
Abstract
Within the Christchurch Health and Development Study (N = 1,265), we examine the prevalence and continuity of firesetting across the life course and explore whether adolescent firesetting is a risk marker for adult internalizing and externalizing behaviors. Life course continuity of firesetting was low. Adolescent firesetting (3%) correlated with antisocial behaviors and adverse family circumstances. Independent of conduct disorder, adolescent firesetting showed limited associations with adulthood internalizing outcomes, but associated with most externalizing outcomes (e.g., cannabis use disorder, OR = 2.08, 95% CI = [1.14, 3.78]). Further adjustment for antisocial tendencies and family circumstances reduced associations; the largest effect to remain was for alcohol use disorder (OR = 2.08, 95% CI = [1.19, 3.63]). Therefore, for most externalizing behaviors, adolescent firesetting is a marker (i.e., indicates future risk), but not an independent risk marker (i.e., does not have independent specificity). For adolescents who set fires, clinical treatment should assess comorbid conduct disorder and family instability and consider a range of problematic outcomes.
Keywords
Deliberate firesetting by children and adolescents is an enduring social problem and can be present with or without conduct disorder (MacKay et al., 2006). Although a curiosity in fire is developmentally appropriate, the intentional and deliberate lighting of fires can have devastating consequences (Ellithy et al., 2022). Suspicious and deliberate fires have been estimated to account for approximately half of all vegetation fires in Australia (Bryant, 2008), and arson is estimated to cost the Australian community approximately US$2.3 billion per year (Smith et al., 2014). Furthermore, between 2014 and 2018, fire departments in the United States responded to 30,460 fires caused by fire-play and 52,260 intentional structure fires, resulting in approximately 450 fatalities, 1,460 injuries, and more than US$1 billion in property damage each year (Campbell, 2021a, 2021b). The human costs of deliberate fires are also significant, with firesetting as a recognized risk factor for pediatric burn injury (Tyler et al., 2019).
Child and Adolescent Firesetting Behavior
Engaging in fire-play (e.g., playing with matches or fireworks, putting paper on fire) is developmentally normal (Lambie et al., 2015), and childhood firesetting is predominantly driven by curiosity or fire interest with less intent of harm (Gaynor, 2002). However, firesetting in adolescence is suggested to be more deliberate and pathological (Lambie et al., 2023), and result from a desire to test boundaries, and from delayed maturation related to risk assessment and decision-making (Gaynor, 2002; Pooley & Ferguson, 2017), and maladaptive or antisocial motivations (Fineman, 1995). Of all deliberately lit fires, children and adolescents are responsible for around 30% to 60% (Dolan et al., 2011; Lambie et al., 2013), with almost one in three adolescents reporting having engaged in firesetting behavior (Del Bove et al., 2008; MacKay et al., 2009). Patterns of firesetting behavior generally align with the developmental trajectories of offending and antisocial behaviors (Moffitt, 2017a), peaking in early-to mid-adolescence (Del Bove et al., 2008; Klein et al., 2008). Nevertheless, approximately 50% to 60% of children and adolescents who set fires repeat this behavior (Kolko et al., 2005; MacKay et al., 2009), and an estimated half of those who light fires in adolescence continue firesetting during adulthood (Barrowcliffe & Gannon, 2015). Despite this, no research has prospectively examined the continuity of firesetting from childhood through adolescence into adulthood. Research examining the life course trajectory of firesetting is critical for understanding this behavior and for targeting prevention and early intervention initiatives.
Firesetting and Conduct Problems
Some have argued that firesetting by children and adolescents is best understood as part of a spectrum of maladaptive and antisocial behaviors (Lambie & Randell, 2011). Firesetting is one of the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) symptoms of conduct disorder and therefore many externalizing and internalizing factors associated with this behavior are similar to those seen in those who have broader conduct problems (American Psychiatric Association, 2013). Similar to children and adolescents who have conduct problems, young people who set fires are likely to have a history of adverse childhood/family experiences and problematic behaviors, high levels of emotional dysregulation, and mental health problems (Perks et al., 2019). Compared to adolescents who have not set fires, including those with a diagnosis of conduct disorder (Kolko et al., 1985), problematic internalizing and externalizing behaviors are generally more severe and persistent (Martin et al., 2004). For example, childhood and adolescent firesetting behavior has been associated with a range of existing or later problems including overt (e.g., aggression) and covert (e.g., lying, stealing, vandalism) antisocial behavior (Kolko et al., 2005; Repo & Virkkunen, 1997), animal cruelty (Baglivio et al., 2017; Becker et al., 2004; Sakheim & Osborn, 1999), substance use (MacKay et al., 2009; Martin et al., 2004), depression (Martin et al., 2004), and suicidality (Räsänen et al., 1995; Tanner et al., 2016). Unsurprisingly, diagnosed conduct disorder is also strongly associated with firesetting in children and adolescents (MacKay et al., 2006). However, although conduct disorder is frequently diagnosed among children and adolescents who set fires, conduct disorder is neither necessary nor sufficient to explain firesetting behavior, as not all of those who set fires meet the diagnostic criteria for conduct disorder and vice versa (MacKay et al., 2006). Further, not all young people who set fires do so in the context of wider antisocial behavior.
Developmental Theories of Criminal Behavior
While there is a lack of empirical literature on the continuity of firesetting and its relationship with conduct problems, well established developmental theories of criminal behavior suggest two main trajectories of antisocial behavior (Moffitt, 2017a). The adolescent-limited trajectory is characterized by psychological discomfort caused by a “maturation gap,” and a desire for dependent status, autonomy, and peer acceptance (Moffitt, 2017b). Adolescent-limited youth tend to engage in “near normative” and transient antisocial behavior during adolescence, which dissipates through social maturation by early adulthood (Moffitt, 2017b). In contrast, the life-course-persistent trajectory represents a minority of young people whose offending is persistent and pathological in nature and is characterized by higher rates of parental/parenting difficulties, family conflict, under-controlled temperament, neurological problems, and personality difficulties (Moffitt, 2017a). Although the adolescent-limited and life-course-persistent trajectories are empirically supported, their applicability to firesetting is yet to be established with only one study having longitudinally examined the relationship between childhood and adult firesetting (Tyler et al., 2022), and none having examined the continuity of firesetting from childhood, through adolescence, to adulthood.
Previous Research
Although well established that early-life conduct problems associate with adulthood internalizing and externalizing problems (Erskine et al., 2016; Fergusson et al., 2005, 2015), the role played by firesetting remains unclear. We do not understand whether the association between adolescent firesetting and adult internalizing and externalizing problems is independent of conduct disorder symptoms. Previous studies have suggested that firesetting is either (a) part of a spectrum of antisocial behaviors engaged in by children and adolescents (Walters, 2023), (b) an indicator of more severe and pervasive forms of conduct problems, but not an independent risk marker (Becker et al., 2004; Forehand et al., 1991; Stickle & Blechman, 2002), or (c) has some specificity independent of conduct problems (Howell Bowling et al., 2013; Kolko et al., 1985; MacKay et al., 2006).
Past research either does not account for conduct problems or has mostly relied on cross-sectional designs and pooled clinical samples of children and adolescents, with only one population-based study (based on the Christchurch Health and Development Study, CHDS) having looked longitudinally at adulthood outcomes among children (< 10 years of age) who set fires, while accounting for conduct problems (Tyler et al., 2022). Therefore, no population-based research has explored whether firesetting in adolescence, rather than in childhood (Tyler et al., 2022), is associated with internalizing and externalizing problems in adulthood, independent of conduct problems. Examining this relationship is critical for understanding life course trajectories for young people who set fires, and for assessment and intervention planning. Particularly, whether prevention and early intervention strategies should target firesetting specifically or conduct problems more generally.
The Current Study
Our current research extends on our earlier study within CHDS that focused on adult outcomes among children who set fires (Tyler et al., 2022). This previous work showed that while childhood firesetting is associated with adult externalizing and suicidal behavior, it is not an independent risk marker (Tyler et al., 2022). However, compared to childhood firesetting, adolescent firesetting is suggested to be more antisocial and pathological in intent (Lambie et al., 2023). It is therefore plausible that, although childhood firesetting was not an independent risk marker (Tyler et al., 2022), firesetting during the adolescent period may serve as an independent risk marker for later harm. Within CHDS, a New Zealand community birth cohort followed to age 35 to 40 years, the current research aims to determine whether adolescent firesetting has specificity as a risk marker for adult internalizing and externalizing behaviors independent of adolescent conduct problems. Given that adolescent conduct disorder and firesetting are not mutually exclusive (MacKay et al., 2006), and that adolescents who set fires are more likely to engage in extreme antisocial behavior relative to their non-firesetting peers (Kolko et al., 1985; Martin et al., 2004), we hypothesize that adolescent firesetting will have some independent specificity as a risk marker for adult internalizing and externalizing problems. In secondary exploratory analysis, we describe the continuity of firesetting behavior measured during childhood (annually 7-10 years of age), adolescence (annually 14-16 years of age), and adulthood (35 and 40 years of age), and report the prevalence of adolescent firesetting.
Method
Study Design and Participants
All data were collected within the CHDS, a longitudinal birth cohort study of 1,265 children (50% male) born in the urban region of Christchurch, New Zealand in the mid 1977 (Fergusson & Horwood, 2001). Longitudinal waves were assessed at birth (in 1977), 4 months, 1 year, annually to age 16, and then at ages 18, 21, 25, 30, 35, and 40 years (in 2017). At baseline, participants identified as New Zealand European (84%), New Zealand Māori (13%), and Pacific Island ethnicities (3%). At each wave of data collection, trained interviewers conducted in-person interviews using structured self-report and parent-report instruments. Overall, retention has been high in CHDS with 904 of the original cohort completing assessments at age 40 years, representing 74% of surviving cohort members. Our main analyses were based on data collected at age 14 to 16 (N = 996) through age 35 to 40 years (N = 904). Compared to those lost to follow-up, the retained samples at each age underrepresented individuals from socially disadvantaged backgrounds (e.g., low socioeconomic status and parental education level). Therefore, to account for any selection effects arising from missing data, we use data-weighting methods in all main analysis (Carlin et al., 1999). The New Zealand Health and Disability Ethics Committee approved CHDS. Participants and parents provided written consent for each wave of data collection.
Measures
Because CHDS is a 40-year study, we have not summarized all CHDS measures, but we have described all covariates, exposure variables, and outcome variables relevant to the current study below. Where diagnoses have been indicated, this was based on the validated survey tools and no diagnosis was made by a clinician. For example, the Composite International Diagnostic Interview (CIDI) is a structured diagnostic interview developed for use by lay interviewers in research purposes to generate diagnoses of mental disorders and has been extensively appraised for such use (e.g., Kessler et al., 2004). For additional details about the validity and derivation of DSM symptom criteria and behavioral or mental disorder classification, please see previous works (Fergusson et al., 2010; Kessler et al., 2004, 2007).
Child (7-10 Years) and Adolescent (14-16 Years) Firesetting
Childhood firesetting was measured with parent-reported conduct problems at age 7 to 10 years. Parents were asked if the participant “sets or starts fires” in the previous year, answers were given on a three-point scale from 1 = doesn’t apply to 3 = certainly applies. Participants whose parents rated this as certainly applies in at least one interview were classed as having childhood firesetting.
As part of a broader assessment of adolescent conduct problems (see below), at the age 14- and 16-year assessment, participants were asked the number of times they had “set or started fires where you should not be burning anything” in the previous year. Parents were also asked if their child had “set or started fires” in the previous year. Responses ≥ 1 (either by participant or parent at the age 15- or 16-year assessment) were coded as yes, the participant set fires.
Adolescent Conduct Disorder (14-16 Years)
Participants and their parents were interviewed separately at two assessments (age 14-15 and age 15-16 years) using the Self-Report Early Delinquency Scale (Moffitt & Silva, 1988) to derive a Diagnostic and Statistical Manual of Mental Disorders, revised 3rd edition (DSM-III-R) diagnosis of conduct disorder. Diagnoses were made based on combined data (parent and self-report) from the two assessments.
Externalizing Outcomes (16-40 Years)
All externalizing outcomes were derived from self-report interviews completed during the following assessment periods: 16 to 18, 18 to 21, 21 to 25, 25 to 30, 30 to 35, and 35 to 40 years of age.
Substance use disorders
We derived symptoms of alcohol use disorder (AUD), nicotine use disorder, and cannabis use disorder (DSM-IV or DSM-V [at age 40 years] abuse or dependence) from the CIDI (Robins, 1988). Those who met criteria for disorder at each assessment period were classified as having that disorder.
Property offending and violence perpetration
Participants completed the Self-Report Delinquency Inventory (Moffitt & Silva, 1988) at each assessment period. For property offending, this inventory measures the intentional damage of others’ property, breaking and entering, shoplifting, theft, and car conversion. A dichotomous variable (yes: any property offending reported) was created for each assessment period.
The same inventory (Moffitt & Silva, 1988) was used to measure violence perpetration, supplemented by additional custom-written items, such as “carrying a hidden weapon,” “aggravated burglary/robbery,” and “being involved in a gang fight.” In its entirety, this measure captures a range of violent behaviors including physical assault, use of a weapon against others, cruelty to animals, robbery, and sexual violence. A dichotomous variable (yes: any violence perpetration) was created for each assessment period.
Internalizing Outcomes (16-40 Years)
All internalizing outcomes were derived from self-report interviews completed during the following assessment periods: 16 to 18, 18 to 21, 21 to 25, 25 to 30, 30 to 35, and 35 to 40 years of age.
Suicidal ideation
Using an item from the major depression section of the CIDI, participants reported on suicidal thoughts (Robins, 1988). We derived a dichotomous variable (yes: ideation) representing whether at least one incident of suicidal ideation was present for each assessment period.
Anxiety disorder and major depression
At each assessment period, participants completed the CIDI to report symptoms of depression and anxiety since the previous assessment wave (Robins, 1988). Using DSM diagnostic criteria for major depression and anxiety disorder (American Psychiatric Association, 1994), we created two dichotomous variables (yes: anxiety disorder; yes: major depression) representing whether participants met criteria for either disorder at each assessment period.
Potential Covariates (Birth-16 Years)
Potential covariates to control for in analyses were selected based on their association with early-life conduct problems, firesetting, and later adverse outcomes, including social, individual, and familial factors.
Childhood abuse (0-16 years)
At ages 18 and 21 years, sample members were questioned about their experience of sexual abuse during childhood (< 16 years) (Fergusson et al., 1996). Questions included abusive experiences from episodes involving non-contact abuse (e.g., indecent exposure) to episodes involving attempted or completed intercourse. A four-level scale was devised reflecting the most extreme form of sexual abuse reported by the young person at either age.
At ages 18 and 21 years, sample members were questioned about their experience of physical punishment during childhood (< 16 years) (Fergusson & Lynskey, 1997). Questioning spanned an array of experiences with physical punishment and the frequency with which these occurred during childhood. A four-level scale was devised reflecting the most extreme form of physical punishment reported by the young person at either age.
Parental intimate partner violence (0-16 years)
At the age of 18 years, participants answered questions about their experience of violence between parental figures during their childhood (prior to age 16 years), with questions derived from Conflict Tactics Scale (CTS: Straus, 1979). Separate questioning was conducted for violence initiated by the father against the mother, and for violence initiated by the mother against the father. Items were combined into a single scale score representing overall exposure across both parents.
Parental education and family socioeconomic status (birth)
Maternal and paternal education were assessed at baseline (participant birth) using a three-level scale measuring the highest level of educational achievement attained. Family socioeconomic status (SES) was assessed at the time of the survey of child’s birth using the Elley and Irving (Elley & Irving, 1976) scale of SES for New Zealand.
Family standard of living and income (0-10 years) and family instability (0-15 years)
At each assessment period, we obtained a global assessment of the material living standards and income of the family via interviewer rating. We averaged the ratings over the period 0 to 10 years. As a measure of family instability, parents also reported the number of changes of parenting figures of age 0 to 15 years.
Childhood attention problems and withdrawn or anxious behavior (7-9 years)
Childhood attention problems and anxiety/withdrawal was measured using a CHDS-developed scale based on validated questionnaires (Conners, 1970; Fergusson & Horwood, 1993; Rutter et al., 1970). Parents and teachers completed the 15-item scale at participant age 7, 8, and 9 years. Each item was rated on a three-point Likert-type scale, ranging from 1 (doesn’t apply) to 3 (certainly applies). The scale created from the items reflects children’s tendency toward anxious/withdrawn behavior.
Childhood IQ (8-9 years)
Participants were assessed with the revised version of the Wechsler Intelligence Scale for Children modified for New Zealand conditions (Wechsler, 1974). At age 8 and 9 years, total IQ scores were computed using the method described in the test manual. The reliabilities of these measures were assessed using the split-half methods ranged from .93 to .95. For the current analysis, IQ was based on an average of the total IQ score at the two ages.
Adolescent grade point average (11-13 years)
Teacher ratings assessed participant school performance in reading, handwriting, written expression, spelling, and mathematics using a five-point scale ranging from very good to very poor. As a global measure of educational achievement from 11 to 13 years, ratings were summed across years and curriculum areas and averaged to provide GPA.
Parent illicit drug use and alcohol problems (11-15 years)
Parents were questioned regarding their history of illicit drug use at participant age 11 years. Participants were classified as having a parent history of illicit drug use if one of his or her parents reported a history of illicit drug use. Parent alcohol problems were assessed with parent report at participant age 15 years. We also created a dichotomous measure of whether or not the participants’ parents reported experiencing problems with alcohol.
Adolescent personality (14-16 years)
Neuroticism (α = .80) and extraversion (α = .79) were both assessed using a short form version of the Neuroticism scale of the Eysenck Personality Inventory (Eysenck & Eysenck, 1964) at age 14 years.
Adolescent ADHD, oppositional defiant disorder, anxiety disorder, and major depression diagnosis (14-16 years)
Cohort members and their parents were interviewed separately at two assessments (age 14-15 and age 15-16 years) using items from the Diagnostic Interview Schedule for Children to derive DSM-III-R diagnoses of attention-deficit/hyperactivity disorder (ADHD) (Costello et al., 1982), oppositional defiant disorder, anxiety disorder, and major depression. Diagnoses were made based on combined data (parent and self-report) from the two assessments.
Adolescent deviant peers (15 years)
At the age 15-year assessment, participants and their parents were asked about how many of the young person’s friends had a history of substance use (including tobacco, alcohol, or illicit drugs) or criminal behavior. The highest number of the participant or parent report was taken as the measure of deviant peer affiliation.
Parental bonding (16 years)
Participants responded to the maternal and paternal care scales of the Parental Bonding Instrument (Parker et al., 1979). This scale measures the extent to which parents provide support, affection and nurturing; high scores indicate high levels of care.
Statistical Analyses
All models were fitted in Stata version 17.0. Following descriptive analysis, we generated correlation coefficients between adolescent firesetting and all potential covariates. For our main analysis, we used chi-square tests to examine the percentage of those in the cohort who experienced each outcome at any age period, with and without adolescent firesetting. Next, we used three generalized estimating equation (GEE) models to test our hypothesis to estimate the associations between adolescent firesetting and adult outcomes. We treated all outcomes across adulthood as repeated measures, with the effect estimate being the population-averaged odds ratio (OR) or the incidence rate ratio (IRR, for the count of outcomes) across all age periods. GEE models are robust to missing data under the assumption that data are missing-at-random, data are included as long as a participant has at least one observation of the repeated measure, N = 1,025 to 1,053 participants had data on at least one observation for each outcome (81%-83% of original cohort), and GEE models account for the correlated nature of repeated measures within individual cases (Schafer & Graham, 2002).
First, we estimated the unadjusted bivariate associations between firesetting and each outcome. Second, we fitted the same models adjusting for adolescent (age 14-16 years) conduct problems. With the third and final model fully adjusted for adolescent conduct problems, sex (male or female), and covariates (correlated p ≤ .05 with firesetting). Final models were selected by forward and backward selection of covariate factors to derive stable and parsimonious models.
Results
Continuity of Firesetting Behavior Across Childhood, Adolescence, and Adulthood
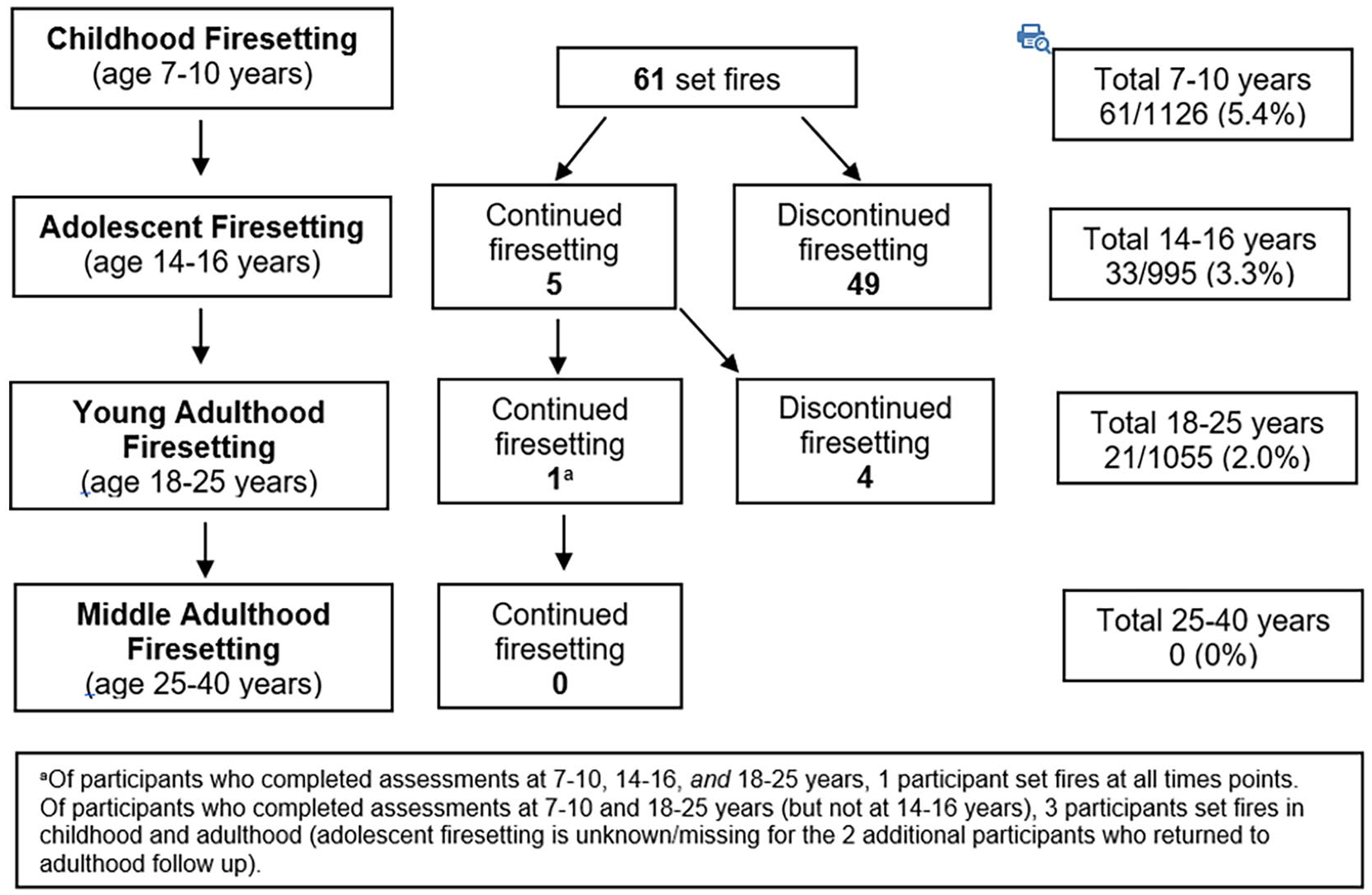
Figure 1 shows that the continuity of firesetting across the life course in this community cohort was low. As previously reported (Tyler et al., 2022), at age 7 to 10 years, 61 (5.4%) children reported setting fires. Of those 61 children, 54 responded to the questionnaire at 14 to 16 years, 49 (91%) of those participants reported that they did not set fires during adolescence, and 5 (9%) reported setting fires during both childhood and adolescence. In total, 21 participants (2%) set fires during adulthood, all below 25 years of age. Of the participants who completed assessments at each developmental period (childhood, adolescence, and young adulthood), only one participant set fires at all three time points (see Figure 1 notes). Only five participants set fires in both childhood and adolescence, and only four set fires in both adolescence and young adulthood.
Continuity of Firesetting From Childhood to Adulthood
Prevalence, and Correlates, of Adolescent Firesetting
In total, 33 participants reported lighting fires at age 14 to 16 years (3.3% of the sample retained to age 16 years), 28 (85%) of whom were male and 28 (85%) of whom did not set fires during childhood. As shown in Table 1, although small in magnitude, adolescent firesetting correlated positively with childhood and adolescent attention problems and withdrawn behaviors. Positive correlations were also evident with adolescent grade point average (GPA), depression, and deviant peer affiliations; and with family standard of living (0-10 years), parent drug use, parent alcohol problems, and parent offending. Negative correlations were obtained between firesetting and childhood IQ, maternal education, family income, and parental bonding/care.
Correlates of Adolescent (14-16 Years) Firesetting
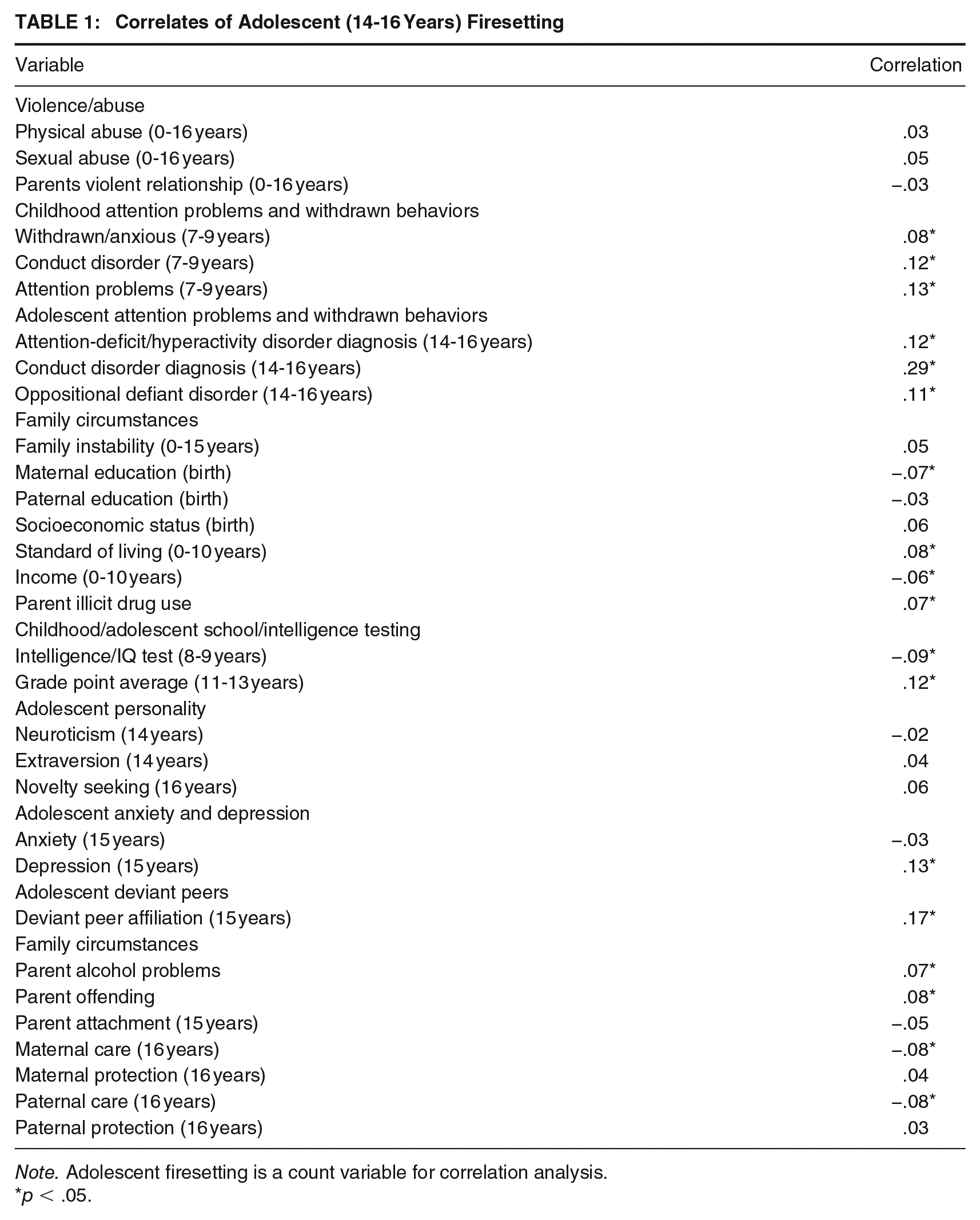
Note. Adolescent firesetting is a count variable for correlation analysis.
p < .05.
Associations Between Adolescent Firesetting and Adult Outcomes
Table 2 shows the percentage of participants with or without adolescent firesetting who reported each outcome at least once in any age period between years 16 to 18 and 35 to 40. Prevalence of all externalizing and internalizing outcomes was greater within participants who set fires during adolescence. Within the firesetting group, the experience of substance use (> 35%), and to a lesser extent aggression (violence/property offense) or anxiety/depression (> 20%), was relatively common.
Prevalence of Adult Externalizing and Internalizing Behavior for Those With and Without Adolescent Firesetting at Age 14 to 16 Years
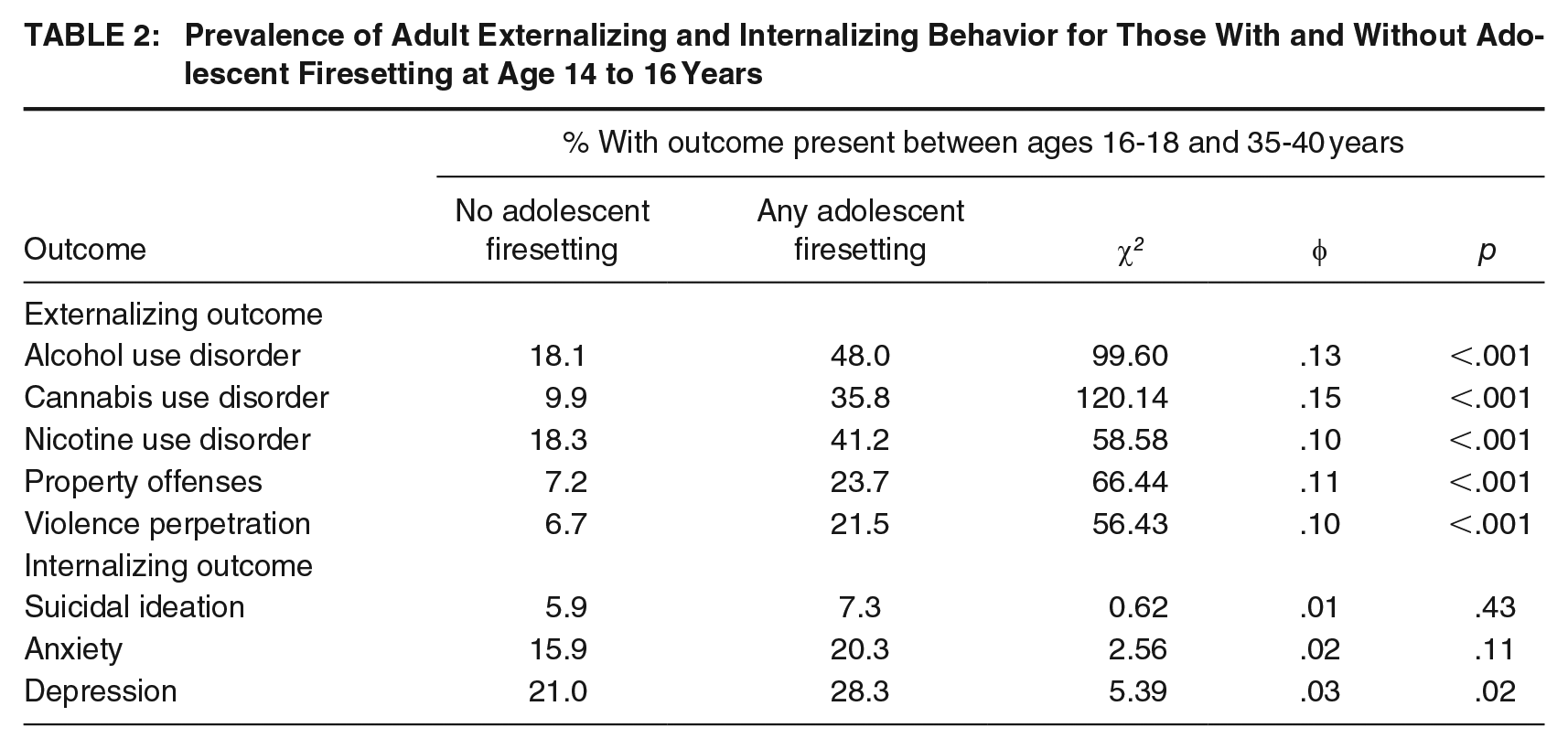
Table 3 shows the associations between adolescent firesetting and adult outcomes from the three sets of population-averaged GEE models: unadjusted models (Model 1), adjusted for adolescent conduct problems (Model 2), and fully adjusted for adolescent conduct problems and covariates (Model 3). In Model 1, there were several unadjusted associations between firesetting and externalizing outcomes, with effect sizes ranging from modest to large. The largest effects were obtained for cannabis use disorder and violence perpetration; for example, the odds of having a cannabis use disorder during adulthood were nearly six times greater among participants who did versus did not set fires during adolescence (OR = 5.79, 95% CI = [3.42, 9.72]). Although the effects with individual internalizing outcomes were small (ORs < 2.0), the rate of experiencing a higher total number of internalizing outcomes during adulthood was 1.3 times (95% CI = [0.97, 1.81]) greater for those who set versus did not set fires during adolescence, with the rate of experiencing a greater number of outcomes (externalizing or internalizing) 2.3 times greater (95% CI = [1.97, 2.75]).
Associations Between Adolescent Firesetting (14-16 Years) and Adult Externalizing and Internalizing Behavior
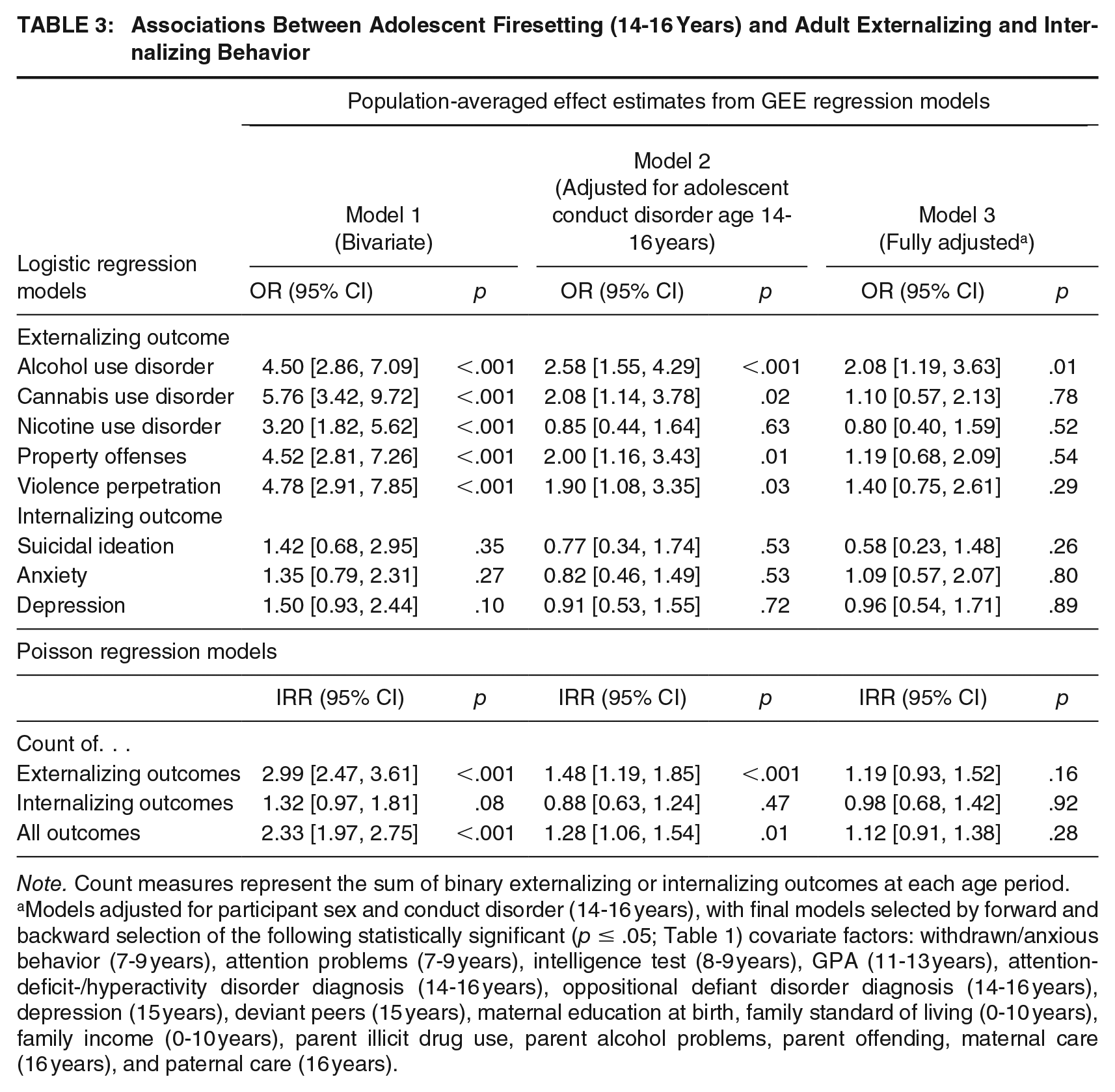
Note. Count measures represent the sum of binary externalizing or internalizing outcomes at each age period.
Models adjusted for participant sex and conduct disorder (14-16 years), with final models selected by forward and backward selection of the following statistically significant (p ≤ .05; Table 1) covariate factors: withdrawn/anxious behavior (7-9 years), attention problems (7-9 years), intelligence test (8-9 years), GPA (11-13 years), attention-deficit-/hyperactivity disorder diagnosis (14-16 years), oppositional defiant disorder diagnosis (14-16 years), depression (15 years), deviant peers (15 years), maternal education at birth, family standard of living (0-10 years), family income (0-10 years), parent illicit drug use, parent alcohol problems, parent offending, maternal care (16 years), and paternal care (16 years).
In Model 2, adjusting for adolescent conduct problems, the effects associated with adolescent firesetting reduced to modest in size. The largest effect obtained in this second series of models was for AUD: over and above the experience of conduct disorder, the odds of having AUD during adulthood remained two and a half times greater among participants who set versus did not set fires during adolescence (OR = 2.58, 95% CI = [1.55, 4.29]). In addition, despite potential conduct disorder, adolescent firesetters were still two times more likely to have cannabis use disorder and display antisocial behaviors (Table 3). For internalizing outcomes in Model 2, all effects are reduced and reversed, yet for those with (vs without) adolescent firesetting behaviors, the rate of experiencing a greater number of adverse internalizing outcomes remained 1.3 times greater (95% CI = [1.06, 1.54]), and the rate of experiencing a greater number of externalizing outcomes remained 1.5 times greater (95% CI = [1.19, 1.85]).
In the final Model 3, further adjustment for potential covariates reduced most effect sizes to small. The largest effect to remain was the association between adolescent firesetting and AUD (OR = 2.08, 95% CI = [1.19, 3.63]). Also noteworthy was that the rate of experiencing more total externalizing outcomes remained 1.2 times greater (95% CI = [0.93, 1.52]) among those who set fires.
Discussion
This is the first prospective study to report (a) the continuity of firesetting from childhood to adolescence, and from adolescence to adulthood, (b) the prevalence of firesetting behavior in adolescence, and (c) to examine adulthood substance use, antisocial behavior, and mental health among adolescents who set fires, independent of adolescent conduct problems. We found low continuity of firesetting over time, with few children who set fires going on to do so as adolescents or as adults. In this cohort, firesetting prevalence in adolescence was 3% and was not only associated with a range of antisocial adolescent behaviors, but also with adulthood externalizing problems up to 25 years later. However, inconsistent with our hypothesis that adolescent firesetting would have some independent specificity as a risk marker for adult problems, most associations with adulthood problems reduced on adjustment for adolescent conduct disorder and reduced further on adjustment for family circumstances and other antisocial tendencies; supporting the idea that firesetting is part of a spectrum of maladaptive and antisocial behaviors (Lambie & Randell, 2011). Taken together, although firesetting during adolescence is suggested to be more antisocial and pathological than firesetting during childhood (Lambie et al., 2023), we draw a similar conclusion to our previous work which found that childhood firesetting was a risk marker for adulthood externalizing and suicidal behaviors (Tyler et al., 2022). That is, as an extension to previous analysis (Tyler et al., 2022), our current results indicate that firesetting during the adolescent years is associated with adulthood problems, but that this had little independent specificity when also accounting for conduct problems, antisocial tendencies, and family circumstances.
Results in Relation to Past Research
We found that the prevalence of firesetting was highest in childhood (5%), reducing to 3% in adolescence, and 2% in early adulthood. This pattern contrasts previous work that suggests firesetting peaks in adolescence and that self-reported prevalence ranges from 6.3% to 33% (Del Bove et al., 2008; Klein et al., 2008; MacKay et al., 2012). However, 3% prevalence is consistent with the low base rates (1% to 4%) reported in studies where malicious intent is included in the firesetting definition (MacKay et al., 2012). The low prevalence rate in our cohort may also be lower than the previous reports because we measured firesetting between ages 14 and 15 years, and previous research suggests that firesetting peaks between 12 and14 years, and declines after that point (i.e., 14-15 years) (Del Bove et al., 2008; Klein et al., 2008). Rates may also be lower because children with conduct disorder are more likely to discontinue in research than those without (Fröjd et al., 2011). Clinical research suggests that children and adolescents who engage in continued and severe firesetting are more likely to have a diagnosis of conduct disorder (Sakheim & Osborn, 1999); therefore, it is possible that some individuals who would have continued firesetting in adolescence were lost through attrition. That said, the general pattern of results indicates that firesetting in this cohort broadly aligns with an adolescent-limited trajectory of antisocial behavior (Moffitt, 2017a).
Similar to past research (Martin et al., 2004), we found that adolescent firesetting was correlated with problematic childhood and adolescent behaviors (e.g., inattentive/withdrawn behavior, deviant peer relationships) and with adverse family circumstances (e.g., lower income and education, parental drug use). In further prospective analysis, we found moderately large (odds ratios between 3 and 6) unadjusted associations between adolescent firesetting and adult externalizing problems, but minimal associations with internalizing problems and suicidal ideation. Consistent with research showing firesetting to be an indicator or marker of more severe conduct disorder, rather than an independent syndrome (Stickle & Blechman, 2002), the majority of associations with firesetting reduced notably on adjustment for adolescent conduct disorder. However, in line with past research patterns (Martin et al., 2004; Repo & Virkkunen, 1997), the associations between adolescent firesetting and later alcohol and cannabis use disorder and antisocial behavior remained over and above the presence of conduct disorder. Yet, evidence that adolescent firesetting was an independent risk marker for such problematic adult behaviors was weak on further adjustment for sex, and other childhood/adolescent and family circumstances (e.g., family standard of living, parent alcohol problems, childhood attention problems, adolescent depression etc.). Most effects reduced to small, except for one remaining association between firesetting and adulthood AUD—adjusting for sex, conduct disorder, and all covariates, adolescents who set fires remained twice as likely to experience adulthood AUD.
Strengths and Limitations
The current research represents one of only a small number of prospective longitudinal studies of firesetting behavior and extends our understanding of the continuity and trajectories of adolescent firesetting. Our results are strengthened by our use of a community-representative sample of adolescents, given the low detection rates for youth firesetting (Del Bove et al., 2008). Although we cannot exclude under-reporting of firesetting behavior, we note that participants in this cohort are used to being asked about socially deviant behaviors, and they disclose these behaviors at high rates (Fergusson et al., 2005). However, our study was limited by a single item that was used to measure firesetting behavior within a broader measure of conduct problems, and the diagnostic structure of conduct problems has evolved since this cohort was in adolescence. We also acknowledge that the reported diagnoses in this study were based on the relevant assessment instrument and were not made by a clinician. However, despite changes in the diagnosis and measurement of conduct problems, the simplicity of the single firesetting item in our study means that the item is still relevant to adolescents today. Nevertheless, variations in the prevalence of firesetting have been noted in the wider literature dependent on operationalization and the informant source, with definitions including unsanctioned firesetting and self-reports yielding higher rates than those focusing on malicious intent and parental or professional reports (MacKay et al., 2012). We also did not measure the motivation, frequency, or seriousness of firesetting behavior, all of which may be important to assess when studying links to externalizing behavior (Del Bove et al., 2008; MacKay et al., 2009; Sakheim & Osborn, 1999). Moreover, CHDS is a birth cohort that is broadly representative of the population in Christchurch, New Zealand in the 1970s. In interpreting and translating our results, it is important to consider that adolescents in the 1980s are different from the 2020 cohort of adolescents of today. Furthermore, because the use of fire can differ between sociocultural contexts and countries (Pyne, 2019), our results may not generalize to other locations and cultures.
Implications and Conclusion
Firesetting is a potentially serious form of externalizing behavior. However, because firesetting is a relatively uncommon behavior in the population, coupled with the fact that it may not be spontaneously reported due to it being a highly stigmatized behavior (Vaughn et al., 2010), clinicians working with adolescents who present with any externalizing problems should consider the potential presence of undisclosed firesetting behavior.
Explanatory models of antisocial behaviors among young people have divided those behaviors into adolescence-limited and life-course-persistent types (Moffitt, 2017a). Within this typology, our data suggest that most firesetting during adolescence does not occur as part of a life-course-persistent pattern of firesetting, although many adolescents who set fires do go on to display other antisocial behaviors as adults. Where an individual has a history of firesetting, our data point to an elevated long-term risk of substance use disorder, property offenses and violent offending while the absolute long-term risk of further firesetting is surprisingly low. This implies that clinical assessment and management among people with an identified history of firesetting needs to focus on a broad range of outcomes in addition to firesetting behavior, including general behavioral problems, substance use, and mental health needs. Regardless of the overall low continuity and lack of independent associations between adolescent firesetting and adulthood outcomes, firesetting can be associated with injury, loss of life, and environmental damage. Moreover, many social housing and residential treatment providers exclude people with a history of firesetting (Ellison et al., 2013; Her Majesty’s Inspectorate of Probation, 2020). As a result, people who have set fires are difficult to resettle back into the community (Allender et al., 2005). This can lead to young people and their families being marginalized from services, resulting in poorer outcomes. The low rate of continuity between firesetting in adolescence and adulthood suggests that service providers should apply a more detailed contextual risk assessment in this situation, rather than declining referrals outright. However, those with firesetting are at elevated risk of a broad set of other antisocial behaviors in the future. Clinical risk management should therefore focus on all potential antisocial behaviors rather than primarily focusing on firesetting.
Consequently, effective identification, assessment, and intervention for adolescent firesetting remain important and clinicians assessing adolescents presenting with conduct problems should enquire as to the presence of firesetting so that appropriate intervention can be provided. Although the current study extends the limited evidence base on the trajectories of firesetting, further longitudinal research that characterizes the onset, continuation, and desistance of young people’s firesetting and associated outcomes is critical for developing a deeper understanding of this behavior and for directing resources and developing effective primary, secondary, and tertiary prevention strategies.
Footnotes
Authors’ Note:
The Christchurch Health and Development Study, Joseph M. Boden, and James A. Foulds are funded by the Health Research Council of New Zealand (Program Grant 16/600). We would like to thank all past and present researchers and participants within the Christchurch Health and Development Study.