
Abstract
This article examines the role of mental health, substance use, and comorbidity in relation to time to reincarceration. Our study included all people released from provincial correctional facilities in British Columbia, Canada, from 2012 through 2014 (N = 13,109). Using data from a mental health screening tool, we examined the relationship between four diagnostic groups (mental health needs alone, substance use disorders alone, co-occurring disorders, and no disorders) and time to reincarceration over a 3-year follow-up period. We found that people with co-occurring disorders and substance use disorders were at substantially elevated risk of reincarceration compared with those with no disorders or mental health needs alone. Mental health needs alone was not significantly associated with reincarceration after adjusting for covariates. Correctional, health, and social services must work synergistically to improve health and criminal justice outcomes, particularly for people with substance use and co-occurring disorders.
A substantial body of evidence demonstrates that people with mental illness and substance use disorders are disproportionately represented in prisons (Al-Rousan et al., 2017; Butler et al., 2021; Chang, Larsson, et al., 2015; Fazel et al., 2016). Despite the high prevalence of mental health and substance use–related needs in this setting, disorders are frequently underdiagnosed and undertreated among people who experience incarceration (Fazel et al., 2016). Routine screening at intake to custody is considered best practice (Correctional Service Canada, 2012; National Institute for Health Care Excellence [NICE], 2017) and it provides an opportunity to identify people with unmet health needs, deliver treatment and support during incarceration, and plan for discharge. Unfortunately, there are limited options to divert people with mental health and substance use needs from custodial sentences into appropriate community-based or forensic care, as well as limited services in custody to prevent reoffending after release (Nicholls et al., 2018; Ogloff et al., 2004). Researchers in several jurisdictions have investigated whether psychiatric diagnoses are associated with repeat offending or recidivism (Baillargeon et al., 2010; Wilson et al., 2011, 2014), but strong conclusions are limited by variability in methods, including differences in measures, definitions of mental illness, and sampling approaches.
Recidivism, broadly defined as reengaging in criminal behavior after receiving a prior sanction or intervention, is typically measured by rearrest, incurring new charges, a reconviction, and/or return to prison (King & Elderbroom, 2014). Rates of recidivism are used worldwide as a measure of the effectiveness of criminal sanctions and offender management programs. Recidivism is common, as shown in a recent systematic review, including studies from 25 countries, which found that 2 years postconviction, the rate of rearrest is between 26% and 60% (Yukhnenko et al., 2019). A study found that 37% of those with a jail sentence of 6 or more months and 23% of those with a community sentence in Ontario, Canada, were reconvicted within 2 years (Ontario Ministry of the Solicitor General, 2019). The 2-year reconviction rate in the province of British Columbia, Canada, is at least 50% for those released from provincial custody according to government reports (BC Justice and Public Safety Council, 2017).
Literature demonstrates that mental illness and substance use may contribute to risk of recidivism (Rezansoff et al., 2013; Wilson et al., 2011, 2014). Studies have confirmed that substance use disorder is a robust predictor of any reconviction (Rezansoff et al., 2013) and reincarceration (Wilson et al., 2011, 2014). Research on the relationship between mental illness and recidivism has also concluded that adults who present with mental illness are more likely to be reincarcerated, reconvicted, and remain in custody for longer periods of time than their counterparts without mental illness (Messina et al., 2004; Rezansoff et al., 2013). Considerable research suggests that mental illness, in combination with substance use disorders, is significantly related to crime and violence (Ogloff et al., 2015; Van Dorn et al., 2012). For example, a longitudinal study, including 34,653 people in the United States, found that the incidence of violence was higher for people with serious mental illness, but only significantly so for people with co-occurring substance use disorder (Elbogen & Johnson, 2009). Importantly, broad categories of mental disorder and substance use disorder represent people with heterogeneous conditions. Nonetheless, they remain useful in the context of criminal justice and health policy because they reflect the organization of programs and services (Rezansoff et al., 2013).
The Relationship Between Co-Occurring Disorders and Recidivism
A small number of studies have examined the association between co-occurring disorders (COD; that is, mental disorders and substance use disorders) and recidivism, typically finding positive associations. Baillargeon et al. (2010) conducted a retrospective cohort study of more than 61,000 people incarcerated in a Texas prison and found that people with COD were significantly more likely to have experienced multiple reincarceration events over a 6-year follow-up compared with people with substance use disorder alone. Wilson et al. (2011) examined recidivism patterns in a large U.S. urban jail system over a 4-year period (N = 24,290). Using linked Medicaid claims and jail data, they compared four groups: those with no disorder, serious mental illness only, substance use disorders only, and COD. They found that people with COD had the highest number of readmissions to jail, with 68% returning to jail at least once in the 4-year follow-up (compared with 50% of the mental illness only group). Using the same cohort data, Wilson et al. (2014) found that after release from prison, people with COD spent the shortest amount of time in the community before returning to prison.
We are aware of one Canadian study by Rezansoff et al. (2013), which examined the relationship between COD and recidivism (in their study, the term “dual diagnosis” is used, rather than COD). The authors ascertained psychiatric diagnoses in a provincial prison sample in British Columbia (N = 31,014) using linked administrative health and justice data. They found that those with COD (23% of the sample) had significantly higher odds of recidivism (OR = 2.08) and multiple convictions (OR = 1.93) than people with no disorder. The studies conducted to date use official health records to ascertain diagnoses, which may significantly underestimate untreated illness in this population, and they control for only a small set of demographic and justice-related variables in their statistical models.
Current Study
In this study, we examined the relationships between mental health needs, substance use disorder, and COD, with time to reincarceration over a multiyear follow-up period, using population-level data for adults incarcerated in British Columbia, Canada. We hypothesized that reincarceration would be weakly associated with mental health needs only, and strongly associated with substance use disorder only and COD, with the COD group being at highest risk. Congruent with previous findings, we expected that people with COD would have the shortest time to reincarceration. The likelihood of recidivism as well as the timing of recidivism or justice system contact are key to understanding the processes underlying the effects of criminal sanctions and interventions and for identifying the highest risk periods for targeted prevention.
Method
Data Sources
The primary data source for this study is the Jail Screening Assessment Tool (JSAT; Nicholls et al., 2005) and the data were obtained from BC Corrections Research Branch. This tool, used in all facilities operated by BC Corrections, is a validated, detailed screener that has been recorded electronically since 2008 and has remained consistent throughout the study period. The JSAT is carried out using a 15- to 20-min structured interview to assess current functioning and need for mental health and substance use services, and comprises demographic, social, clinical, and risk variables. Trained intake screeners complete the JSAT interview during every prison admission, such that individuals with multiple incarcerations have multiple JSAT records. These data are entered into an electronic medical record housed on the Primary Assessment and Care (PAC) databases of the Ministry of Justice Corrections Branch.
Criminal justice information for each client was obtained from BC Correction’s CORNET (Corrections Operations Network) database, the primary repository for all data relating to an individual’s involvement with the BC Corrections system. CORNET is the electronic platform used by the Corrections Branch for the administration of sentences and supervision of people convicted of criminal offenses in BC. Our CORNET data set includes dates of admission and release, the movement reason (e.g., new sentence, sentence end, and breach), movement direction (in/out), facility name (to/from), custody description (Correctional Services Canada, remand, and provincial sentence), community sentence description (e.g., parole, bail order, and probation order), and dates of death that occur while a person is under BC Correction’s supervision.
The JSAT and the CORNET data sets both contain unique Client Identification Numbers, and this was used for the linkage. Additional checks were conducted using probabilistic identifiers, such as name and sex. Both data sets may contain multiple records for each Client ID and, to verify the admission type, we matched the JSAT to a corresponding CORNET record for only new admissions to custody. The JSAT records without a corresponding CORNET record for a new admission were excluded.
Institutional Approvals
The study was approved by the University of British Columbia Behavioral Research Ethics Board and Simon Fraser University Research Ethics Board (REB no. 17-02653), and the BC Corrections Performance, Research, and Evaluation Unit.
Setting
BC Corrections, a provincial government entity, is responsible for those sentenced to 2 years or less and people on remand. As such, clients who go on to be sentenced to federal custody will first pass through a provincial facility while waiting for trial and/or sentencing. However, as we do not have release dates for people who were transferred to federal custody, we excluded them from our sample. We also excluded people on immigration holds.
Study Population
This retrospective cohort study includes every adult who was (a) released from a BC provincial correctional facility, (b) had taken part in a JSAT interview upon admission, and (c) was released to the community between October 1, 2012, and September 30, 2014. If an individual had more than one release, the baseline incarceration was their first release during this time. There were 15,073 people released from prison during the study period. After excluding those who were transferred to federal custody, those who were on immigration holds, and those who died during baseline incarceration, the final sample included 13,109 people. The follow-up period was 3 years from the baseline release date.
Sociodemographic Variables
Baseline sociodemographic measures used in this study include sex (male/female), age, Indigenous status (includes Aboriginal, First Nations, Inuit, Metis, and Native), marital status (married/common law Y/N), housing (homeless/unstable housing Y/N), employment (full-time employment, part-time employment, or unemployed), education level (less than high school, high school completion, or postsecondary), receiving social support or disability payments (Y/N), and family support (frequent family support, some family support, or no family support).
Clinical Variables
Measures of clinical complexity included self-reported intellectual disability/head injury (Y/N), past suicide attempts (Y/N), psychiatric symptoms, score of ≥4 versus <4 as measured by the Brief Psychiatric Rating Scale (BPRS), and evidence of personality disorder traits (Y/N), per the intake interviewer. The BPRS is a validated tool used to measure psychiatric symptoms, such as depression, anxiety, hallucinations, psychosis, and unusual behavior (Overall & Gorham, 1962). Whereas the BPRS is normally coded on a 7-point scale, it is coded on a 3-point scale on the JSAT. As per prior research, a score of ≥4 on the BPRS reflects the presence of two symptoms, the presence of one symptom with the possible presence of three symptoms, or the possible presence of four symptoms (Gagnon, 2009).
Criminal Justice Variables
Criminal justice variables included incarceration in the previous year (Y/N), custody status (sentenced/remanded), and the length of stay for the index incarceration (<30 days vs. ≥30 days). These variables are well-known predictors of recidivism (informed by the literature, for example, Risk–Needs–Responsivity model; Bonta & Andrews, 2007; Bonta et al., 2014) and/or are independently associated with mental health and substance use needs and are therefore potential confounders in the relationship between mental health needs, substance use disorder, and reincarceration (Bonta et al., 2014). Additional details about the baseline measures can be found in the supplemental material.
Diagnostic Groups
We created four mutually exclusive categories for the condition variable: mental health needs only, substance use disorders only, COD, and no disorder. The mental health needs definition included a combination of reported history of mental health treatment and mental health needs identified within the “Mental Health Treatment” and “Management Recommendations” sections of the JSAT (details have been published in Butler et al., 2021). A client was coded as having a substance use disorder if current abuse or long-term severe abuse in any of the six JSAT drug categories—alcohol, heroin, cocaine, methamphetamine, marijuana, and other drugs—was positively indicated. A client was coded as having COD if both the mental health needs and substance use needs criteria were met on the same record.
Outcome Measures
The primary outcome measure was time to first reincarceration after the baseline release. The reincarceration could be for any new crime or a breach of conditions and was determined using the date of the first readmission to custody recorded in the BC CORNET database for which the person spent at least one night in custody and had a JSAT completed. Participant observation time was censored at date of death or 3 years after the baseline release date (i.e., if there was no record of reincarceration), whichever came first. The 3-year follow-up was calculated from each person’s release date. Although reincarceration as a measure of recidivism may not capture lower level offenses, it is also an important measure because there are well-known adverse impacts that are specific to custodial sentences. For example, mental health problems may be exacerbated or caused by conditions of confinement, including lack of purposeful activity, overcrowding, exposure to violence, and separation from family (De Viggiani, 2007; Schneider et al., 2011).
Analyses
We calculated proportions for baseline measures, stratified by diagnostic category. We used Pearson’s χ2 tests to examine differences in baseline sociodemographic, clinical, and criminal justice characteristics between the four diagnostic groups. We also used Pearson’s χ2 tests to compare the proportion of people reincarcerated within 3 years by diagnostic group. We calculated effect sizes to examine the substantive significance using Cramer’s V (ϕ) for the χ2 estimates. Cramer’s V of .10 provides a good minimum threshold for suggesting there is a substantive relationship between two variables; a result of .2 to .3 is considered moderately strong, and ≥.3 is considered strong (Marchant-Shapiro, 2015).
We used the Kaplan–Meier method to conduct survival analyses, examining number of days to reincarceration, stratified by diagnostic group (Stel et al., 2011). We fitted a Cox proportional hazards model—a multivariable approach for time-to-event regression analyses—to examine the association between psychiatric condition and risk of reincarceration. Schoenfeld residuals were plotted to confirm that the proportional hazards assumption was met.
Alpha level .05 was used for all statistical tests. All analyses were performed in R version 3.6.1 using dplyr, ggplot2, survival and survminer packages (R Development Core Team, 2020). All predictor variables were identified prior to analysis on the basis of previous literature and were included simultaneously in the Cox model as relevant adjustment variables in the primary association of interest, diagnostic category, and reincarceration. We created a correlation matrix with all baseline variables to test for multicollinearity and found that Pearson’s correlations were all below an acceptable level for inclusion in the model. We performed a log-rank pairwise χ2 test with Benjamini–Hochberg adjustment to compare the survival distributions across the four diagnostic groups.
Results
Descriptive Results
Cohort characteristics at baseline are summarized in Table 1. Women comprised 12% of the cohort, and 29% of people self-identified as Indigenous. Forty percent of people reported being on government assistance and 43% had less than a high school education. The mean age was 36 years (SD ± 10.9, range 18–84 years). With respect to our exposure, 3,019 people (23%) were categorized as having COD, 4,097 people (31%) had substance use needs only, 1,862 people (14%) had mental health needs only, and 4,131 people (32%) had no disorder. All variables differed significantly by diagnostic group, with varying effect sizes. Moderate associations were found for being on government assistance, employment status, suicide attempts, and psychiatric symptoms.
Cohort Characteristics at Baseline Stratified by Diagnostic Group
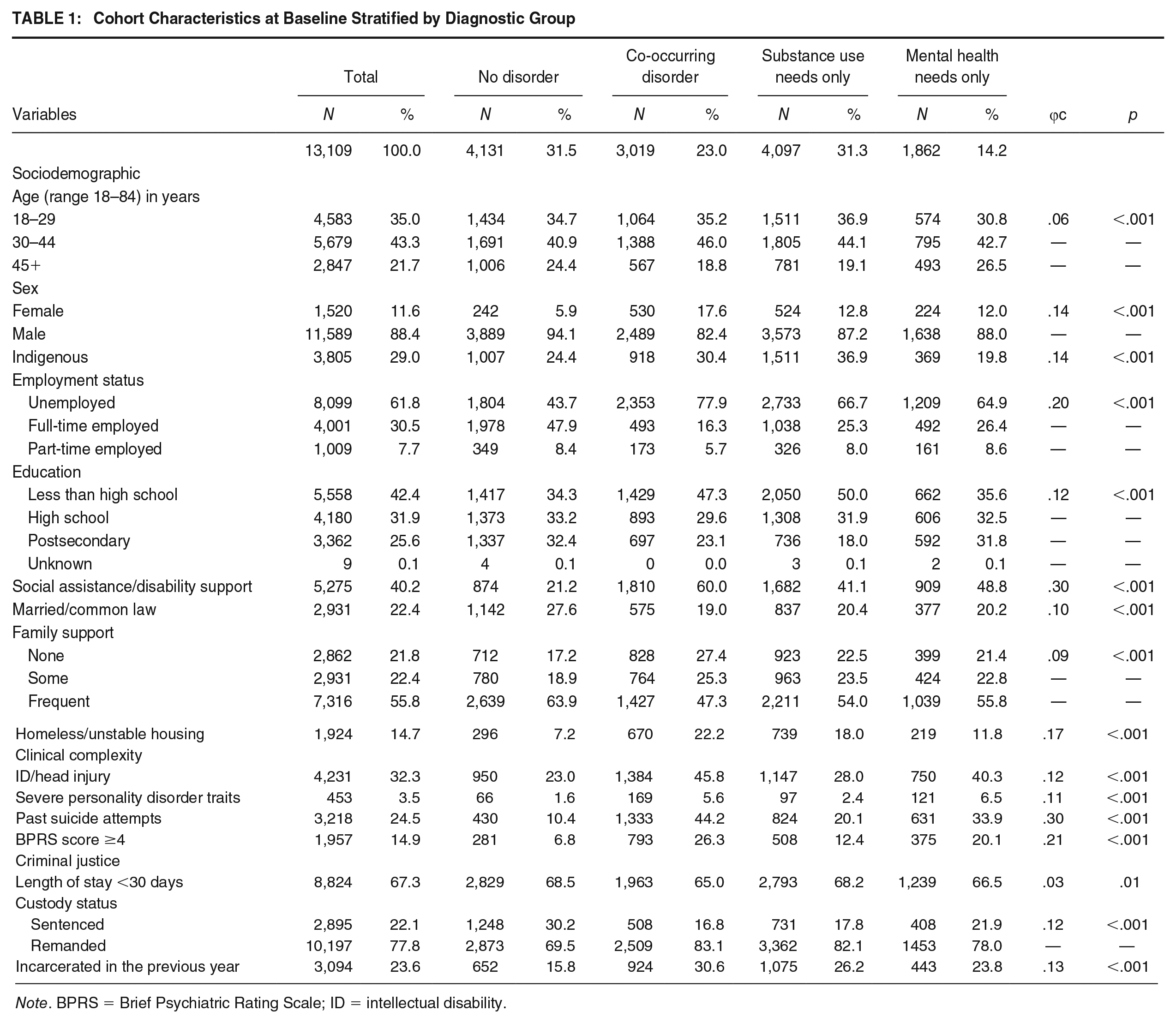
Note. BPRS = Brief Psychiatric Rating Scale; ID = intellectual disability.
Almost half of people with COD (47%) and exactly half of those with substance use needs had not completed high school (compared with 36% with mental health needs only, and 34% with no disorder). Over half (60%) of people in the COD group reported being on some form of government assistance (compared with 41% with substance use needs only, 49% with mental health needs only, and 21% with no disorder). People with COD were the least likely to report frequent family support, stable housing, or employment, and more likely to identify as female. The percentage of people with COD who reported being unemployed at admission was 78%, compared with 44% of those with no disorder. People with COD were the most likely to have been incarcerated in the past year (31%). In terms of clinical complexity, people with COD were the most likely to have an intellectual disability or a head injury, past suicide attempts, and/or psychiatric symptoms. Among those with COD, 46% had an intellectual disability or head injury, compared with 23% of those with no disorder. The vast majority of both the COD and substance use disorder group were on remand (83% and 82% respectively, compared with 78% of people categorized in the mental health needs only group and 70% of people in the no disorder group).
Reincarceration
Of the 13,109 people in the sample, 61% (n = 8,055) were reincarcerated within 3 years. Of those with at least one reincarceration, 27% had COD (n = 2,185), 35% (n = 2,853) had substance use needs only, 12% (n = 1,000) had mental health needs only, and 25% (n = 2,017) had no disorder. The proportion of people in each diagnostic category who were reincarcerated within 3 years is summarized in Figure 1. Among the COD group, 72% of people were reincarcerated, followed by people with substance use disorder only (70%), mental health needs only (54%), and no disorder (49%). The χ2 test for reincarceration and all diagnostic groups was significant (p <. 001) with medium effect size (V = .21). All pairwise tests were significant at p ≤. 01 after adjusting for multiple comparisons using the Holm method. The effect sizes for the pairwise comparisons, in order of smallest to largest effect size, are as follows: COD × substance use disorder: V = .03; mental health needs × none: V = .05; substance use disorder × mental health needs: V = .15; COD × mental health needs: V = .19; substance use disorder × none: V = .21; and COD × none: V = .24).
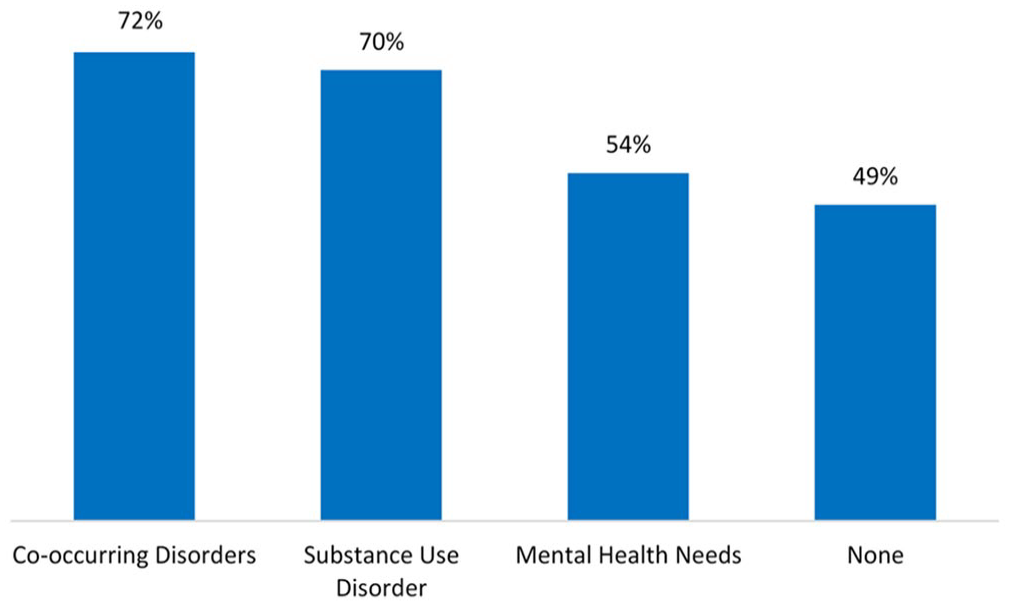
Percentage of People Reincarcerated Within 3 Years by Diagnostic Group
The Kaplan–Meier curve for reincarceration is displayed in Figure 2. People with COD had the shortest median survival time to reincarceration (220 days), followed closely by substance use needs only (263 days). In contrast, the median survival time for people with mental health needs only was significantly longer (806 days). Using a pairwise log-rank χ2 test, all six pairwise comparisons were significant at p ≤. 001. The log rank χ2 tests compare the trajectories of reincarceration (i.e., frequency and time), so a significant pairwise comparison is a difference in reincarceration trajectories between groups, not just time to reincarceration.
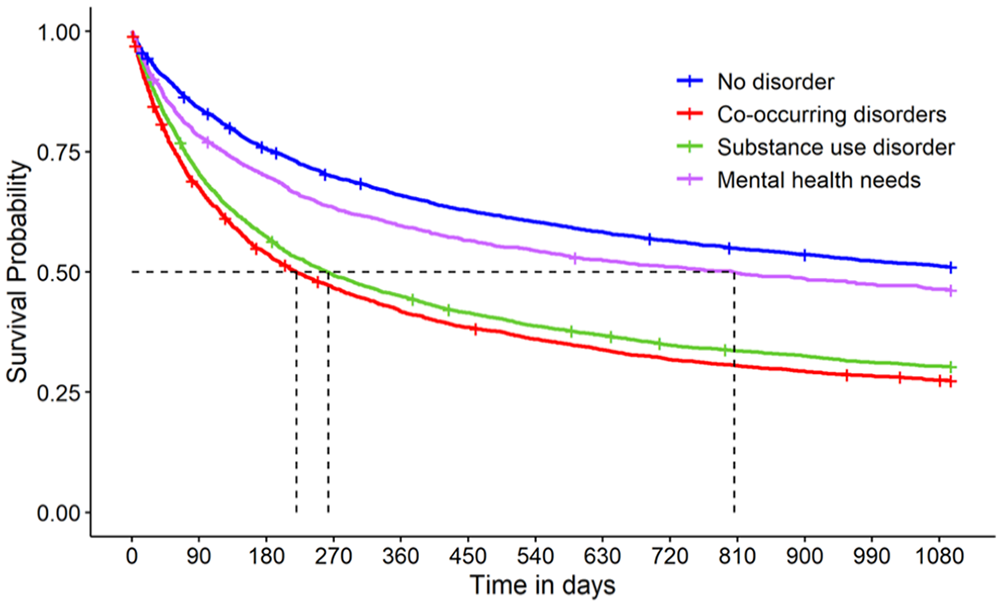
Survival Curve for Time to Reincarceration by Diagnostic Group
In the unadjusted Cox proportional hazards model, being female and having a university education were negatively associated with reincarceration. Reincarceration was more common in younger age groups; being 45 years of age or older was significantly protective against reincarceration. Indigenous identity, unemployment, homelessness, lacking family support (having some or none), intellectual disability/head injury, personality disorder traits, previous incarceration, being on social assistance, psychiatric symptoms, and any mental health needs or substance use needs were all significantly associated with reincarceration (unadjusted hazard ratios are available in supplemental material). After adjustment for covariates (Table 2), the single strongest predictor of reincarceration was COD, adjusted hazard ratio (aHR) = 1.57, 95% confidence interval [CI] [1.47, 1.69], followed closely by substance use needs alone (aHR = 1.52, 95% CI [1.43, 1.62]). Mental health needs alone was not significant in the adjusted model with an aHR of 1.05 (95% CI [0.97, 1.13]).
Adjusted Hazard Ratios (and 95% CIs) Examining the Association Between Diagnostic Group at Baseline and Reincarceration
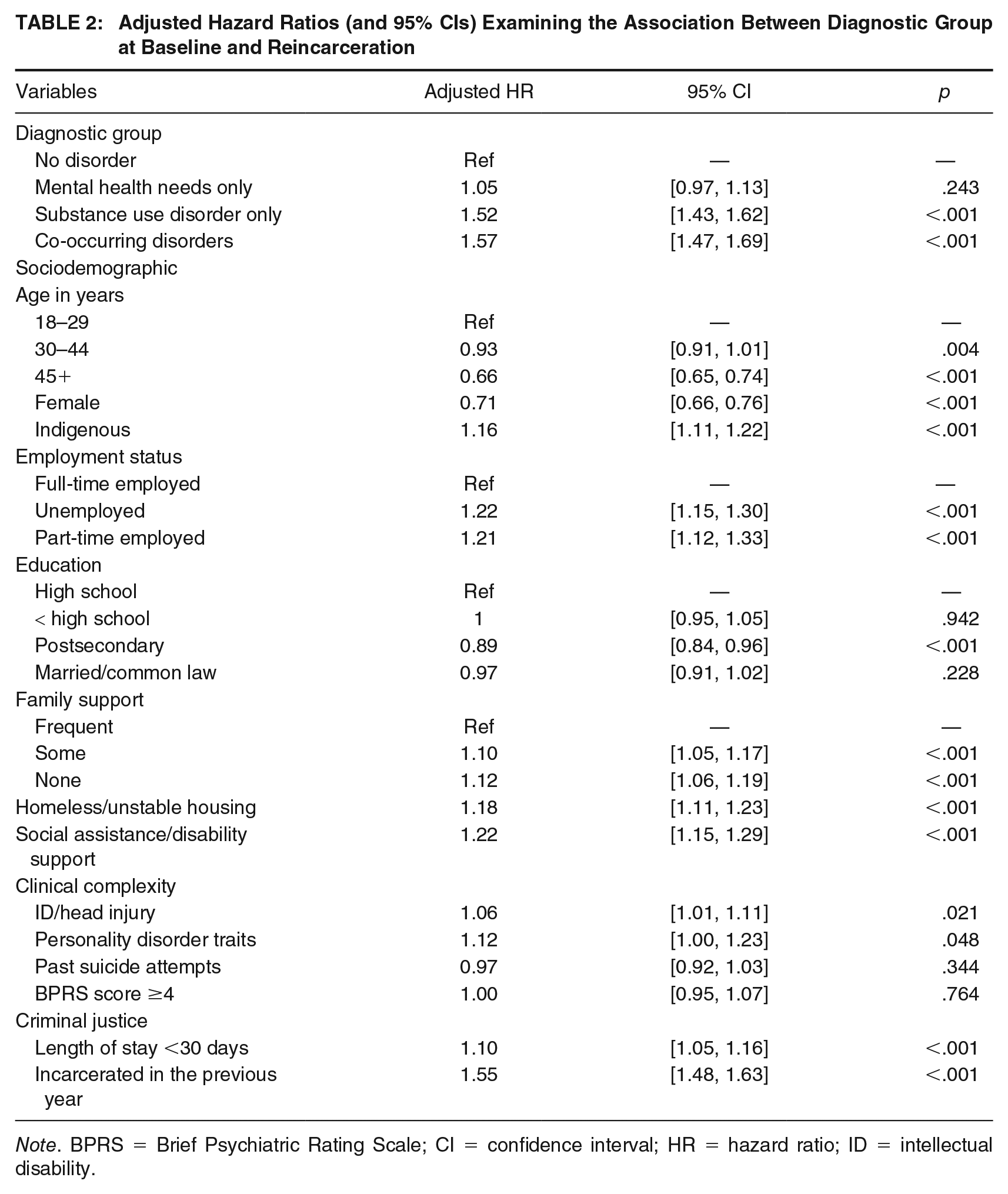
Note. BPRS = Brief Psychiatric Rating Scale; CI = confidence interval; HR = hazard ratio; ID = intellectual disability.
Discussion
As hypothesized, COD and substance use disorder alone were positively and significantly associated with reincarceration—people in these categories had the highest rate of reincarceration and the shortest time in the community before experiencing a reincarceration event. Those with no disorder had the lowest risk of reincarceration, with the median survival time extending beyond the 3-year postrelease period. After adjustment for covariates, having mental health needs alone was not significantly associated with reincarceration compared with people with no disorder. The COD group had the highest proportion of people experiencing at least one reincarceration during follow-up.
Our findings are consistent with previous studies that have found differential risk of reincarceration between people with mental illness, substance use disorder, and COD (Rezansoff et al., 2013; Wilson et al., 2014; Zgoba et al., 2020). This study adds to the evidence that the excess risk of recidivism associated with mental illness is largely mediated by co-occurring substance use and social determinants of health (Chang, Lichtenstein, et al., 2015; Fazel et al., 2017; Fusar-Poli et al., 2023). Importantly, while mental illness is relevant to criminal justice involvement, the contribution to the risk of crime and violence specifically is considered modest (Thornicroft, 2020). In our study, the significant relationship between mental health needs and reincarceration did not hold up after adjustment for relevant covariates. Epidemiological studies, research, and public policy often fail to consider social determinants of health when examining crime and violence among individuals with mental illness (Fusar-Poli et al., 2023). Although nonsubstance-related mental illness generally does not appear to be a strong risk factor for crime, it is nonetheless a responsivity factor. Many psychiatric illnesses cause functional impairments that can significantly affect a person’s response to interventions targeting criminogenic needs (Osher et al., 2012). For example, a person with untreated psychosis may not benefit from an intervention to treat antisocial cognition until their clinical symptoms are addressed. As such, the treatment of mental health conditions remains an essential component of interventions to prevent recidivism and improve outcomes.
One of the most reliable findings in criminology is the relationship between substance use and criminal offending (Bonta et al., 2014; Chang, Larsson, et al., 2015; Whiting et al., 2021; Zgoba et al., 2020). Research suggests that a large portion of the crimes committed by people with substance use disorder is fundamentally driven by the need/motivation to obtain drugs (White & Gorman, 2000) and people with drug involvement are more likely to commit economically motivated crimes and to have illegal earnings (Bennett et al., 2008; Gottfredson et al., 2003; Kirwan et al., 2015; Uggen & Thompson, 2003). Other explanations have focused on the pharmacological model that proposes that the relationship between the effects of drug intoxication (e.g., impairment judgment) and its byproducts (e.g., withdrawal, sleep deprivation) can increase risk of criminal behavior (Gottfredson et al., 2003; White & Gorman, 2000). Although it is apparent that an important connection exists between substance use and crime, the precise nature of the relationship remains elusive (White, 2016) and understanding which treatment modalities are most appropriate for custodial settings remains a critical gap in knowledge (Zaller et al., 2022).
COD and substance use disorder were significantly associated with reincarceration in both the unadjusted and adjusted models in our study, but the sizable attenuation of the hazard ratios after adjustment for a range of covariates demonstrates that the risks associated with substance use and COD intersect with many other risk–need issues. Specifically, people in the COD group were the most likely to report less than high school education, unemployment, being on social assistance, lacking family support, and homelessness/unstable housing, which is consistent with previous research on COD populations (Dickey et al., 2002; Haverfield et al., 2019; Rush & Koegl, 2008; Watkins et al., 2004).
It is notable that, after adjustment for several dynamic risk factors, COD remained the single strongest predictor of reincarceration. Studies have found that co-occurring substance use is a key predictor of violence among people with serious mental illness (Whiting et al., 2021; Witt et al., 2013). Research has also shown a significant decrease in violence among people with serious mental illness who are stabilized on antipsychotic medication and mood stabilizers (Fazel et al., 2014). Nonadherence to psychiatric medication, which is a major impediment to the treatment of serious mental illness, is elevated among people with COD because substance use is strongly associated with unintentional nonadherence to treatment (Velligan et al., 2017). Adherence enhancement approaches, which have the potential to reduce crime and violence, must therefore simultaneously target the substance use needs of this subgroup, ideally through integrated treatment programs (Drake et al., 2001). Integrated treatment refers broadly to a flexible combination of treatments from the mental health and addiction fields that are blended together in the treatment of an individual with COD (Ziedonis et al., 2005).
Implications
The study lends support to previous evidence demonstrating the need for treatment and services to support people during incarceration and at the time of release from custody. Among people released from prison, resuming drug use and reoffending is common in the initial postrelease period, particularly in the context of poor social support, financial insecurity, and unstable housing (Binswanger et al., 2012). Policy discussions about the criminalization of people with substance use disorders and COD often fail to consider the intersectional structural vulnerability and overlapping inequities that contribute to the ongoing harms that they experience (Friedman et al., 2021). Some of the consequences of drug criminalization include a highly toxic illicit drug supply, stigma, and harms associated with having a criminal record, such as increased barriers to employment, housing, and education (Butler et al., 2022; Collins et al., 2019; Félix & Portugal, 2016; Watson et al., 2021). Compared with people with mental disorder, people with substance use disorder are more likely to be blamed and judged for behavior that may be both a symptom of their condition (e.g., relapse to drug use) and a risk factor for reincarceration (e.g., conditions of parole/probation often include abstaining from drugs; Lloyd, 2013). Recognition of the failures associated with prohibitionist drug policy has led to advocacy for alternative approaches and calls for decriminalization of drugs. In 2022, the federal government approved a request from British Columbia’s Ministry of Health for an exemption from the Canadian Drugs and Substances Act that decriminalizes personal possession (up to 2.5 g cumulative) of certain drugs for adults aged 18 years and older in the province as of January 2023 (Government of British Columbia, 2022). Future research will be required to determine whether this policy significantly reduces incarceration among people with substance use disorder and COD.
The prevalence of mental health needs among people in custody and the relationship to reincarceration ought to be interpreted within the context of the broader system of mental health care and services (or lack thereof) for people in the intersection of mental health and the law. A person can be found Not Criminally Responsible on Account of Mental Disorder (or “NCR”) and will then receive care within the forensic mental health system rather than being sent to a correctional facility. However, NCR adjudications are rare as they apply only to severe mental illness (generally with psychotic symptoms) at the time of the offense. NCR cases represent less than 1% of adult criminal court cases processed annually in Canada (Miladinovic & Lukassen, 2015). Outside of this narrow NCR regime, Canada has limited extrajudicial options to support people with mental illness who come into conflict with the law. In contrast, in the United Kingdom, a person can be diverted from a custodial sentence to hospital for treatment by a court under the Mental Health Act 1983, and this can occur at both the pre- and postsentencing stages of the criminal justice process (Ministry of Justice UK, 2021). In addition to limited criminal justice diversion opportunities, community mental health services often fail to meet the needs of people with mental illness before they become involved in crime in Canada (Penney et al., 2023). A study of all people found NCR in three Canadian provinces over 5 years found that most people who were found NCR had been under the purview of the civil psychiatric system with a median of two prior civil psychiatric hospitalizations (Crocker et al., 2015). The findings suggest that reductions in offending by people with serious mental illness may be achieved by prioritizing and adequately funding violence risk assessment training and interventions to prevent further mental health deterioration within civil psychiatry (Crocker et al., 2015).
Systems-level changes are required to increase options to divert people away from custodial dispositions, reduce treatment barriers, and increase the suitability of services in community to match client needs and preferences. Incarceration provides an opportunity (however regrettable) to identify undiagnosed and untreated mental health and substance use needs and connect people to resources. The transition period from custody to community is a high-risk time for adverse outcomes, including mortality and return to custody (Butler et al., 2023; Kouyoumdjian et al., 2016). Given the short length of stay in provincial correctional settings, case management, thorough discharge planning, and linkage to community services should be prioritized. Prison-based and community-based health services need to synergize to ensure a warm handoff, especially for postrelease mental health, substance use, and COD treatment (Chowdhury et al., 2022).
Strengths and Limitations
This study is the first of its kind in Canada to examine the impact of mental health needs and substance use needs on time to reincarceration, using a population-based sample. Most studies to date have relied on linked administrative health data to ascertain diagnoses and are typically limited to demographic variables, such as age, sex, ethnicity, education, and offending history. This study uses universal mental health screening information at the time of admission to custody, likely capturing people who may not have a diagnosis recorded in a health database either because they have not sought treatment and/or faced barriers to accessing treatment. Because the primary data source is a detailed screening instrument containing rich sociodemographic and clinical information, the variables in the model that are known predictors of reincarceration allowed us to isolate the independent effect of substance use and COD on reincarceration more confidently than other studies available in the literature (Rezansoff et al., 2013; Wilson et al., 2011, 2014).
This study also has some notable limitations. The definition of COD we used reflects self-reports of both current substance use needs and mental health needs at the same time, so this proportion may be an underestimate of the true prevalence of COD in the population. Although there are limitations associated with self-report data, studies with marginalized populations show that self-report measures are highly reliable and valid, particularly for health care use and drug use (Carroll et al., 2016; Emmert et al., 2015; Somers et al., 2016). Our definition of mental health needs lacks diagnostic specificity. Previous research has found that rates of violence among people with mental illness differ widely between diagnostic groups. For example, research has found that rates of violence are substantially elevated for people with personality disorders and schizophrenia spectrum disorders (Whiting et al., 2021). So, while we found that mental illness alone was not a strong risk factor for reincarceration, it is possible that important relationships exist between specific conditions and reincarceration for specific crime types.
Our data did not include any information on geographic destination at the point of release, so potential loss to follow-up could not be completely assessed. We were also unable to control for all deaths, which means that we may have underestimated the role of mental health and substance use diagnoses on reincarceration, and specific disorder subgroups are likely to be differentially affected by this limitation. For example, a BC-based study found that people with previous incarceration history were more than 4 times more likely to die from overdose than those who had never experienced incarceration (Gan et al., 2021), demonstrating that there may be shared mechanisms that elevate risk of both death and reincarceration. Finally, the statistical model excludes some risk factors for mental health needs, substance use disorder, and reincarceration that were unavailable in our data set (e.g., pro-criminal attitudes, peers involved in crime).
Conclusion
Using a population-level cohort of people released from custody, our study found that substance use disorder and COD are significantly related to reincarceration over time. Mental health and substance use risk–needs intersect with other key criminogenic risk factors, such as low education, unemployment, unstable housing, and lack of social support. Correctional, health, and social services must work synergistically to reduce reincarceration and other adverse outcomes, particularly among people with substance use and COD.
Supplemental Material
sj-docx-1-cjb-10.1177_00938548241238327 – Supplemental material for Mental Health Needs, Substance Use, and Reincarceration: Population-Level Findings From a Released Prison Cohort
Supplemental material, sj-docx-1-cjb-10.1177_00938548241238327 for Mental Health Needs, Substance Use, and Reincarceration: Population-Level Findings From a Released Prison Cohort by Amanda Butler, Tonia L. Nicholls, Hasina Samji, Sheri Fabian and M. Ruth Lavergne in Criminal Justice and Behavior
Footnotes
Authors’ note:
The authors would like to acknowledge Dr. Leigh Greiner, Director of Research and Strategic Planning at BC Corrections, for her invaluable feedback on the project proposal and support during the data cleaning process. We also gratefully acknowledge Dr. Maureen Olley, Director of Mental Health Services at BC Corrections, for helping to develop the diagnostic codes and for responding to several queries. AB, HS, and SF declare no conflicts of interest. TN is an author of the Jail Screening Assessment Tool (JSAT) manual and provides JSAT workshops under contract. This work was funded by a Frederick Banting & Charles Best Canada Graduate Scholarships–Doctoral Award (CGSD) from the Canadian Institutes for Health Research held by AB during her doctoral work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.