
Abstract
Suicide remains the leading cause of death in U.S. correctional facilities, underscoring the importance of identifying factors contributing to elevated risk. Drawing on national data on jail fatalities from 2011 to 2019, this study examines suicide risk across macro-level (community infrastructure), meso-level (facility characteristics), and micro-level (individual vulnerabilities) domains. Multivariate regression analyses indicate that, at the micro-level, being young, White, male, unconvicted, or serving a short length of stay increases suicide likelihood. Rural isolation is associated with higher suicide rates, whereas overcrowding is linked to lower rates. Interaction models further demonstrate that rural jails without overcrowding experience the highest suicide rates. Findings highlight the complex interplay among individual, facility, and community factors, pointing to the need for targeted, multi-level prevention efforts. Policy, practice, and research implications are discussed to inform evidence-based strategies for reducing suicide in correctional settings.
Introduction
Jail suicide is the leading cause of death in U.S. correctional facilities (Noonan & Carson, 2011). In U.S. jails, the suicide mortality rate is 46 per 100,000 persons in custody, which is significantly higher than the rate of 13.4 per 100,000 in the general population and 16 per 100,000 in prison (Carson & Cowhig, 2020). Between 2001 and 2019, suicides accounted for 24% to 35% of all deaths among persons in local jail, compared to 5% to 8% of deaths in state and federal prisons (Carson, 2021). During this period, jail suicides rose 13%, with more than half occurring within the first 30 days of incarceration—an area of concern for correctional administrations, researchers, and the public. Suicide victims share common risk factors with the general population, including prior attempts, mental illness, substance use disorders, and depressive symptoms (Goss et al., 2002; Suto & Arnaut, 2010). However, these issues are highly concentrated in jails, where nearly 48% of detainees have both mental illness and substance use disorders (Meyer et al., 2014). This population often cycles through jails for low-level, nonviolent offenses (Xin et al., 2024).
Despite their high needs, jails struggle to provide adequate treatment due to practical and methodological constraints (Bronson & Berzofsky, 2017). A major challenge is high turnover—many individuals are confined for only hours or days with uncertain release times, making comprehensive assessments and treatment difficult (Dalbir et al., 2024). When institutional neglect combines with overcrowding, low staffing ratios, and restricted freedom, it exacerbates individual pre-existing problems to increase suicide risk (Dye, 2010; Hayes, 2012). This is particularly concerning given that approximately 7 million people cycle through jails annually (Zeng, 2023), with 428,000 admitted multiple times each year. Jails are the correctional setting with the most public contact. Pretrial detainees, who make up 65% of jail populations, are often held because they cannot afford bail (Sawyer & Wagner, 2023). Jail suicides disproportionately affect marginalized individuals facing poverty, unemployment, and unstable housing (Barker et al., 2014). Socioeconomic disadvantages increase the likelihood of prolonged pretrial detention, a concern given that 77% of jail suicide victims (2000–2019) were pretrial detainees (Carson, 2021). Without clearer insight into contributing factors, these individuals remain at risk. This study addresses the gap by examining individual, facility, and community factors and offering prevention recommendations. While limited to cases of in-custody deaths and thus not generalizable to the broader jail population, this study offers valuable insight by profiling suicide deaths relative to other deaths, helping to inform prevention efforts.
Suicide Risk Factors
Micro-Level Factors: Individual Characteristics
The importation model suggests that incarcerated individuals’ behavior stems from personal characteristics that may be maladaptive in correctional settings. Applied to jail suicide, it argues that demographic, psychological, and social factors best explain suicidal behavior (Dye, 2010), as individuals bring pre-existing attitudes, values, and experiences that influence their risk while incarcerated. Justice-involved individuals with pre-existing health and behavioral conditions, including mental illnesses like depression or schizophrenia (Craig et al., 2024; Yi et al., 2017), untreated substance use disorders (Singer et al., 2025), co-occurring disorders, or a history of suicide attempts (Dalbir et al., 2024), become especially more vulnerable in custody. Although suicide is not a mental illness, it is often linked to untreated or undiagnosed mental health conditions (Goss et al., 2002; Hanson, 2010). Many individuals enter custody with unmet psychological needs, and the abrupt transition to confinement intensifies distress due to the sudden loss of medications, health care, and social support (Tartaro, 2019). This heightened stress can trigger feelings of helplessness, depression, trauma, and anxiety, increasing suicide risk (Cunha et al., 2023; Tripodi & Bender, 2007). Hayes (2012) found about one-third of jail suicide victims had a history of mental illness or suicidal behavior.
Research has identified individual-level characteristics linked to jail suicides (Dillon, 2013; Hanson, 2010). Earlier studies found that victims are often young, single, White males, typically arrested for nonviolent offenses and intoxicated at arrest (Hayes, 1989; Mumola & Noonan, 2008). More recent data show a shift, with nearly half of jail suicides involving charges for violent or personal offenses such as murder, rape, drug possession, driving under the influence (DUI), and assault (Hayes, 2012). Hanging remains the predominant method, usually with bedding or clothing (Carson, 2021; Hayes, 1989). From 2000 to 2019, most victims were aged 25–44 (Carson, 2021), although suicides among individuals 55 and older rose by 6% between 2015 and 2019, reflecting the growing presence of older adults in jail suicides. While many victims were placed in isolation and died within 24 hours of incarceration (Davis & Muscat, 1993), more recent trends show a decline in first-day suicides, with risk peaking between 24 and 48 hours and again after 60 days (Frottier et al., 2002). The U.S. Bureau of Justice Statistics reports that 66% of jail suicides (2015–2019) occurred within the first 30 days, most within the first 2 weeks (Carson, 2021).
Meso-Level Factors: Facility Characteristics
The deprivation model (Sykes, 1958) explains that the behavior of persons in custody could be explained by deprived prison or jail environments. Harsh incarceration conditions, such as overcrowding, restricted autonomy, and inadequate health care, often contribute to severe psychological distress, elevating suicide risk (Craig et al., 2024). In these situations, jail suicide can emerge as a response to adverse conditions, driven by frustration and a hostile atmosphere that fosters maladaptive behavior. Thus, the jail environment itself can become a catalyst for suicidal behavior given the anguish or pain it causes individuals. Hanson (2010) found that institutional overcrowding combined with institutional instability and the presence of a violent environment may lead to an increase in correctional suicides. Villarreal (2015) found suicides are more likely in overcrowded, maximum-security facilities. Housing arrangements like single-cell or isolated housing with limited supervision are critical risk factors (Dye, 2010). Facility size also matters: small- to medium-sized jails (under 100 beds) have suicide rates two to six times higher than larger facilities, with the highest rates in jails holding fewer than 50 individuals (Dillon, 2013; Tartaro & Ruddell, 2006). Alarmingly, fewer than 20% of these jails conduct formal suicide assessments at intake, and only about half provide annual suicide prevention training (Tartaro & Ruddell, 2006). Their remote locations further limit access to care during detention and after release. With limited local health providers, jails often focus on short-term stabilization over long-term treatment, leaving them ill-equipped to manage high-risk individuals (Batastini et al., 2020; Skubby et al., 2013).
Jails face unique challenges as temporary detention centers unlike prisons. Jails house diverse populations, including pretrial detainees, individuals awaiting transfer, probation or parole violators, those with mental health issues, and people under the influence (Subramanian et al., 2015; Tartaro, 2019). Managed by local governments, jails vary in treatment quality and living conditions based on community resources, leading to inconsistent care, harming mental health, and increasing suicide risk. Busy booking areas with high admissions, discharges, and agitated individuals complicate care (Irwin, 1985). In smaller rural jails, budget constraints, understaffing, rushed screenings, and limited programming exacerbate challenges (Ellison et al., 2018). Combined with population diversity and scarce resources, these conditions mirror maximum-security deprivation, while incarceration shock, loss of control, separation from social support, and interpersonal conflict further elevate suicide and self-harm risks (Hayes, 2012; Tartaro, 2019).
Macro-Level Factors: Community Characteristics
Community-level factors play a critical, although often underexplored, role in understanding jail suicides. While individual and facility characteristics remain important, the broader community infrastructure (resources, accessibility, and proximity) substantially shapes the health and safety of incarcerated individuals. The current study introduces a theoretical framing for understanding and connecting community resources to what occurs within a correctional setting. Through the lens of socio-ecological resilience, access to resources or various forms of capital, such as economic or social capital, is essential for a social unit (e.g., a person or place) to endure and persist (i.e., the first stage of resilience) following exposure to an internal or external threat (see St John & Nemati, 2024). Without key resources, people and places are unlikely to withstand internal and external threats. Here, a subset of the Resilient Infrastructure Framework (RIF) can be applied to explore community factors influencing jail dynamics in greater depth (Caverzan & Solomos, 2014).
The RIF highlights how systems withstand, adapt to, and recover from disruptions while maintaining critical services (Gardoni & Murphy, 2020). This extends beyond physical structures like buildings and transportation (Vishnu et al., 2018) to social infrastructure such as health care and social services (Canada et al., 2022). Hospital proximity signals potential access to care (Guagliardo, 2004) and reflects community health care capacity (Deng & Bennett, 2023). Stronger health care systems are linked to healthier communities and life-saving outcomes, including suicide prevention (Bertoli & Grembi, 2017; Nicholl et al., 2007). The argument is that resilient infrastructures reduce life-threatening risks. Hospital placement also highlights geographical barriers to care (Stacherl & Sauzet, 2023). In the United States, proximity to health care institutions guides resource allocation, as seen in Health Professional Shortage Areas, which use spatial distance to direct federal support (Health Resources and Services Administration, n.d.). This proximity–health link also holds internationally, as shown in studies from China (Du et al., 2024) and Canada (Bissonnette et al., 2012).
RIF is particularly relevant to jails, where in-facility health care depends heavily on community resources. Integration with emergency medical and mental health services is essential for safety (Batastini et al., 2020; Skubby et al., 2013). While few studies explicitly apply RIF, findings show hospital proximity strengthens jail resilience (Rosen et al., 2024) by relieving facilities of severe mental health cases. Helms et al. (2016) state:
. . . the presence of community hospitals is generally a strong indicator of a dense network of medical and mental health professionals operating in proximity to the hospitals. Their professional presence and capacity for offering treatment services in the community is likely to be associated with a reduced perceived need for mental health operations within the jail environment. Many jails operating in close proximity to community hospitals simply transport the most severely mentally ill to the hospitals and clinics for needed services, or alternatively bring medical and mental health staff into the jail to address [incarcerated persons] mental health concerns. (p. 1051)
Building on this point, community-level factors demonstrate how geography and infrastructure shape mental health outcomes in jails. Proximity to medical facilities is crucial for managing crises and preventing suicides, as nearby hospitals enable timely interventions, while delays can increase suicide risk (Guagliardo, 2004). Barry et al. (2023) also found suicide linked to access to nearby health care in a community sample. In jails, access includes partnerships with nearby hospitals for timely mental health assessments and emergency care. Such collaborations are common during medical crises (Chari et al., 2016) and were evident during COVID-19, when local clinicians provided care to incarcerated individuals (Wang et al., 2020). Limited transportation is another barrier; studies show that rural locations, long travel distances, and lack of public transportation make in-person visits to jails largely inaccessible (Sitren et al., 2021; Sturges, 2002), physically isolating people in jail from support networks. This reinforces the study’s premise that greater distances from families and social support reduce visitation due to logistical challenges (Christian, 2005). This is concerning, as the World Health Organization identifies lack of visitation as a key suicide risk factor, with studies linking it to depression (Monahan et al., 2011) and suicide attempts (Liebling, 1993). In another example, the degree of urbanization of a jail’s location is a key factor influencing access to health care and community resources. Urban areas typically have more developed health care systems, social services, and support programs critical for addressing the mental health needs of incarcerated individuals (Helms et al., 2016). In contrast, jails in rural regions often face resource scarcity (Douthit et al., 2015), limiting access to essential mental health services and exacerbating poor outcomes (Ziller et al., 2010). This underpins a geographical element of community infrastructures where more urbanized areas may fare better due to access to health care resources. Finally, research has established a connection between community economic well-being and health outcomes. Weeks et al. (2023) found that localities with greater financial resources often have better community health outcomes, likely due to stronger health care infrastructure. Therefore, jails may similarly reflect fluctuations in community financial health, with greater economic resources leading to improved health services and outcomes in correctional facilities.
Current Study
Although there is some degree of an understanding of individual- and facility-level factors related to jail suicides, the existing literature has notable limitations. First, most past studies have focused on prisons rather than jails (e.g., Smith et al., 2014; Stoliker, 2018), despite the significant disparity in suicide rates between local jails and federal or state prisons, where the rate of jail death is significantly higher. Second, most of the published research on jail suicides in more than last two decades relies heavily on the U.S. Death in Custody Reporting Program (DCRP). While the DCRP remains essential to this research, newer and underused data sets, such as the Reuters Death in Custody data—one of the largest public accounts of U.S. jail deaths (Eisler & Smith, 2021), offer valuable opportunities. Publicly released in late 2020 and covering deaths from 2008 to 2019, the Reuters database remains largely untapped despite providing more recent data coverage; only a few studies (e.g., Adler & Chen, 2023; Eisler & Smith, 2021) have used Reuters data to examine jail suicides. Third, there is a diminishing trend of jail suicide research since the 1980s—the low quantity of research as fatal suicide trends for people in jails increase is concerning. Finally, while previous research has identified individual, facility, and situational correlates associated with jail suicide risks, there remains no research examining jail suicides within a broader, macro-level community context. To address these existing methodological limitations, the current study uses the Reuters death-in-custody data (2011–2019) to answer the following research questions:
The hypotheses, based on theory and prior research, propose that younger, White, male individuals, those incarcerated for shorter periods, or awaiting trial are most at risk of suicide. At the meso-macro levels, overcrowding, maximum-security custody, rural location, distance from hospitals and transit, and limited county resources are expected to increase suicide rates. While predictors of jail suicide—especially individual-level factors—are well established, leveraging newer public data offers a chance to validate past findings and deepen understanding of suicide risk in jail settings.
Method
Data Sources
To examine the individual, facility, and community factors associated with suicide in jails in the United States, multiple sources of data were used. Information on deaths in custody was obtained from Reuters’ death-in-custody database, which is based on official facility records rather than coroner or medical examiner reports. Through Freedom of Information Act (FOIA) requests, Reuters initially sought fatality data from 2008 to 2019 across all 50 states, prioritizing the 10 largest county jails in each state and those with an average daily population (ADP) of at least 750 individuals. However, these criteria were not uniformly applied, as some data were collected from facilities with lower ADPs. In total, Reuters documented 7,571 deaths in custody across 523 jails in 45 states 1 during this period. For the current study, the Reuters dataset was supplemented with publicly available state- and county-level sources to enhance coverage and ensure data completeness across jurisdictions. For example, county-level median income data were obtained from the American Community Survey for 2011 to 2019. County-level urbanicity data were drawn from the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS) for 2013, the latest year available for urban–rural classifications. Distance to hospitals was calculated using hospital location data from the Justice Community Opioid Innovation Network, overlaying it with point locations for each jail, and measuring the distance between the jail and nearest hospital in ArcGIS. Distances from the nearest highway or bus stop were obtained from Google Maps by recording their distance from the jail’s physical address. Data on facility security level and total beds were obtained from official jail websites. Facility- and county-level variables were merged to create a facility-level data set, while the Death in Custody file provided information on decedents’ age, race, length of stay (LOS), and custody status. The final analytic sample comprised 1,738 individuals who died by suicide between 2011 and 2019.
Variables
These two data sets, one at the individual level and the other at the facility level, provided broad information on the decedents’ characteristics as well as information on the facility they were housed in. The merged community-facility data set included facility-level variables (overcrowding, security level, suicide rate) and community-level factors such as median income, distance to the nearest hospital, bus stop, highway, and county urbanicity. Overcrowding was calculated by dividing ADP by total available beds to assess whether the jail was, on average, overcrowded. Jails with mixed security levels were coded by their highest classification (e.g., minimum-medium as medium).
For the individual model, the dependent variable was whether an individual had died from suicide (coded as 0) or another cause (coded as 1). These models included covariates for the participant’s age, race, sex, LOS, and custody status, coded as follows: Age (continuous), Race (0 = White, 1 = Black, 2 = Hispanic, 3 = Other), Sex (0 = male, 1 = female), LOS above/below mean (0 = below, 1 = above), and Custody Status (0 = not convicted, 1 = convicted). To reduce the influence of extreme values and facilitate meaningful interpretation, the continuous LOS variable was dichotomized using the sample median (17 days) as the threshold. This empirically grounded approach classified deaths as occurring during relatively short or long periods of incarceration and provided a standardized basis for comparative analysis.
In the facility-level models, the dependent variable was the suicide rate at each facility, expressed per 100,000 individuals. This rate was calculated by dividing the total number of suicides in a given year by the jail’s ADP for that year. The models contained covariates for the distance to the nearest hospital (in miles), overcrowding status (0 = not overcrowded, 1 = overcrowded), and security level (0 = minimum, 1 = medium, 2 = maximum). Furthermore, the variable of median income was coded as (0 = above national median, 1 = below national median). Median income is used to measure community financial resources, reducing the influence of income extremes and offering a more balanced view of county economic conditions. Additional variables included urbanicity (0 = large central metro, 1 = large fringe metro, 2 = medium metro, 3 = small metro, 4 = micropolitan, 5 = non-core). Finally, distances to the nearest bus stop and highway were coded as categorical variables (0 = under 1 mile, 1 = 1–2 miles, 2 = over 2 miles). Distance to the nearest hospital was coded as a continuous variable (miles) to capture precise variability in health care access, as even small differences may meaningfully impact service utilization and health outcome. 2
Analytical Strategy
The first model, the individual model, utilized a multivariate logistic regression to examine the association between an individual’s death by suicide, their demographic characteristics, their custody status, and the LOS. Given that the death by suicide was a binary variable, the multivariate logistic model was the appropriate choice (Peng & So, 2002). The variables included were drawn from the extant literature related to individual characteristics related to suicides broadly and to suicide in jails specifically. Next, the facility–community-level model utilized a multivariate Poisson regression with standard errors clustered on each facility. The output was expressed in terms of Incident Rate Ratios (IRRs). The Poisson distribution models were appropriate given the positively skewed and equidispersed data. Poisson models are appropriate for modeling count-based, rare events that occur over time. The variables included were drawn from the extant literature surrounding suicide in jails specifically and community characteristics related to suicide broadly. Pre-analytical diagnostics were conducted prior to running all models, and analyses were conducted using STATA 18.
Results
Descriptive Statistics
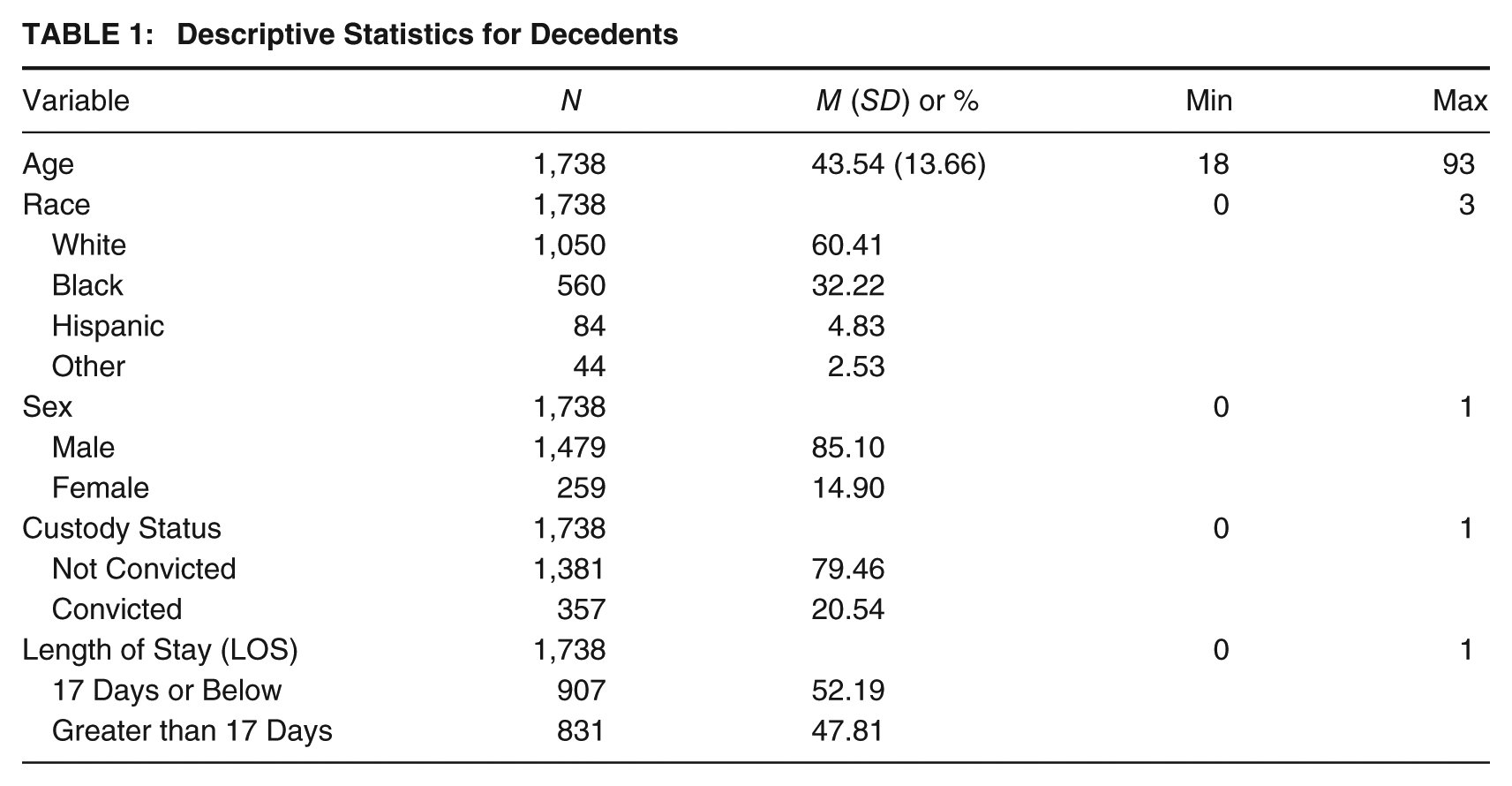
The average age at death was 43.54 years. Most individuals were White (60.41%), followed by Black (32.22%), with Hispanic (4.83%) and Other racial groups (2.53%) comprising smaller proportions. The sample was predominantly male (85.10%), with females representing 14.90%. Most individuals had not been convicted at the time of death (79.46%), while approximately one-fifth had been convicted (20.54%). In terms of LOS before death, over half (52.19%) of the data set died below the median time of all other deaths in the data set (i.e., 17 days), with the remaining sizable minority (47.81%) being in the facility longer than the median LOS before death. Descriptive statistics for the individual-level data set are available in Table 1.
Descriptive Statistics for Decedents
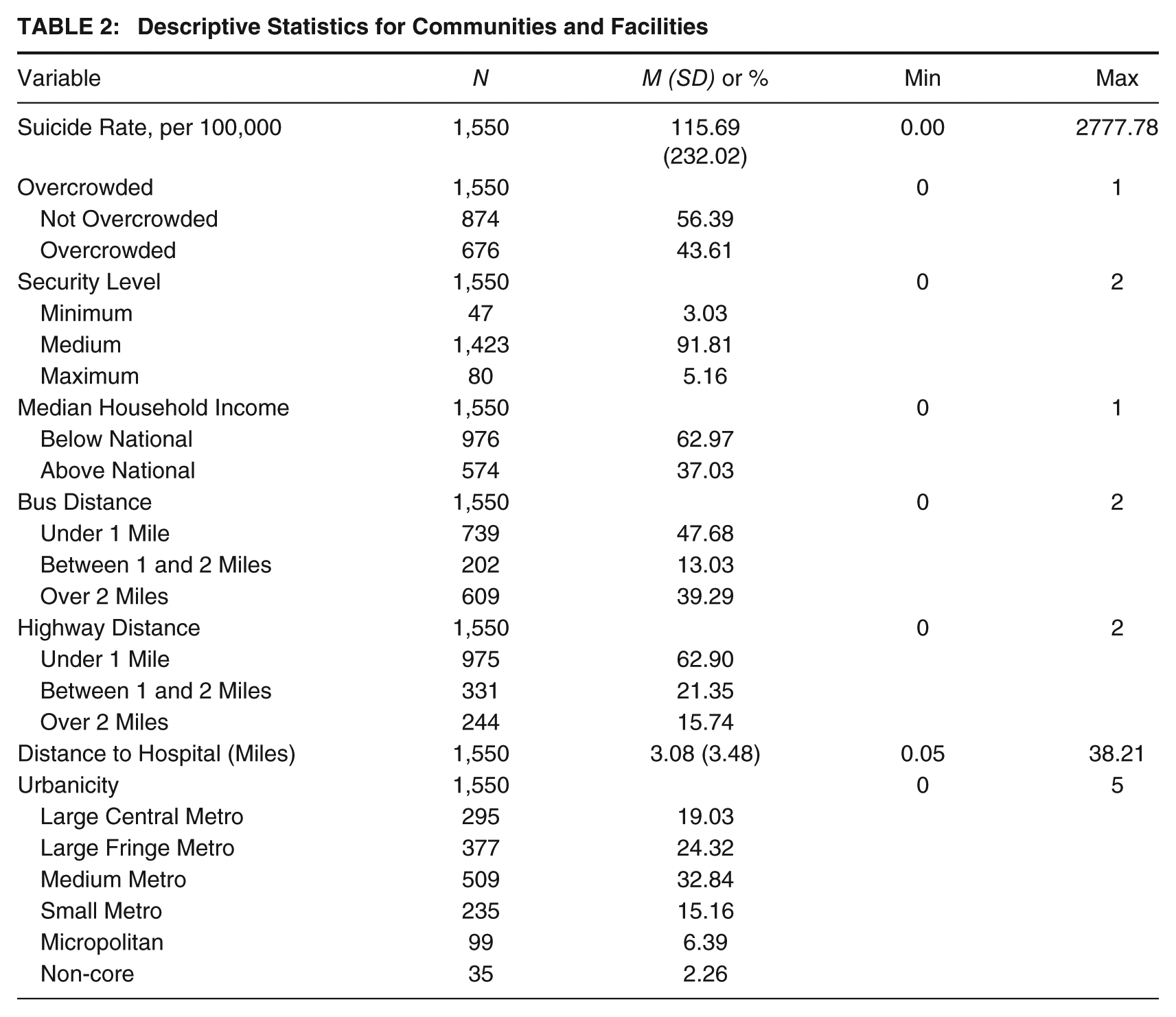
At the facility–community level, the mean suicide rate was 115.69 per 100,000. Overcrowding affected 43.61% of facilities. Most were medium-security (91.81%), with 3.03% classified as minimum-security and 5.16% as maximum-security. A majority of facilities were located in communities below the national median income (62.97%). Nearly half were within 1 mile of a bus stop (47.68%), and most were within 1 mile of a highway (62.9%). The mean distance to the nearest hospital was 3.08 miles, with more than half of facilities situated 2 miles or farther away. Facilities were most commonly located in medium metro counties (32.84%), followed by large fringe metro (24.32%) and large central metro counties (19.03%) (see Table 2).
Descriptive Statistics for Communities and Facilities
Logistic Regression Results
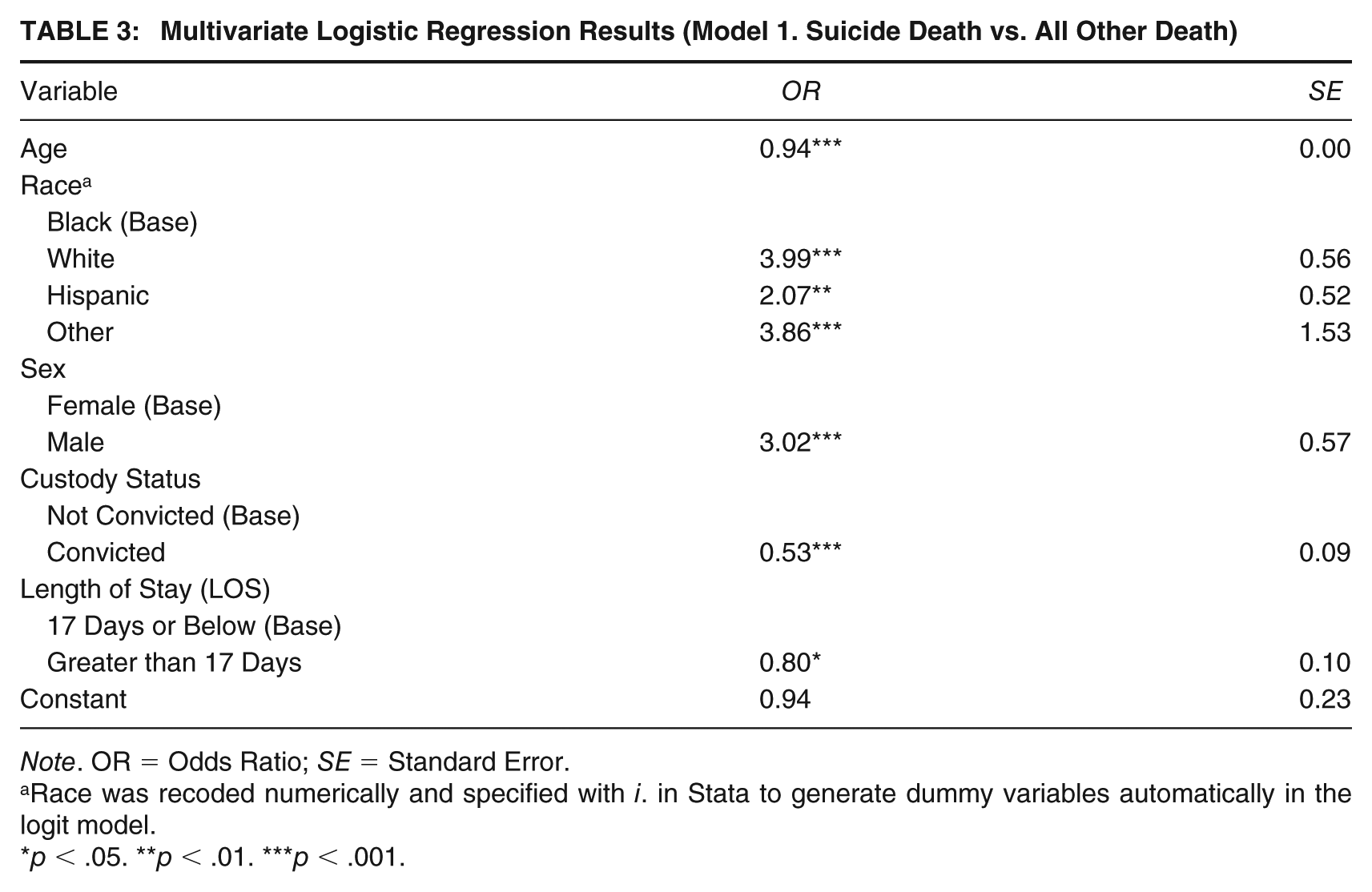
Within the multivariate logistic regression results, age was identified as a significant factor with every year of age of the decedent being associated with a 6% (odds ratio [OR] = .94) less chance of their death being by suicide. Race was also identified as a significant factor with White decedents having nearly four times (OR = 3.99) higher chance of death by suicide, Hispanics having more than twice (OR = 2.07) as high chance of death by suicide, and Other races having a 3.86 (OR = 3.86) greater chance of death by suicide as compared to the Black decedents. Being male was associated with more than three times higher odds of dying by suicide (OR = 3.02) compared to being female. Convicted individuals had a 47% lower likelihood of suicide than those not convicted (OR = 0.53). Finally, those who died in the facility less than the average LOS had a 20% (OR = 0.80) lower chance of death by suicide (see Table 3).
Multivariate Logistic Regression Results (Model 1. Suicide Death vs. All Other Death)
Note. OR = Odds Ratio; SE = Standard Error.
Race was recoded numerically and specified with i. in Stata to generate dummy variables automatically in the logit model.
p < .05. **p < .01. ***p < .001.
Poisson Regression Results
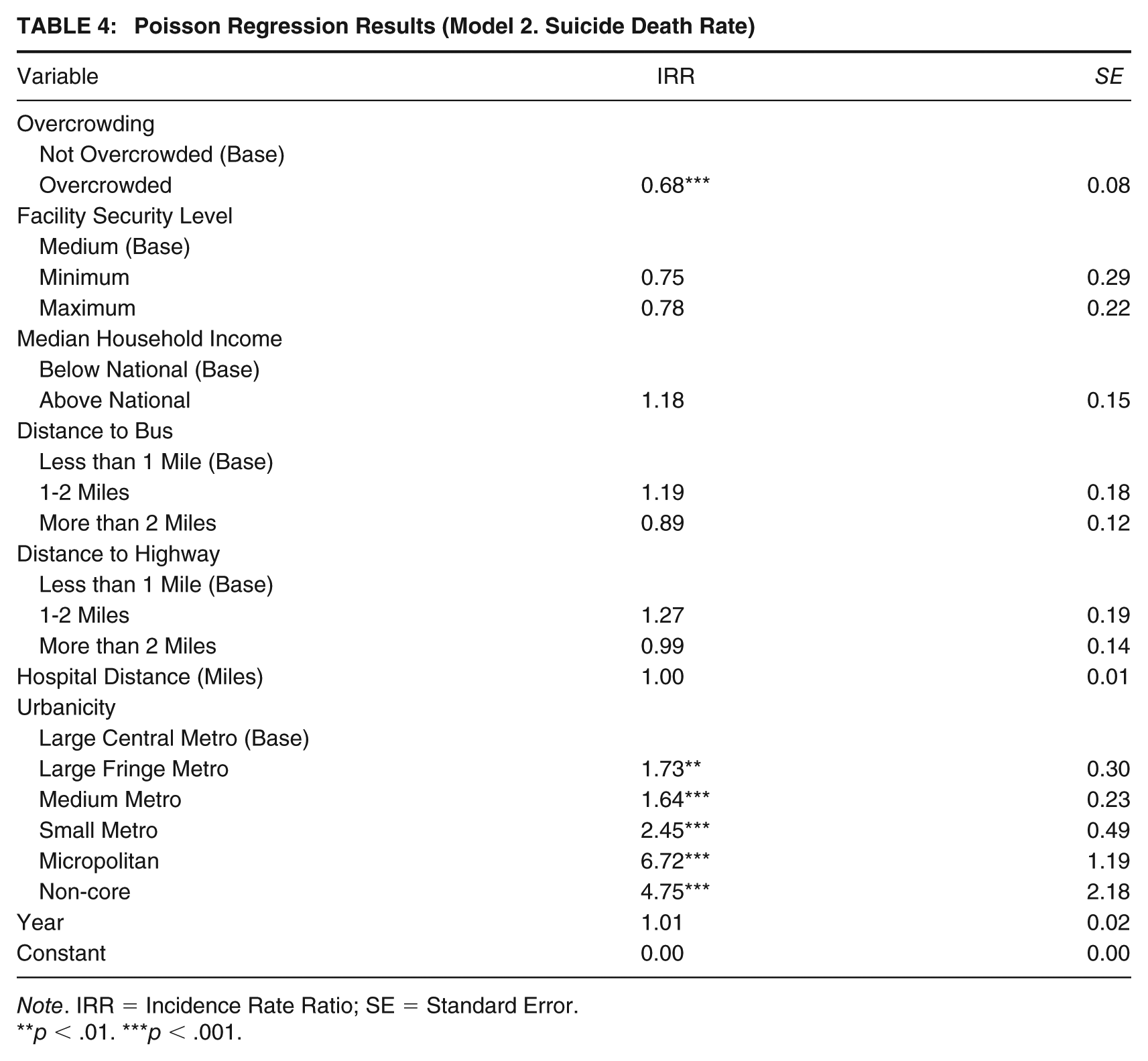
The Poisson Regression results identified several significant relationships. Being in an overcrowded facility resulted in a 32% (IRR = 0.68) lower rate of dying by suicide versus other causes of death. The other significant relationships were found in the urbanicity of the county the facility was located in. All results for urbanicity are compared to a large central metro. Facilities located in large fringe metro counties had a 73% (IRR = 1.73) greater rate of dying by suicide, those located in medium metro counties had a 64% (IRR = 1.64) greater rate, those located in small metros had a 2.45 (IRR = 2.45) times greater rate, those located in micropolitan counties had 6.72 (IRR = 6.72) times higher rate, and those in non-core counties had a 4.75 (IRR = 4.75) greater rate of death by suicide. Full results of the Poisson Regression are in Table 4.
Poisson Regression Results (Model 2. Suicide Death Rate)
Note. IRR = Incidence Rate Ratio; SE = Standard Error.
**p < .01. ***p < .001.
Post Hoc Analyses Results
Based on the initial Poisson regression results, the model was re-run with an interaction between overcrowding and urbanicity to better understand their combined impact. The model identified significant relationships in those facilities that were not overcrowded and in more rural areas. Specifically, the models found that non-overcrowded facilities in micropolitan counties had 4.31 (IRR = 4.31) greater rates of suicide and non-core counties had 17.67 (IRR = 17.67) greater rates of suicide, both compared to non-overcrowded facilities located in large central metros. It should be noted that due to the high standard error, non-core results should be taken with caution. Results from the interaction effects are in Table 5.
Crowding and Urbanicity Interaction Effects (Model 3. Suicide Death Rate)
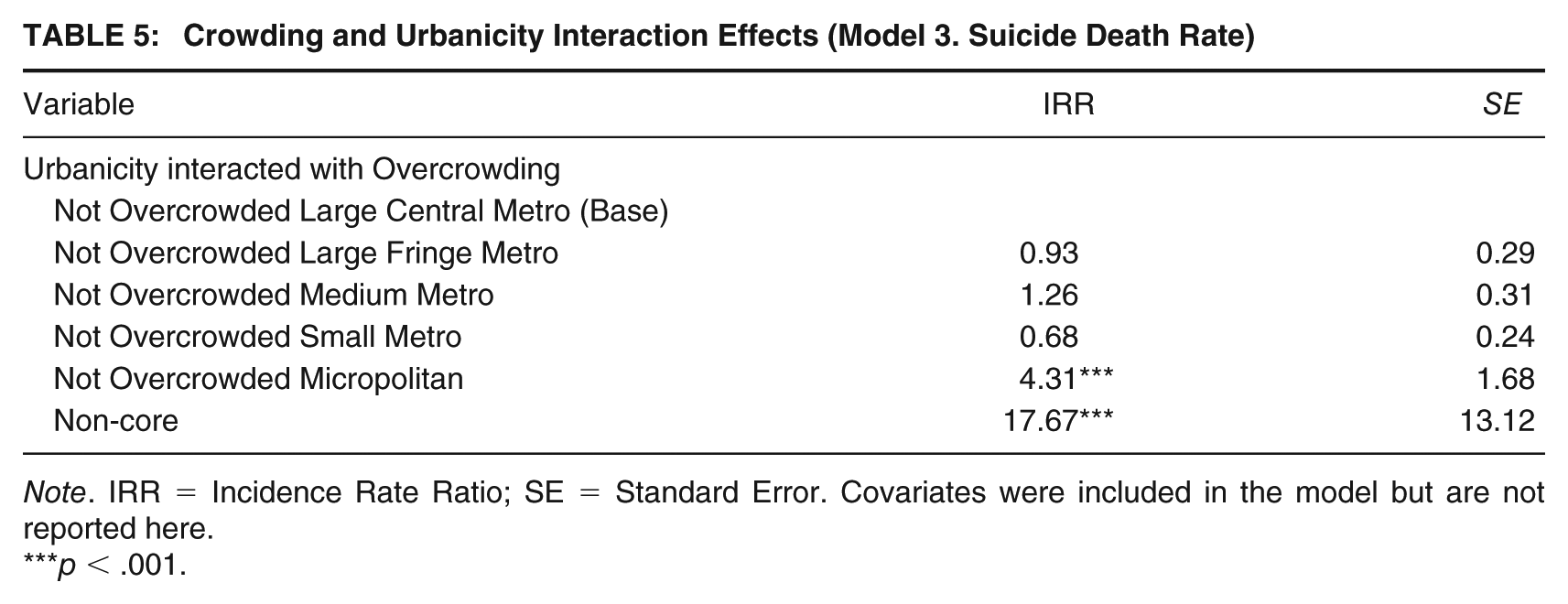
Note. IRR = Incidence Rate Ratio; SE = Standard Error. Covariates were included in the model but are not reported here.
***p < .001.
Discussion
This study provides a comprehensive exploration of the factors contributing to suicide risk within jail environments, highlighting the complex interplay between macro-level (community infrastructure), meso-level (facility conditions), and micro-level (individual characteristics) influences. The findings emphasize that external community resources, internal facility conditions, and individual characteristics all play pivotal roles in shaping the mental health outcomes of incarcerated individuals. These insights support a need for a multifaceted and context-sensitive approach to suicide prevention in U.S. jails.
Individual-Level Influence: Persons in Custody
Although demographic profiles should not be viewed as definitive predictors, they help jail personnel identify individuals at heightened risk of suicide. The findings of this study reaffirm prior literature regarding individual-level demographic factors associated with jail suicides. As well documented in previous research, the current study found that young, unconvicted White males are at the highest risk of committing suicide in jails. These demographics should serve as guidelines to help jail personnel identify individuals at risk of suicidal ideation and attempts, ensuring proper screenings, assessments, and close supervision. Moreover, LOS is linked to recent trends of suicides occurring within 2 months or less in jails. Earlier research found most suicides occurred within the first 24 hours of incarceration (Hayes, 1983, 1989), linked to uncertainty, fear, withdrawal, cultural shock, and limited coping mechanisms (Bronson & Berzofsky, 2017). This study identifies the first 17 days as a high-risk period, highlighting the need for interventions to stabilize acute stress and hopelessness.
Meso-Level Influence: Facility Characteristics
At the meso-level, this study found an inverse relationship between overcrowding and suicide rates. Although typically seen as a contributor to institutional crises, overcrowding may, in some contexts, act as a protective factor against suicide. Similar to Huey and McNulty’s (2005) findings in prisons, overcrowded conditions may reduce suicide opportunities through increased peer supervision. Multi-occupancy cells or dormitories showed lower suicide rates, suggesting a complex link between social density and mental health. Facility size, design, staffing ratios, population diversity, and security levels also impact these dynamics. For example, Villarreal (2015) found higher suicide rates in overcrowded maximum-security facilities, suggesting that less restrictive environments may offer protective benefits. While overcrowded jails pose operational challenges, findings suggest undercrowded jails may face equal or greater suicide risks, potentially due to insufficient programs and medical care. Limited social interaction and rehabilitative opportunities can increase idleness (Kerle, 1998), exacerbating depression and suicide risk over time. Further research is needed on intake processes and treatment services, focusing on how they intersect with varying crowding levels.
Macro-Level Influences: Community Infrastructure and Resources
The macro-level analysis highlights the role of community infrastructure in shaping jail suicide risk, although findings were mixed. Using the RIF, which suggests communities with better health care and social services are better equipped to support incarcerated populations, results only partially confirmed this. Geographical remoteness in rural and less urbanized areas was linked to higher suicide rates, aligning with correctional (Ruddell & Mays, 2007; Tartaro & Ruddell, 2006) and community research (Hirsch & Cukrowicz, 2014; Motillon-Toudic et al., 2022). However, hospital proximity, expected to reduce risk by enabling timely mental health care, showed no significant effect. The null finding for hospital distance likely reflects the complexity of health care access. While it captures physical proximity—what Guagliardo (2004) calls potential access—it overlooks whether the hospital has adequate resources or is meaningfully integrated with the jail, known as realized access.
Proximity to highways and bus stops was not a significant suicide risk factor, suggesting that transportation access, while facilitating visitation, may not reduce isolation or depression enough to impact suicide risk. Although distance from highways was expected to increase isolation and mental health challenges, the data did not support this. One explanation is that suicides in jails occur within 17 days of admission, making transportation access less influential than initial coping struggles and sentencing uncertainty. Furthermore, many detainees come from rural areas with limited transportation, possibly reducing its impact on isolation and mental health.
Similarly, median income did not predict suicide outcomes, likely reflecting its limited ability to capture how taxpayer contributions vary across counties. It also overlooks other funding sources, such as subsidies that support jail operations. Future research should employ more comprehensive financial metrics, including detailed funding allocations and supplementary resources, to better assess links between community financial resources and jail conditions.
Spatial Disadvantage: A Macro-Meso Interaction
This study supports a compounded isolation effect, as shown in the interaction analyses, aligning with research on spatial disadvantages, which suggests that people in more remote, under-resourced areas face compounded adverse outcomes (Lichter & Johnson, 2007; Wiesel et al., 2018). Rural jail populations present a high prevalence of behavioral health conditions, and when combined with non-overcrowded conditions, suicide risk may rise due to limited access to community resources, external support systems, and reduced social interaction within the facility. Such environments may intensify despair, raising an important philosophical question of whether excessively underpopulated facilities could harm mental well-being of individuals. If this holds, it may warrant investigating the impact of capacity thresholds on mental health outcomes. Where feasible, transferring individuals from sparsely populated facilities to those offering more social interaction and stimulation could be considered.
Practical and Policy Implications
The findings highlight practical and policy implications for U.S. jails, particularly in rural areas, where pretrial detention is growing rapidly (Kang-Brown & Subramanian, 2017) and suicide rates are higher. Rural jails operate with smaller budgets, fewer specialized health care providers, and limited access to resources, increasing reliance on medication management or restrictive housing (Ruddell et al., 2021; Tartaro & Ruddell, 2006). Many use generic intake questionnaires with vague mental health items, leading to underdiagnosis of serious needs. Unlike urban facilities, rural jails often lack validated screening tools. Implementing the Brief Mental Health Screen, which trained staff can complete in under three minutes, could improve early identification of at-risk individuals in resource-limited settings (Kohl & Tovar, 2024). Screening should extend beyond intake to address stress and withdrawal, with multiple assessments during the first 17 days and ideally 30 days. Substance use and mental health treatment reduce suicide risk. Interventions like Dialectical Behavioral Therapy, Cognitive Behavioral Therapy, and Cognitive Therapy for Suicidal Patients target cognitive and behavioral factors linked to suicidality (González-Prendes & Resko, 2012). Policymakers should strengthen jail health care and suicide prevention, especially in rural areas, by incentivizing providers through tax breaks, grants, or loan forgiveness to expand services and partner with jails.
Another key strategy to address health care gaps in jails is leveraging telehealth and technological innovations. Remote solutions (e.g., telemedicine, videoconference technology) mitigate workforce shortages, reduce reliance on corrections staff, and deliver cost-effective care in resource-limited facilities, with outcomes comparable to in-person services (Batastini et al., 2020; Rosen et al., 2024). Telehealth also ensures continuity of care post-release through medication management, follow-ups, and Medicaid re-enrollment. Recent Centers for Medicare and Medicaid Services policy changes allow states to apply for 1115 Waivers, permitting Medicaid funds for care up to 90 days pre-release (Buck et al., 2024)—a critical step toward lifting the Medicaid/Medicare ban in jails (Olson et al., 2020) and improving reentry outcomes.
Moreover, administrators can develop and implement comprehensive policies, staff training, and environmental controls within jails to minimize opportunities for self-harm. All staff, not just mental health professionals, should be equipped to recognize suicidal ideation and intervene effectively. Training in suicide prevention and detox protocols, combined with high-visibility housing, helps mitigate risks through early detection. Fostering positive social dynamics also aids prevention efforts. For example, New York City jails employ Suicide Prevention Aides for peer support and additional observation, a practice adopted by some U.S. prisons (Tartaro & Klenk, 2023). Such roles detect early signs of suicidal ideation and leverage peer relationships to enhance collective responsibility and mental health awareness.
Arguably, minimizing unnecessary pretrial detention is the most proactive way to reduce suicide risk. Bail reform and front-end diversion initiatives, such as Crisis Intervention Training, mobile crisis outreach, and specialized courts, can redirect individuals in mental health crises from jails, easing overcrowding and lowering associated risks. While aforementioned initiatives can be promising, a “one-size-fits-all” approach is unlikely to succeed. Jails vary in size, funding, and local resources, requiring tailored interventions. Whether through enhanced screening, telehealth, or community alternatives, progress depends on funding. Political advocacy, media attention, and innovative financing are crucial for resource-limited rural jails to implement evidence-based solutions that improve mental health and reduce suicide risk.
Limitations and Future Research
Key limitations to this study are acknowledged. First, the sample was restricted to cases of deaths in custody, preventing a holistic view of suicidality in jail settings and excluding the possibility of establishing a comparison group. Future studies should consider using data that also reflects persons who did not die while incarcerated, as well as broadened outcomes like attempted versus completed suicides. Second, due to the quantitative nature of this study, it cannot explain the underlying reasons behind the relationships observed. To better understand how meso- and macro-level factors contribute to suicidality, more in-depth qualitative analysis may be beneficial, as everyone’s emotional and cognitive experiences are shaped by unique circumstances, such as mood disorders, life histories, and interpersonal dynamics, which are often difficult to quantify or observe. The measures of community infrastructure could be expanded. Hospital concentration within a spatial boundary may better capture health care access than proximity alone (Deng & Bennett, 2023). While proximity indicates potential access, it does not reflect a hospital’s capacity for mental health care or its integration with jails. Assessing hospital-jail collaboration and available resources would offer deeper insight. Third, another limitation is the exclusion of specific variables related to jail suicides that may improve the predictive accuracy of the analyses. Key factors, such as facility operations and management policies (e.g., use of solitary confinement, programming availability, visitation policies, screening and assessment processes), as well as personnel information (e.g., staffing ratios, diversity, and training), were not included. The inclusion of these factors could provide a more comprehensive understanding of the correlates of jail suicides and how these factors interact. Finally, given the exploratory nature of the present findings and the acknowledged data limitations, direct policy prescriptions are not warranted at this stage. However, the results highlight an urgent need for stronger legislative and policy frameworks to improve the collection, reporting, and accessibility of data on suicides, suicidal ideation, and related mortality in correctional systems. Expanding national-level data access—whether through statutory requirements, standardized reporting protocols, or interagency coordination—would enable systematic integration of administrative records, qualitative accounts, and longitudinal datasets. Such infrastructure is essential to capture the full spectrum of suicidal behaviors, from ideation and attempts to completed suicides, as well as deaths occurring after community reentry. These advancements will provide the empirical foundation needed to develop targeted, evidence-based prevention strategies in correctional settings and beyond.
Footnotes
Authors’ Note:
There are no conflicts of interest to declare. The authors gratefully acknowledge the invaluable contributions of the project team members who supported this study: Katharine McGrath, Noa Glover, Joanna Haydon, Elizabeth Cairns-Callen, Julia Sheehan, Josh Sugino, and Elijah Woodberry. The authors also extend their appreciation to the Editorial Board of Criminal Justice and Behavior and the anonymous reviewers for their thoughtful and constructive feedback throughout the review process.