
Abstract
Correctional officers work in a stressful environment and are exposed to elevated levels of critical incidents. Such exposure can lead to negative psychological outcomes like burnout. However, positive psychological experiences including well-being and posttraumatic growth are also possible under such adverse conditions. Therefore, the purpose of this study was to explore predictors of burnout, well-being, and posttraumatic growth in a sample of correctional officers (N = 142). The results of multiple regression analyses indicated that age, workplace adversity, and resilience were significant predictors of correctional officer burnout. A sense of workplace belongingness and the use of adaptive coping strategies were significant positive predictors of well-being and posttraumatic growth. Trait resilience and the receipt of social support were additional significant positive predictors of well-being. These results highlight the importance of individual, interpersonal, and organizational factors in promoting positive health outcomes, preventing negative health outcomes, and providing avenues for staff support.
Keywords
Correctional officers work within the confines of prison with people who tend to be highly distressed (Crawley, 2004). Not only do they maintain security, but they also act as proxy counselors, health care workers, and first responders to appropriately care for the people under their supervision (Crawley, 2004). Thus, their work can be highly stressful and expose them to potentially traumatic critical incidents such as prison resident self-harms (Carleton et al., 2019). Given this context, it is unsurprising that correctional officers show high rates of posttraumatic stress disorder (PTSD; Carleton et al., 2019), burnout (Lambert et al., 2015), stress (Butler et al., 2019), depression, and anxiety (Regehr et al., 2021).
Nonetheless, the broader literature suggests that mental illness is not the most common psychological outcome, and that well-being and growth are possible under adverse conditions (e.g., Bonanno et al., 2012). For example, 2021 census data found that under 10% of Australian correctional officers self-reported a mental illness suggesting that approximately 90% were able to remain mentally well (Australian Bureau of Statistics [ABS], 2021). Indeed, the salutogenic model of health (Antonovsky, 1996) considers health to exist on a continuum ranging from dis-ease to health-ease and argues that an understanding of both ends of the continuum is needed to adequately promote health beyond disorder absence. The salutogenic model of health postulates that life is innately stressful leading to tension which can be negative, neutral, or positive. Whether tension leads to negative, neutral, or positive health outcomes depends on the person’s ability to manage tension and draw on appropriate resistance resources. Some resistance resources can support health (protective factors) while others can hinder health (risk factors), and it is a person’s ability to appropriately draw on these resources that determines their health status.
Most prior correctional officer research has been pathogenic with a focus on the dis-ease end of the continuum (e.g., Butler et al., 2019; Regehr et al., 2021). This means that the health-ease end of the continuum remains underresearched for correctional officers, including resistance resources that predict their health. The salutogenic model of health (Antonovsky, 1996) serves as the theoretical foundation of this study which aimed to explore the health of Australian correctional officers across the health continuum to answer the following research question:
The Australian Context
Approximately 19,861 Australians work as correctional officers (ABS, 2021) across 115 prisons which are predominantly high security and government operated (Australian Government Productivity Commission [AGPC], 2022). They care for over 40,000 people (ABS, 2022, 2023), many of whom identify as male and/or Aboriginal or Torres Strait Islander and live with a mental illness (Australian Institute of Health and Welfare [AIHW], 2022; AGCP, 2022). Thus, Australian correctional officers not only maintain prison security but also assist with prison resident rehabilitation, education, and health care.
Little is known about the health of Australian correctional officers in comparison with international officers. The available Australian research has been predominantly pathogenic, suggesting Australian officers frequently experience potentially traumatic critical incidents and mental illnesses (e.g., Eriksson, 2021; Trounson et al., 2016, 2022). Very little Australian research has explored correctional officer health as more than disorder absence. Trounson et al. (2022) explored the social and emotional well-being of Aboriginal and Torres Strait Islander officers and found that resistance resources like connection to culture, morale, social relationships, and somatic health impacted well-being. However, the results are unlikely to transfer to non-Indigenous officers. More recently, Miller et al. (2023) qualitatively explored the mental health of Australian officers and found that they could experience personal growth and a sense of purpose in addition to mental illness symptoms.
Burnout
Burnout develops after prolonged exposure to stress and is characterized by high levels of emotional exhaustion and depersonalization and low levels of perceived personal accomplishment (Maslach & Jackson, 1981). It is often experienced by caring professionals like psychologists and social workers and is being recognized in correctional staff (Forman-Dolan et al., 2022). If left untreated, burnout can develop into symptoms of depression and anxiety (Koutsimani & Montgomery, 2023). Therefore, correctional officer burnout is important to understand given its potential deleterious effects on health.
The existing literature suggests individual demographic factors like age or sex have limited impact on correctional officer burnout (Forman-Dolan et al., 2022; Lambert et al., 2015, reviews). Other individual resistance resources like resilience and coping have stronger effects. For example, resilience has been shown to be protective against correctional officer emotional exhaustion (Klinoff et al., 2018), as has adaptive problem-focused coping strategies (Gould et al., 2013). In contrast, maladaptive coping strategies like denial can contribute to burnout (e.g., Hughes-Taylor & Swartz, 2021).
Workplace stressors are thought to be the strongest predictors of correctional officer burnout and can be classified as stressors intrinsic to the job, those related to workplace relationships, and those related to the organizational climate (Forman-Dolan et al., 2022). Stressors intrinsic to the job include work overload, lack of autonomy, and perceived danger. A perception of danger, including exposure to critical incidents, has consistently been linked to correctional officer burnout (e.g., Choi et al., 2020) as well as distress and PTSD (e.g., Ellison et al., 2022; Trounson et al., 2019). Workplace social support, particularly from supervisors and peers, can protect correctional officers from developing burnout as can support from loved ones (Cavallari et al., 2021; Isenhardt et al., 2019; Lambert et al., 2010). Similarly, variables related to a positive organizational climate are protective against correctional officer burnout. For example, a sense of organizational support (Gao et al., 2022), cohesion among colleagues (Isenhardt et al., 2019), and trust in supervisors and management (Lambert et al., 2012) negatively predict correctional officer burnout. A sense of workplace belongingness appears protective against burnout in other high-risk occupations (e.g., Shakespeare-Finch & Daley, 2017).
Well-Being
In contrast to the abundance of research on correctional officer burnout and pathology, there are comparatively few studies exploring correctional officer well-being. Contributing to this is the lack of consensus regarding the operationalization of well-being (Dodge et al., 2012). Two of the most widely adopted conceptualizations are Diener’s (1984) subjective well-being (SWB) and Ryff’s (1989) psychological well-being (PWB). SWB refers to the presence of positive affect and life satisfaction and the absence of negative affect (Diener, 1984). PWB is conceptualized as positive functioning across six domains: self-acceptance, positive relationships, autonomy, environmental mastery, purpose, and personal growth (Ryff, 1989). Regardless of the definition adopted, it is widely acknowledged that well-being extends beyond disorder absence (Dodge et al., 2012). Despite this, most research exploring correctional officer well-being has measured markers of pathology, inferring health as the absence of pathology (e.g., Burhanullah et al., 2022; Cavallari et al., 2021).
Where well-being has been recognized as more than the absence of pathology, it tends to have been narrowly defined by focusing on officer job satisfaction (Butler et al., 2019) or life satisfaction (Miller et al., 2022). Qualitative literature suggests that resistance resources like connection to culture, social support, and adaptive coping supports correctional officer well-being, while exposure to operational and organizational stressors like violence, a masculine organizational culture, and low managerial support reduces officer well-being (Miller et al., 2023; Ricciardelli & Power, 2020; Trounson et al., 2022). Research into other frontline occupations suggests that adaptive coping, social support, resilience, and workplace belongingness promote well-being (e.g., Harnett et al., 2023; Huynh et al., 2014; Shakespeare-Finch & Daley, 2017); while maladaptive coping and perceived danger reduce well-being (e.g., Laffey et al., 2020; Trounson et al., 2019).
Posttraumatic Growth
Posttraumatic growth can also occur after exposure to highly stressful events that initially overwhelm a person’s capacity to cope (Tedeschi et al., 2018). Posttraumatic growth refers to positive transformative changes over five broad domains: appreciation of life, personal strength, spiritual or existential beliefs, relationships with others, and identifying new possibilities. Posttraumatic growth is yet to be comprehensively examined in correctional officers. To the authors’ knowledge, Tatebe et al. (2020) remain the only ones to have measured posttraumatic growth in correctional officers. American emergency responders, including a subsample of correctional officers, showed posttraumatic growth scores indicative of significant growth, and correctional officers had the highest level of growth across groups. While helpful in showing that correctional officers can experience posttraumatic growth, comprehensive analyses were not conducted to provide an understanding of the resistance resources that predict officer posttraumatic growth.
Konyk and Ricciardelli (2023) qualitatively explored posttraumatic growth in Canadian correctional officer recruits who recognized growth in their compassion for others and sense of personal strength. However, as the participants were recruits the experiences that precipitated their posttraumatic growth did not occur in a correctional context. Similarly, Miller et al. (2023) found that correctional officers experienced personal growth in domains consistent with posttraumatic growth including appreciation for life and freedom, personal strength, and ability to understand and relate to others. While this research provides preliminary evidence that posttraumatic growth is possible for correctional officers, the predictors of correctional officer posttraumatic growth remain unexplored.
Posttraumatic growth has been examined more frequently in other frontline occupations like firefighters (e.g., Armstrong et al., 2014) and emergency medical dispatchers (e.g., Shakespeare-Finch et al., 2015). Such literature has found that resistance resources like social support, workplace belongingness, and perceived danger can promote posttraumatic growth (e.g., Armstrong et al., 2016; Dyball et al., 2022; Shakespeare-Finch et al., 2015). Research with civilians further suggests that adaptive coping and resilience can promote posttraumatic growth (Kong et al., 2018; Prati & Pietrantoni, 2009), while maladaptive coping can limit posttraumatic growth (e.g., Kalaitzaki et al., 2023).
The Current Study
Limited research has explored correctional officer health across the health continuum, particularly well-being and posttraumatic growth. Therefore, this study aimed to address this gap by exploring predictors of correctional officer burnout, well-being, and posttraumatic growth. It was hypothesized that:
Method
Participants
Participants were 142 Australian correctional officers working in a frontline capacity (i.e., had frequent direct contact with prison residents). The sample consisted of 89 men and 52 women (one participant did not divulge their gender identity) who ranged in age between 21 and 69 years (M = 46.12, SD = 10.91). Participants had between 1 and 34 years (M = 9.91, SD = 7.14) experience working in corrections and had worked an average of 74.2 hours (SD = 26.11) in the fortnight preceding survey completion. Most participants were Caucasian (87.3%), married or in a de facto relationship (63.4%), certificate/diploma educated (66.9%), had no prior frontline work experience (69%), worked in high security prisons (92.3%), and worked with male prison residents (78.9%). Most participants (n = 137; 96.5%) had experienced at least one critical incident which they perceived to be severe (range 0 to 9; M = 7.17, SD = 2.19). The most commonly experienced critical incidents were witnessing/responding to prison resident self-harm or suicide attempt (55.6%), responding to a death in custody (21.8%), responding to a civilian medical emergency (21.1%), witnessing/responding to a staff assault (18.3%), and experiencing grief and loss (15.5%). 1
A priori power analyses indicated that a sample size over 200 would be ideal but that the current sample size was sufficient. Using a generic sample size calculation (G*Power Version 3.1; Faul et al., 2007) for a regression model with a medium (R2 = .13) to large (R2 = .26) overall effect, 80% power, a Bonferroni corrected alpha level of .016 (.05/3 analyses), and 18 independent variables (predictor variables and all demographic/control variables), between 115 and 135 participants were required. For a medium-to-large overall effect size with 90% power and a Bonferroni-corrected alpha, between 211 and 253 participants were required. Only demographic and control variables found to be significant in preliminary analyses were included in regressions. Therefore, the number of independent variables was reduced, further reducing the need for a larger sample.
Procedure
Ethical approval was obtained from the University Human Research Ethics Committee (approval number 5707) and the correctional department’s research committee. Data were collected in 2023 postpandemic after health restrictions were lifted in Australia. Participants were recruited from five prisons selected by the correctional department including both high- and low-security and male and female centers. An invitation to participate, including information about the study and the survey link, was emailed to correctional officers by their employer. Those that wished to participate voluntarily completed the online survey and were offered the chance to win one of the three $100 AUD vouchers. Data analysis followed, including a series of multiple regression analyses to assess what resistance resources predicted emotional exhaustion, well-being, and posttraumatic growth. Multiple testing corrections were applied using the Benjamini–Hochberg (BH) method with a false discovery rate of 10% (Benjamini & Hochberg, 1995).
Measures
The online survey asked participants about their exposure to critical incidents and their experiences of burnout, well-being, posttraumatic growth, coping, social support, workplace adversity, workplace belongingness, and resilience. See Supplementary Material for the full survey battery.
Sociodemographic Variables
Participants provided basic sociodemographic information about their age, gender identity, relationship status, educational attainment, previous frontline work experience, shift work patterns, and tenure, as well as characteristics of the specific prison they worked at including security level and prison resident sex.
Critical Incident Exposure
Participants were provided with the following definition of a critical incident and asked if they had experienced a critical incident at work and/or in their personal lives: a critical incident is an event that a person witnessed or was confronted with that involved threatened or actual danger to themselves or another person and which evoked a strong emotional response. This differentiated incidents common to emergency service occupations from those experienced as critical or traumatic. Participants then rated the severity of the incident on a scale from 0 (not traumatic) to 9 (severely traumatic).
Burnout
Burnout was operationalized as emotional exhaustion and was measured using three items from the abbreviated Maslach Burnout Inventory (Riley et al., 2017): (a) I feel emotionally drained from my work, (b) I feel fatigued when I get up in the morning and have to face another day on the job, and (c) working with people all day is really a strain for me. Responses ranged from 0 (never) to 6 (everyday) and higher scores represented higher levels of emotional exhaustion. The abbreviated Maslach Burnout Inventory has been validated against the Maslach Burnout Inventory and demonstrated comparable sensitivity and specificity (Riley et al., 2017), and generated a Cronbach’s alpha of .85 in this study.
Well-Being
Well-being was assessed using the Mental Health Continuum Short Form (MHC-SF; Keyes et al., 2008). The MHC-SF is a 14-item measure of well-being over three subscales: emotional well-being (consistent with SWB; three items), PWB (six items), and social well-being (five items). Participants were asked about their well-being over the past month, for example, how often they felt happy (emotional well-being), that you had something important to contribute to society (PWB), or that you had warm and trusting relationships with others (social well-being). Responses ranged from 0 (never) to 5 (everyday) with higher scores representing higher well-being. The MHC-SF has established good internal consistency (Lamers et al., 2011), as supported by this study (overall α = .94; subscale α = .87 - .91).
Posttraumatic Growth
Posttraumatic growth was measured using the Posttraumatic Growth Inventory X (PTGI-X; Tedeschi et al., 2017). The PTGI-X is a 25-item measure of posttraumatic growth across five subscales: personal strength (four items), relations with others (seven items), ability to see new possibilities (five items), appreciation of life (three items), and spiritual/existential change (six items). Sample items include I have a great feeling of self-reliance (personal strength), I more clearly see that I can count on people in times of trouble (relationships with others), I developed new interests (new possibilities), I changed my priorities about what is important in life (appreciation of life), and I have a greater sense of harmony with the world (spiritual/existential change). Participants rated how much change occurred due to the critical incident they described at the beginning of the survey or the incident they perceived as most severe if they described more than one incident. Responses ranged from 0 (change did not occur at all) to 5 (change happened to a very great degree). Total scores range from 0 to 125 with higher scores representing greater posttraumatic growth. The PTGI-X has demonstrated reliability across cultural groups (Tedeschi et al., 2017) and this study confirmed high overall (α = .96) and subscale (α = .73–.90) internal consistency.
Coping Strategies
Coping strategies were assessed using the dispositional version of the Brief COPE (Carver, 1997). The dispositional version asks about coping strategies typically used by participants rather than in response to a specific stressor. The Brief COPE has 14 subscales (two items each) however, a two-factor solution was used due to low subscale internal consistency. The two-factor solution included adaptive coping (active coping, planning, positive reframing, acceptance, religion, humor) and maladaptive coping (venting, denial, substance use, behavioral disengagement, self-distraction, self-blame). Sample items include I concentrate my efforts on doing something about the situation I’m in (adaptive coping) and I use alcohol or other drugs to make myself feel better (maladaptive coping). The emotional and instrumental support subscales were excluded from the adaptive coping factor as social support was measured separately. Participants were asked how often they used coping strategies ranging from 1 (I do not do this at all) to 4 (I do this a lot) with higher scores representing greater use of the strategy. This study demonstrated acceptable overall (α = .76) and subscale reliability (adaptive coping α = .79; maladaptive coping α = .77).
Social Support
Social support was measured with the Brief 2-Way Social Support Scale (Brief 2-Way SSS; Obst et al., 2019). This is a 12-item measure of social support across four subscales (three items each): giving emotional support (e.g., I give others a sense of comfort in times of need), giving instrumental support (e.g., I am a person others turn to for help with tasks), receiving emotional support (e.g., there is someone in my life I can get emotional support from), and receiving instrumental support (e.g., I have someone to help me if I am physically unwell). Participants completed the scale in reference to their experiences outside of work. They indicated how generally true each statement was ranging from 0 (not at all) to 5 (always) with higher scores representing higher levels of social support. The Brief 2-Way SSS has showed good internal consistency, test–retest reliability, concurrent and predictive validity (Obst et al., 2019), and this study confirmed good overall (α = .89) and subscale reliability (α = .60–.92).
Workplace Adversity
Workplace adversity was measured using the 36-item Work-Related Environmental Adversity Scale (WREAS; Trounson et al., 2016). Workplace adversity includes seven subscales: perceived environmental threat (seven items), environmental unpredictability (five items), need for vigilance (four items), expectation of workplace trauma (five items), work-life separation (five items), inability to achieve respite at work (five items), and preoccupation with negative consequences of one’s actions (five items). Sample items include I believe that my working environment is one that leaves me susceptible to harm (environmental threat), in my working environment it is hard to know what will happen next (environmental unpredictability), I believe that in my working environment I need to be constantly aware of my surroundings (need for vigilance), in my working environment you need to be prepared to see things that might be difficult to deal with (expectation of workplace trauma), I find that even when I leave work it still seems to be on my mind (work-life separation), when at work it is hard to relax (inability to achieve workplace respite), and I believe that in my working environment my actions can often result in serious consequences (action-consequence). Responses ranged from 1 (Strongly disagree) to 7 (Strongly agree) and higher scores indicated higher levels of adversity. The WREAS has demonstrated adequate discriminant and convergent validity and high internal consistency in use with correctional officers (Trounson et al., 2016, 2019). This study generated an excellent Cronbach’s alpha of .96.
Workplace Belongingness
Workplace belongingness was assessed using six items from the original 18-item Psychological Sense of Organizational Membership (PSOM) scale (Cockshaw & Shochet, 2010). Sample items include the managers/supervisors here respect me, people in this organization are friendly to me, and people here notice when I’m good at something. Participants rated their sense of belongingness on a scale from 1 (not at all true) to 5 (completely true) with higher scores indicating higher belongingness. The six-item PSOM showed good internal consistency in this study (α = .89).
Resilience
The six-item Brief Resilience Scale (BRS; Smith et al., 2008) was used to assess trait resilience (i.e., general rather than dispositional resilience). Sample items include I tend to bounce back quickly after hard times, it does not take me long to recover from a stressful event, and I usually come through difficult times with little trouble. Responses range from 1 (strongly disagree) to 5 (strongly agree) where higher scores represent higher resilience. The BRS has shown convergent and divergent validity, discriminant predictive validity, and internal consistency (Smith et al., 2008) as confirmed by this study (α = .88).
Results
Preliminary Analyses and Descriptive Statistics
Data were analyzed using SPSS Version 27 (IBM Corp., 2020). Missing data were missing at random and were imputed using the maximum likelihood imputation method. Preliminary analyses (Supplementary Material) revealed no significant differences in burnout, well-being, or posttraumatic growth based on gender, prior frontline work experience, ethnicity, relationship status, educational attainment, security level, and prison resident sex. Therefore, these variables were excluded from primary analyses to maximize power. As seen in Table 1, demographics like age, tenure, hours worked, and critical incident severity were often not significantly correlated with the dependent variables and were therefore excluded from primary analyses to maximize power. There were no breaches of the linearity, homoscedasticity, and multivariate normality assumptions.
Correlation Matrix and Descriptive Statistics
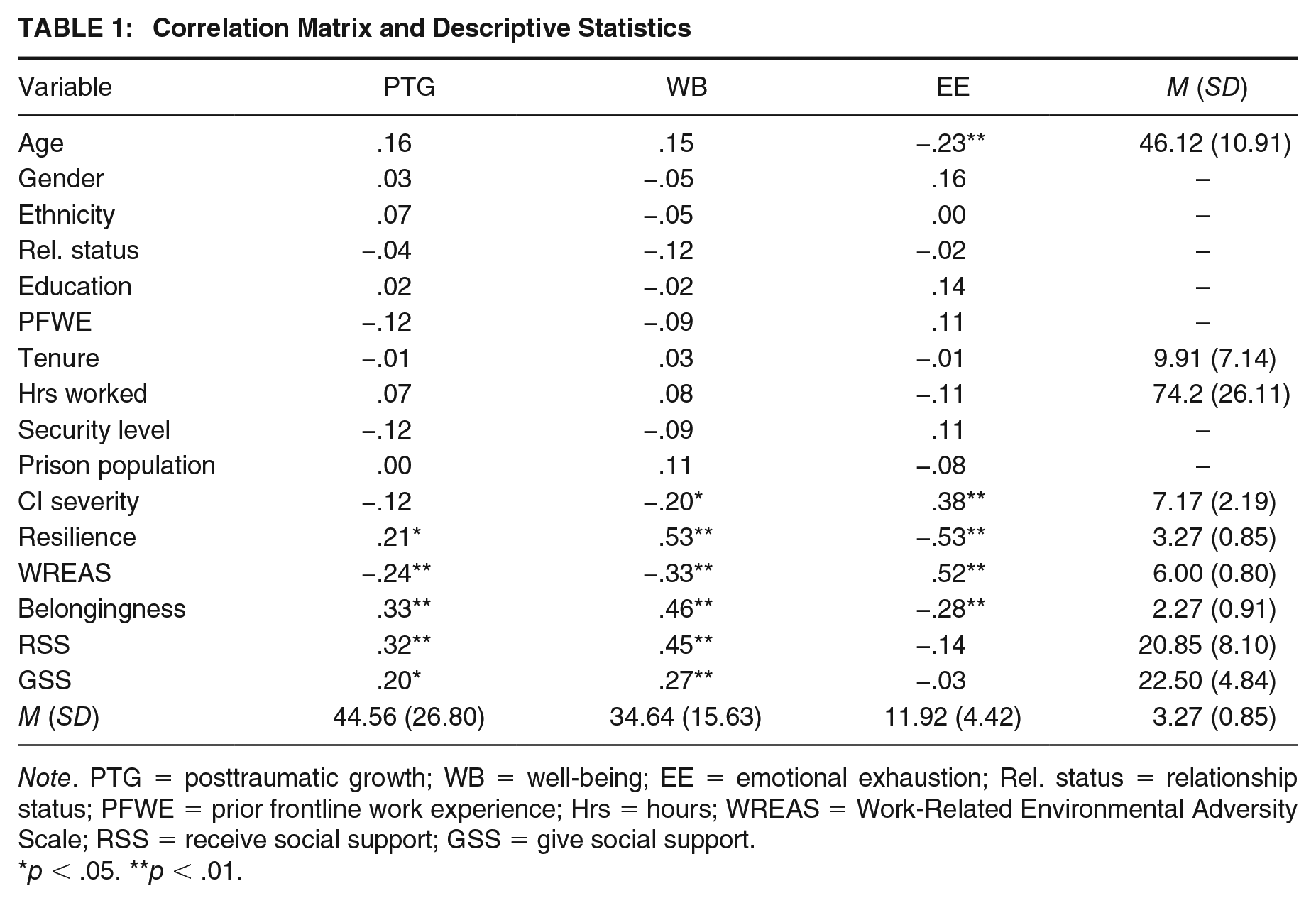
Note. PTG = posttraumatic growth; WB = well-being; EE = emotional exhaustion; Rel. status = relationship status; PFWE = prior frontline work experience; Hrs = hours; WREAS = Work-Related Environmental Adversity Scale; RSS = receive social support; GSS = give social support.
p < .05. **p < .01.
The descriptive statistics displayed in Table 1 show that participants had high emotional exhaustion, moderate well-being, and low-to-moderate posttraumatic growth. Emotional exhaustion scores were higher than those of medical professionals (M = 8.65; Riley et al., 2017), posttraumatic growth scores were lower than a previous sample of correctional officers (M = 57.4; Tatebe et al., 2020), and well-being scores were comparable with those of a sample of police officers (M = 32.6; Harnett et al., 2023). Average workplace adversity scores were slightly higher than a previous sample of correctional officers (M = 5.36; Trounson et al., 2016), and workplace belongingness scores were lower than disability service personnel (M = 3.81; Cockshaw & Shochet, 2010) and paramedics (M = 3.48; Shakespeare-Finch & Daley, 2017). Resilience scores were comparable with those of frontline groups (M = 3.68; Shakespeare-Finch & Daley, 2017), as were giving (M = 21.79) and receiving (M = 22.78) social support scores (Shakespeare-Finch et al., 2019). The social support scores suggest the current sample felt they gave more support than they received, contrasting prior frontline samples where this pattern was reversed (e.g., Armstrong et al., 2014).
Predicting Burnout
The overall burnout model was significant with independent variables together explaining 48.6% of the variance in emotional exhaustion, R2 = .486, F(9, 128) = 13.43, p < .001. As displayed in Table 2, age and trait resilience were significant negative predictors of emotional exhaustion, uniquely explaining 2% and 4% of variance respectively. Higher age and higher resilience were significantly associated with lower levels of emotional exhaustion. Environmental adversity was a significant positive predictor of emotional exhaustion such that higher environmental adversity was associated with higher emotional exhaustion, and uniquely explained 5% of the variance. Other variables were not significant individual predictors of emotional exhaustion.
Multiple Regression Analyses Predicting Emotional Exhaustion, Well-Being, and Posttraumatic Growth
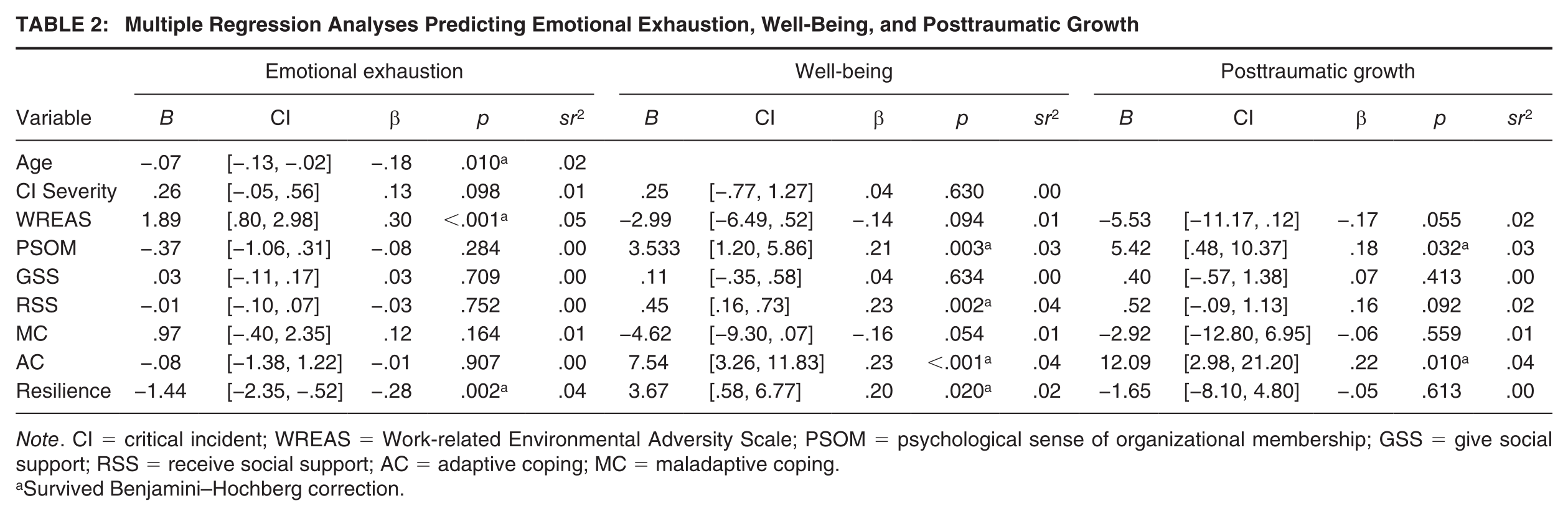
Note. CI = critical incident; WREAS = Work-related Environmental Adversity Scale; PSOM = psychological sense of organizational membership; GSS = give social support; RSS = receive social support; AC = adaptive coping; MC = maladaptive coping.
Survived Benjamini–Hochberg correction.
Predicting Well-Being
The overall well-being model was significant with the independent variables together predicting 50.1% of the variance in well-being, R2 = .501, F(8, 132) = 17.20, p < .001. As seen in Table 2, workplace belongingness, receiving social support, adaptive coping, and trait resilience were significant positive predictors of well-being, uniquely explaining between 2% and 4% of the variance in well-being. A higher sense of workplace belongingness, higher receipt of social support, higher use of adaptive coping strategies, and higher levels of resilience were associated with higher well-being. Critical incident severity, environmental adversity, giving social support, and maladaptive coping did not significantly predict well-being.
Predicting Posttraumatic Growth
The overall model was significant with the independent variables together predicting 22.9% of the variance in posttraumatic growth, R2 = .229, F(7, 134) = 5.68, p < .001. As displayed in Table 2, workplace belongingness and adaptive coping were significant positive predictors of posttraumatic growth, uniquely explaining 3% and 4% of the variance in posttraumatic growth respectively. A higher sense of workplace belongingness and high use of adaptive coping strategies were associated with higher levels of posttraumatic growth. Other variables were not significant individual predictors of posttraumatic growth.
Discussion
This study aimed to explore predictors of correctional officer health across the health continuum. The descriptive data suggested that the correctional officers showed poorer mental functioning, including higher emotional exhaustion and lower levels of posttraumatic growth, compared to other frontline samples. Resistance resources found to support correctional officer well-being and/or posttraumatic growth included a sense of workplace belongingness, the use of adaptive coping strategies, trait resilience, and social support.
Burnout
The model of burnout was significant and explained 48.6% of the variance in emotional exhaustion. Prior studies of correctional officer burnout have explained between 23% and 59% of the variance (Burhanullah et al., 2022; Griffin et al., 2010). Hence, the inclusion of novel predictors explained more variance than some prior models. The findings supported prior literature which found that demographic variables (e.g., gender and ethnicity) were not associated with officer burnout (Lambert et al., 2015). One notable exception was age which significantly negatively predicted burnout. This inverse relationship is supported by some prior research (e.g., Burhanullah et al., 2022); however, most prior research has found no significant association (e.g., Choi et al., 2020).
It was hypothesized that protective factors would negatively predict burnout and resilience did negatively predict burnout. Resilience has been underresearched in correctional officers, but the available data supports the current findings (e.g., Klinoff et al., 2018). Opposing the hypothesis, workplace belongingness did not significantly predict burnout. Workplace belongingness is yet to be examined in relation to correctional officer burnout. However, prior research has found variables indicative of a sense of belongingness including organizational support (Gao et al., 2022), collegial cohesion (Isenhardt et al., 2019) and trust in superiors (Lambert et al., 2012) to be protective against burnout. The average workplace belongingness score of the current sample was lower than other frontline samples where workplace belongingness reached significance as a predictor of depression (Cockshaw & Shochet, 2010) and distress (Shakespeare-Finch & Daley, 2017). This low score may explain why workplace belongingness failed to achieve significance in this study.
Social support failed to predict officer burnout. The relationship between the receipt of social support from loved ones and symptoms of pathology in correctional officers is ambiguous with some studies finding a significant negative association (e.g., Isenhardt et al., 2019) and others finding no association (e.g., Harvey, 2014). The findings of this study support the latter, suggesting that social support from friends and family is not protective when attempting to cope with work-related burnout. The provision of social support has yet to be examined in correctional officers; however, research into other high-risk occupations supports the findings that giving social support is not protective against pathology (e.g., Shakespeare-Finch et al., 2015). Adaptive coping also failed to predict burnout. The relationship between adaptive coping and burnout is ambiguous as some strategies classified as adaptive by this study are more protective than others. For example, Gould et al. (2013) found that problem-focused strategies like action coping and planning were significant negative predictors of officer emotional exhaustion while emotion-focused strategies including acceptance, humor, and positive reframing were not associated with emotional exhaustion. This differential protective effect for adaptive coping strategies has been corroborated for officer PTSD symptoms (Hughes-Taylor & Swartz, 2021).
It was further hypothesized that workplace adversity and maladaptive coping would positively predict burnout. Environmental adversity scores significantly positively predicted officer burnout. Environmental adversity (and related variables like perceived threat) has previously been positively associated with correctional officer stress, depression, anxiety, and burnout (Hu et al., 2015; Trounson et al., 2016, 2019). Environmental adversity may lead to burnout due to the need to remain hypervigilant to danger. Maladaptive coping failed to reach significance in predicting correctional officer burnout. The findings regarding the relationship between burnout and coping strategies classed as maladaptive remains mixed (e.g., Gould et al., 2013; Hughes-Taylor & Swartz, 2021) suggesting further research is needed.
Well-Being
The overall model of correctional officer well-being was significant with the predictors together explaining 50.1% of the variance. Well-being as operationalized by this study has not previously been measured in correctional officers; however, prior models of correctional officer life satisfaction have explained between 6% and 44% of variance (Lambert, 2008; Lambert et al., 2009). Therefore, this study explained more variance in well-being than prior studies by including novel predictors and measuring well-being more comprehensively. The hypothesis that protective factors would positively predict well-being was partially supported by the data. Adaptive coping was a significant positive predictor of officer well-being corroborating prior research with diverse samples (e.g., Fischer et al., 2021). The receipt of social support significantly and positively predicted officer well-being supporting prior research with diverse populations (e.g., Biswas et al., 2022). However, research with other frontline groups has found that support from diverse sources was differentially protective (Lowery & Cassidy, 2022). Thus, further exploration on sources of support and officer well-being could be enlightening. Workplace belongingness and resilience also significantly predicted officer well-being. The relationships between workplace belongingness, resilience, and correctional officer well-being have not previously been explored; however, workplace belongingness and resilience have each been significantly linked to indicators of well-being in other frontline groups (e.g., Huynh et al., 2014; Shakespeare-Finch & Daley, 2017).
Contrary to the hypothesis, the provision of social support did not significantly predict correctional officer well-being. This contrasts prior research which found correctional officers drew satisfaction from supporting prison residents (Miller et al., 2022, 2023) and that providing support significantly predicted well-being in emergency medical dispatchers (Shakespeare-Finch et al., 2015). However, this study assessed officers’ provision of support to loved ones rather than prison residents. Officers may have depleted their resources from providing support to prison residents such that the provision of support to others felt burdensome rather than beneficial. Another potential explanation is that the imbalance in perceived receipt and provision of support negated any potential benefits of providing support (Wang & Gruenewald, 2019). Maladaptive coping and workplace adversity also did not predict well-being. Contradicting the current findings, prior research with diverse samples has found a significant negative relationship between maladaptive coping and well-being (e.g., Fischer et al., 2021). However, maladaptive coping was approaching significance (p = .054) and the nonsignificant finding may have been due to low power. Similarly, prior research has found a significant negative association between environmental adversity and correctional officer thriving (Trounson et al., 2019) or a significant positive association between perceived danger and officer life satisfaction (Lambert et al., 2005).
Posttraumatic Growth
The model was significant with predictors collectively explaining 22.9% of the variance in posttraumatic growth. Adaptive coping significantly predicted posttraumatic growth, as supported by the findings of a meta-analysis of 103 posttraumatic growth and benefit finding studies which found a significant positive association between adaptive coping and growth (Prati & Pietrantoni, 2009). Similarly, workplace belongingness was a significant positive predictor of posttraumatic growth as supported by prior research (e.g., Armstrong et al., 2016). Resilience was not a significant predictor of posttraumatic growth. The relationship between resilience and posttraumatic growth is contentious, with some studies finding a significant positive relationship, some finding no relationship, and others finding an inverse relationship (see Henson et al., 2021, review). Further complicating this is the variation in operationalization and measurement of resilience as a trait, a process, or an outcome. The lack of a significant relationship between resilience and posttraumatic growth found in this study may be because resilient people tend to struggle less with adversity, meaning they are less likely to engage in the meaning-making behaviors that promote posttraumatic growth (Westphal & Bonanno, 2007).
Giving and receiving social support also did not predict posttraumatic growth. Receiving social support is theorized to promote self-disclosure and subsequently posttraumatic growth (Tedeschi et al., 2018); however, research findings remain mixed. For example, some have found a significant positive association between received social support and posttraumatic growth (e.g., Shakespeare-Finch et al., 2015) and others have found no relationship (e.g., Armstrong et al., 2014; Shakespeare-Finch et al., 2019). Similarly, findings relating to the provision of social support and posttraumatic growth is mixed with some studies finding a positive association (e.g., Shakespeare-Finch et al., 2019) and others finding no association (e.g., Armstrong et al., 2014).
Environmental adversity and maladaptive coping did not significantly predict posttraumatic growth. Environmental adversity and posttraumatic growth have not previously been simultaneously assessed though perceived danger was found to be significantly associated with posttraumatic growth in a sample of veterans (Dyball et al., 2022). However, environmental adversity was approaching significance (p = .055) and therefore this nonsignificant finding may have been due to low power. Maladaptive coping does not encourage meaning-making practices that promote posttraumatic growth; however, the relationship between maladaptive coping and posttraumatic growth remains unclear. For example, some research has found a significant inverse relationship between the two variables (e.g., Kalaitzaki et al., 2023), some has found no relationship (e.g., Kirby et al., 2011), and others have found a positive relationship (e.g., Isguder et al., 2018). Specific maladaptive coping strategies may have different relationships with posttraumatic growth.
Implications, Strengths, and Limitations
The results of this study can guide interventions that act to improve correctional officer well-being and prevent burnout. As workplace belongingness was a significant predictor of well-being and posttraumatic growth and is malleable to change, interventions that aim to enhance belongingness are likely to be effective. Strategies to improve workplace belongingness include team building activities and improved supervisory support. Prior research has suggested psychoeducation for correctional officers (e.g., Senol-Durak et al., 2021) and this study argues that such training could be expanded to cover well-being and posttraumatic growth. Such training should support the development of resilience and adaptive coping strategies which significantly predicted well-being. Finally, receipt of social support from loved ones significantly predicted well-being, implying that resources for friends and families of officers on supporting their loved one may be beneficial.
This study expanded prior literature which did not explore predictors of correctional officer posttraumatic growth (Tatebe et al., 2020). It comprehensively measured well-being extending prior research which has predominantly operationalized correctional officer well-being as life satisfaction only (Miller et al., 2022). And finally, this study explored correctional officer health across the health continuum compared to prior research which has predominantly adopted a pathogenic lens. This study provided insight into the health and well-being of correctional officers by showing that they exhibited higher levels of emotional exhaustion, moderate well-being, and lower posttraumatic growth in comparison other frontline groups. These data provide a more holistic understanding of correctional officer health which can then more effectively guide health promotion strategies.
Nonetheless, there were some limitations to this study. Burnout was operationalized as emotional exhaustion only, ignoring the depersonalization and personal accomplishment components. However, prior research on correctional officers has similarly focused on emotional exhaustion (e.g., Clements & Kinman, 2021) as it is considered the first component of burnout (Toppinen-Tanner et al., 2002). The generalizability of the results may be limited as most of the sample were high security officers (92.3%) working with male prison residents (78.9%). Thus, future research should aim to elucidate whether differences exist between low-, medium-, and high-security officers and officers working with male and female prison residents by recruiting a larger, more diverse sample. Finally, the cross-sectional nature of the data prevented causal conclusions from being drawn.
Conclusion
This study used a salutogenic framework to explore the health continuum in a sample of correctional officers. It was the first study to comprehensively explore posttraumatic growth and well-being in correctional officers and provided important information about their predictors. Potentially malleable factors like coping strategies, the receipt of social support, and a sense of workplace belongingness were significantly related to correctional officer health outcomes and may act as targets for health promotion interventions.
Supplemental Material
sj-docx-1-cjb-10.1177_00938548241233932 – Supplemental material for Predicting Burnout, Well-Being, and Posttraumatic Growth in Correctional Officers
Supplemental material, sj-docx-1-cjb-10.1177_00938548241233932 for Predicting Burnout, Well-Being, and Posttraumatic Growth in Correctional Officers by Olivia Miller, Jane Shakespeare-Finch and Dagmar Bruenig in Criminal Justice and Behavior
Footnotes
Correction (August 2024):
Article has been updated online to correct a typographical error in Table 2.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.