
Abstract
This study examined whether there would be significant group-level and reliable individual changes in psychopathy measured via the Psychopathy Checklist–Revised (PCL–R) and the Interpersonal Measure of Psychopathy (IM–P) scores in a sample of 187 adult individuals with violent and sexual offense histories incarcerated and treated in a German social therapy facility (STF). Measurements were taken at entry into the STF and at (most) an 18-month follow-up. The results of dependent t-tests were significant, showing significant reductions in PCL–R and IM–P scores. Stronger significant reductions were observed for PCL–R Factor 1 scores and its corresponding facets compared with Factor 2 scores. Reliable individual changes measured via the Reliable Change Index (RCI) showed improvements in PCL–R and IM–P scores for some participants.
Psychopathy is defined as a clinical construct consisting of interpersonal, affective, lifestyle and antisocial traits and behaviors according to the Psychopathy Checklist–Revised (PCL–R; Hare, 2003). Historically, the differentiation between primary and secondary psychopathy is an intensively discussed issue in the research about and the clinical work with psychopathy. According to Lykken (1995), primary psychopathy is primarily characterized by fearlessness and a relatively weak reactivity to emotional stimuli and social cues, whereas secondary psychopathy is by contrast characterized by relatively high levels of positive and negative emotionality, impulsiveness, and sensation seeking. Several researchers and studies have examined this differentiation and have provided evidence for its relevance in (sub-)clinical and forensic samples and settings (Newman et al., 2005; Vaughn et al., 2009). Similarly, and closely related to the first issue, the discussion about categorical or dimensional concepts of psychopathy has been accompanying the scientific and clinical work regarding psychopathy into the present day (Coid & Yang, 2008; Yildirim & Derksen, 2015).
When it comes to treating incarcerated individuals with psychopathic personality traits in forensic settings, the existing literature has historically been pervaded by clinical pessimism, beginning with Cleckley (1988), and most famously propagated by Rice et al.’s (1992) infamous Oak Ridge treatment program study, where treatment was shown to increase the recidivism rates for incarcerated individuals with psychopathic personality traits. However, the past few years have produced a growing body of literature indicating that incarcerated individuals with psychopathic personality traits might be treatable after all (D’Silva et al., 2004; Lewis, 2018; Olver, 2018; Olver & Wong, 2009; Polaschek, 2014; Salekin et al., 2010). Due to their increased risk of recidivism (Brunner et al., 2019), these individuals present a high-risk (and potentially a high-need) group of patients according to the Risk-Need-Responsivity (RNR) Model (Andrews & Bonta, 2010), making them “prime targets” (Larsen, 2019, p. 257) for treatment.
Results from previous studies have indicated that incarcerated individuals with psychopathic personality traits could mostly benefit from multimodal treatment programs (Olver, 2018; Simourd & Hoge, 2000). Olver (2018) summarized effective treatment programs for these individuals as “broadly CBT-based” (p. 302) and appropriately intense for a high-risk group while simultaneously targeting their criminogenic needs according to the RNR model (Andrews & Bonta, 2010). Furthermore, they should include a high level of involvement of specially trained staff alongside “supervision and monitoring” (Olver, 2018, p. 302) of the incarcerated individuals with psychopathic personality traits. However, extending these established treatment methods to include insight-oriented approaches such as psychoanalysis increased the success rate of treatment programs for these individuals (Salekin, 2002), highlighting the importance of challenging unhelpful thoughts and increasing the incarcerated individual’s self-awareness during treatment (Lewis, 2018). Specific foci should additionally be placed on deficits in emotional understanding and information processing (Lösel, 1998). Even authors in favor of the management of incarcerated individuals with psychopathic personality traits have agreed that treatment could be effective if it were implemented as a high-intensity program that mirrors established treatment programs for regular offenders, including CBT alongside relapse prevention, anger management, prosocial modeling, and motivational interviewing (Harris & Rice, 2006). Integrating these approaches into an effective treatment program might be the key to treating incarcerated individuals with psychopathic personality traits, thereby reducing their risk of sexual and violent recidivism, as previous, similar programs have already done (Olver & Wong, 2009).
Interestingly, past studies on the treatment of incarcerated individuals with psychopathic personality traits have mostly focused on their recidivism rate as an outcome. However, it is still unclear if the implied treatments reduce recidivism rates due to the change in psychopathic characteristics or due to other criminogenic characteristics (Polaschek, 2014). In addition, psychopathy has often been treated as a responsivity factor, meaning it is an attribute moderating the achievement of treatment targets (Hildebrand & de Ruiter, 2012), and not a treatment target itself. As a result, evidence for the effectiveness of treating psychopathic personality traits has been lacking (Wilson & Tamatea, 2013). However, traits in other personality disorders have been shown to change through treatment (Roberts et al., 2017), indicating that changes in psychopathic personality traits through treatment might be possible (Wong et al., 2012). This would imply that psychopathy might be more of a dynamic risk factor than previously assumed (Miller, 2006) and that it should not be treated as a responsivity factor but rather as a criminogenic need (Andrews & Bonta, 2010).
Social-Therapeutic Treatment in Germany
Social therapy facilities (STFs) in Germany are meant to provide treatment and social support to people who have been sentenced due to considerable or repeated offenses and who are in danger of reoffending (Arbeitskreis Sozialtherapeutische Anstalten im Justizvollzug e.V., 2016). STFs combine psychotherapeutic, educational, and occupational approaches in an integrative concept, which is meant to include the environment of individuals who offend both in- and outside the STF while establishing a therapeutic community inside the STF (Wischka & Specht, 2001). This concept is applied through various offers including individual and group therapy, education, and vocational training. Overall, STFs aim to reduce the risk of recidivism for individuals who offend and improve their interpersonal and social skills.
All STFs feature an individually defined treatment plan that is updated regularly (Moosburner et al., 2022b). This plan determines the STFs treatment options and usually includes a therapeutic focus. Moosburner et al. (2022b) analyzed the treatment options available in German STFs in 2019, with results revealing a conceptual focus on cognitive-behavioral therapy with additional psychodynamic and schema therapy. Furthermore, individuals who offend received an average of 4 hours of therapy per week, which was administered by specially trained staff. These results indicate that the integrative concept used for treatment in STFs is already in line with Olver’s (2018) suggestions for the treatment of incarcerated individuals with psychopathic personality traits. Consequently, social-therapeutic treatment, as has been implemented in STFs in Germany, could be effective in reducing psychopathic traits, indicating that psychopathy might in fact be malleable and potentially a dynamic risk factor. This study aimed to analyze participants’ changes in PCL–R and Interpersonal Measure of Psychopathy (IM–P) scores while attending a multimodal STF treatment. Measurements were taken at entry into the STF and an (at most) 18-month follow-up measurement.
Method
Procedure
This study was part of the extensive research project “Evaluation of the Social-Therapeutic Correctional Facility Hamburg” (Brunner et al., 2016), which has been conducted by the Institute for Sex Research, Sexual Medicine, and Forensic Psychiatry at the University Medical Center Hamburg since 2010. The research project is authorized and funded by the Ministry of Justice of the Hanseatic City of Hamburg, Germany. All participants were informed of the study’s purpose and gave written consent for their participation in accordance with the Declaration of Helsinki. Approval for the study was granted by the ethical committee of the Hamburg Chamber of Psychotherapists.
The design of this current study was a within-subject, pre-post comparison of measures of psychopathy for individuals with violent and sexual offense histories. Pre-treatment measurements were conducted within the first weeks of admission into the STF by psychologists with official certification for administering the PCL–R and consisted of semi-structured interviews, information derived from case files, and observations of behavior in the interview. This is analogous to the clinical practice of risk assessment in most German correctional facilities. As these data were collected for an ongoing, extensive research project, raters were blind to the purpose of this specific study but aware of broader research goals associated with the data collection. None of the psychologists who conducted these measurements were involved in the treatment of this study’s participants. Regular follow-up measurements occurred on average after 18 months (M = 18.45, SD = 6.96) but were conducted shortly before release or relocation into a different facility if participants were treated for less than 18 months. Follow-up measures consisted of the same materials as pre-treatment measures and were mostly conducted by the same psychologists as pre-treatment measures, with only select exceptions.
Participants
The original sample consisted of 189 male individuals with sexual, violent, and other offense histories who were tested with both the PCL–R and IM–P at entry into the STF beginning December 2010 and took part in follow-up testing between December 2011 and May 2021. Participants were considered individuals with sexual, violent, or other offense histories based on the index offense that led to their incarceration and treatment in the STF. Descriptive analyses revealed two participants that showed strong increases (M = 7.5 points) in prorated PCL–R sum scores from measurement at entry to follow-up, which might have been due to a lack of information for items that were measured at entry into the STF. These increases over a short period of time (24 months) were considered outliers due to systematic bias (Mokros et al., 2017) and were subsequently excluded from any further group-level or individual analyses. The remaining 187 participants were aged between 21 and 68 years (M = 37.87, SD = 12.21) and consisted of 106 individuals with sexual, 64 individuals with violent, and 17 individuals with other offense histories.
Measures
Psychopathy Checklist–Revised
The PCL–R (Hare, 2003; German version Mokros et al., 2017) measures the clinical construct of psychopathy via 20 items on a 3-point scale (0, 1, or 2) with a maximum sum score of 40 points. The instrument possesses two intercorrelated factors with two underlying facets each. Factor 1 consists of interpersonal (Facet 1) and affective (Facet 2) deficits, while Factor 2 includes an impulsive lifestyle (Facet 3) and antisocial behavior (Facet 4). The PCL–R is commonly administrated using semi-structured interviews and available file information. Missing data or omitted items can be compensated using prorated scores (Mokros et al., 2017). While the structure of psychopathy assessed by the PCL–R is considered dimensional by modern research (Sellbom & Drislane, 2021), thresholds are adopted for research purposes. Scores between 0 and 16 are considered low, scores between 17 and 24 are assumed to be medium, and scores above 24 qualify as high. Mokros et al. (2014) calculated descriptive statistics (M = 21.30, SD = 7.60) for a sample of 1,046 Austrian male individuals with sexual offense histories with an internal consistency of α = .84. In addition, Mokros et al. (2014) also report descriptive statistics and internal consistencies for the Factors and Facets of the PCL–R. Generally, a large body of literature supports the reliability and validity of the PCL–R (e.g., Hare et al., 2000).
Interpersonal Measure of Psychopathy
The IM–P (Kosson et al., 1997; German version Endres, 2005) is an observational measure consisting of 21 items with the purpose of quantifying the interpersonal interactions occurring during PCL–R interviews. The measure shows positive correlations with all PCL–R facets and a 17-item, 3-factor structure (Dominance, Grandiosity, and Boundary Violations) fit a sample of American inmates (Vitacco & Kosson, 2010). The instrument measures the frequency of certain nonverbal behaviors and interactions on a scale of 1 (behavior did not describe interaction with participant at all) to 4 (behavior described interaction with participant perfectly), for a maximum total score of 48. Zolondek et al. (2006) reported descriptive statistics (M = 7.37, SD = 7.14) for a sample of 93 North American inmates. Internal consistencies for the IM–P range from α = .89 (Zolondek et al., 2006) to α = .91 (Kosson et al., 1997). Although the IM–P is supposed to be administered by an independent observer, both PCL–R and IM–P were rated by the same raters in the present data, which may have led to bias and overestimation of certain items (Yoon et al., 2022).
Analyses
All analyses were conducted using the IBM SPSS Statistics 23 and Microsoft Excel 2016 software and were divided into correlations, linear mixed model (LMM), and dependent t-tests as well as analyses of reliable individual change. Since incarcerated individuals with high psychopathic personality traits drop out of treatment in STFs at high rates due to poor treatment response, low motivation, and disruptive behaviors (Brunner et al., 2019), it was assumed that the present sample would not contain many individuals who offend that would be considered high psychopathy by traditional European research thresholds (PCL–R ≥25). Exploratory analyses confirmed that only 20 participants in the present sample could be considered high psychopathy within this definition. Therefore, this study utilized the entire sample of 187 participants to retain the statistical power needed for the analyses. As the PCL–R and IM–P ratings were conducted by the same rater and the IM–P’s purpose is to provide additional information in a PCL–R interview, a certain overlap can be assumed between measures in this study. Therefore, Pearson correlations were calculated between prorated PCL–R and IM–P sum scores for measurements at entry and at follow-up. Results showed a strong correlation between adjusted PCL–R and IM–P sum scores at entry, r(185) = .55, p < .001 and at follow-up r(173) = . 49, p < .001.
Correlations
Pearson product–moment correlations were used to investigate the relationship of participants’ change over the course of treatment with their prorated PCL–R and IM–P scores at entry as well as their age. Therefore, a change score was calculated by subtracting the participant’s follow-up measurement scores from their scores at entry. This was done for the prorated PCL–R sum score as well as its prorated factor and facet scores and the IM–P score. Effect sizes were interpreted according to Cohen (1988), with 0.10, 0.30, and 0.50 seen as small, moderate, and large effect sizes, respectively.
LMM Analyses
We ran LMM analyses with the prorated PCL–R sum scores, including factor and facet scores as well as the IM–P sum score as dependent variables, and added a fixed effect for time and the participants’ age. Participant was included as a random effect. Our models utilized the restricted maximum likelihood (REML) approach and applied Satterthwaite’s method to estimate degrees of freedom and generate p-values.
Dependent t-Tests
Prerequisites were inspected for the calculation of dependent t-tests, which were used to analyze the change of prorated PCL–R scores and its factors and facets scores as well as the sum score for the IM–P from measurement at entry to follow-up within different groups. Outliers that violated the standard normal distribution were excluded from further analyses. Effect sizes were reported as Cohen’s d, with effect sizes above 0.20, 0.50, and 0.80 seen as small, moderate, and large (Cohen, 1988). To counteract any errors due to multiple testing, Bonferroni-Holm corrections were applied.
Reliable Change Index
To investigate whether any observed changes in the within-subject dependent t-tests were reliable on an individual level, the Reliable Change Index (RCI) (Jacobson & Truax, 1991) was calculated for the prorated PCL–R sum score and that of its factors and facets as well as for the IM–P sum score. This allowed an analysis of whether each individual improved, deteriorated, or remained unchanged compared with the baseline (Wise, 2004). The RCI was calculated using Jacobson and Truax’s (1991) formula
with x2 representing the individual’s measurement at follow-up and x1 representing the individual’s measurement at entry. SD0 refers to the standard deviation of the measure in a normative sample and α signifies the test–retest reliability of the measure. If the resulting RCI scores are ±1.64, which represents a 1-sided 95% confidence interval, reliable change can be assumed (Wakeling et al., 2013; Wise, 2004). More specifically, scores larger than 1.64 can be seen as reliable improvements, while scores smaller than −1.64 can be interpreted as reliable deteriorations within the 95% confidence interval. Consequently, scores between −1.64 and 1.64 indicate that no reliable change has occurred. For ease of interpretation in this study, reliable improvements (RCI > 1.64) were referred to as Improved, reliable deteriorations (RCI < −1.64) were referred to as Deteriorated, and scores between −1.64 and 1.64 were referred to as Unchanged. Standard deviations and internal consistencies/intraclass correlations from the study by Mokros et al. (2014) were used to calculate the RCIs for the PCL–R and its factors and facets (N = 1.046). The RCI for the IM–P was calculated using the standard deviation and intraclass correlations of the sample described in Zolondek et al.’s (2006) study (N = 93).
Results
Changes in PCL–R Scores: Aggregate Sample
Table 1 shows results for all N = 187 participants, which indicated a significant reduction in prorated PCL–R sum scores from measurement at entry into the STF to measurement at follow-up.
Results of Dependent t-Tests Examining the Reduction of Prorated PCL–R Sum Scores for Different Groups
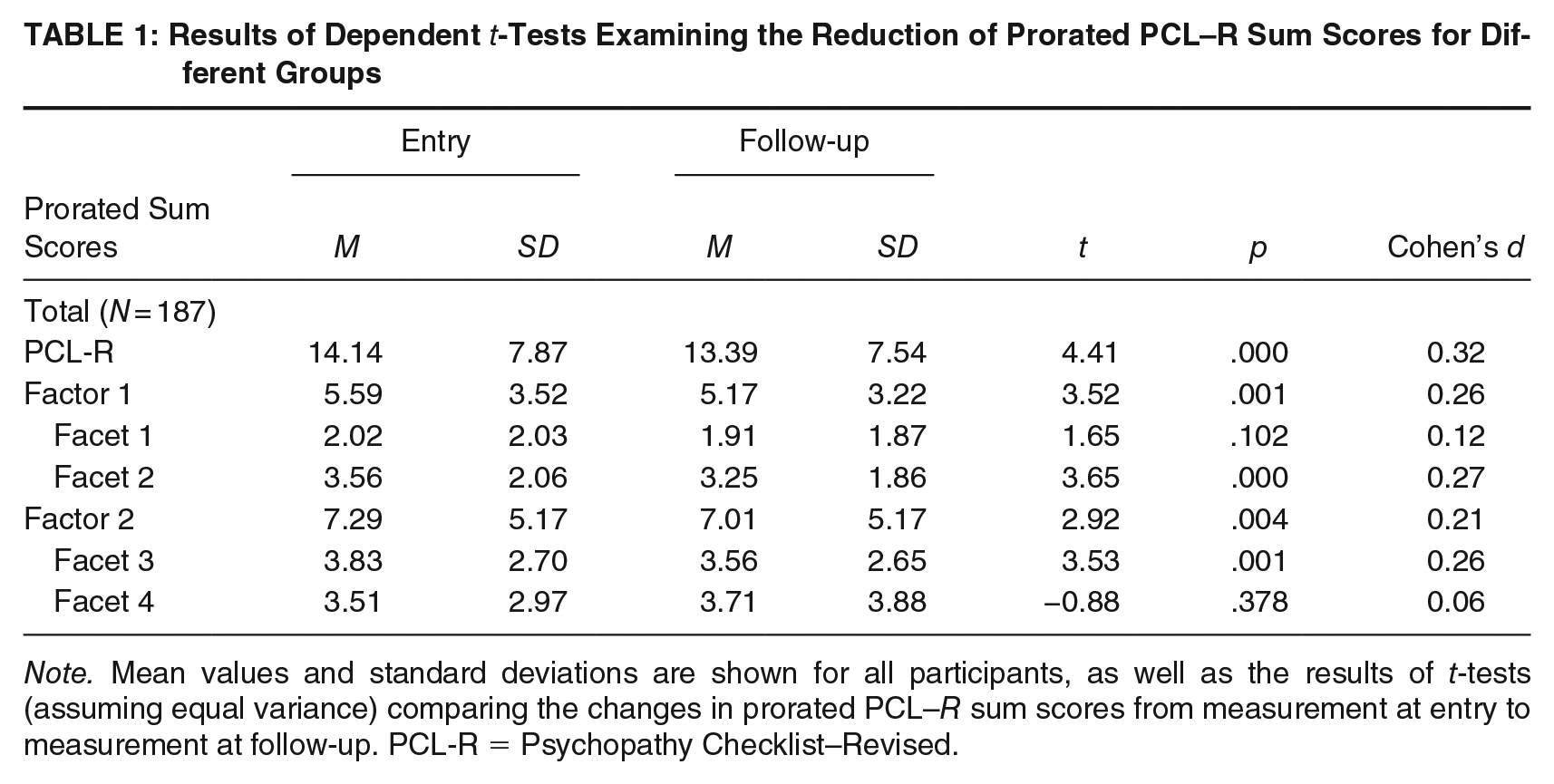
Note. Mean values and standard deviations are shown for all participants, as well as the results of t-tests (assuming equal variance) comparing the changes in prorated PCL–R sum scores from measurement at entry to measurement at follow-up. PCL-R = Psychopathy Checklist–Revised.
To inspect whether participants with higher pre-treatment scores would also show significantly more change over the course of treatment, prorated PCL–R measurements at entry were correlated with the participants’ PCL–R change scores. The results shown in Table 2 revealed a small positive correlation between a higher prorated PCL–R sum score at entry and participants’ PCL–R change scores, r(185) = .29, p < .001. This indicates that participants with higher PCL–R scores at entry showed more change over the course of treatment. The results of the LMM analysis are reported in Table 3 and indicate that significant change in prorated PCL–R sum scores occurred in part as a function of time.
Correlations Between PCL–R and IM–P Change Scores and Entry Scores and Age
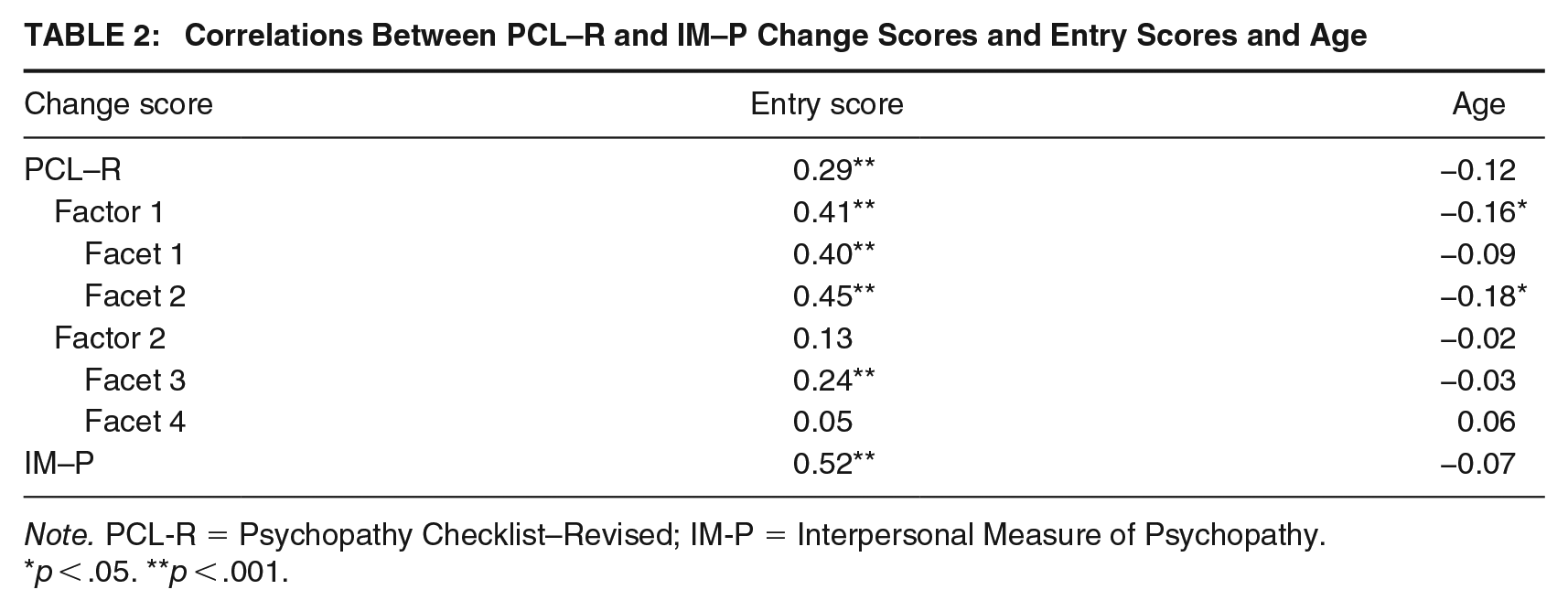
Note. PCL-R = Psychopathy Checklist–Revised; IM-P = Interpersonal Measure of Psychopathy.
p < .05. **p < .001.
Results of the LMM Model Testing the Effect of Time and Age on Prorated PCL–R and IM–P Sum Scores
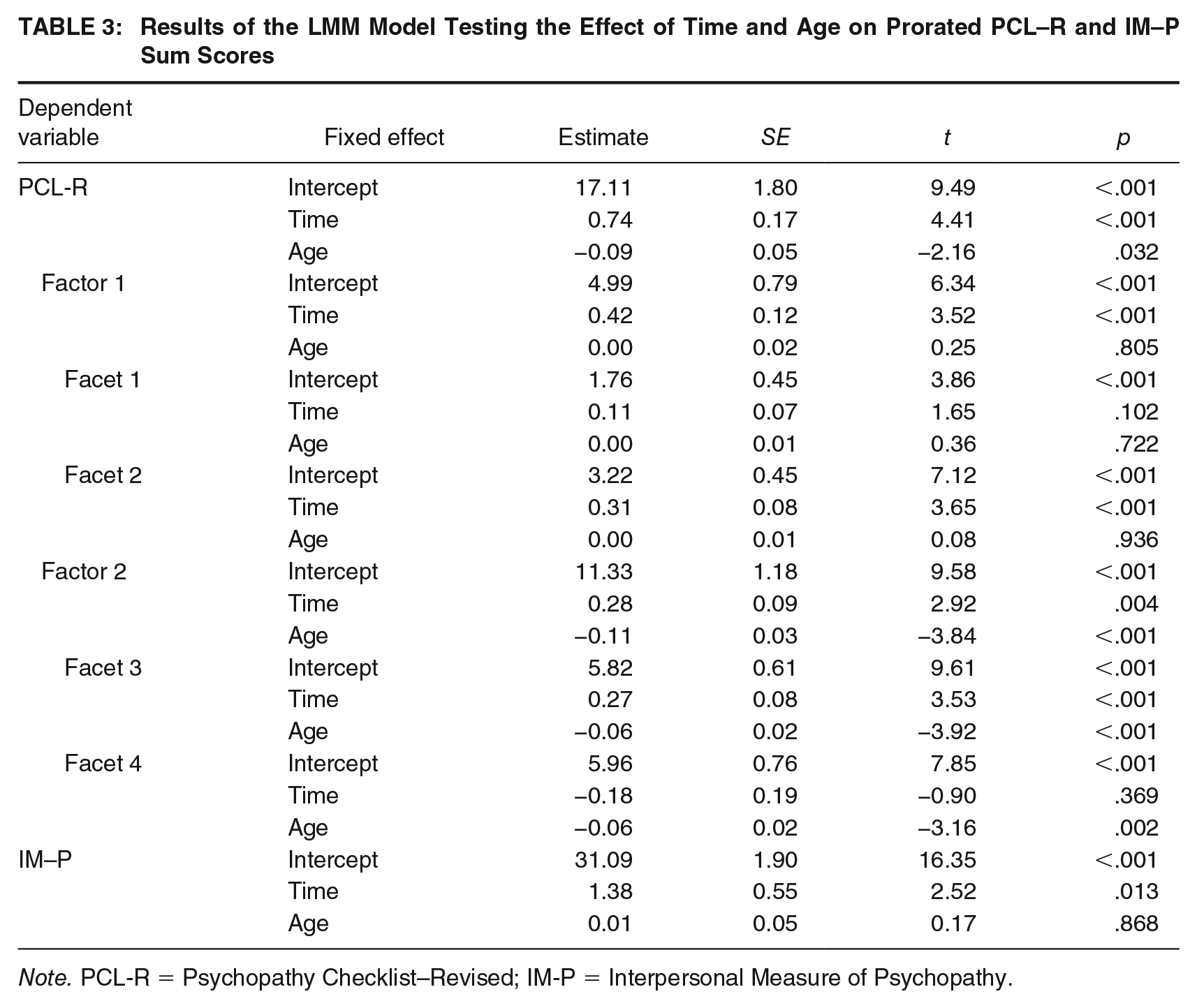
Note. PCL-R = Psychopathy Checklist–Revised; IM-P = Interpersonal Measure of Psychopathy.
Changes in PCL–R Factor and Facet Scores
Dependent t-tests were also conducted for the two underlying factors of the PCL–R and their four facets, to examine whether the reductions observed for the prorated PCL–R sum scores were attributable to specific changes in certain factors or their facets. Table 1 shows the results for all 187 participants. Overall, the results revealed a significant reduction in prorated Factor 1 PCL–R sum scores from measurement at entry to follow-up, with a small effect size. Prorated Factor 2 sum scores demonstrated a significant reduction, albeit with a slightly smaller effect size than Factor 1 sum scores. The results of LMM analyses are shown in Table 3. Overall, significant main effects of time were observed for Factor 1, Facet 2, Factor 2, and Facet 3.
Furthermore, to examine whether participants with higher pre-treatment factor and facet scores would also show significantly more change over the course of treatment, all prorated PCL–R factor and facet measurements at entry were correlated with the participants’ PCL–R factor and facet change scores. Results are shown in Table 2. There was a moderate positive correlation between prorated PCL–R Factor 1 scores at entry and the corresponding change scores, r(185) = .41, p < .001. Moderate positive correlations were also observed for the correlations between prorated Facet 1 and 2 scores at entry and their change scores, F1: r(185) = .40, p < .001; F2: r(185) = .45, p < .001. While there was a small positive correlation between prorated Factor 2 scores at entry and the corresponding change scores, r(185) = .13, p = .084, the correlation was not significant. This was also the case for the correlation of prorated Facet 4 scores and its change scores, r(177) = .05, p = .505. However, the small correlation between prorated Facet 3 scores and the corresponding change scores was significant, r(185) = .24, p = .001.
Changes in PCL–R Scores and Age
To inspect whether participants’ age played a role in their change in PCL–R scores during the treatment, correlations were calculated between the participants’ age at entry and their PCL–R change scores. The results shown in Table 2 revealed a small negative correlation between age and change on the prorated PCL–R sum score, r(185) = −.12, p = .099; however, the results were non-significant. These correlations were repeated for the change scores of the PCL–R factors and facets. A small significant negative correlation was observed between age Factor 1 change scores, r(185) = −.16, p = .025. Although the negative correlation between age and Facet 1 change scores was negligible, r(185) = −.09, p = .749 and non-significant, the correlation between age and Facet 2 change scores showed a significant small negative correlation, r(185) = −.18, p = .014, indicating that younger participants showed significantly more change on Facet 2 of the PCL–R over the course of treatment. Results for Facets 3 and 4 showed negligible correlations that were both non-significant; F3: r(185) = −.03, p = .705; F4: r(177) = .06, p = .463. As reported in Table 3, the results of the LMM analysis showed the main effects of age for the prorated PCL–R sum score as well as for Factor 2 and its facets, indicating that a younger age played a significant role in the change of these scores.
Changes in IM–P Scores: Aggregate Sample
The results of a dependent t-test with all n = 175 participants that were fully assessed with the IM–P at entry and at follow-up revealed a significant reduction of IM–P sum scores from measurement at entry (M = 33.21, SD = 9.08) to follow-up (M = 31.67, SD = 8.17), t(174) = 2.78, p = .006, d = 0.21, with a small effect size. To inspect whether participants with higher pre-treatment scores would also show significantly more change over the course of treatment, IM–P measurements at entry were correlated with the participants’ IM–P change scores. Table 2 results revealed a moderately large correlation between IM–P sum scores at entry and participants’ IM–P change scores, r(173) = .52, p < .001. This indicates that participants with higher IM–P scores at entry showed more change over the course of treatment. The results of the LMM analysis in Table 3 indicate that significant change in IM–P sum scores occurred in part as a function of time.
Changes in IM–P Scores and Age
To inspect whether participants’ age played a role in their change in IM–P scores during the treatment, correlations were calculated between the participants’ age at entry and their IM–P change scores. Results are shown in Table 2 and revealed a small negative correlation between age and change on the IM–P sum score, r(173) = −.07, p = .371; however, the results were non-significant. Table 3 results of the LMM analysis showed no significant main effect of age for changes in IM–P sum scores, supporting the assumption that age did not influence changes in IM–P sum scores.
RCI for the PCL–R Scores Including Factors and Facets
RCI analyses were conducted for the prorated PCL–R sum scores as well as the prorated sum scores of all factors and facets. Participants were then assigned the previously defined unchanged (U), improved (I), and deteriorated (D) categories via the cut-off score. Results for the prorated PCL–R sum score are reported in Table 4. Overall, most participants prorated PCL–R sum scores did not change reliably, but a small number of reliable improvements were observed. For Factors 1 and 2 of the PCL–R, most participants did not show any reliable change; however, improvements were more frequently found for Factor 1 across all variables. On the facet level, a lack of reliable individual change was also the norm. Nevertheless, improvements were observed for Facets 1 and 2, more so than for Facets 3 and 4. In fact, no reliable improvements were observed for Facet 4.
Frequencies of Prorated RCI Categories for Prorated PCL–R Sum Scores and IM–P Sum Scores
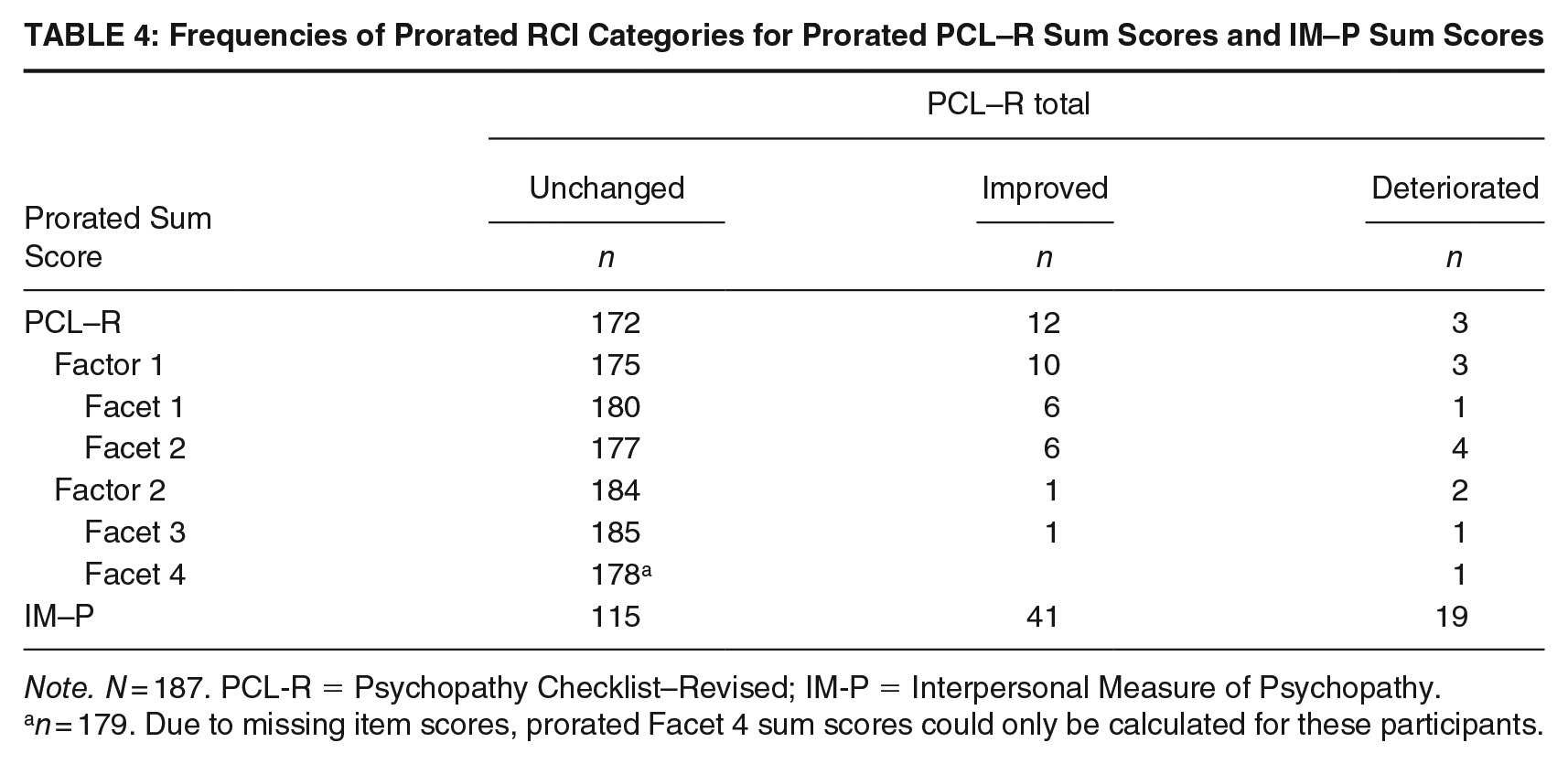
Note. N = 187. PCL-R = Psychopathy Checklist–Revised; IM-P = Interpersonal Measure of Psychopathy.
n = 179. Due to missing item scores, prorated Facet 4 sum scores could only be calculated for these participants.
RCI for the IM–P Scores
RCI analyses were also conducted for the IM–P sum scores and participants were assigned the unchanged (U), improved (I), and deteriorated (D) categories via the cut-off score. The corresponding results can be found in Table 4. While a lack of reliable individual change was also frequently observed for the IM–P sum scores, the ratio of no change to improvements was smaller than for the PCL–R results. However, this increase in observed improvements was accompanied by an increase in observed deteriorations as well.
Discussion
This study sought to examine whether psychopathic personality traits could be modified through treatment in an STF that targeted participants’ recidivism risk. Changes in prorated PCL–R and IM–P scores, including prorated PCL–R factor and facet scores, between two points of measurement were analyzed. To ensure that any observed significant changes were reliable on an individual level, the RCI was utilized. Dependent t-tests revealed significant reductions in prorated PCL–R and IM–P sum scores for the 187 participants over the course of their treatment in the STF. Significant moderate, positive correlations were found between the prorated PCL–R sum scores at entry and the corresponding change scores, indicating that individuals with higher PCL–R scores at entry also showed more significant change over the course of treatment. This correlation was also observed for the IM–P sum score at entry and its change score, highlighting a similar significant change over the course of treatment in the STF. These results were replicated for the PCL–R factors and facets, with Factor 1 scores (including Facets 1 and 2) showing stronger significant correlations compared with Factor 2 scores (including Facets 3 and 4). In addition, small inverse correlations were observed between the participants’ age and their PCL–R and IM–P change scores, indicating that younger participants showed greater change over the course of treatment. While these correlations did not reach significance, small significant inverse correlations were found between age and Factor 1 and Facet 2 of the PCL–R, highlighting that these aspects of psychopathy might be more malleable in younger participants. LMM analyses supported most of these findings, indicating that both time and age played a significant role in the observed changes for prorated PCL–R sum scores, although the estimates were small overall. However, for changes in IM–P sum scores, age did not play a significant role. Reliable individual changes measured via the RCI showed improvements for PCL–R and IM–P scores for some participants. The RCI results for the PCL–R factors and facets mirrored those of the group-level analyses, indicating that more improvements occurred for Factor 1 and its facets rather than Factor 2.
Group-Level Changes
The treatment provided by the STF, which targeted the participants’ recidivism risk, was shown to be effective in significantly reducing PCL–R and IM–P scores for this study’s participants, thereby implying that changes in psychopathic personality traits are possible. Furthermore, these significant reductions were observed after around 18 months of treatment, indicating that these changes were rapid. These results are a logical addition to past research, considering that the treatment program utilized in the STF, while not specifically designed to treat psychopathy, presents a high-intensity, multimodal approach that is in line with many of the suggestions for effective treatments of incarcerated individuals with psychopathic personality traits and follows RNR principles (Andrews & Bonta, 2010; Lewis, 2018; Lösel, 1998; Olver, 2018). Specifically, elements of the utilized cognitive-behavioral therapy with percentages of psychodynamic psychotherapy and schema psychotherapy (Moosburner et al., 2022b) might have succeeded in enhancing the participants’ critical thinking and victim awareness, thereby targeting their deficits in emotional understanding (Lösel, 1998), that are measured by the PCL–R. These approaches, paired with the high level of involvement by a variety of specially trained staff such as psychotherapists and social workers in the STF, might have been key for the observed significant reductions in psychopathic personality traits in the present study. However, at the same time, this study did not differentiate between individuals who offended with psychopathy (i.e., PCL–R ≥30; primary psychopathy) and individuals who offended with psychopathic traits (secondary psychopathy). As such, the results should be interpreted under the reduced validity of the sample for categorical psychopathy.
As part of analyses on the factor and facet levels of the PCL–R, the results revealed that the most significant changes occurred for Factor 1 and its interpersonal and affective facets, not for Factor 2 and its lifestyle and antisocial facets. This implies that the underlying traits on the interpersonal and affective facets, such as a lack of empathy, grandiosity, pathological lying, or a failure to accept responsibility, might have been affected by the integrative, multimodal STF treatment as a byproduct of the overall goal of reducing the participants’ recidivism risk and subsequently changed. Furthermore, the lack of change on the antisocial facet of the PCL–R is unsurprising, as four of the five items used to measure this facet are static and based on the offender’s history. Therefore, it might be of interest to analyze the one item on the antisocial facet which can change due to treatment (poor behavioral control) separately.
Reliable Individual Changes
This study relied on the standard deviations and internal consistencies of large dysfunctional samples (Mokros et al., 2014; Zolondek et al., 2006) to calculate the RCI. Results revealed multiple reliable individual changes for the entire sample, but most of the sample showed no reliable individual change over the course of treatment. It is possible that the few participants who showed reliable individual improvements remained in treatment longer than those who remained unchanged or even got worse on an individual level. This would imply that the duration of treatment could be an important factor to consider when analyzing the effectiveness of treating psychopathic personality traits (Lewis, 2018).
Implications
This study adds to a growing body of literature suggesting that incarcerated individuals with psychopathic personality traits are treatable instead of “manageable” (Lewis, 2018; Olver, 2018; Salekin et al., 2010) and distances itself from the clinical pessimism of the past. In addition, it sheds some light on “what works” in the treatment of these individuals, extending it to German STFs. While the main goal of STFs is to reduce the participants’ recidivism risk, they also seem uniquely equipped to deal with the high-risk, high-need group, that incarcerated individuals with psychopathic personality traits represent (Brunner et al., 2019; Larsen, 2019; Olver, 2018; Olver & Wong, 2009), offering an integrative, multimodal approach that is in line with what is considered effective treatment for this specific group (Andrews & Bonta, 2010; Lösel, 1998; Olver, 2018).
This study also moves away from the idea of treating psychopathy as a “behavioral entity” (Lewis, 2018, p. 191), showing that underlying changes to psychopathic personality traits are achievable at a small scale. The social and emotional capabilities of at least some incarcerated individuals with psychopathic personality traits do seem to change on a significantly observable level as measured by the PCL–R and IM–P in interviews with participants. This is especially true for the interpersonal and affective aspects of psychopathy, highlighting underlying changes to the impaired information processing and emotional understanding of these individuals.
Overall, these measured significant reductions and reliable individual changes on the PCL–R and IM–P over the course of a treatment that targeted recidivism risk have the potential to call the traditional view of psychopathy as a static risk factor into question (Miller, 2006). Psychopathy might be more of a stable-dynamic risk factor than previously thought, although the present study did not measure the actual reoffending behavior. Consequently, no conclusion can be made as to whether psychopathy, as measured in this study, is truly a dynamic risk factor. However, the implications of these findings tentatively call the use of the PCL–R as a static risk assessment tool (Polaschek & Daly, 2013; Skeem et al., 2011) into question and raise the question about differential effects (why are changes only observable for some but not for all incarcerated individuals with psychopathic personality traits?).
Reevaluating the changeability of psychopathic personality traits could lead to more incarcerated individuals with these traits receiving treatment that could lead to their increased rehabilitation which would be of decided societal value (Lösel, 2001; Polaschek & Daly, 2013). Changes to their psychopathic personality traits and possible subsequent reductions in recidivism might not only be cost-effective but may also reduce the strain on penal institutions while improving their social climates (Lösel, 2001). Therefore, future studies should seek to reinvestigate just how malleable psychopathic personality traits are alongside their relationship to a reduced recidivism in incarcerated individuals with said traits. Establishing psychopathy as a stable-dynamic risk factor might lead to the evaluation of effective treatments for individuals who offend with psychopathy cementing their place in the present research paradigm.
Limitations
There are limitations to the present study. First and foremost, there was no control group of participants that did not receive social-therapeutic treatment. As such, the current results can only be interpreted as correlative, not causal since changes that might have occurred outside of treatment could not be accounted for. The present results should be interpreted under the limited representativity and external validity of the study’s sample, which included individuals with sexual and violent offending histories and elevated psychopathic traits that were part of a treatment program targeting their recidivism risk. Not only did some individuals refuse to participate in follow-up testing, but participants with high levels of psychopathy also have a higher chance of responding poorly to and dropping out of STF treatment, leading to higher rates of recidivism (Brunner et al., 2019; Lösel, 1998). Dropouts are often excluded from studies with STF samples, as was the case here. This may have led to an overestimation of the present results, and future studies should also include dropouts to ensure that treatment effects are not overestimated. In addition, caution should be used when interpreting these results with regard to other STFs in Germany, as they are heterogeneous institutions with varying clientele and treatments (Moosburner et al., 2022a). This study also could not control for moderating variables that may have influenced the treatment outcome, such as duration of treatment or therapeutic climate. Adjusting future studies to meet these criteria might help us understand what specific STF treatments could be effective for treating incarcerated individuals with psychopathic personality traits.
Future Directions
As this study has shown, psychopathy might be more dynamic than previously assumed, and underlying psychopathic personality traits might be malleable to treatments such as those in German STFs. Future research should extend to more STFs in Germany, to inspect whether the present results are simply an artifact of this specific treatment regimen or whether certain aspects of STF treatments, that are meant to reduce recidivism risk, are fit for treating incarcerated individuals with psychopathic personality traits. Furthermore, including dropouts and longer follow-up periods, extending to time after release outside of the STF, would allow us to investigate whether the changes to psychopathic personality traits are of a lasting nature or immediate results of the treatment in the STF. In addition, conducting these analyses with a sample of what might be considered individuals with high psychopathy in European research settings (PCL–R ≥25) or primary psychopathy (PCL–R ≥30) might lead to more differentiated results concerning, but not limited to, age and the amount of observable change. Finally, moderating variables such as therapeutic climate and staff involvement should be controlled for to ensure the results in this study are not influenced by other factors.
Conclusion
This study examined whether psychopathic personality traits could be modified through treatment in an STF that targeted the participants’ recidivism risk. Results indicate that psychopathic personality traits change significantly over an 18-month period for individuals who offend with psychopathic traits, especially on the interpersonal and affective facets of the PCL–R. This seems to be especially true for younger individuals. These results are also reliable on an individual level for certain participants. Overall, it seems that psychopathic personality traits might be malleable to the STFs high-intensity, multimodal treatment that targets deficits in information processing and emotional understanding, although there is an inverse correlation with increasing age for certain factors and facets of the PCL–R. These changes to psychopathic personality traits imply that psychopathy might be more of a dynamic risk factor than previously assumed and that treatment rather than management of individuals with psychopathic personality traits in forensic settings should be further investigated. This study contributes to shifting the discussion from “if” individuals who offend with psychopathic traits can be treated to extending the “what works” approach to include treatments that target recidivism risk for said individuals, highlighting the possibility of change in psychopathic personality traits, which could be of decided value for penal institutions.