in terms of postponing immediate gratification; and the chronicity of offending, indicated by behavior that is persistent rather than a series of isolated incidents.
Mercado et al. (2005) highlighted several key factors, including impulsivity, risk-taking, lack of empathy, poor self-regulation, low frustration tolerance, and limited insight that obstructs an individual’s ability to govern their actions and leads to a preference for immediate gratification without considering potential consequences. In a follow-up study, legal professionals, psychologists, and jury-eligible undergraduates were surveyed to investigate how four key factors—verbalized lack of control, history of sexual crimes, offense planning, and substance use—relate to assessments of volitional impairment. Their results found that the surveyed groups identified verbalization of lack of control and history of pedophilic behavior as significant factors, while no notable effect was found for the degree of offense planning or substance use.
Jackson and Hess (2007) noted that the combination of personality disorders and previous sexual offenses may amplify impulsive and uncontrollable behavior. In addition, the presence of a paraphilia or paraphilic disorder is likely to restrict behavioral choices, compromising an individual’s ability to manage sexual impulses. Clinical assessments that consider the severity of these conditions and the individual’s awareness of the consequences of their actions may also inform volitional opinions. Patterns of repetitive offending suggest a persistent lack of control, while self-reports from individuals with a history of sexual offending may provide insights into their impaired volition. Neuropsychological assessments may also provide evidence of impulse control deficits. Observations of impulsivity during incarceration, supervision, treatment, or confrontational interviews suggest the presence of ongoing challenges within structured environments. Evaluators need to delineate clearly how an individual’s mental disorder(s) impede behavioral control, particularly given the absence of precise legal or clinical definitions of volition.
The Code of Federal Regulations (CFR) § 549.95 addresses the civil commitment of sexually dangerous persons and outlines considerations related to “serious difficulty in refraining from sexually violent conduct or child molestation if released” (Department of Justice, 2008). The regulation indicates that determinations regarding volitional impairment may include the following factors, though they are not limited to them: (a) evidence of repeated contact or attempted contact with one or more victims of sexually violent conduct or child molestation, (b) denial of or inability to appreciate the harm, wrongfulness, or likely consequences of engaging or attempting to engage in sexually violent conduct or child molestation, (c) results from interviews, testing, or risk assessment tools, (d) indicators such as offending under supervision, offending despite the likelihood of being caught, expressed intent to re-offend, and admission of an inability to control behavior, and (e) completion or failure to complete sex offending treatment programs.
Winsmann (2012) emphasized the importance of structured professional judgment and an idiographic approach, suggesting that dysfunction in frontal lobe activity can lead to “perseverative responses” that reduce an individual’s ability to inhibit impulsive actions despite negative outcomes. To assess decision-making and impulsivity effectively, Winsmann recommends utilizing tools such as the Wisconsin Card Sorting Test (WCST), the Iowa Gambling Task (IGT), and the Barratt Impulsiveness Scale–11th edition (BIS-11). It also highlights the necessity of considering both historical and current behavior in addition to testing to obtain a thorough understanding of their volitional impairment, cautioning against relying solely on past actions to determine impairment in behavioral control.
Current Study
Despite the critical role of volitional impairment in SVP commitment proceedings, there is a striking lack of empirical knowledge about how practicing forensic professionals conceptualize and apply the construct. This gap raises significant concerns about the reliability of forensic assessments. The present study investigates how a select group of forensic professionals conceptualize and assess volitional impairment in the context of SVP civil commitment evaluations. The primary goal is to identify the factors forensic experts consider relevant, understand their interpretations of key concepts, and examine the variability in their judgments using case vignettes. Understanding these perspectives is essential for developing guidelines, improving assessment practices, and ensuring fairness and scientific rigor in forensic evaluations. The Institutional Review Board at University of California, Irvine approved this study.
Method
Transparency and Openness
The study adheres to the Transparency and Openness Promotion (TOP) Guidelines. The data and survey materials are available at https://osf.io/6b4cq/?view_only=422ff2352203400f846e99fa264b781c. No preregistration was conducted for this study.
Participants
The participants in this study were drawn from a pool of forensic professionals specializing in conducting SVP evaluations. This pool was identified through two primary sources: a list of evaluators board-certified in forensic psychology by the American Board of Professional Psychology (ABPP) who listed SVP commitment as an area of expertise, and the researchers’ existing knowledge of individuals who frequently conduct SVP assessments. These evaluators were contacted via email, which included a link to the study and detailed instructions for participation.
The email informed potential participants that the study would take approximately 30 to 45 minutes. It involved a series of questions and scenarios related to their professional expertise in assessing volitional impairment. Upon completion of the study, participants were offered a US $50 Amazon gift card as compensation. Despite the well-known limitations of the convenience sampling method, the study targeted an extremely specific group of forensic professionals to ensure a focused and knowledgeable sample whose insights could meaningfully inform the study’s objectives.
Twenty-nine participants completed the study, which took a median of 37 minutes to complete. All participants held doctoral degrees, including PhDs (n = 22, 76%) and PsyDs (n = 6, 21%), as well as medical degrees (MD; n = 1, 3%). All identified their primary areas of expertise as forensic psychology and psychiatry. A significant portion of the sample (72%) was board-certified in forensic psychology or forensic psychiatry, reflecting their advanced qualifications in this area.
Participants varied in the years they had been practicing as licensed clinicians. Some had 5 to 10 years of experience (14%), while roughly half of the sample (48%) reported practicing for over 20 years. Their involvement in SVP civil commitment evaluations ranged from occasional assessments (1 to 5 per year; 48% of the sample) to regular (6 to 15 per year; 21%) to frequent involvement (16 or more per year; 24%). Throughout their careers, participants reported conducting anywhere from fewer than 10 (14% of the sample) to more than 100 SVP evaluations (55% of the sample), highlighting both early-career and highly experienced practitioners.
Participants reported the extent to which their professional practice involved working with individuals who had committed sexual offenses. For some (10% of the sample), these cases comprised less than 10% of their workload, while for others (31% of the sample), this population made up the majority (76% to 100%) of their practice. Half of the sample indicated that 50% or more of the professional practice involved working with this population. The average number of years working with this population was 21.4 (SD = 10), with a range of 6 to 46 years. The participants primarily practice in 14 different states, the most common states being New York (17% of the sample), Minnesota (10% of the sample), Texas (10% of the sample), and Wisconsin (10% of the sample).
While all participants had received formal training in assessing the risk of sexual offending, a minority (35%) had received specific training or education on assessing volitional impairment in SVP cases. When asked to describe the training, several participants indicated that they could not recall or found it challenging to distinguish between training on risk assessment and volitional impairment assessment. When asked about their comfort level in assessing volitional impairment, 21% of the sample reported being somewhat or extremely uncomfortable, while 72% reported being somewhat or extremely comfortable, and 7% reported being neither comfortable nor uncomfortable. A majority (72%) indicated that they used a combination of structured risk assessment and clinical judgment when assessing volitional impairment. Some participants noted that they rely on collateral information (e.g., documented evidence of recent rule violations or other records) and statements about being unable to resist impulses.
Procedure
This study had four sections. The first section of the study involved open-ended questions to gather participants’ personal and professional views on volitional impairment. The use of open-ended questions was intended to limit suggestibility. Participants were asked the following:
Please list the factors you consider important in assessing volitional impairment during SVP commitments. Are there specific clinical or behavioral “red flags” that suggest that an individual has significant volitional impairment? How do specific legal definitions or requirements in your jurisdiction influence your assessment of volitional impairment? In your experience, how well do the legal criteria for volitional impairment align with clinical reality? How do you handle cases where volitional control fluctuates over time (e.g., periods of control vs. periods of offending)?
To understand participants’ threshold for volitional impairment, they were asked, “At what point do you consider a lack of control over sexual behavior sufficient to qualify as volitional impairment in the context of SVP civil commitment evaluations?” There were four response options:
The second section involved a Likert-type-scale assessment of 31 factors that may or may not be relevant to volitional impairment. Participants rated each factor on a 5-point scale, ranging from “strong evidence against volitional impairment (This option strongly suggests that volitional control is intact.)” to “strong evidence supporting volitional impairment (This option strongly suggests that volitional control is impaired.).” This allows the study to quantify the weight experts attribute to various factors in their evaluations. The items were presented in randomized order. The 31 factors are as follows:
In the third section, participants were presented with two hypothetical cases designed to analyze their approaches to assessing volitional impairment and to identify variability in their judgments. These vignettes illustrate various scenarios where the concept of volitional impairment is complex, enabling us to examine how forensic professionals apply their expertise in nuanced contexts. They also highlight the factors that evaluators prioritize, such as treatment success, external influences (e.g., alcohol use), and the persistence of deviant impulses.
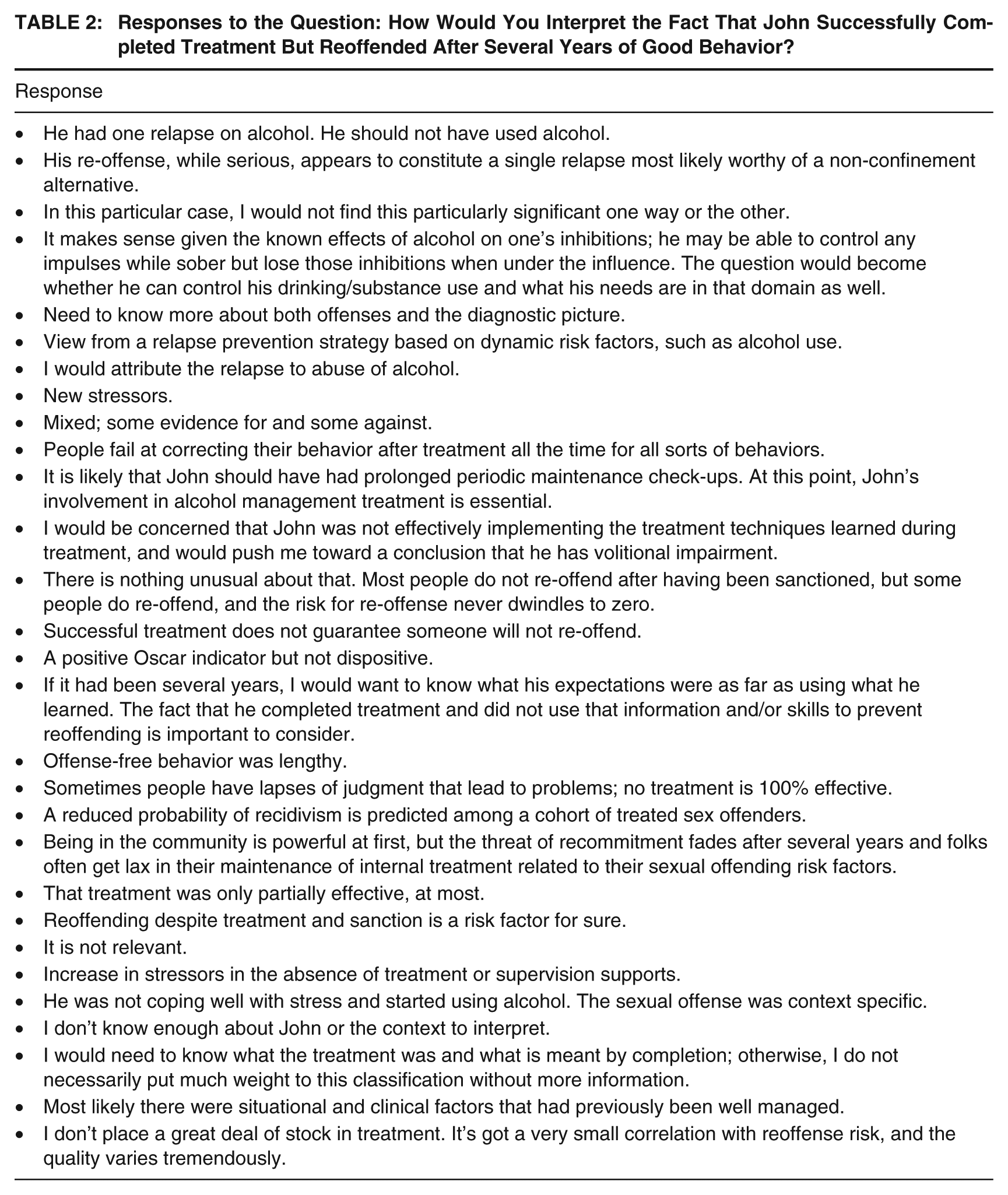
The first vignette described John, a 45-year-old man, who has a history of sexual offending. John was convicted of sexually assaulting a co-worker 10 years ago, served a prison sentence, and completed an outpatient treatment program. For several years after his release, John maintained a stable job, demonstrated good behavior, and reported no sexual offending. However, he recently reoffended by sexually assaulting a stranger at a bar after consuming alcohol. He cited stress at work and heavy drinking as factors that impaired his ability to control his impulses.
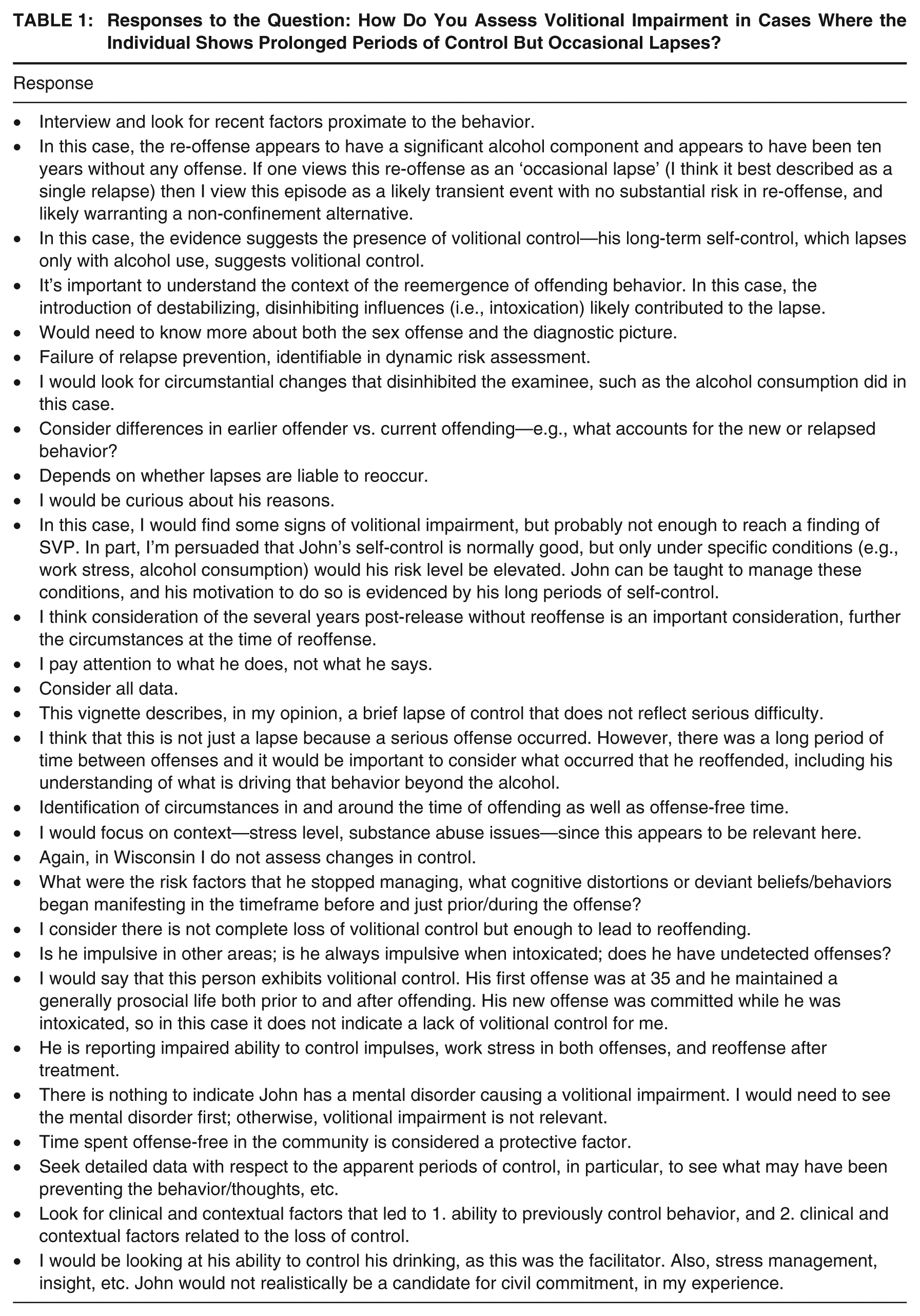
This vignette highlighted a situation where prolonged periods of self-regulation are interrupted by isolated lapses, prompting participants to evaluate how such patterns align with the criteria for volitional impairment. Participants were asked the following questions about John: How do you assess volitional impairment in cases where the individual exhibits prolonged periods of control but occasionally lapses? How would you interpret the fact that John completed treatment but reoffended after several years of good behavior? Based on the above information, would you conclude that John meets the legal criteria for volitional impairment?
The second vignette described David, a 35-year-old man with a long history of deviant sexual fantasies involving minors, though he has never physically acted on these urges. David voluntarily sought therapy and has consistently attended sessions for 5 years to manage his thoughts. Despite his proactive efforts, David admits that his fantasies are persistent, intrusive, and sometimes dominate his thoughts for several hours a day. Recently, he was found to have downloaded child sexual abuse material, though he insists he has no intention of harming a child physically. He claims he lacks control over his urges to consume this material.
This vignette presents a case of ongoing internal struggle, allowing us to explore how persistent deviant fantasies and related actions, like consuming illegal material, influence assessments of volitional impairment and risk for escalation. Participants were asked the following questions about David: How do you assess volitional impairment in cases where the individual shows prolonged periods of control but occasional lapses? Does the fact that David downloaded child pornography affect his risk of contact offending in the future? The fourth section collected demographic information about the participants, which was reported above.
Results
Personal and Professional Views on Volitional Impairment
The complete set of responses to the open-ended questions appears in Online Supplement (available in the online version of this article). There is significant variability in the extent to which impairment must be evident for the individual to qualify as demonstrating volitional impairment. No participants required “complete loss of control.” Only 10% of participants found “minor lapses in control” sufficient, 41% found “moderate lapses in control” sufficient, and 48% of the sample required “significant loss of control” to meet the threshold. The differences in thresholds suggest that even if evaluators considered and gave the same weight to factors, they would arrive at different conclusions regarding volitional impairment.
Evaluation of Factors Relevant to Volitional Impairment
Participants’ ratings of 31 items assessing their evidentiary value for supporting a finding of volitional impairment are presented in Figure 1. Overall, 32% of responses were categorized as neutral/no impact, 34% as moderate evidence supporting, and 24% as strong evidence supporting. This distribution suggests that the majority of items were viewed as having at least moderate relevance to evaluations of volitional control.
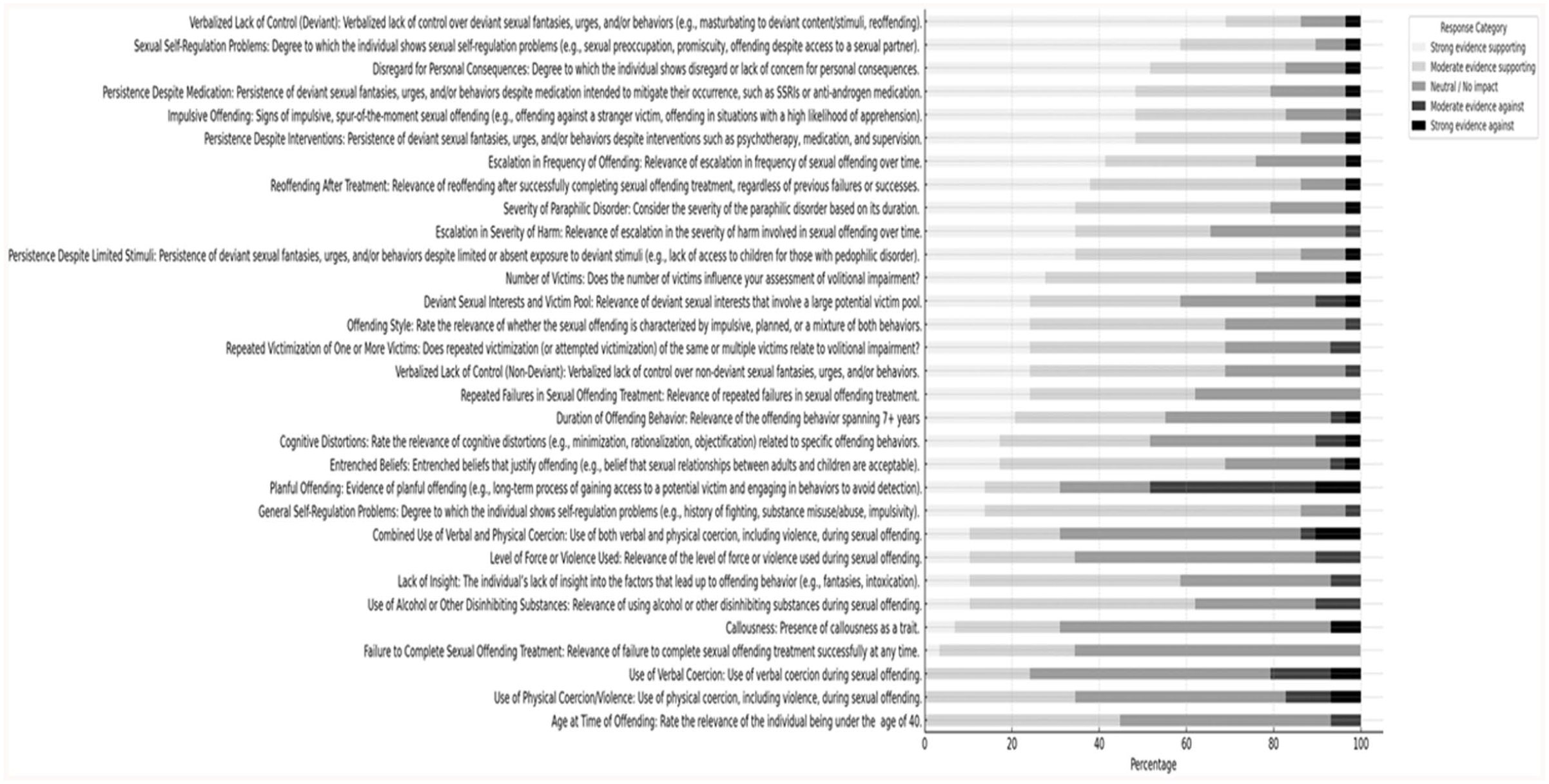
Relevance of Different Factors for Assessing Volitional Impairment
Several items received particularly strong support. Verbalized Lack of Control (Deviant) emerged as the most strongly endorsed, with 69% of respondents rating it as strong evidence supporting. Sexual Self-Regulation Problems received 59% strong support, and Disregard for Personal Consequences garnered 52%. Persistence Despite Medication and Impulsive Offending each received 48% strong support, further highlighting their perceived importance.
Items with the lowest proportion of neutral/no impact responses reflect areas where respondents expressed more decisive views. Sexual Self-Regulation Problems had the lowest neutrality (7%), followed by Verbalized Lack of Control (Deviant), Reoffending After Treatment, General Self-Regulation Problems, and Persistence Despite Limited Stimuli, each with only 10% neutral responses. These findings suggest that respondents viewed these items with greater clarity and consensus regarding their evidentiary significance.
While several items generated strong support, others revealed considerable divergence in opinion. Items such as Number of Victims, Failure to Complete Sexual Offending Treatment, and Duration of Offending Behavior received a relatively even spread across response categories, suggesting less agreement among respondents. This distribution may indicate that these factors are perceived as context-dependent or of uncertain relevance to volitional impairment. Their interpretive weight may vary based on other characteristics of the case.
A small subset of items received higher proportions of responses indicating moderate or strong evidence against volitional impairment. In particular, the Use of Alcohol or Other Disinhibiting Substances and Age at the Time of Offense were viewed skeptically, with some respondents discounting their relevance altogether. This pattern suggests that these factors, although potentially associated with offending behavior, may not be seen as directly implicating impaired volitional control.
The most strongly endorsed items—such as Control Issues (Deviant), Sexual Self-Regulation Problems, and Persistence Despite Medication—reflect internal, dispositional features related to impaired self-regulation. These items align closely with psychological theories of volitional dysfunction and appear to resonate with evaluators’ conceptualizations of impaired control. In contrast, externally observable or demographic factors received comparatively less support.
Several items, including Cognitive Distortions, Planful Offending, and Entrenched Beliefs, received high proportions of neutral/no impact responses. This pattern may reflect perceived ambiguity about their relevance or legal significance, or a belief that their implications depend on additional contextual factors. High neutrality could also signal ambivalence stemming from unclear statutory definitions or conflicting interpretations of case law.
Applied Analysis of Volitional Impairment
Applied Analysis of John
Participants’ open-ended responses to the questions about John are provided in Tables 1 and 2.
Responses to the Question: How Do You Assess Volitional Impairment in Cases Where the Individual Shows Prolonged Periods of Control But Occasional Lapses?
Responses to the Question: How Would You Interpret the Fact That John Successfully Completed Treatment But Reoffended After Several Years of Good Behavior?
Overall, 21% of participants determined that John would meet the legal criteria for volitional impairment, and 79% determined he would not. It is conceivable that some of the disagreement among participants may stem from different statutory definitions of volitional impairment, which vary by state, as noted in the introduction. To explore this possibility, we examined the agreement rate among evaluators in each state (thus holding constant the statutory definition of volitional impairment). Table 3 reports the rate of agreement for each state in which there was more than one evaluator; the evaluators reached the same conclusion in five of the nine states with multiple evaluators.
Inter-Rater Agreement of Whether “John” Meets the Criteria for Volitional Impairment
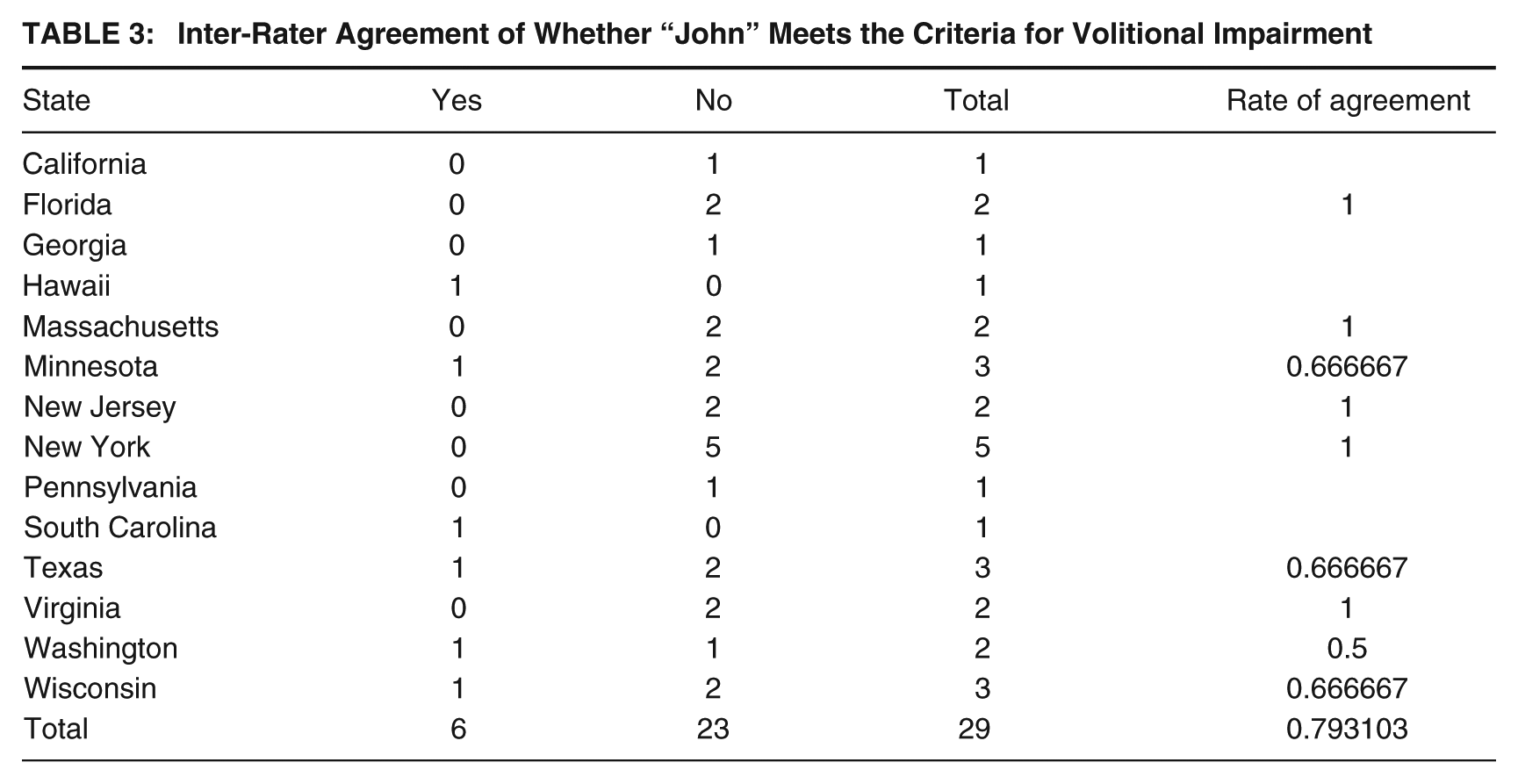
The total rate of agreement is essentially a weighted average, as it takes into account the differing total cases for each state. This means that states with larger totals contribute more heavily to the overall agreement rate. Overall, evaluators reached the same conclusion 79% of the time when holding constant the state in which they practice.
Applied Analysis of David
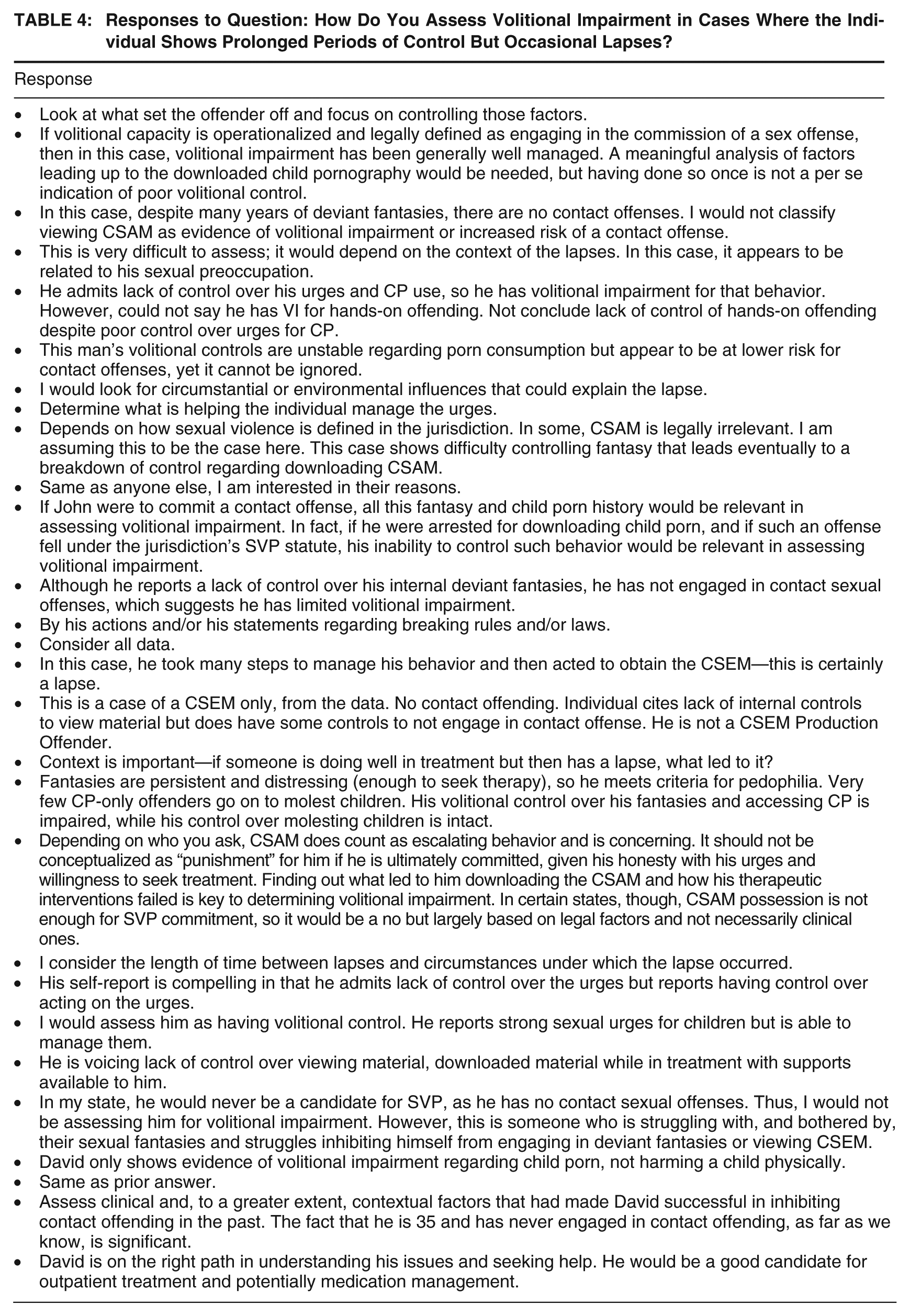
Participants’ open-ended responses to the questions about David are provided in Tables 4 and 5.
Responses to Question: How Do You Assess Volitional Impairment in Cases Where the Individual Shows Prolonged Periods of Control But Occasional Lapses?
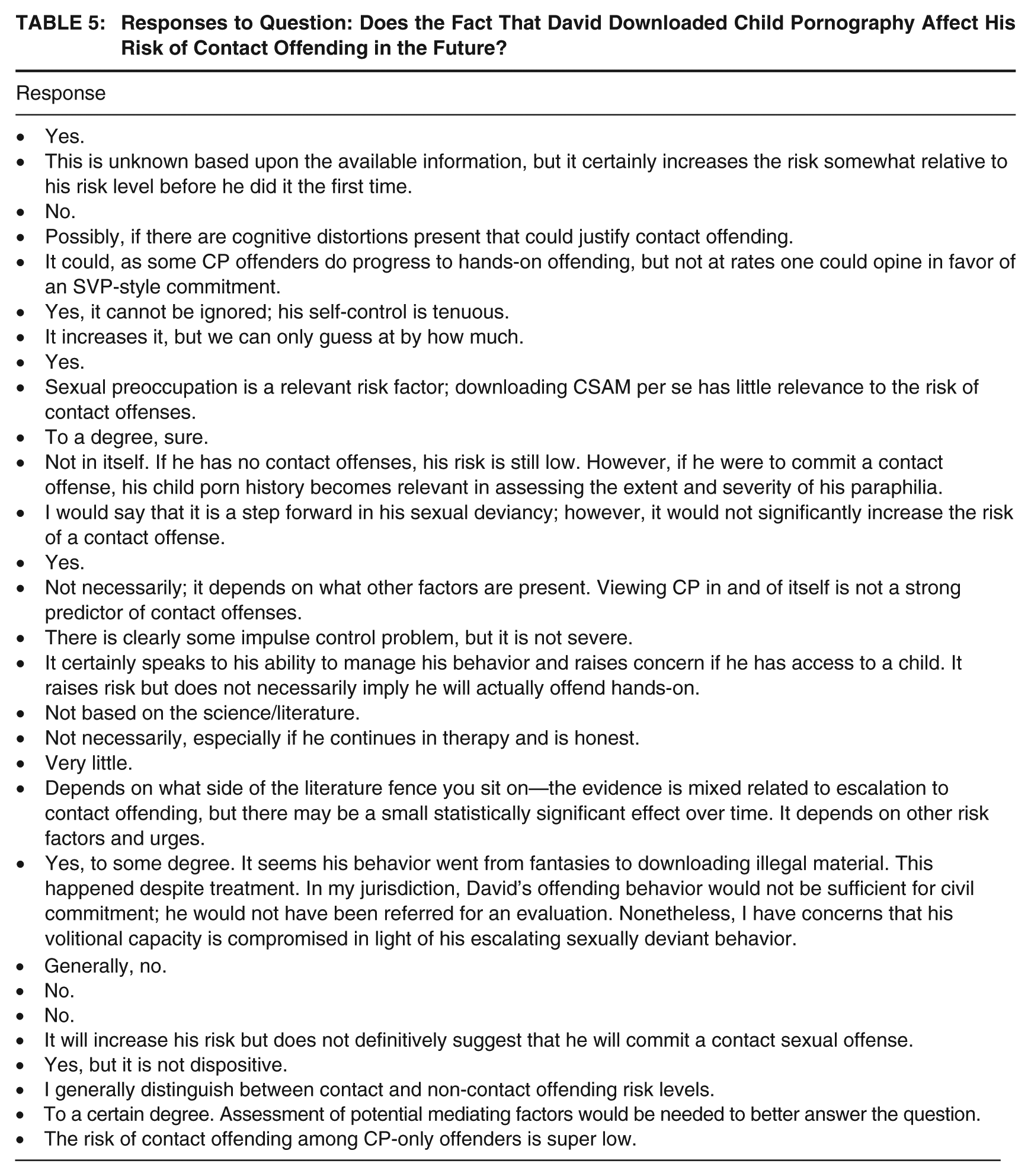
Responses to Question: Does the Fact That David Downloaded Child Pornography Affect His Risk of Contact Offending in the Future?
Overall, 28% of participants determined that David would meet the legal criteria for volitional impairment, and 72% determined he would not. We examined the agreement rate among evaluators in each state, thus holding constant the statutory definition of volitional impairment. The results appear in Table 6.
Inter-Rater Agreement of Whether “David” Meets the Criteria for Volitional Impairment
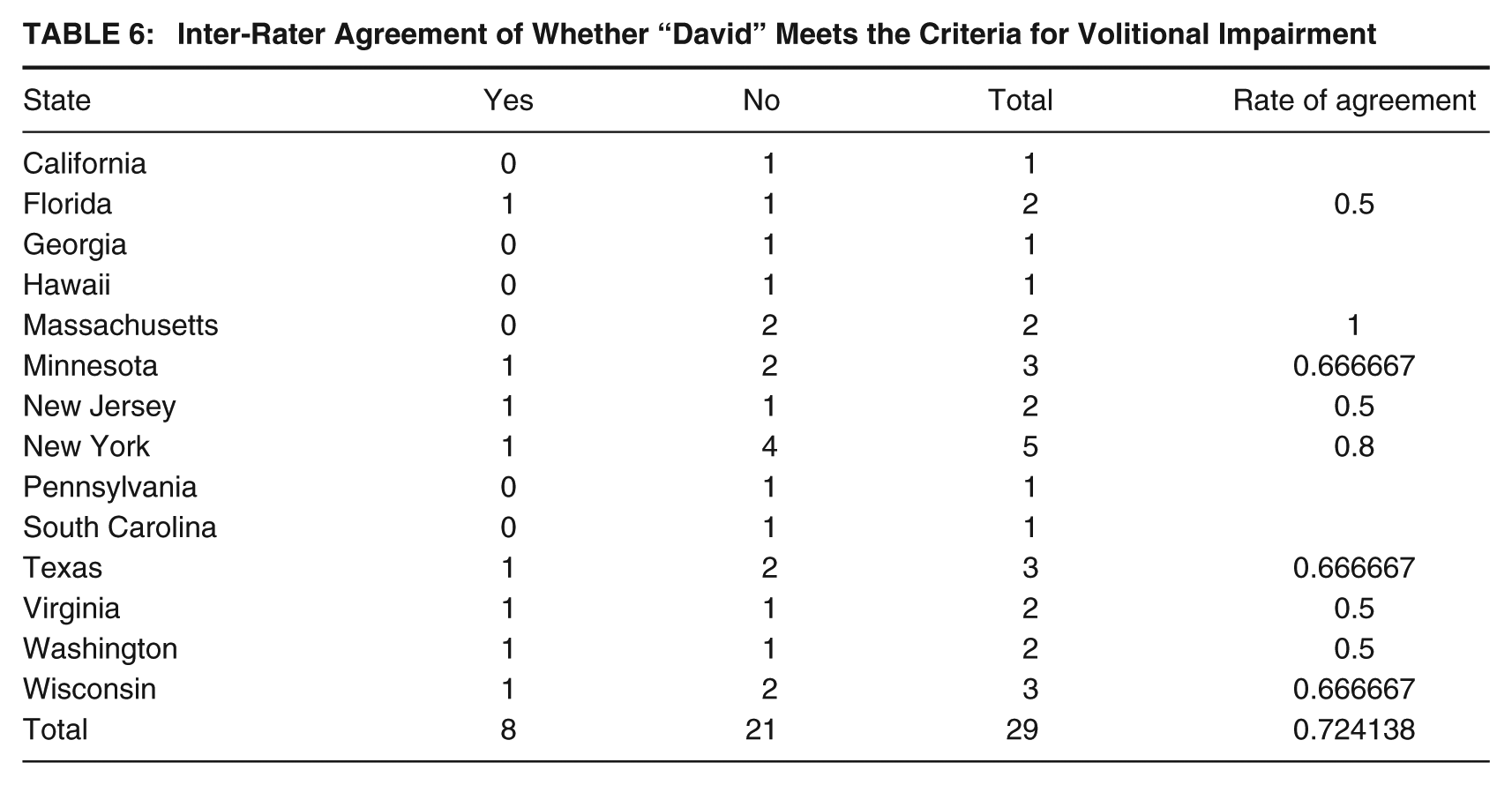
The rate of agreement is reported for each state in which there was more than one evaluator; the evaluators reached the same conclusion in only one of the nine states with multiple evaluators. This decidedly low rate of agreement is concerning.
Discussion
The present study highlights significant variability in how forensic professionals conceptualize and assess volitional impairment in the context of Sexually Violent Person (SVP) civil commitment evaluations. Our findings indicate that, despite the centrality of volitional impairment to SVP statutes, there is no consistent or standardized approach to its assessment among evaluators. These results align with prior critiques that the concept lacks clear operational definitions, making it difficult to apply in a reliable and scientifically rigorous manner.
One of the most striking findings was the considerable variation in evaluators’ interpretations of volitional impairment. Although certain factors, such as persistent deviant urges, repeated treatment failure, and disregard for personal consequences, were widely endorsed as relevant indicators, the weight given to these factors differed substantially across participants. This inconsistency suggests that forensic evaluators are influenced by their jurisdictional definitions, professional training, and personal frameworks for understanding self-regulation and behavioral control.
Our analysis of hypothetical case vignettes further underscores this variability. For the case of John, whose long period of behavioral control was disrupted by an alcohol-related sexual offense, 79% of evaluators determined that he did not meet the criteria for volitional impairment, while 21% concluded that he did. Similarly, in the case of David, who exhibited persistent deviant fantasies but had no history of contact offenses, evaluators were divided, with 72% concluding that he did not meet the criteria and 28% determining that he did. These disparities persisted even when holding jurisdiction constant, as evaluators practicing within the same legal framework often reached different conclusions about the presence of volitional impairment.
Limitations
While this study provides valuable insights into the variability of forensic assessments of volitional impairment in SVP civil commitment evaluations, several methodological limitations should be considered when interpreting the findings. First, the study relied on a relatively small sample of forensic evaluators (N = 29). Although the participants were highly experienced professionals, their perspectives may not fully represent the broader population of forensic evaluators who conduct SVP assessments. In addition, as participation was voluntary, there is the potential for self-selection bias. As a result, those with strong opinions on volitional impairment may have been more likely to participate. This may have influenced the degree of variability observed in the findings. Second, the study design relied on self-reported assessments and vignette-based judgments rather than direct case evaluations or real-world forensic reports. While hypothetical scenarios offer a controlled way to assess evaluator decision-making, they do not fully capture the complexity of real-world cases, where additional contextual factors, longitudinal behavioral data, and legal arguments influence determinations.
The study also does not account for the role of adversarial legal settings in shaping forensic opinions. In real-world SVP proceedings, evaluators often serve as expert witnesses for either the state or the defense, potentially influencing their interpretations based on legal advocacy rather than purely clinical reasoning. Future research should examine whether evaluators’ assessments shift depending on their role in adversarial settings and whether training in forensic neutrality could mitigate such influences.
Despite these limitations, this study highlights critical gaps in the assessment of volitional impairment and underscores the need for clearer guidelines and standardized tools to improve forensic evaluations in SVP commitment cases. Addressing these methodological challenges in future research will be essential to ensuring more consistent, reliable, and legally defensible determinations of volitional impairment.
Implications for Legal and Clinical Practice
The observed variability in assessments raises important concerns about the consistency and fairness of SVP commitment proceedings. Given that a determination of volitional impairment can result in indefinite civil confinement, it is imperative that forensic evaluations be as reliable and objective as possible. Our findings suggest that, without standardized guidelines, these determinations may be highly subjective, potentially leading to arbitrary or inconsistent application of SVP statutes (Jackson & Hess, 2007; Mercado et al., 2005).
From a clinical practice perspective, these findings suggest that forensic evaluators should adopt a more structured and evidence-based approach when assessing volitional impairment. One immediate takeaway is the need for evaluators to distinguish between transient situational factors (e.g., intoxication, stress) and enduring impairments in behavioral control. Many evaluators in our study appeared divided on how to interpret lapses in self-regulation, some attributing them to volitional impairment, others viewing them as manageable risk factors. To address this, clinicians should integrate longitudinal data into their assessments, examining patterns of behavior over time rather than isolated incidents of loss of control.
Another important implication for clinical practice is the necessity for forensic professionals to clarify their conceptualization of volitional impairment within their reports. Given that different evaluators apply different thresholds for impairment, standardizing language in forensic reports may enhance judicial understanding and reduce subjective variability in court decisions. For example, instead of using broad, undefined terms such as “difficulty controlling behavior,” forensic reports should specify whether an individual exhibits volitional impairment across different contexts despite structured interventions and whether their behavior is resistant to known treatment modalities (Mercado et al., 2006).
Clinicians conducting SVP assessments should also consider adopting structured professional judgment (SPJ) tools specifically designed for volitional impairment, much like how actuarial risk assessment tools (e.g., Static-99R) are used in recidivism evaluations. Currently, the field lacks an equivalent measure for assessing impaired volition. Developing and utilizing such tools would help forensic professionals systematically consider all relevant factors, minimizing subjective bias in their evaluations (Sreenivasan, Hoffman, et al., 2020).
In addition to individual assessment practices, these findings also have broader policy implications. The legal system relies heavily on expert testimony in SVP cases, yet our study underscores the risk of variability in forensic opinions undermining the integrity of commitment decisions. Courts may benefit from judicial training on the limitations of forensic evaluations regarding volitional impairment, as well as clearer statutory guidelines that delineate the necessary threshold for commitment (DeMatteo et al., 2015). Without more precise legal and clinical alignment, commitment decisions may continue to be inconsistent, creating due process concerns and potential legal challenges.
Need for Standardized Guidelines and Assessment Tools
Developing standardized guidelines for assessing volitional impairment is particularly challenging due to the absence of “ground truth” for what constitutes impaired volition. Unlike risk assessment tools, which can be validated against measurable recidivism outcomes, volitional impairment is a subjective and legally constructed concept that lacks clear biological or behavioral markers. As a result, creating a reliable and valid assessment tool would require a multi-step, iterative process involving empirical research, expert consensus, and legal validation.
A structured tool for volitional impairment could be developed through a Delphi method, where a panel of forensic psychologists, psychiatrists, legal scholars, and policymakers systematically refine consensus-based criteria (e.g., Singh et al., 2015). This tool could incorporate empirically supported risk factors, behavioral indicators, and structured interview components. To ensure reliability, items should be weighted based on their demonstrated association with expert determinations of volitional impairment in prior cases. Further validation should involve retrospective case analyses to assess the tool’s consistency across evaluators and its predictive validity regarding judicial determinations.
In addition, the tool should distinguish between chronic versus situational loss of control, integrating case-specific contextual factors. For example, evaluators could be required to code for the persistence of deviant urges across multiple settings, resistance to treatment interventions, and observable impulsivity in institutional or supervised environments. Developing standardized scoring rubrics, akin to structured professional judgment risk assessment tools, would further enhance inter-rater reliability and ensure a more defensible forensic opinion in court.
Until such tools are developed, clinicians should take several practical steps to improve the reliability of their assessments. First, evaluators should synthesize multiple data sources, such as treatment records, clinical interviews, actuarial risk scores, and collateral reports, to construct a well-rounded assessment of volitional capacity. Forensic reports should explicitly document the evaluator’s rationale, linking behavioral evidence to legal definitions of volitional impairment. This may involve providing detailed justifications for why certain indicators were weighted more heavily in the final determination. Evaluators should participate in collaborative training sessions with attorneys and judges to ensure forensic testimony aligns with legal expectations and statutory interpretations of volitional impairment. Before a structured tool is created, clinicians can benefit from using structured case templates that outline key indicators of volitional impairment and require evaluators to systematically document their analysis.
Conclusion
This study highlights the substantial inconsistencies in forensic evaluations of volitional impairment, raising concerns about the reliability of SVP commitment determinations. Our findings emphasize the need for clearer legal definitions, standardized assessment procedures, and enhanced forensic training to ensure that evaluations are conducted in a fair, objective, and scientifically grounded manner. Future research should explore the development of structured assessment tools and investigate how legal and clinical frameworks can be harmonized to improve the consistency of volitional impairment evaluations in SVP cases.
Supplemental Material
sj-docx-1-cjb-10.1177_00938548251389454 – Supplemental material for Unraveling Volitional Impairment: Forensic Psychological Perspectives on Volitional Impairment in Sexually Violent Person Commitments
Supplemental material, sj-docx-1-cjb-10.1177_00938548251389454 for Unraveling Volitional Impairment: Forensic Psychological Perspectives on Volitional Impairment in Sexually Violent Person Commitments by Nicholas Scurich, Marc A. Martinez and Daniel A. Krauss in Criminal Justice and Behavior
Footnotes
Authors’ Note:
The authors have no conflicts of interest to report. The study materials and data reported in this manuscript are available here: ![]() . The data and ideas presented in this manuscript have not been previously disseminated in any public forum. They have not been presented at conferences, posted online, or shared through other public channels.
. The data and ideas presented in this manuscript have not been previously disseminated in any public forum. They have not been presented at conferences, posted online, or shared through other public channels.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.