
Abstract
A growing body of research is beginning to highlight the difficulty clinicians have in distinguishing delusional beliefs from conspiratorial beliefs. This mixed-methods study examined how 198 forensic mental health professionals in Canada and the United States differentiate delusional beliefs from conspiratorial beliefs. Participants were presented with an experimental vignette describing a forensic patient’s symptoms and were asked to diagnose the individual and, if qualified, opine on the defendant’s competency to stand trial. Results showed that idiosyncratic and highly rigid and distressing beliefs significantly predicted the diagnosis of a psychotic disorder, whereas shared beliefs held with low/moderate rigidity and distress significantly predicted the identification of conspiratorial beliefs. Despite participants’ abilities to differentiate delusional and conspiratorial beliefs, some participants reported that they lacked sufficient training in this area. Future research should examine if factors other than the social context and rigidity of the belief influence the differentiation of delusional and conspiratorial beliefs.
Introduction
Accurately assessing the presence and severity of mental disorders is crucial in forensic evaluations. In most jurisdictions, a diagnosis of a statutorily defined qualifying mental disorder is required for defendants to meet the legal criteria for certain findings, such as competency to stand trial (CST), criminal responsibility, and more (K. S. Douglas et al., 2012). Forensic mental health professionals (FMHPs) often use the Diagnostic and Statistical Manual of Mental Disorders (DSM), to guide diagnostic decisions and increase diagnostic reliability. Recently updated in 2022, the DSM (5th ed., text rev.; DSM-5-TR; American Psychiatric Association [APA], 2022) is widely accepted by clinicians and courts in North America, despite recent criticisms surrounding its lack of transparency and scientific validity, risk of false positives, and concerns with diagnostic legitimacy (Cohen et al., 2021; Mehdi et al., 2022; Wakefield, 2016). Although the DSM was designed primarily for clinical settings, rather than forensic contexts, FMHPs often utilize this manual when providing evaluation and treatment of individuals with mental illness (Al-Rousan et al., 2017; Bradley-Engen et al., 2010; Diamond et al., 2001; Fries et al., 2013; Prins, 2014).
The growing prevalence of mental disorders and substance use disorders among criminal defendants has led to increases in court-ordered CST evaluations (Tussey et al., 2022). The competency crisis, or the imbalance between referrals for CST evaluations and trained professionals who can conduct these evaluations, has resulted in unadjudicated defendants languishing in custodial environments, lawsuits, and millions of dollars in fines paid by state governments (Gowensmith, 2019). Psychotic disorders are particularly common among individuals found incompetent to stand trial (Pirelli et al., 2011). Given the prevalence of psychotic disorders among legally involved individuals, the possible implications of these disorders on a defendant’s legal circumstances, and the impacts on overburdened forensic mental health systems, diagnostic accuracy is of great importance.
Empirical data show that FMHPs have varied interrater reliability across all diagnostic categories, but high agreement when diagnosing psychosis (Gowensmith et al., 2017). Despite this reliability, FMHPs are increasingly completing evaluations that require diagnostic clarifications between delusions expressed as part of a psychotic disorder, and beliefs related to conspiracy theories (Cunningham, 2018). This differentiation can be crucial in determinations of CST, criminal responsibility, and more, and recent research highlights the difficulties that clinicians face when differentiating delusional beliefs and conspiratorial beliefs.
Delusional Beliefs
Accurately differentiating delusional and conspiratorial beliefs is essential as severe and persistent mental illness, such as schizophrenia spectrum disorders, are particularly common in forensic mental health systems (Gulayets, 2016; Pirelli et al., 2011). Unsurprisingly, defendants diagnosed with psychotic disorders are more likely to be found incompetent to stand trial and to present successful insanity defenses (Gulayets, 2016; Pirelli et al., 2011). Delusional beliefs secondary to delusional disorder, a schizophrenia spectrum disorder, are fixed, false belief(s) that persist in the face of conflicting evidence (APA, 2022). Delusions typically manifest within one individual, emerge from abnormal subjective experiences, and are often directly related to that individual (Pierre, 2021; Starcevic & Brakoulias, 2021). Those with delusional disorder typically do not experience marked functional impairments; however, inherent to the involvement in the legal system, forensic patients with delusional disorder often have more functional impairments than the general population. Due to the absence of other psychotic symptoms, delusional beliefs resulting from delusional disorder may resemble nonpsychotic conspiratorial beliefs.
Conspiratorial Beliefs
Conspiracy theories, also referred to as extreme radicalized or overvalued beliefs, are unusual beliefs surrounding the causes of social and political events that are shared among a group (K. M. Douglas et al., 2019). Oliver and Wood (2014) found that over half of all Americans endorsed at least one conspiracy theory related to current political events. Although conspiracy theories have long been part of North American culture, increasing human interconnectivity via the internet has led to an unparalleled exchange of ideas and information.
Recent research has shown that individuals who report social media as their primary source of news endorse higher levels of conspiratorial beliefs; however, the internet likely only increases conspiracy beliefs in those who are already predisposed to this type of thinking (Enders et al., 2021; Uscinski et al., 2022). For example, social media has played a crucial role in spreading and reinforcing conspiracy theories surrounding COVID-19 caused by the spread of misinformation (Dow et al., 2021; Stano, 2020). Social media provides a feedback mechanism that validates individuals’ conspiratorial beliefs through interactions with other users, such as likes and shares, or retweets on X/Twitter (Greve et al., 2022), and the internet can increase the endorsement of conspiracies by facilitating access to these beliefs through personalizing algorithmically selected content for viewers (Grandinetti & Bruinsma, 2023).
The content of conspiracy theories can be diverse in nature. Conspiracy theories vary in their plausibility, and some may be rooted in realistic events, such as the belief that targeted individuals are subjected to surveillance, whereas others include improbable and radical beliefs. There is a lack of research around the prevalence and types of conspiracy theories FMHPs are encountering currently. Nonetheless, some conspiracy theories that have become more prevalent in recent years in the United States include gang stalking (i.e., beliefs that targeted individuals are subject to mass surveillance, harassment, and mind-control; Pierre, 2020), sovereign citizens (i.e., individuals who believe they are not bound by U.S. laws; Parker, 2014), and beliefs related to Project MKUltra (i.e., that the U.S. Central Intelligence Agency performed illegal experimentation on citizens). Havana syndrome conspiracies are present in both the United States and Canada and consist of beliefs that diplomats have experienced “sonic attacks” in Cuba (Bartholomew, 2018). In addition, many conspiracy theories, such as QAnon, are rooted in antisemitism and discrimination and prejudice against Jewish people (Riedl et al., 2024).
Prior research has found that racial and ethnic differences exist among those who endorse conspiracy theories. Although Black Americans endorse higher levels of conspiracism than White Americans, the source of misinformation and content of conspiracies differ between these groups due to discrimination and racism (Simmons & Parsons, 2005). Conspiracy theories endorsed by White Americans tend to be rooted in tropes related to freedom and protection of the republic (Prasad, 2022). However, as Black Americans have a long history of exclusion and exploitation in the United States, cultural mistrust (i.e., a cultural coping response that expresses distrust, suspicion, and self-consciousness used by people of color to protect themselves from racism and discrimination; Dixon et al., 2023) can cause conspiratorial or paranoid-seeming beliefs. Mental health professionals can misinterpret this presentation as psychotic, leading to an overdiagnosis of psychotic disorders in Black American populations (Whaley, 2002). Although limited research has examined this overdiagnosis in legal settings, FMHPs may also misattribute this cultural mistrust as delusions or paranoia (Dixon et al., 2023), and some studies found higher rates of conspiracy endorsement among Black defendants (Paradis et al., 2018; Parker, 2014). This misattribution can have significant implications for the fair and just treatment of individuals within the legal system, potentially leading to inappropriate interventions or unjust outcomes.
Differentiating Delusional Beliefs From Conspiratorial Beliefs
For several reasons, it can be challenging to differentiate delusions secondary to a psychotic disorder from conspiratorial thinking; however, differences exist (Cunningham, 2018; Joshi et al., 2006; Starcevic & Brakoulias, 2021). Cunningham (2018) developed a structured professional judgment tool to help guide clinicians when differentiating delusions from extreme beliefs. In his MADDD-or-Rad-17 model, Cunningham highlights essential aspects to consider, such as focusing on the content of the belief, considering whether it is shared, evaluating how the public would view the belief, addressing the individual’s level of distress, and more.
In contrast to delusions, conspiracy beliefs are shared within a culture or subculture (Cunningham, 2018). Conspiracies are often derived from social motives, such as the need for social identification and a positive self-image (K. M. Douglas et al., 2019). Conspiracies are learned from others (rather than organically derived) and are usually shared with similar-minded people to receive validation (Starcevic & Brakoulias, 2021), whereas delusions come from within the individual and are often directly related to that individual (Pierre, 2021). Although delusions can be shared in some cases (i.e., shared psychotic disorder), this typically only occurs among family members or individuals with close emotional ties (Al Saif & Al Khalili, 2022).
In addition to social influences, the content and style of the belief are important. For instance, while conspiratorial beliefs can sometimes be plausible and argued using actual events, the reasoning behind delusional beliefs is often highly implausible (Starcevic & Brakoulias, 2021). Individuals with delusions also display high rigidity and psychological distress related to their beliefs, unlike those who believe in conspiracies (Bortolotti et al., 2021; Starcevic & Brakoulias, 2021). Although diagnostic criteria of delusional disorder does not include impaired functioning (APA, 2022), functional impairments may arise from distress and actions taken in response to delusional beliefs (Bortolotti et al., 2021; Cunningham, 2018; Starcevic & Brakoulias, 2021). Nonetheless, the lower impairment associated with delusional disorder can increase the challenge in differentiating between beliefs based in delusion versus conspiracy.
The Present Study
Limited studies have outlined the differences between delusional and conspiratorial beliefs (e.g., Cunningham, 2018; Joshi et al., 2006; Pierre, 2019; Starcevic & Brakoulias, 2021); however, there is a gap in the literature concerning how FMHPs distinguish these beliefs in legal settings. Although Rahman et al. (2020) found that psychiatrists could differentiate between delusions, extreme overvalued beliefs, and obsessions, their vignettes depicting delusions included other psychotic symptoms. For delusional disorder, the absence of other psychotic symptoms may increase the challenge of differentiating between delusions and extreme beliefs.
Given the importance of accurately assessing the presence of mental disorders in forensic settings, it is essential to examine how FMHPs differentiate delusional beliefs from conspiracies in the absence of other psychotic symptoms. Therefore, this study explored the factors that influenced FMHPs’ differentiation of delusional beliefs and conspiratorial beliefs in the context of competency to proceed. This mixed-methods study consisted of an online survey with an experimental vignette and had three objectives. First, we aimed to examine how race, the social context of the belief (i.e., whether it is shared within a group or idiosyncratic), and rigidity and distress impact FMHPs’ diagnosis and competency evaluations and had two hypotheses:
Other aspects of the study were exploratory and guided by the following research questions:
Method
Participants
A total of 278 participants were recruited via psychology and psychiatry association mailing lists and listservs, social media, and snowball sampling. Individuals were eligible to participate in this study if they were (a) licensed psychologists or psychiatrists, (b) working in the field of forensic mental health services, and (c) currently practicing in Canada or the United States. In sum, 17 participants did not meet these inclusion criteria and were excluded from analyses. Another 17 participants accessed the link but did not answer any survey questions, 18 did not pass the bot screening security feature (i.e., CAPTCHA or Completely Automated Public Turing test to tell Computers and Humans Apart task), and 28 exited the survey before reaching the vignette or completing the manipulation checks.
This left a final sample of 198 participants, which consisted of 165 (83.3%) psychologists and 33 psychiatrists (16.7%), with most practicing in the United States (psychologists: n = 141; psychiatrists: n = 27) in comparison to Canada (psychologists: n = 24; psychiatrists: n = 6). Respondents were between 24 and 77 years old (n = 186, M = 39.3, SD = 12.0) and 112 (59.6%) identified as women, 73 (38.8%) as men, and 1.6% preferred not to report their gender. Most participants identified as White (n = 144, 76.2%), and fewer identified as Latin American (n = 14, 7.4%), Black (n = 10, 5.3%), Asian (n = 6, 3.2%), another ethnicity (i.e., Native Hawaiian or other Pacific Islander, mixed background, Native American; n = 9, 4.8%), or preferred not to answer (n = 6, 3.2%). Participants also indicated the types of psycho-legal evaluations they completed within the past 24 months and their primary practice settings (see Supplementary Table 1, available in the online version of this article).
Procedure and Stimulus Materials
Participants were recruited using several psychology and law listservs and membership lists, including the American Psychology-Law Society mailing list, the Canadian Psychological Association Justice Stream mailing list, the International Association of Forensic Mental Health Services mailing list, the Women and Nonbinary Forensic Mental Health listserv, and the PsyLawList listserv. Participants were also recruited using convenience and snowball sampling through postings on social media (i.e., X/Twitter and Facebook) and emails to colleagues. They were also encouraged to enter a draw to win one of the five US$100 Amazon gift cards. This study received approval from the Research Ethics Board at the University of Manitoba, and data were collected between October 3, 2022, and December 1, 2022. Deidentified data and study materials can be made available by emailing the corresponding author. This study was not preregistered.
This study was administered online using Qualtrics and included a vignette with three independent variables with two levels each, creating a 2 (race: Black or White) × 2 (social context of the belief: independent or idiosyncratic) × 2 (rigidity/distress: high or low/moderate) factorial design. Participants were randomly assigned one of the eight vignette variations. Two manipulation check questions were added to ensure participant understanding and attention. Briefly, the vignette portrayed the situation of a 42-year-old man, Mr. Smith, who was arrested on a charge of harassment (see Supplementary Materials, available in the online version of this article). Mr. Smith’s competency to proceed was raised by his defense attorney due to his seemingly odd beliefs, including that he was being “gang stalked.” Given the prevalence of substance use among defendants referred for CST evaluations (Tansey et al., 2022) and to increase the ecological validity and typical complexity observed in CST cases, Mr. Smith was noted to have a significant history of methamphetamine use. However, to avoid participants attributing his symptoms solely to his methamphetamine usage, we specified that Mr. Smith had refrained from substance use for the past 2 months. This vignette was reviewed by several forensic psychologists to ensure it depicted an accurate case and the study was piloted with 15 advanced doctoral graduate students in the United States and Canada.
Manipulations
The first independent variable manipulated in the vignette was race; Mr. Smith was either described as White or Black. In manipulating the social context of the belief, Mr. Smith’s endorsement varied between shared beliefs among a group and idiosyncratic beliefs. We integrated multiple factors of Cunningham’s (2018) model pertaining to the social dimension of beliefs to ensure comprehensive coverage. This encompassed the origin of the belief (whether from a social cause or idiosyncratically) and its communal or individualistic nature. This holistic approach reflects the nuanced social/antisocial dynamics inherent in differentiating delusions from conspiracies, as emphasized in the literature (Cunningham, 2018; K. M. Douglas et al., 2019; Pierre, 2019; Starcevic & Brakoulias, 2021). In the shared beliefs manipulation, Mr. Smith learned about gang stalking on Reddit and spent a great deal of time discussing his beliefs with other targeted individuals. He reported being gang stalked by law enforcement officers and corrections officers. In the idiosyncrasy manipulation, Mr. Smith reported that his beliefs started when he noticed that a neighbor had installed a doorbell camera on their home to monitor Mr. Smith’s comings and goings. He believed his neighbors, family, and co-workers were engaged in gang stalking against him and had reduced contact with these individuals as a result.
Furthermore, the rigidity of Mr. Smith’s belief and his level of distress were manipulated. Psychotic delusions often involve an inability to entertain alternative explanations and highly rigid delusional beliefs are correlated with high levels of distress (Starcevic & Brakoulias, 2021). Hence, we integrated the closely linked factors of rigidity and distress to depict prototypical cases of delusional or conspiratorial beliefs and to present a realistic clinical portrayal. In the high rigidity/distress condition, Mr. Smith reported high levels of concern and distress, appeared agitated, and was certain that others were monitoring him. In the low/moderate rigidity/distress condition, Mr. Smith believed it was possible that others were not monitoring him, he reported a moderate level of concern and distress, and his affect and mood were euthymic.
Dependent Measures
Participants were asked to provide a diagnosis or a nondiagnostic identification for Mr. Smith and rated their confidence in their diagnosis from 0% to 100%. Participants were presented with predetermined response options which included common diagnoses with symptoms of delusions (i.e., schizophrenia, delusional disorder, substance-induced psychotic disorder, schizotypal personality disorder) and nondiagnostic possibilities that could lead to extreme beliefs (i.e., belief in a conspiracy theory or reality-based concerns caused by racial injustice). A follow-up question included a write-in option to allow participants to provide a diagnosis other than the pre-set options provided. If participants selected that they were trained in CST evaluations, they were also asked If the individual demonstrated a factual understanding of the proceedings against him (e.g., his charges, the allegations against him, courtroom procedures and participants, available pleas, plea bargaining process, etc.), correctly identified his attorney and reported a positive and trusting relationship with his attorney, would you likely opine this person competent or incompetent to stand trial?
This question included key elements of CST trial specified by American and Canadian law (Criminal Code of Canada, 1992; Dusky v. United States, 1960). Participants rated their confidence in their CST opinion from 0% to 100%.
Exploratory Questions
A series of exploratory open- and closed-ended questions were included to examine which factors FMHPs consider while differentiating delusions from conspiracies and to outline the training they received to make this differentiation. We also asked participants to select up to three factors they commonly consider when distinguishing delusions from conspiracies based on Cunningham’s (2018) model. Finally, participants were asked to explain how they differentiate delusions from conspiratorial beliefs in their practice and responses were qualitatively examined.
Data Analysis
Quantitative Analysis
Analytical strategies included descriptive statistics used to understand the study sample and the frequency of each diagnosis and competency decision. Chi-square analyses were used to evaluate participants’ performance on the manipulation check questions, and confidence in diagnosis and competency decisions were analyzed using independent t-tests. To answer our hypotheses, chi-square analyses and a binominal logistic regression were used to examine the effects of the independent variables on diagnosis and competency evaluations. Fisher’s exact test was used for chi-squares with expected counts of less than five per cell. For a binominal logistic regression with three predictors (race, social context of the belief, and rigidity/distress), results of a G*Power analysis (Faul et al., 2007) indicated that 77 participants were needed to generate a power of .80 (α = .05) to detect an effect size of .15 or larger. All assumptions were checked prior to data analysis. For a binominal logistic regression with uneven counts in the dependent variable categories, it is recommended to have a minimum of 10 counts per predictor in each dependent variable category (Long, 1997; Peduzzi et al., 1996). Therefore, our dependent variable categories were required to have a minimum count of 30 cases each.
Qualitative Analysis
Braun and Clarke’s (2006, 2019) step-by-step reflexive thematic analysis guided this study’s inductive exploratory qualitative data analysis. This approach involves six steps: (a) becoming familiar with the data by reading it thoroughly and noting initial ideas, (b) creating initial codes from the data, (c) creating themes based on the initial codes, (d) reviewing the themes and generating a thematic “map,” (e) defining and naming the themes generated, and (f) producing the report and relating the analysis back to the research questions and the literature. The first author followed this process and thoughtfully engaged with the responses and created initial codes from common answers. The first author then created themes based on information that reflected patterned responses and meaning and that related to factors considered by FMHPs when differentiating delusional beliefs from conspiratorial beliefs. Interrater reliability was conducted by the first author and an undergraduate-level research assistant using Dedoose (Dedoose Version 9.0.62, 2022), a web application that facilitates interrater coding and reliability. Themes were collapsed and joined through this process to improve clarity and reduce the overlap between initial subthemes. Cohen’s kappa, k = .81, indicated very good agreement.
Results
Manipulation Checks
Two multiple-choice manipulation check questions were presented following diagnosis/identification and competency opinions to ensure that participants understood and recalled the vignette’s information. For the first manipulation check, 73.3% (n = 74) of participants in the shared beliefs condition correctly recalled that the defendant believed that law enforcement and corrections officers were engaged in gang stalking against him, and 75% (n = 72) of participants in the idiosyncratic condition correctly identified that his family, neighbors, and friends engaged in gang stalking against him, χ2(2, N = 197) = 98.2, p < .001, V = .71. For the second manipulation check, 77.3% (n = 75) of participants correctly recalled the defendant’s race when he was Black, and 74.2% (n = 72) correctly identified his race when he was White, χ2(2, N = 194) = 75.85, p < .001, V = .63. We excluded 79 participants who failed or did not answer one or both manipulation check questions from the analyses examining the vignette manipulations’ effects on the dependent variables; however, these participants were retained for exploratory and qualitative analyses. Therefore, the analyses examining the independent variables effects on the dependent variables included 119 of the 198 (60.1%) responses.
Diagnosis and Conspiracy Theory Identification
The most frequently selected diagnoses were substance/medication-induced psychotic disorder (n = 40, 33.9%) and delusional disorder (n = 39, 33.1%). Other less commonly assigned diagnoses included schizophrenia (n = 4, 3.4%) and schizotypal personality disorder (n = 2, 1.7%). In lieu of identifying the defendant with a psychiatric disorder, 26.3% (n = 31) participants indicated the defendant was expressing beliefs based in a conspiracy theory and 1.7% (n = 2) indicated that the defendant was exhibiting reality-based concerns caused by racial injustice. A Fisher’s exact test indicated that there were no significant differences in the diagnoses and identification of conspiracy theories between psychologists and psychiatrists, p = .508. Furthermore, there were no significant differences in the diagnoses and conspiracy theory identifications of American and Canadian participants, χ2(1, N = 114) = 1.97, p = .160, Φ = .13.
Sixty-seven participants (57.3%) chose to provide an alternative diagnosis in a write-in option and 13 of these participants provided other diagnoses than those listed. These included unspecified schizophrenia spectrum disorder and other psychotic disorder or other specified schizophrenia and other psychotic disorder (n = 8, 12%), bipolar disorder (n = 2, 3%), paranoid personality disorder (n = 1, 1.5%), schizoaffective disorder (n = 1, 1.5%), trauma or stress-related disorder (n = 1, 1.5%), and possible malingering (n = 1, 1.5%).
Hypothesis 1: Social Context of the Belief
We hypothesized that participants would be more likely to diagnose Mr. Smith with a psychotic disorder when his belief was idiosyncratic and more likely to attribute his belief to a conspiracy theory when it was shared. As predicted, significantly more participants in the shared condition identified Mr. Smith’s beliefs as originating from a conspiracy theory (n = 21, 35.6%) compared with participants in the idiosyncratic condition (n = 10, 16.9%), χ2(1, N = 118) = 5.29, p = .021, Φ = .21. Conversely, participants in the idiosyncratic condition diagnosed Mr. Smith with a psychotic disorder (n = 46, 78%) at a higher rate than those in the shared condition (n = 37, 62.7%), but this difference was not significant, χ2(1, N = 118) = 3.29, p = .070, Φ = .16.
A binominal logistic regression was used to test if race, the social context of the belief (i.e., whether the belief was shared or idiosyncratic), and the rigidity/distress of the belief significantly predicted the diagnosis of a psychotic disorder or a conspiracy theory identification. For this analysis, all psychotic disorder diagnoses (i.e., delusional disorder, schizophrenia, and substance-induced psychotic disorder) were combined and compared against the identification of a conspiracy theory; this excluded five responses that did not fit either of these categories (i.e., schizotypal personality disorder and reality-based concerns due to racial injustice). The model was significant, χ2(3, N = 114) = 13.66, p = .003 (See Table 1). This model explained 16.4% (Nagelkerke R2) of the variance of the dependent variable and correctly identified 75.4% of cases. As shown in Table 1, the social context significantly contributed to the model. Therefore, when Mr. Smith’s beliefs were idiosyncratic, participants were 2.92 times more likely to identify his belief as a symptom of a psychotic disorder than as emerging from a conspiracy theory.
Independent Variables’ Effect on the Diagnosis of a Psychotic Disorder or Conspiracy Theory Identification
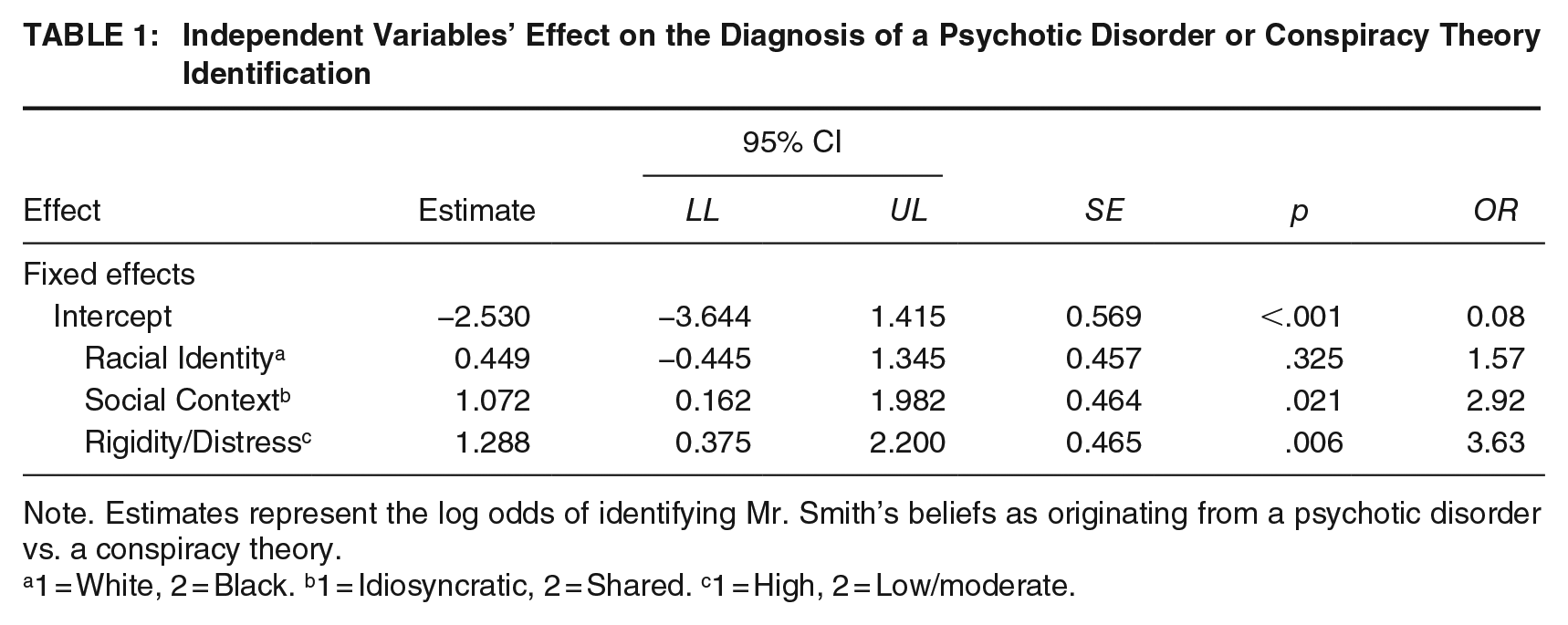
Note. Estimates represent the log odds of identifying Mr. Smith’s beliefs as originating from a psychotic disorder vs. a conspiracy theory.
1 = White, 2 = Black. b1 = Idiosyncratic, 2 = Shared. c1 = High, 2 = Low/moderate.
Hypothesis 2: Rigidity and Distress
We also hypothesized that participants would be significantly more likely to diagnose Mr. Smith with a psychotic disorder when he displayed high rigidity and distress and significantly more likely to attribute his belief to a conspiracy theory when he displayed lower rigidity and distress. In line with our prediction, distress/rigidity of the belief had a significant effect on the diagnosis of a psychotic disorder and on the identification of a conspiracy theory. More participants in the high rigidity/distress condition (n = 50, 82%) diagnosed Mr. Smith with a psychotic disorder than those in the low/moderate condition (n = 33, 57.9%), χ2(1, N = 118) = 8.18, p = .004, Φ = .26. In contrast, more participants in the low/moderate condition (n = 21, 36.8%) attributed Mr. Smith’s beliefs to a conspiracy theory than those in the high rigidity/distress condition (n = 10, 16.4%), χ2(1, N = 118) = 6.36, p = .012, Φ = .23.
The binominal logistic regression conducted with race, social context and rigidity/distress also displayed a significant effect of rigidity and distress. When Mr. Smith was high in rigidity and distress, participants were 3.63 times more likely to identify his belief as a symptom of a psychotic disorder rather than a conspiratorial belief, supporting our hypothesis.
Defendant’s Racial Identity
We also examined whether Mr. Smith’s race would impact the participants’ diagnostic decisions. Participants in the condition with a Black defendant attributed Mr. Smith’s beliefs to a psychotic disorder (n = 43, 69.4%) at similar rates to participants in the condition with a White defendant (n = 40, 71.4%), χ2(1, N = 118) = 0.06, p = .805, Φ = .02. Similar results were found between race and conspiracy theory identification, χ2(1, N = 118) = 0.514, p = .473, Φ = 0.07; participants who viewed the vignette with the Black defendant attributed Mr. Smith’s beliefs to a conspiracy at similar rates compared with those viewed the vignette with the White defendant (Black defendant condition: n = 18, 29%; White defendant condition: n = 13, 23.2%). Further, race did not significantly contribute to the logistic regression model. These results indicate that the defendant’s race did not influence participants’ diagnoses.
Confidence in Diagnoses and Conspiracy Identification
We used independent samples t-tests to examine differences in confidence levels of diagnosis and identification provided (see Supplementary Table 2, available in the online version of this article). Confidence in diagnosis ranged from 0% to 97% and averaged 54.5% (SD = 20.0%). There were no significant difference in participants’ level of confidence between those who attributed Mr. Smith’s beliefs to a psychotic disorder (M = 53.3%, SD = 18.0%) and those who attributed his beliefs to a conspiracy theory (M = 59.4%, SD = 22.8%), t(111) = 1.47, p = .145, d = 0.31. There were also no significant differences in participants’ level of confidence in their diagnosis between the conditions of the independent variables for race, Black defendant (M = 53.7%, SD = 20.2%) and White defendant (M = 55.3%, SD =19.9%), t(116)= −0.43, p = .667, d = -0.08; and rigidity/distress, low/moderate (M = 52.6%, SD = 20.5%) and high (M = 56.3%, SD = 19.5%), t(116)= 1.00, p = .320, d = 0.18. However, significant results arose when examining the social context of the belief. Participants in the shared condition were significantly more confident in their diagnosis (M = 58.6%, SD = 18.1%) compared with those in the idiosyncratic condition (M = 50.5%, SD = 21.1%), t(116)= 2.25, p = .026, d = 0.41.
No significant differences were found in confidence levels between participants’ professions (psychologists: M = 54.0%, SD = 20.7, psychiatrists: M = 58.5%, SD = 12.7, t[116]= 0.73, p = .466, d = 0.22) and countries (United States: M = 54.5%, SD = 19.8, Canada: M = 54.5%, SD = 21.4; t[116]= 0.00, p = .998, d = 4.98e−4). However, participants who believed they had received sufficient training to differentiate delusional beliefs from conspiratorial beliefs were more confident in their diagnosis (M = 59.2%, SD = 19.1) than those who did not believe they had received sufficient training (M = 48.5%, SD = 19.7), t(114) = 2.94, p =.004, d = 0.55.
CST Opinions
We conducted exploratory analyses to examine whether the defendants’ race, the social context of their belief, and their rigidity/distress would influence CST opinions. Most psychiatrists (n = 9, 75%) and psychologists (n = 86, 80.4%) who passed the manipulation check questions were qualified to complete CST evaluations. A Fisher’s exact test revealed that there were no significant differences in the number of psychologists versus psychiatrists that were qualified to complete CST evaluations, p = .706. Psychologists trained in CST evaluations completed these evaluations, on average, 57.4% (SD = 30.6) of the time in their role, ranging from 1% to 100%. Psychiatrists who indicated they were qualified to conduct CST evaluations reported that they spent 39.4% (SD = 20.4, minimum = 10%, maximum = 60%) of the time in their role completing these evaluations. Only 42.1% of Canadian participants were qualified to complete CST evaluations (psychologists: n = 5, psychiatrists: n = 3), compared with 87% of Americans (psychologists: n = 81, psychiatrists: n = 6), χ2(1, N = 119) = 19.99, p <.001, Φ = .41. Of those qualified to complete CST evaluations, 74.7% (n = 63 psychologists, n = 8 psychiatrists) responded that they would consider the defendant competent to stand trial.
Chi-square analyses revealed that the rate at which participants indicated they believed that Mr. Smith would be competent to stand trial was unaffected by the independent variables’ manipulations of race: χ2(1, N = 95) = 0.29, p = .590, Φ = .06, and of the social context of the belief: χ2(1, N = 95) = 0.03, p = .862, Φ = .02. However, participants were more likely to believe that the defendant would be incompetent to stand trial when the rigidity/distress was high (n = 18, 75%) and more likely to believe that the defendant would be competent when the rigidity/distress was low/moderate (n = 38, 53.5%), χ2 (1, N = 95) = 5.87, p = .015, Φ = .25.
We also examined differences in participants’ level of confidence in their CST opinions in each of the independent variable conditions (see Supplementary Table 3, available in the online version of this article). Confidence levels ranged from 10% to 100% and averaged 67.8% (SD = 22.6). Participants’ overall lower levels of confidence may reflect the limited information provided in the vignette.
Results from independent t-tests displayed no significant differences in participants’ level of confidence in their competency opinions when manipulating the defendant’s race, social context, or rigidity/distress (see Supplementary Table 3). There were no significant differences in confidence levels between professions, psychologists: M = 67.1%, SD = 22.7, psychiatrists: M = 75.2%, SD = 20.8; t(92) = 1.03, p = .305, d = 0.36, or between those who reported receiving sufficient training to differentiate delusions from conspiracies (M = 69.9%, SD = 20.3) and those who did not (M = 64.8%, SD = 25.8), t(92) = 1.07, p = .144, d = 0.19. However, Canadians reported significantly higher confidence levels in their competency opinions (M = 87.8%, SD = 20.0) than Americans (M = 66.0%, SD = 22.0), t(92) = 2.71, p = .004, d = 1.00.
Conspiracy Theories—Frequency Analysis
The most common conspiracy theories participants identified in their own field of work were gang stalking (n = 115, 58.1%) and sovereign citizens movement (n = 95, 48.0%). Havana syndrome (n = 35, 17.7%) and MK Ultra (n = 30, 15.2%) conspiracies were less common, but still prevalent. Thirty participants (15.2%) provided additional conspiracy theories than those listed, including QAnon, COVID-19, Illuminati, Freemasons, and police corruption or government surveillance. Five participants (2.5%) stated that they had not seen any conspiracy theories in their practice. Gang stalking was the most reported conspiracy by both Canadian and American participants (American: n = 98, 58.3%; Canadian: n = 17, 56.7%) and sovereign citizens conspiracies were encountered more frequently by Americans (n = 88, 52.4%) compared with Canadians (n = 7, 23.3%), χ2(1, N = 198) = 8.61, p = .003, Φ = .21. Canadians encountered Havana syndrome conspiracies more frequently (n = 8, 26.7%) than Americans (n = 27, 16.1%), but this difference was not significant, χ2(1, N = 198) = 1.96, p = .161, Φ =.10.
Training and Cunningham’s Factors
Although most participants believed they had received sufficient training to differentiate delusions from conspiracy theories (n = 121, 62.4%), 73 participants (37.6%) reported self-perceived insufficient training. No significant difference was found between Canadian (n = 17, 60.7%) and American (n = 104, 62.7%) participants who believed they had received sufficient training, χ2(1, N = 194) = 0.04, p = .845, Φ = .01, or between psychologists (n = 103, 63.6%) and psychiatrists (n = 18, 56.3%), χ2(1, N = 194) = 0.61, p = .434, Φ = .06. Many participants reported receiving this training from workshops or training (n = 125, 63.1%), consultations (n = 113, 57.1%), research (n = 85, 42.9%), and doctoral coursework (n = 61, 30.1%). Some indicated that they received this training from other sources (n = 13, 6.6%), which included supervised clinical training, fellowships and internships, clinical experience, reading the literature, and attending workshops with Dr. Mark Cunningham. Few participants indicated that they had not received any training to differentiate delusions from conspiracy theories (n = 14, 7.1%).
Participants selected up to three factors they most considered when distinguishing delusions from conspiracies based on Cunningham’s MADDD-or-Rad-17 model’s seven primary arenas of analysis (see Supplementary Table 4, available in the online version of this article). The most endorsed factor was assessing the cognitive style of the belief (n = 98, 49.5%), followed by the social influences (n = 87, 43.9%) and behavioral/action factors (n = 81, 40.9%). Less commonly endorsed factors included assessing the social inclusion of the individual (n = 74, 37.4%), the individual’s distress and social dysfunction (n = 68, 34.3%), the content of the belief (n = 66, 33.3%), and prodromal symptomology (n = 49, 24.7%). Nine participants (4.5%) provided factors other than those listed, such as determining if the belief is compartmentalized or shared with family members or close friends, the function of the belief, and examining for history of substance abuse.
Open-Ended Responses
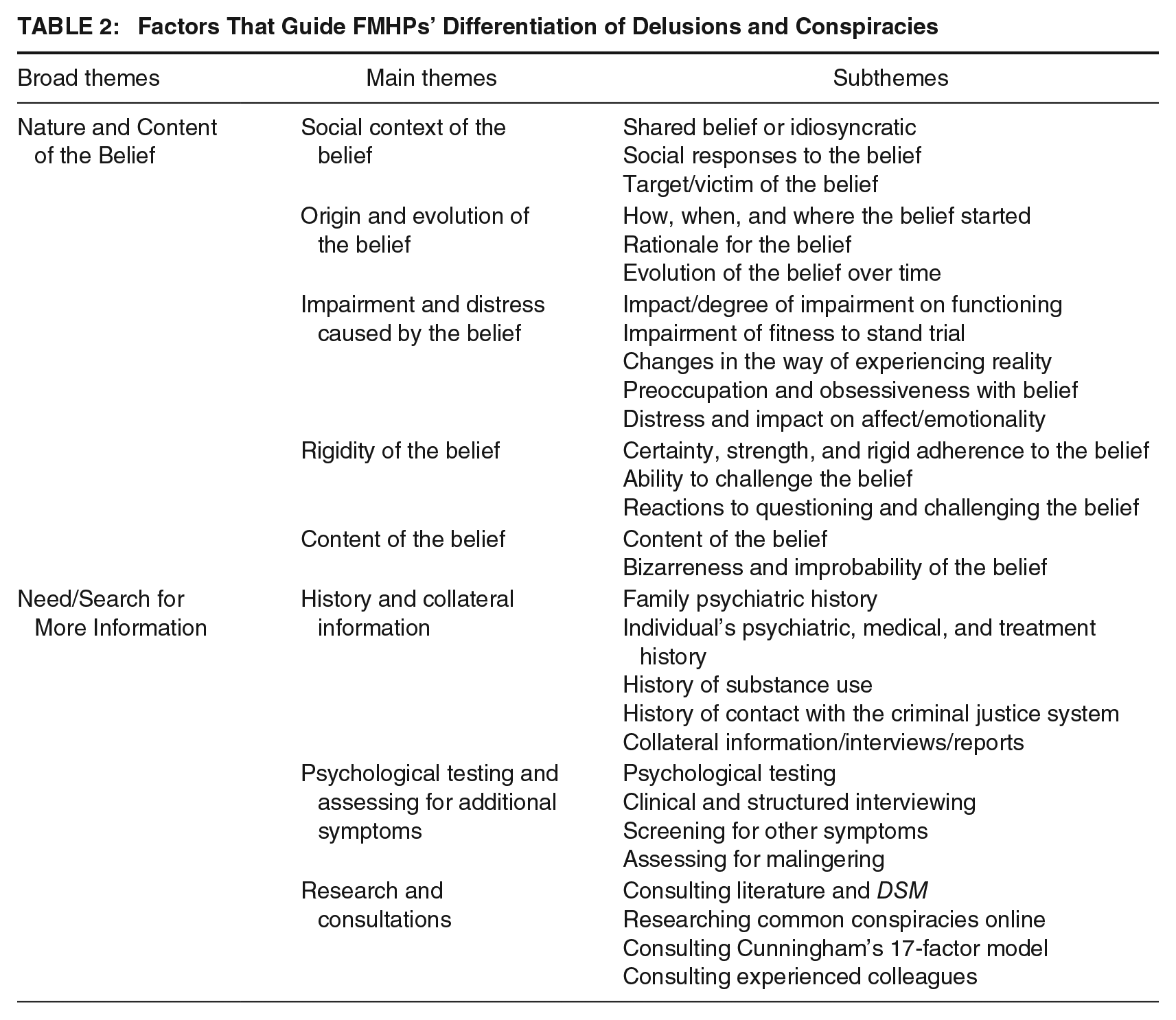
Two broad themes emerged from the exploratory thematic analysis of the 129 responses, “Nature and Content of the Belief” and “Need/Search for Additional Information.” “Nature and Content of the Belief” included the main themes of “social context of the belief,” “origin and evolution of the belief,” “impairment and distress caused by the belief,” “rigidity of the belief,” and “content of the belief.” The second broad theme, “Need/Search for Additional Information,” included “history and collateral information,” “psychological testing and assessing for additional symptoms,” and “research consultations” (see Table 2).
Factors That Guide FMHPs’ Differentiation of Delusions and Conspiracies
Nature and Content of the Belief
Social context of the belief
Participants reported considering whether the belief was socially derived or whether it was idiosyncratic. Participants stated that they would collect information to address if the belief was shared within a group, culturally informed, or unique to the individual. As one participant explained, “If the belief is shared by a sufficient number of others as to be culturally acceptable in some regard, it is no longer a delusion, even if the belief falls well outside the mainstream. . .” Participants also highlighted the importance of determining the target of the belief, specifying that the target of a delusion would only be the individual themself. In contrast, conspiracy theories often include numerous targets. Participants also mentioned assessing the social responses to the individual’s belief, such as whether the belief is reinforced and validated by others and how loved ones react to the individual’s belief.
Origin and evolution of the belief
Participants emphasized the importance of determining the origins of the belief, specifically how it started, when it started, and where it started. They also mentioned trying to understand the reasoning, rationale, and evidence the individual presents to justify the belief and determining how reasonable this evidence is. Others mentioned evaluating whether the belief may have reality-based components, which can help differentiate conspiracies and delusions from entirely reality-based concerns. One participant stated: “I have had defendant’s whose lawyers state that they are delusional and [I have] found evidence that their statements were true and not psychotic or a conspiracy.” Another vital factor was determining how the belief changed and progressed; some participants explained that changes in the belief over time might indicate a conspiracy theory.
Impairment and distress caused by the belief
Functional impairment included impairments that affected daily functioning, behaviors and emotions, social and family relationships, occupation, and decision-making. Significant distress, the effect on emotionality, and the level of preoccupation and obsession with the belief were also commonly emphasized. Participants also mentioned evaluating the individual’s ability to reality-test and explained how this could help differentiate conspiratorial thinking and delusional beliefs: Their delusional thinking affects a significant portion of their grasp of reality and can negatively affect such spheres of functioning as occupational, social and familial . . . Conversely, those who entertain conspiracy theories are able to maintain most spheres of functioning despite entertaining beliefs in a conspiracy.
Rigidity of the belief
Participants indicated evaluating the belief’s strength and intensity and how confident individuals are in their belief. This included determining how resistant the belief is to contradicting evidence and whether the individual can consider other explanations for their experiences. While conspiracy theories can be resistant to conflicting evidence, some participants explained the clear differences between conspiratorial beliefs and delusional beliefs: It depends on how strongly the individual holds the belief. For example, are they willing to consider alternative explanations for it, or is it a rigidly held belief that stays fixed despite tangible evidence to refute it. In my experience, delusional beliefs stay present no matter what evidence there is to the contrary.
Content of the belief
In terms of content, participants mentioned examining what is believed, whether it is bizarre, and the plausibility of the belief. However, as one participant stated, conspiracies and delusions may resemble each other in the degree of believability: Paranoia and conspiracy theories can be in the realm of believable (e.g., the police are following him and harassing him because of his history with the police/in jail) to less believable (e.g., the police set him up to be arrested), to outlandish (e.g., the CIA is implanting neuralinks).
Need/Search for Additional Information
History and collateral information
Gathering as much collateral information as possible from third parties such as families, friends, neighbors, or others was commonly expressed by participants. Participants mentioned collecting information about the individual’s psychiatric, medical, and treatment history, their family’s psychiatric history, and determining substance use history. Specifically, in the legal context, participants mentioned that gathering information about past imprisonment and competency evaluations could provide relevant information.
Psychological testing and assessing for additional symptoms
Participants reported using psychological tests and assessment tools, such as the Personality Assessment Inventory (PAI; Morey, 2007) and Millon Clinical Multiaxial Inventory (MCMI; Millon et al., 2015), or structured clinical interviewing to gather more information about the beliefs. Participants also stated that they would assess for additional symptoms that could be characteristic of psychotic disorders, “The presence of additional psychotic symptoms in addition to the unusual beliefs (e.g., hallucinations, disorganized speech or behavior, negative symptoms) is helpful in differential diagnosis.” Three participants mentioned considering the possibility of malingering or symptom exaggeration when assessing delusional beliefs in legal settings.
Research and consultations
Participants reported consulting resources such as Cunningham’s (2018) 17-factor model and the DSM criteria when making this differentiation. Furthermore, participants mentioned consulting experienced colleagues, reviewing literature about conspiracy theories and delusional beliefs, and researching common conspiracies or the individual’s specific beliefs online to see if they are consistent with current conspiracy theories.
I try to keep informed about recent overly valued beliefs shared by groups, such as sovereign citizen and gang stalking, to be familiar with those typical beliefs. I do this by reading articles as well as reading about such groups online, to see what recent views are about such groups, as conspiracies seem to be growing and changing by the day.
Discussion
Extreme radicalized beliefs, such as strong endorsement of conspiracy theories, may closely resemble delusional beliefs, causing issues around diagnosis in CST and other forensic evaluations. Consistent with our hypothesis, results of this study suggested that the social context (i.e., whether it is shared or idiosyncratic) and the rigidity and distress (i.e., low/moderate or high) of the belief influenced how FMHPs differentiated delusions from conspiratorial beliefs. Contrary to some existing literature, the race of the defendant did not influence the participants’ ability to make this differentiation. Further confirmation of the importance of these factors was found through qualitative analysis, in which many participants also mentioned the social context and rigidity of the belief when describing how they typically differentiated delusions from conspiracy theories. In addition, participants considered the origin of the belief and its evolution, the level of impairment and distress caused by the individual’s belief, and the content of the belief. Participants also indicated gathering additional information and records to assist them with this determination, including collecting historical and collateral information, using psychological tests, reviewing relevant literature, and consulting colleagues.
Results from this study are consistent with the literature suggesting that clinicians conceptualize delusions as idiosyncratic, whereas conspiracies are thought to be shared among a group (Cunningham, 2018; K. M. Douglas et al., 2019; Pierre, 2021; Starcevic & Brakoulias, 2021). In their qualitative responses, participants reported determining the target(s) of the delusion; this is supported by findings indicating that delusions originate from the individual and that this individual is typically the sole target or victim of the delusion (Pierre, 2021; Starcevic & Brakoulias, 2021). Furthermore, in the case of multiple targets, considering the relationship between targets is important to evaluate the probability of shared delusional belief, which typically occurs among individuals with close emotional ties (Al Saif & Al Khalili, 2022; Joshi et al., 2006). Participants were more likely to attribute Mr. Smith’s beliefs to a delusion when his beliefs were highly rigid, suggesting that participants understood that individuals with delusions often cannot articulate disconfirming evidence for their beliefs, have difficulty considering alternative hypotheses, and often display irritability or agitation when their beliefs are challenged (Cunningham, 2018). Participants also reported evaluating other factors such as functional impairment, reasoning or rationale for the belief, plausibility of the belief, distress, and the evolution of the belief over time, factors that are all present in the existing literature (Bortolotti et al., 2021; Kiran & Chaudhury, 2009; Pierre, 2021; Starcevic & Brakoulias, 2021).
In our examination of functional impairments associated with delusional beliefs, participants emphasized the negative consequences on social functioning. Although the endorsement of conspiratorial beliefs can also be detrimental to interpersonal relationships (van Prooijen et al., 2022), conspiracies are shared among groups. Therefore, research comparing conspiracies and delusions tends to focus on the isolating nature of delusions and the communal aspect of conspiracy theories (Bortolotti et al., 2021; Starcevic & Brakoulias, 2021), potentially elucidating why participants primarily observed social impairments among delusions. This reflects the complexity of differentiating delusions and conspiracies when delusional individuals display low functional impairments and distress. It may be harder to identify less distressing and impairing delusions given that these are key elements to many psychotic disorders (APA, 2022).
Although the literature suggests that a history of discrimination may be cause for higher levels of conspiratorial beliefs in Black Americans (Parker, 2014; Prasad, 2022; Simmons & Parsons, 2005; Whaley, 2002), participants were just as likely to attribute Mr. Smith’s belief to a conspiracy theory when his race was described as White compared with Black. The defendant’s race did not influence participants’ diagnostic impressions, possibly due to the increase in culturally focused training for both psychiatrists and psychologists (Benuto et al., 2019; Venkataramu et al., 2021). Instead, in their open-ended responses, participants mentioned considering the individual’s rationale, reasoning, and evidence for the belief. Research indicates that conspiratorial beliefs can sometimes be plausible and argued using actual events, whereas the evidence and explanations behind delusional beliefs are often highly implausible, unacceptable, and incorrigible (Kiran & Chaudhury, 2009; Starcevic & Brakoulias, 2021).
Participants also mentioned considering additional factors not included in the vignette and often referred to Cunningham’s (2018) MADDD-or-Rad-17 model. If the content of the belief resembled a conspiracy, many participants indicated that they would examine whether it differed from the conspiracy or included personalization. Participants also mentioned assessing the improbability and the bizarreness of the belief, consistent with Cunningham’s model. In the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; APA, 2000), bizarre delusions exceeded the criteria for delusional disorder; however, diagnostic changes in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) expanded the delusional disorder criteria to include bizarre delusions. Nonbizarre delusions can closely resemble conspiracies, making this distinction difficult (Cunningham, 2018); however, a bizarre belief may allow the evaluator to rule out conspiratorial beliefs, a factor several participants noted as important for their assessment.
Likely influenced by general best practices within forensic psychology and psychiatry, participants also indicated that they would gather collateral information and information on the individual’s history, research the beliefs online and in the literature, and conduct psychological testing and assess for other symptoms. Cunningham’s (2018) model includes prodromal symptomatology, and while additional symptoms may not be necessary for specific diagnoses (e.g., delusional disorder; APA, 2022), they may rule out the possibility of conspiratorial beliefs.
Most participants reported receiving sufficient training to differentiate delusional beliefs from conspiracy theories; however, some did not. Those who reported receiving sufficient training displayed higher confidence levels in their diagnosis than those who did not, indicating that training increases FMHPs’ confidence when making this diagnosis. Insufficient training in this area may lead to disagreements among FMHPs, which can be problematic in forensic settings (e.g., Parker, 2014). Therefore, there is a need to increase FMHP’s training in this area to improve the quality of these assessments and increase FMHP’s confidence in their evaluations.
The courts often rely on the expertise of FMHPs to provide information on the defendant’s mental state at the time of an offense (Gulayets, 2016). Both forensic psychologists and psychiatrists can complete these assessments in the United States (K. S. Douglas et al., 2012; Meyer & Gutheil, 2017). Only forensic psychiatrists can complete these evaluations in Canada (Gulayets, 2016); however, there is a growing recognition that psychologists are assisting with these reports or writing them as sole authors (Goldenson et al., 2023). No significant differences were found between psychiatrists and psychologists when diagnosing psychotic disorders or identifying conspiracy theories and they displayed similar confidence levels for their diagnoses and competency evaluations. These results indicate that forensic psychologists and psychiatrists differentiate delusional beliefs from conspiracy theories similarly and display similar levels of confidence in their differentiation. Furthermore, CST evaluations are generally only completed by forensic psychiatrists in Canada (Gulayets, 2016); as 80% of the Canadian sample (n = 24) were psychologists, this may explain why there were significantly more Americans trained in CST evaluations than Canadians. Formal education, training, and experience in forensic mental health is crucial to properly complete these evaluations (Sadoff & Dattilio, 2012). Results from this study showed that forensic psychologists trained in competency evaluations did not differ from forensic psychiatrists in their competency opinions, suggesting that forensic psychologists are equally competent as forensic psychiatrists in this area when receiving proper training.
Limitations
We want to acknowledge the methodological limitations of this study. First, although we aimed to recruit forensic psychologists and psychiatrists throughout the United States and Canada, this sample was overrepresented by forensic psychologists and Americans. This limited the analyses examining differences between these professions and countries. Moreover, although this study included individuals from diverse backgrounds, most participants identified as White women.
To ensure participant retention, the vignette was brief, which impacted its ecological validity. In addition, participants displayed low to moderate confidence ratings in their diagnoses and competency opinions, which may limit the generalizability of these results. Written vignettes may also be less effective than other forms of vignettes, such as recordings or actual redacted cases (Erfanian et al., 2020). Another limitation of our vignette lies in the decision to combine rigidity and distress into one manipulation to depict typical cases of delusional or conspiratorial beliefs. While this was intended to offer an accurate clinical representation, it may have introduced complexities into our manipulations. Moving forward, researchers should manipulate these factors independently to refine our understanding of their individual contributions.
We also presented pre-set options when asking participants to provide a diagnosis or identification for the defendant’s beliefs, which may have biased these responses. This decision was made based on pilot study results, in which participants often did not provide a diagnosis or identification for the belief when presented with a write-in option. The follow-up questions allowed participants to identify other disorders or causes for the defendant’s beliefs.
Future Research
This study aimed to explore how FMHPs differentiate delusions from conspiracies. However, this study only included three manipulations to ensure brevity of the vignette. Future research should examine if other factors (e.g., behavioral and action factors, grandiosity, psychological disorganization) influence FMHPs’ differentiation of delusional belief and conspiracy theories. Future research could also manipulate the relationships of those who share the belief to explore FMHPs’ ability to differentiate between shared psychotic disorder and conspiratorial beliefs. Finally, we presented conspiracies and delusional beliefs as a dichotomy; future research should explore whether FMHPs consider this issue as a dichotomy and whether they are able to identify complex situations in which both types of beliefs may be present.
Conclusion
Results from this study indicate that forensic mental health professionals consider similar factors when differentiating delusional beliefs from conspiratorial beliefs. The social context of the belief and its rigidity and distress influenced whether FMHPs attributed an individual’s beliefs to a psychotic disorder or a conspiracy theory. However, the individual’s race did not influence FMHPs’ diagnoses or competency decisions. Furthermore, this study found no significant differences between psychologists and psychiatrists in diagnosis, competency evaluations, or confidence scores. Although participants generally agreed and indicated similar factors when making this differentiation, many did not believe they had received sufficient training to make this differentiation, suggesting a need for more training in this area.
Supplemental Material
sj-docx-1-cjb-10.1177_00938548241262490 – Supplemental material for Delusion or Conspiracy? How Forensic Mental Health Professionals Differentiate Delusional Beliefs From Extreme Radicalized Beliefs
Supplemental material, sj-docx-1-cjb-10.1177_00938548241262490 for Delusion or Conspiracy? How Forensic Mental Health Professionals Differentiate Delusional Beliefs From Extreme Radicalized Beliefs by Katérine Aminot, Tara J. Ryan and Alicia Nijdam-Jones in Criminal Justice and Behavior
Footnotes
Authors’ Note:
We would like to thank William J. Newman for his assistance with recruiting participants and reviewing this manuscript. This article is based on an undergraduate research project by Katérine Aminot, for which Alicia Nijdam-Jones served as the research advisor. This work was partly supported by an AP-LS Undergraduate Student Grant-in-Aid from the American Psychology-Law Society and an Undergraduate Research Award from the University of Manitoba. A portion of these data was presented at the American Psychology-Law Society Conference, March 2023, Philadelphia, PA and at the Canadian Psychological Association 5th North American Correctional and Criminal Justice Psychology Conference, June 2023, Toronto, ON.