
Abstract
Intimate partner violence (IPV) is a major public health issue with long-lasting consequences, necessitating effective treatments to disrupt its intergenerational transmission. However, the common one-size-fits-all approach in IPV programs may fail to acknowledge the diversity among perpetrators. This study compared three types of IPV perpetrators entering treatment: self-referred, legally mandated, and formally pressured. Among 1,302 men surveyed, self-referred men were generally older, more educated, and reported more clinical symptoms than those in the other groups. They appeared more ready to change and less influenced by social desirability biases. Legally mandated men reported fewer minor IPV behaviors, but more severe behaviors compared with self-referred men. They seemed to minimize or deny their behavior, failing to acknowledge their problem with violence. Formally pressured men exhibited mixed characteristics. They appeared to be motivated by the fear of losing custody of their children. These findings underscore the need for tailored therapeutic approaches.
Intimate partner violence (IPV) is a major public health issue in Canada and globally (Cotter, 2021; World Health Organization, 2021). In Canada, about 44% of women and 36% of men who have been in a relationship report having experienced at least one form of IPV in their lifetime (Cotter, 2021). In addition to its high prevalence, literature reviews have linked physical and psychological IPV to numerous repercussions for victims, such as chronic pain, depression, posttraumatic stress disorder, substance abuse, and suicidal ideation (e.g., Dokkedahl et al., 2022; Lawrence et al., 2012). Violence is more often perpetrated by men than by women and often results in the most severe consequences for women, sometimes even leading to fatalities (World Health Organization, 2021), justifying a focus on men perpetrators. Beyond its immediate consequences, IPV is entrenched within a perpetual intergenerational cycle (Cotter, 2021), emphasizing the critical need for effective treatments to disrupt this pattern. Given its complexity and multifaceted nature, IPV is characterized by a diverse and heterogeneous group of perpetrators (Brassard et al., 2023).
A survey of 238 IPV programs across Canada and the United States by Cannon et al. (2016) found that most programs employed a one-size-fits-all therapeutic approach, despite concerns that this could reduce their effectiveness due to the diverse profiles, sources of referral, and motivations behind violent behavior. A deeper understanding of individuals entering IPV services could lead to more customized services, potentially enhancing treatment effectiveness (Stare & Fernando, 2014). The present study’s aim was thus to compare three types of IPV perpetrators entering IPV treatment based on their referral type: self-referred, legally mandated, and formally pressured. Examining diverse sociodemographic and clinical differences among these groups prior to treatment could enhance the understanding of individual profiles and promote the development of tailored interventions that could address specific needs more effectively (Butters et al., 2021).
Referral Types and IPV
Most research on IPV programs has primarily focused on legally mandated men populations (Tutty et al., 2020). A U.S. survey found that most individuals entering treatment for IPV (89.0%) were legally mandated to do so (Price & Rosenbaum, 2009). However, the situation in Canada is different. In a Canadian study by Brassard et al. (2023) involving 980 men entering treatment for IPV, only 63.6% had undergone a judicial process (related to IPV or other issues), a process with the Youth Protection, and/or had a restraining order preventing them from contacting their (ex-) partner. Another Canadian study specified that among 349 participants entering treatment for IPV-related issues, less than a third (31.8%) attended treatment under a court order (Desbiens et al., 2025). This variability underscores that men entering treatment can differ based on their referral type and the legal context of their country (Tutty et al., 2020).
Unlike other forms of treatments, IPV-related interventions are not always initiated voluntarily, leading to debates about their outcomes (Hachtel et al., 2019). A meta-analysis has shown a reduction in the risk of recidivism after treatment (Karakurt et al., 2019), whereas others indicated little to no IPV reduction (Arias et al., 2013; Babcock et al., 2024). Parhar et al. (2008) found in their meta-analysis that voluntary treatment significantly reduced recidivism, whereas the effectiveness of mandated treatment varied depending on the context. Given the severe consequences of IPV, enhancing the effectiveness of treatments is crucial. Many researchers argue that a one-size-fits-all approach fails to address the diverse needs of individuals entering IPV treatment (Arias et al., 2013; Butters et al., 2021; Cannon et al., 2016; Scott et al., 2017). A U.S. survey found that while most states (75%) conduct an intake evaluation to assess the specific needs of individuals entering IPV treatment, the majority (91%) enforce a standardized treatment approach for all perpetrators (Maiuro & Eberle, 2008). Tailoring treatment to the specific IPV dynamic and to the skills required by perpetrators is essential (Cannon et al., 2016). Mismatches between an individual’s profile and treatment could undermine the therapeutic alliance (Cannon et al., 2016) and contribute to treatment dropout (Brown et al., 1997). Dixon and Browne (2003) emphasized that differences between self-referred and legally mandated individuals need to be considered. The type of referral could serve as a key variable in understanding a person’s needs and providing tailored treatment to better meet those needs.
Yet, in their literature review, Snyder and Anderson (2009) criticized the binary classification of individuals as either legally mandated or voluntary. They argued that there is a continuum of pressure to initiate IPV treatment, and using more than two categories would provide a more realistic portrayal and greater statistical sensitivity. Recently, Seto et al. (2022) highlighted the challenges in determining the level of voluntariness. A participant who seems voluntary might be under external pressure (e.g., from their partner), whereas a legally mandated participant might genuinely choose to engage in treatment. Hence, in their study on anger treatment, Seto et al. (2022) introduced a third intermediate category: the formally pressured referral, where someone is not legally mandated but is pressured to seek treatment by others (e.g., by Youth Protection or due to the fear of losing custody of their children).
Comparisons According to Referral Types
A few studies have compared the characteristics of self-referred and legally mandated IPV perpetrators (Dutton & Starzomski, 1994; Tutty et al., 2020) and individuals with dysfunctional anger (Seto et al., 2022). In a study involving 78 men, Dutton and Starzomski (1994) found no significant sociodemographic differences (e.g., age, education, alcohol consumption) between self-referred (51.3%) and legally mandated (48.7%) men entering treatment. However, the small sample size may have limited the detection of smaller effects. After controlling for social desirability, Dutton and Starzomski (1994) found that self-referred men reported higher perpetrated psychological IPV, and higher levels of depression, anxiety, affect dysregulation, and identity diffusion. Although both groups exhibited high levels of personality disorders, self-referred men scored higher on avoidant personality scales, but did not differ on dependent, narcissistic, and antisocial personality scales.
In a larger study including 964 men, Tutty et al. (2020) found significant sociodemographic and clinical differences between self-referred (21.3%) and legally mandated (78.7%) men entering treatment. Self-referred men were older, had higher education levels, were more likely to live with a partner, had more suicidal thoughts, and reported more childhood interpersonal trauma than legally mandated men. Moreover, self-referred men reported higher levels of physical and psychological IPV, depression, anxiety, affect dysregulation, and self-esteem issues. However, the authors did not discuss these differences, as it was not their primary objective.
Seto et al. (2022) compared 405 individuals entering treatment for anger issues using a third category (i.e., formally pressured). They found that voluntary (self-referred) individuals (61.0%) were generally older and had higher levels of education compared with those who were legally mandated (24.7%). Legally mandated individuals were more likely to have a substance use diagnosis than self-referred. In addition, self-referred individuals scored higher on measures of depression, anxiety, and affect dysregulation. Formally pressured individuals (14.3%) did not significantly differ from the legally mandated and self-referred groups on these characteristics, with their scores falling in between. The small percentage of formally pressured individuals could explain the lack of statistical differences.
In sum, across the studies comparing individuals based on their referral type, several key differences emerged. Self-referred individuals tended to be older, had higher levels of education, reported higher occurrences of perpetrated psychological IPV, experienced higher levels of psychological distress (i.e., depression and anxiety), and exhibited more affect dysregulation. Dutton and Starzomski (1994) hypothesized that these differences might have been found because self-referred men are more concerned with intimacy issues (e.g., desire to preserve their couple relationship), whereas legally mandated men face conflicts over a range of issues. They also suggested that legally mandated men tend to direct their anger toward their partners and the court system, whereas self-referred men tend to direct their anger toward themselves, resulting in greater psychological distress. Seto et al. (2022) further noted that this distress and impairment might have motivated self-referred clients to seek help. Further research with a more balanced distribution among the three referral groups is needed to deepen the understanding of their specific characteristics and offer potential clinical implications.
The Present Study
The study was designed to expand past research, while countering some of the noted limitations. First, it utilized a large clinical sample of men entering IPV treatment in several community organizations, ensuring sufficient statistical power. Second, by including three distinct referral types–self-referred, legally mandated, and formally pressured–the study enabled a comprehensive analysis of how referral type may distinguish perpetrators’ sociodemographic and clinical characteristics. In this study, the formally pressured category included men who were not legally mandated but had been involved in a judicial process related to IPV or family violence, or a process with the Youth Protection, who were referred by these systems, or had a restraining order issued against them by their (ex-) partner. The self-referred category consisted of participants who voluntarily sought treatment without formal external pressure. The use of a Canadian sample ensured more similarly sized groups, allowing for more balanced comparisons and enhanced generalization of the findings. Third, an innovative aspect of this study was its approach to evaluating physical, psychological, and sexual IPV based on severity rather than the mere occurrence of IPV behaviors. As suggested by Brassard et al. (2023), considering the severity of IPV behaviors can help distinguish profiles of perpetrators and provide a deeper understanding of IPV dynamics. Finally, the study allowed the exploration of clinically relevant variables that have not yet been investigated with regards to referral types, such as attachment insecurities and undesirable personality traits.
Objectives and Hypotheses
The main objective of this study was to identify sociodemographic and clinical differences among perpetrators based on their referral type (self-referred, legally mandated, and formally pressured). Due to the lack of empirical support, we formulated three research question.
Research Question 1: (Q1) Where do the formally pressured individuals stand compared with self-referred and legally mandated individuals in terms of age and education, and do other sociodemographic variables differentiate perpetrators based on their referral type?
Research Question 2: (Q2) Does the nature and severity of the perpetrated IPV differentiate perpetrators according to their referral type?
Research Question 3: (Q3) Where do the formally pressured individuals stand in terms of depression, anxiety, and affect dysregulation in relation to the other two groups, and do other clinical variables (i.e., anger, cognitive symptoms, identity diffusion, attachment insecurities, undesirable personality traits) differentiate perpetrators based on their referral type?
Building on the reviewed literature, we formulated two hypotheses.
Hypothesis 1 (H1): We expected that self-referred individuals would be older and have higher levels of education compared with those who are legally mandated (H1).
Hypothesis 2 (H2): We expected that self-referred individuals would report higher levels of depression, anxiety, and affect dysregulation compared with those who are legally mandated (H2).
Method
Procedure
This study was conducted as part of an ongoing collaborative research program involving 22 government-funded community organizations offering treatment for IPV across various region of a Canadian province, encompassing both rural and urban areas. When entering the organization, each user was required to complete a series of online questionnaires (approximately 35 min) using an electronic tablet or a computer, or by being verbally accompanied by a therapist as part of the admission and orientation phase. Data were collected on the secure Qualtrics platform, ensuring rigorous data security standards. The research team analyzed the questionnaires and sent a summary of the interpreted results back to the organizations to help identify each user’s treatment needs. The treatment provided to IPV perpetrators was grounded in various theoretical approaches, all adhering to national guidelines emphasizing cognitive-behavioral principles aimed at fostering accountability for one’s actions and addressing problematic thoughts and behaviors (Roy et al., 2024). Depending on the organization, treatment was delivered through individual sessions, group sessions, or a hybrid format, with the groups including users from various referral types. Services were provided in French, with the option for users to request a translator if they had limited proficiency in the language. Users were introduced to the research project, read the consent form, and were free to either consent to or decline the use of their data for research purposes without affecting the services they received. Only users who agreed to the use of their data were considered study participants. No compensation was provided for participation. Each participant was identified by a code chosen by the organization to ensure their anonymity with the research team. This study received approval from the researchers’ university ethics board.
Participants
Among the 1,501 men who entered the organizations between June and November 2023, 1,321 agreed to take part in the research (88% participation rate), and 1,306 met the inclusion criteria (i.e., identified as men and were aged 18 years or older). Among these, four men were excluded because they could not be classified into any of the referral categories. Thus, the final sample consisted of 1,302 adult men, aged between 18 and 80 years old (M = 38.46, SD = 11.43), who agreed to take part in the study.
Table 1 and Table 2 display the sociodemographic characteristics of the overall sample and in the three referral groups. Most of them reported being assigned as men at birth (99.8%), with the remainder (0.2%) not responding to the question. The participants’ first language was French (91.2%), English (4.8%), Spanish (1.4%), or another language (2.6%, e. g., Arabic, Portuguese). Only 7.7% of the participants were born outside of Canada (e. g., France, Republic of Congo). Most participants were employed either part-time or full-time, whereas others were retired (3.4%), studying part-time or full-time (2.5%), or had another occupation status such as being currently unemployed or on medical leave (28.3%). The majority reported being in a relationship, while others were single (32.5%, including those separated or divorced), in the process of a breakup (13.0%), or had a different marital status (1.6%, e.g., sexual partner only).
Sociodemographic Characteristics of the Overall Sample and Their Distribution by Referral Type (Categorical Variables)

p < .05. **p < .01. ***p < .001.
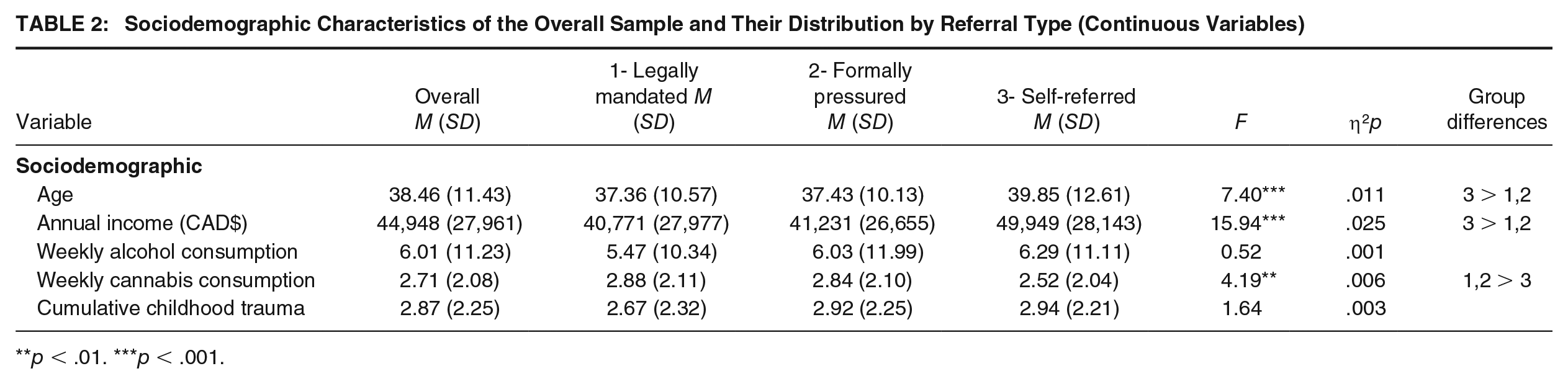
Sociodemographic Characteristics of the Overall Sample and Their Distribution by Referral Type (Continuous Variables)
p < .01. ***p < .001.
Table 3 presents criminal justice involvement of the overall sample and within the three referral groups. Less than a quarter of the participants (n = 310, 23.8%) were classified as legally mandated due to court orders. Close to a third (n = 426, 32.7%) fell into the formally pressured category. The remaining participants (n = 566, 43.5%) were categorized as self-referred, including those who experienced some form of informal pressure (e.g., from a partner). Although all the legally mandated men indicated being court-ordered to treatment, the majority were under conditional release (36%), supervised probation (21%), or parole (9%). The remaining did not specify their correctional status (22%) or reported other statuses (12%), with only 5% indicating that they were awaiting trial. Legally mandated men reported receiving referrals from judicial system (72.3%), health care and social services network (13.2%), Youth Protection (10.6%), close ones (4.5%, e. g., partner, friend), and other sources (8.7%, e.g., community organizations, internet; total is higher than 100% as men could select multiple sources). Formally pressured men reported referrals from Youth Protection (31.0%), judicial system (including lawyers, 28.9%), health care and social services network (26.1%), close ones (15.5%), and other sources (14.3%). Self-referred men reported referrals from health care and social services network (45.8%), close ones (30.6%), and other sources (29.7%). Across all categories, most participants (79.9%) were consulting a specialized IPV organization for the first time.
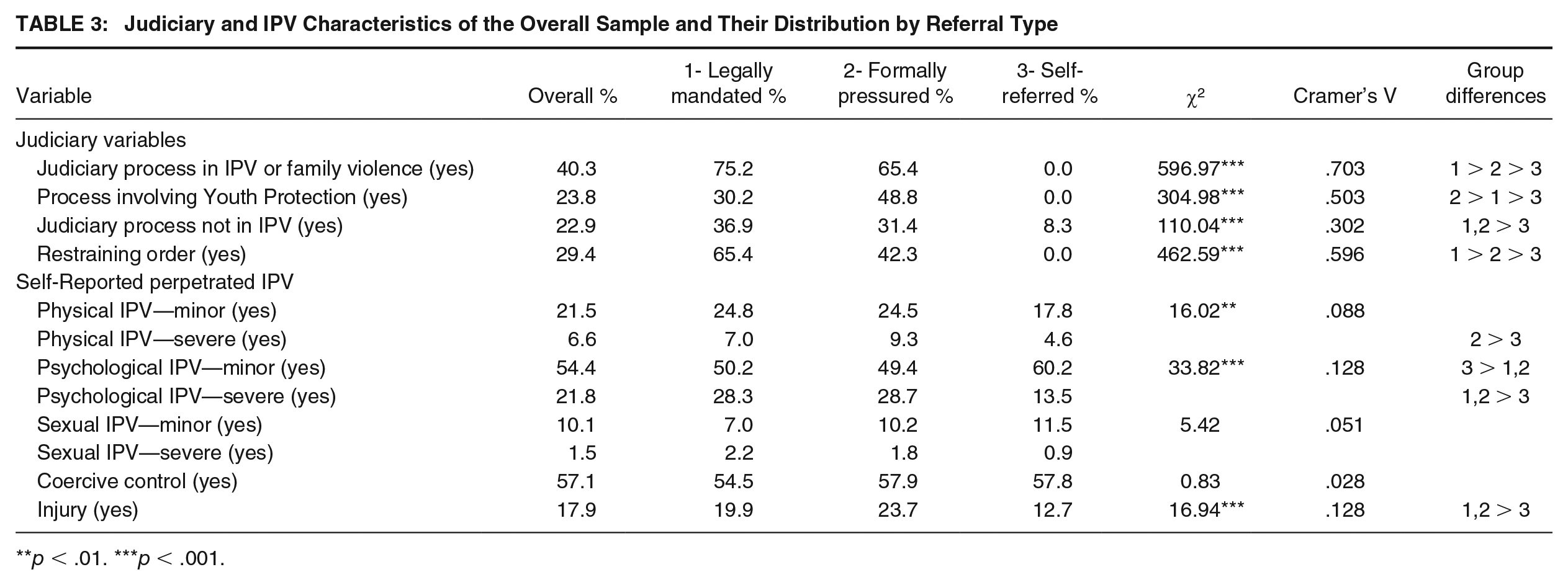
Judiciary and IPV Characteristics of the Overall Sample and Their Distribution by Referral Type
p < .01. ***p < .001.
Measures
A sociodemographic questionnaire was used to collect personal information and criminal justice involvement of the participants (e.g., age, education, substance use, sources of referral). Participants were also asked about their mental health diagnoses and assessed for risks, including suicidal and homicidal tendencies, as well as access to firearms. In addition, measures of childhood interpersonal trauma, IPV, and clinical factors were chosen based on their adequate psychometric properties, brevity, and availability in French, English, and Spanish.
Childhood Interpersonal Trauma
The 12-item short version of the Childhood Cumulative Trauma Questionnaire (CCTQ; Bigras et al., 2017) was used to assess eight types of interpersonal trauma experienced before the age of 18 (physical, psychological, and sexual abuse; physical and psychological neglect; witnessing physical and psychological violence between parents, bullying). Each type of trauma was dichotomized (0 = absence, 1 = presence) and summed to create a cumulative trauma score, ranging from 0 to 8, with higher scores indicating greater exposure to various forms of interpersonal trauma. In the present study, the internal consistency of the interpersonal trauma items was adequate (α = .84, ω = .85).
Intimate Partner Violence
The 20-item short version of the Revised Conflict Tactics Scales (CTS2S; Straus & Douglas, 2004) was used to assess the frequency of perpetrated physical (e.g., I pushed, shoved, or slapped my partner; 2 items), psychological (e.g., I destroyed something belonging to my partner or threatened to hit my partner; 2 items), and sexual (e.g., I used force [like hitting, holding down, or using a weapon] to make my partner have sex; 2 items) IPV, as well as the frequency of perpetrated injury (e.g., My partner had a sprain, bruise, or small cut or felt pain the next day because of a fight with me; 2 items) in the past 12 months. Responses were measured on a 7-point scale, ranging from 0 (this never happened) to 6 (more than 20 times in the past year). For physical, psychological, and sexual IPV, items were categorized based on whether the IPV was minor (e.g., I insulted or swore or shouted or yelled at my partner) or severe (e.g., I punched or kicked or beat-up my partner), and a 3-level severity score was derived for each form of violence following Straus and Douglas’s (2004) recommendations: 0 = no violence, 1 = minor violence only, and 2 = severe violence. Higher scores indicate a greater severity of perpetrated IPV. In the present study, the internal consistency of the eight IPV items was adequate (α = .72, ω = .75).
In addition, a 4-item version of the Coercive Control Scale (CCS; Johnson et al., 2014) was used to assess the coercive control (e.g., I insisted on knowing who my partner was with at all times) perpetrated in the past 12 months. Responses were measured on a 7-point scale, ranging from 0 (this never happened) to 6 (more than 20 times in the past year), higher scores indicating a greater frequency of perpetrated IPV. In the present study, the internal consistency of the four coercive control items was passable (α = .59, ω = .61), which may be due to some men only using specific controlling behaviors, such as isolating their partner, controlling the finances, or surveillance.
Psychological Distress
The 14-item short version of the Psychiatric Symptom Index (PSI; Ilfeld, 1976) was used to assess psychological distress symptoms, including four subscales: depression (e.g., Did you feel downhearted or blue?; 5 items), anxiety (e.g., Did you feel fearful or afraid?; 3 items), anger (e.g., Did you feel easily annoyed or irritated?; 4 items), and cognitive (e.g., Did you have trouble remembering things?; 2 items). Responses were measured on a 4-point scale, ranging from 1 (not at all) to 4 (very often). Relevant items were summed to create individual subscale scores, then rescaled to have a standardized 0–100 range, with higher scores indicating higher symptoms. In the present study, the internal consistency for depression (α = .86, ω = .86), anxiety (α = .82, ω = .82), anger (α = .87, ω = .88), and cognitive symptoms (α = .83) was adequate.
Affect Dysregulation and Identity Diffusion
Two 9-item subscales of the Inventory of Altered Self-Capacities (IASC; Briere, 2000) were used to assess affect dysregulation (e.g., Not being able to control your anger) and identity diffusion (e.g., Feel like you don’t know yourself very well) in the last 6 months. Responses were measured on a 5-point scale, ranging from 1 (never) to 5 (very often). Items were summed to create a global score, higher scores indicating higher affect dysregulation or identity diffusion. In the present study, the internal consistency coefficients of affect dysregulation items (α = .92, ω = .92) and of identity diffusion items (α = .91, ω = .91) were adequate.
Attachment Insecurities
The 12-item short version of the Experiences in Close Relationships (ECR-12; Lafontaine et al., 2016) was used to assess attachment insecurity dimensions, including attachment anxiety (e.g., I worry about being abandoned; 6 items) and attachment avoidance (e.g., I don’t feel comfortable opening up to romantic partners; 6 items). Responses were measured on a 7-point scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Each dimension’s score was calculated by averaging its respective items, with higher scores indicating greater attachment insecurities. In the present study, the internal consistency coefficients for attachment anxiety (α = .90, ω = .91) and attachment avoidance (α = .83, ω = .84) were adequate.
Undesirable Personality Traits
The 12-item version of the Dark Triad Dirty Dozen (DD; Jonason & Webster, 2010; Savard et al., 2017) was used to assess undesirable personality traits, including three subscales: Machiavellianism (e.g., I tend to manipulate others to get my way; 4 items), narcissism (e.g., I tend to seek prestige or status; 4 items), and psychopathy (e.g., I tend to be callous or insensitive; 4 items). Responses were measured on a 9-point scale, ranging from 1 (strongly disagree) to 9 (strongly agree). The score for each subscale corresponds to the average of its respective items, with higher scores indicating a greater presence of undesirable personality traits. In the present study, the internal consistency for Machiavellianism (α = .87; ω = .88), narcissistic (α = .86; ω = .87), and psychopathic traits (α = .75; ω = .75) was adequate.
Data Analysis Strategy
Statistical analyses were performed using the SPSS statistical package, Version 29. Chi-square analyses and multivariate analyses of variance (MANOVA) were used to compare the three referral types on the sociodemographic and clinical measures. For significant MANOVA, univariate ANOVAs and post hoc comparisons were conducted using the Games–Howell test to account for unequal variances and sample sizes.
Results
Table 1 displays sociodemographic characteristics by referral type, whereas Table 2 presents the sociodemographic continuous variables differences among the three referral groups. Self-referred men tended to be older, had higher education levels, higher incomes, and were more likely to report having received a mental health diagnosis (e.g., depression) compared with those who were legally mandated or formally pressured. Compared to the legally mandated group, self-referred men were more likely to be born in Canada. Both self-referred and formally pressured men were more likely to be in a relationship compared with those who were legally mandated. Formally pressured men were more likely to have at least one child than those in the other two referral groups. The variances explained for age (1.1%), education (3.8%), income (2.5%) mental health diagnosis (1.0%), being born in Canada (0.6%), being in a relationship (1.7%), and having at least one child (2.7%) were relatively small. No significant differences were found based on Indigenous status, sexual orientation, employment status, having a partner in a shelter, or cumulative childhood trauma.
In terms of substance use, legally mandated men reported higher stimulant use (e.g., cocaine) in the past 6 months compared with self-referred men. Both legally mandated and formally pressured men reported higher weekly cannabis consumption than self-referred men. Formally pressured men also reported being told by close ones that they had a substance use problem more frequently than legally mandated men. The variances explained for stimulant use (1.3%), weekly cannabis consumption (0.6%), and problematic substance use according to close ones (2.0%) were relatively small. No significant differences were found for the use of depressants (e.g., opiates) and hallucinogens (e.g., LSD) in the past 6 months, or for weekly alcohol consumption. Regarding risk assessment, self-referred men reported more suicidal thoughts than the formally pressured men, who in turn reported more suicidal thoughts than the legally mandated individuals. However, there were no significant differences between the three groups in terms of suicide attempts and homicidal thoughts. Nonetheless, the legally mandated group reported more threats or attempts at homicide than the self-referred group. In addition, men in the self-referred group reported greater access to firearms compared with the other two groups. The variances explained for suicide thoughts (2.2%), homicide threats or attempt (0.7%) and firearm access (2.5%) were relatively small.
Table 3 displays judicial and IPV severity differences among the three referral groups. Legally mandated men were more likely to be involved in judicial processes related to IPV or family violence and to have received a restraining order compared with the formally pressured and self-referred groups. Formally pressured men were more likely than both legally mandated and self-referred men to be involved in a process related to Youth Protection. No self-referred men were involved in judicial processes related to IPV or family violence, a process with the Youth Protection, or received a restraining order, as these were exclusion criteria for this group. Both legally mandated and formally pressured men were more likely to be involved in judicial processes unrelated to IPV compared with the self-referred group. The variances explained for judiciary process in IPV or family violence (49.4%), process involving Youth Protection (25.3%), and no-contact order (35.5%) were high. The variance explained by judiciary process not in IPV was moderate (9.1%).
In terms of perpetrated IPV, formally pressured men reported more severe physical IPV than self-referred men (see Table 3). Self-referred men reported more minor psychological IPV than the two other groups, but the two other groups reported more severe psychological IPV. Moreover, the legally mandated and formally pressured groups reported more perpetrated injuries than the self-referred group. The variance explained in these variables was relatively small (1.6%). No significant group differences were found for minor physical IPV, minor and severe sexual coercion, or coercive control.
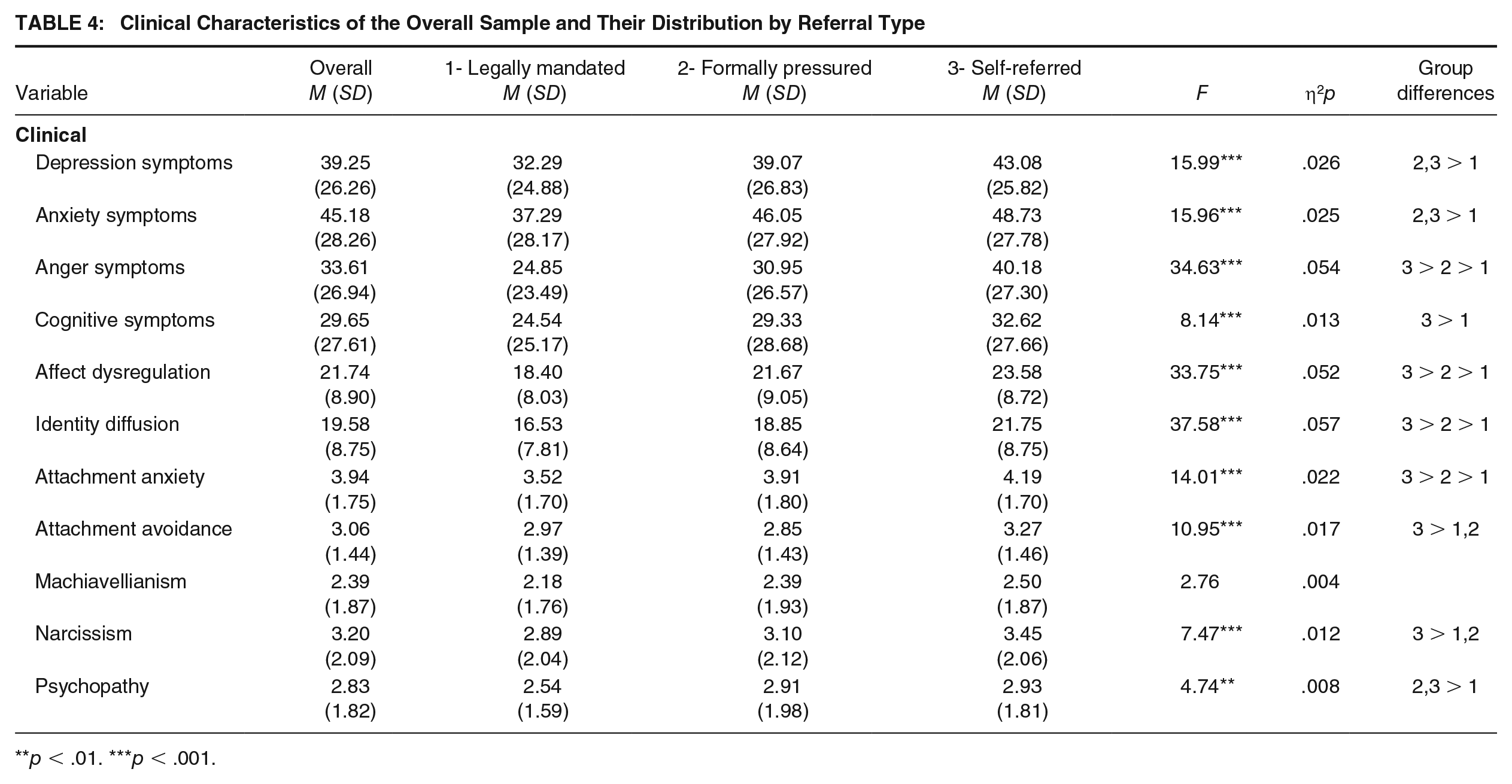
Table 4 shows clinical differences among the three referral groups. Self-referred men reported higher levels of anger, affect dysregulation, identity diffusion, and attachment anxiety than the formally pressured group, who reported higher levels than the legally mandated group. Men in the self-referred group also reported higher levels of attachment avoidance and narcissistic traits than men in the two other groups. In addition, they reported more cognitive symptoms than men in the legally mandated group. Men in both the self-referred and formally pressured groups reported more depression, anxiety, and psychopathy traits compared with men in the legally mandated group. The variances explained for anger symptoms (5.4%), affect dysregulation (5.2%), identity diffusion (5.7%), attachment anxiety (2.2%), attachment avoidance (1.7%), narcissistic traits (1.2%), cognitive symptoms (1.3%), depression symptoms (2.6%), anxiety symptoms (2.5%), and psychopathy traits (0.8%) were relatively small. No significant group differences were found for Machiavellianism traits.
Clinical Characteristics of the Overall Sample and Their Distribution by Referral Type
p < .01. ***p < .001.
Discussion
In this study, we compared three types of IPV perpetrators (self-referred, legally mandated, and formally pressured) based on their sociodemographic and clinical characteristics. Relying on a large sample of men entering IPV treatment within a Canadian province, we were able to study underexplored variables such as the severity of physical, psychological, and sexual IPV. The innovative approach of evaluating IPV in terms of severity rather than frequency provided a more nuanced understanding of IPV dynamics. Our findings suggest distinct profiles of IPV perpetrators based on their referral types. Generally, self-referred men reported more clinical symptoms compared with other referral types, legally mandated and formally pressured men reported more severe forms of IPV than self-referred men, and formally pressured men exhibited a mixed profile, often resembling the legally mandated group, but sometimes resembling the self-referred men.
Self-Referred
Supporting the first hypothesis (H1), self-referred men were older and had higher levels of education compared with those who were legally mandated. Older age often brings increased life experience, maturity, and a stronger desire of meaningful pursuits (Sheldon & Kasser, 2001). In addition, higher levels of education can enhance psychological resources, promote healthier behaviors, and foster a desire to maintain one’s social status (Cohen & Syme, 2013; Niemeyer et al., 2019). Regarding the first research question (Q1), self-referred men had higher incomes, were more likely to be born in Canada, and were more likely to have received a mental health diagnosis compared with both the legally mandated and formally pressured groups. A higher income may enable these men to be more financially capable of voluntarily seeking psychological help, while being born in Canada might facilitate awareness of local resources and reduce fears of discrimination when seeking help. The fact that self-referred men were more likely to have a mental health diagnosis could indicate that they experience more symptoms, but also that they are more inclined to seek medical help (Wu et al., 2023). This suggests that health care services could play an important role in identifying IPV (Dziewa & Glowacz, 2024; Tarzia et al., 2020), which could facilitate voluntary engagement in follow-up care. It is also possible that these men received some pressure to access IPV treatment by a mental health professional. In addition, self-referred (and formally pressured) men were more likely to be in a relationship than legally mandated men, which could be the result of seeking help because of an ultimatum from their partner, as found by Dutton and Starzomski (1994). Furthermore, self-referred men reported more suicidal thoughts–but not suicidal attempts–than the two other groups. This could indicate that self-referred men are more comfortable admitting they experience psychological distress than other groups. However, the fact that they are more likely to have access to a firearm warrants attention, as they have direct access to a means to end their life (or the life of their partner).
Supporting the second hypothesis (H2), self-referred men reported higher levels of depression, anxiety, and affect dysregulation compared with those who were legally mandated. In addition, they reported more anger, affect dysregulation, identity diffusion, attachment insecurity (anxiety and avoidance), and narcissistic traits compared with those who were legally mandated or formally pressured, and reported more cognitive symptoms and psychopathy traits than the legally mandated group, addressing the third research question (Q3). These results reveal a heightened clinical profile in self-referred men, marked by higher scores on all clinical measures. Consistent with Seto et al. (2022), this suggests that self-referred men would be more attuned to their distress, which may have motivated them to seek help voluntarily. By doing so, they may have already initiated a process of change, acknowledging their personal issues (Bowen & Gilchrist, 2004). Their higher scores may also indicate that they are less influenced by social desirability concerns compared with the other groups (Tutty et al., 2020), as the absence of formal external pressure would allow them to be more honest about their behaviors, emotions, and thoughts. In contrast, individuals with higher clinical symptoms may also adopt maladaptive coping mechanisms (Almeida et al., 2021), which could contribute to the denial of more severe instances of IPV.
Legally Mandated
In addition to their lower age, education and income (H1), the legally mandated men were more likely to use substances, namely stimulants (e.g., cocaine), compared with men in the other two groups, as well as cannabis on a weekly basis compared with self-referred men (Q1), which was consistent with the findings of Seto et al. (2022). Expósito-Álvarez et al. (2021) suggest that substance use could serve as a coping strategy to alleviate or numb negative feelings and may indicate higher levels of impulsivity. In addition, a meta-analysis by Cafferky et al. (2018) has linked substance use to the perpetration of IPV. Addressing substance use is important, as it may impede therapeutic engagement and increase the likelihood of treatment dropout (Nguyen et al., 2023). In terms of judicial processes, the legally mandated group was more likely than the other two groups to be involved in other types of judicial processes (e.g., theft, assault, driving under the influence) and to have a restraining order against them. The substance use and judicial involvement may suggest the presence of a heightened criminal profile among legally mandated men. Despite no significant group differences regarding homicidal thoughts, legally mandated men reported more homicide threats or attempts. This suggests that they may act more impulsively (Haden & Shiva, 2008), but it could also indicate a tendency to minimize socially unacceptable thoughts (Tutty et al., 2020) to align with court expectations.
While legally mandated men reported less minor psychological IPV than the self-referred men, they reported more severe psychological IPV and injuries, addressing the second research question (Q2). Evaluating IPV in terms of severity rather than frequency allowed these nuanced findings to emerge, shedding light on previous research that detected higher frequencies of physical and psychological IPV reported by self-referred individuals (Dutton & Starzomski, 1994; Tutty et al., 2020). Consistent with Arce et al. (2024), IPV behaviors may need to be very concrete or severe for legally mandated men to recognize and report them as IPV, suggesting normalization, minimization, and denial of less severe violent behaviors compared with self-referred men. Legally mandated men may underreport perpetrated IPV to evade responsibility and minimize consequences, yet they often admit to severe incidents when these lead to court-mandated treatment. Having already been involved in the system for these acts, they may feel obligated to report them or believe they have nothing to lose by doing so. While the act is recognized, they may still deny personal responsibility (Dziewa & Glowacz, 2024). Their lower scores on all clinical indicators (H2) align with Arce et al. (2024), which found that legally mandated men systematically hid and denied clinical symptoms, including depressive and psychopathic symptoms. Also, Bowen and Gilchrist (2004) found that these men often enter treatment without recognizing that they have a violence problem or fully understanding its impact on victims. These patterns highlight the need for tailored approaches that address denial and minimization while promoting genuine accountability and awareness of the impact of IPV.
Formally Pressured
Men in the formally pressured group did not significantly differ from men in the legally mandated group in terms of age, education, annual income, mental health diagnosis, and weekly cannabis consumption (Q1). However, they were more likely to acknowledge that their close ones believed they had a substance use problem, which is not surprising given their higher likelihood of being in a relationship compared with the legally mandated group. In addition, although they did not receive a court order, they were more likely to be involved in a process related to Youth Protection compared with both the self-referred and legally mandated groups, probably because they were more likely to be the father of at least one child. Although Seto et al. (2022) did not compare the groups based on parental status, about one-third of the formally pressured participants were in this group because they were referred by Youth Protection. In terms of perpetrated IPV, there was no significant differences between men in the formally pressured group and men in the legally mandated group regarding severe psychological IPV and injuries (Q2). However, men in the formally pressured group reported more severe physical IPV than men in the self-referred group. This may be because the violence is already known by Youth Protection, which led to their referral. The involvement of Youth Protection may also play a role, as they tend to show greater leniency toward a father who appears further along in his process of taking responsibility. The risk of losing custody of their children is real, and the commitment required by Youth Protection services can strongly motivate an individual to be exemplary and answer honestly (Buisson et al., 2024).
In terms of clinical measures, the formally pressured men, like the legally mandated men, reported lower levels of attachment avoidance and narcissistic traits compared with the self-referred men (Q3). The formally pressured group scored between the self-referred and legally mandated groups on several clinical variables, including suicidal thoughts, anger symptoms, affect dysregulation, identity diffusion, and attachment anxiety. They also reported similar levels of depressive and anxious symptoms, as well as psychopathic traits, compared with the self-referred men. Despite their profile resembling that of legally mandated men, formally pressured men exhibited a clinical profile that fell between the self-referred and legally mandated groups. Their willingness to report more clinical issues may stem from having children in their care, as the risk of losing them could strongly motivate serious engagement in IPV treatment. Their admission of higher anxiety and depressive symptoms, as well as psychopathic traits might indicate that their process of change is slightly more advanced than that of the legally mandated men, as acknowledging such distress and negative personality traits is challenging and requires a certain level of self-awareness regarding their issues (Bowen & Gilchrist, 2004).
Limitations
Despite its innovative approach and large sample size allowing the comparison of three groups of men entering IPV treatment on a variety of indicators, this study has limitations. First, the absence of a social desirability measure limits the ability to determine whether legally mandated and formally pressured groups are motivated to conceal clinical symptoms. Future research could address this limitation by incorporating such measures. The lower representation of legally mandated men may limit the generalizability of the findings to international samples where most IPV perpetrators are court-ordered to treatment. Compared to the United States, Canada typically has lower rates of legally mandated referrals (Tutty et al., 2020). This may reflect differences in judicial systems as well as health care systems, where Canadian health care professionals may be more likely to refer men to IPV treatment before authorities are involved. Future research could aim for a more balanced yet representative distribution among the referral types. Although the study provided insights into how external pressures relate to perpetrator characteristics, it did not assess motivation levels (e.g., intrinsic, extrinsic, amotivation), which are crucial for understanding readiness to change and treatment engagement. Future research could incorporate measures of motivations and stages of change to capture these nuances across referral types. The sole reliance on perpetrators’ self-reported data may have introduce biases, such as recall bias, lack of introspection, mistrust, minimization or denial of behaviors, and social desirability. In addition, the subscale of coercive control had a lower reliability, which could limit the validity of the results for these behaviors. To address these limitations, future research could use multiple data sources such as therapist reports, (ex-) partners, or legal records to validate self-reported information. Although our sample represented a wide range of age and socioeconomic statuses, it predominantly comprised cisgender heterosexual Canadian men, limiting the generalizability of the findings to culturally diverse populations and the LGBTQ+ community. Future studies could aim to recruit more diverse samples to explore underrepresented groups’ unique experiences. In addition, the cross-sectional design limits the ability to establish whether referral status is related to treatment completion or recidivism. Finally, the relatively low effect sizes highlight the importance of creating profiles based on referrals, motivations, and stages of (or readiness to) change to offer even more specific and tailored interventions.
Implications
Our findings extend previous research and provide insights for developing tailored therapeutic interventions for IPV perpetrators, based on their referral type: self-referred, legally mandated, or formally pressured. Our results suggest that legally mandated men would underreport their violent behaviors and personal difficulties when entering treatment, possibly because of mistrust, resistance, or denial. To address this, programs could assess motivation and readiness to change, striving to help individuals in this group be prepared to engage meaningfully in the process of behavioral transformation. Although levels of motivation were not specifically assessed, it appears that legally mandated men, primarily driven by legal obligations, were more externally motivated than formally pressured men, who, in turn, were more externally motivated than self-referred men. External motivation may require more intensive work to help clients take ownership of their help-seeking process, acknowledge their actions, and genuinely commit to change. Additional pre-treatment sessions could be beneficial for establishing trust and mutual understanding while also supporting legally mandated and formally pressured men in aligning their motivations more closely with those of self-referred men. Also, the tendency of legally mandated and formally pressured men to use substances should also be considered, as it may undermine the effectiveness of IPV treatment (Nguyen et al., 2023). Based on our results, it may be beneficial to educate the general public about behaviors that constitute violence and to encourage close relations to discuss available services when they observe such behaviors. This approach could encourage individuals to seek help at the earliest signs of abusive behavior, rather than waiting for interventions by the justice system. Furthermore, Rosenbaum et al. (2001) suggest that self-referred men may feel discouraged from participating in group-based treatment alongside legally mandated men, who often focus on expressing anger toward the judicial system and show lower levels of responsibility acceptance. In the United States, where most clients are legally mandated, the discrepancy in motivation and feeling of isolation of self-referred clients could even lead them to drop out of treatment (Evans et al., 2024). However, this dynamic might differ in places like Canada, where there is a more balanced mix of referral types (Tutty et al., 2020). Motivational interviewing prior to starting group-based treatment could be useful in identifying users’ stages of motivation and helping them uncover their personal motivations for change (Pinto e Silva et al., 2023). Taken together, our results emphasize the importance of considering the unique characteristics of these three groups, each with distinct profiles, types of violence, and, therefore, differing treatment needs (Butters et al., 2021; Expósito-Álvarez et al., 2021). This approach might foster client retention, engagement, and the overall efficacy of interventions aimed at breaking the cycle of IPV.
Footnotes
Authors’ Note:
This research was funded by a SSHRC Partnership Development grant (# 890-2020-0029). We have no known conflict of interest to report.