
Abstract
Correctional Service Canada implemented Prison Needle Exchange Programs (PNEPs) into federal penitentiaries in 2018 as a harm reduction measure to prevent needle sharing, drug overdose, and limit the spread of infectious disease. However, studies demonstrate how staff resistance hinders the growth of these programs within Canadian prisons. Drawing on interview data produced by 134 federally employed and relatively new correctional officers in Canada, the current study analyzes officers’ levels of support and (more often) opposition to PNEP. Results indicate that, predominantly, staff opposition to PNEP is rooted in safety concerns, a perceived lack of evidence of PNEP’s benefits, and fears the program is not promoting recovery and rehabilitation. By increasing the prevalence of needles in cells, officers report concern of overdose or potential weaponization of needles. Our study informs policy discussions around harm reduction measures in prisons to better promote institutional safety, public health, and nonstigmatized approaches to substance use.
Prison Needle Exchange Programs
Every year, at least 30 million men and women spend time in prisons or custodial settings, with 10 million incarcerated people at any given point in time (United Nations Office on Drugs and Crime [UNODC], 2017). Without access to sterile injecting equipment in prisons, HIV, Hepatitis B and C, and other infectious diseases can be transmitted between incarcerated people who share contaminated needles and syringes. Together with unprotected sexual contact, sharing injection equipment represents the highest risk of transmission of HIV and hepatitis in prisons (UNODC, 2017).
The Prison Needle Exchange Program (PNEP) is a harm reduction measure that aims to prevent needle sharing, fatal and nonfatal overdoses, and the spread of infectious diseases among incarcerated people (Government of Canada, 2019). PNEP provides incarcerated people with sterile injection equipment to avoid harms associated with using unsterilized needles. Beginning in 2018, Correctional Service Canada (CSC) implemented several PNEPs into federal penitentiaries where federally sentenced individuals serve a custodial sentence of 2 years or more, as imposed by the courts (Government of Canada, 2015). To access PNEPs in a federal prison in Canada, incarcerated people must meet with a correctional health nurse at CSC to receive education on substance use, safe consumption, counseling services, and references to other health care providers. Incarcerated people must also receive threat risk assessments and gain approval from an institutional head or Deputy Warden (Government of Canada, 2019).
Prior to implementing PNEP, CSC engaged with the Union of Safety and Justice Employees (USJE), the Professional Institute of the Public Service of Canada, and the Union of Canadian Correctional Officers/Syndicat des Agents Correctionnels du Canada/Confédération des Syndicats Nationaux (UCCO-SACC-CSN), and other partners (Dietz, 2020). Despite these engagement strategies (Dietz, 2020), controversy remains over how effectively PNEP meets its intended public health, safety, and harm reduction objectives. For example, the UCCO-SACC-CSN stated they do not favor the program over Overdose Prevention Sites (OPS), as the circulation of needles in prisons threatens officers’ health and safety (Union of Canadian Correctional Officers/Syndicat des Agents Correctionnels du Canada/Confédération des Syndicats Nationaux [UCCO-SACC-CSN], 2020).
Preliminary research on the introduction of PNEPs in Europe have found most correctional staff are hesitant to support the program because of (1) concerns about their and incarcerated people’s safety, including how needles may be used as weapons; (2) how providing needles may increase the number of incarcerated people who inject substances; and (3) the very presence of PNEP contradicts the correctional institution’s mandate to decrease the presence (or quantity) of substances in prisons (Moazen et al., 2019, 2020; Rosalim, 2020). Moreover, responding to critical incidents involving violence, overdose, or the risk of contracting virus is an occupational stress for officers, where infection can constitute a potentially psychologically traumatic event (Cassiano et al., 2022; Ricciardelli et al., 2022)—a precursor to compromised mental wellness.
Staff resistance is cited as the main reason harm reduction programs, like PNEP, are not widely adopted across international carceral systems (Stöver & Hariga, 2016), since their efficacy relies on cooperation and support across all levels of participation, including politicians, administrators, managers, front-line staff, and service users (Armstrong-Mensah et al., 2021; Michels & Stöver, 2012). In the current study, we seek to analyze Canadian federal correctional officers’ (COs) levels of support and (more often) opposition to PNEP and unpack why many COs are hesitant to endorse the program. Our aim is to inform policy discussions around harm reduction measures in prisons to help better promote institutional safety, public health, and nonstigmatized approaches to substance (mis) use in carceral spaces.
Harm Reduction Philosophy and Effectiveness
Harm reduction is a philosophy, position, approach, and set of practical strategies aimed at reducing negative consequences associated with substance use. Harm reduction is also a social movement built on a belief in, and respect for, the rights of people who use substances (National Harm Reduction Coalition, 2023); as such, harm reduction approaches challenge criminalization and punishment of substance use. Harm reduction understands abstinence from substances is not always possible (or realistic) and prioritizes the reduction of the social, economic, and health-related harms of substance use (Sander et al., 2019).
Despite recent evidence emphasizing how punishing substance use causes more harm than good (Global Commission on Drug Policy, 2016), several jurisdictions across the globe continue to focus on abstinence models, which prioritizes substance eradication through increased security, and the identification and punishment of substance users in prisons (Moazen et al., 2020; Wright et al., 2015). Research finds stigmatizing substance users in prison hinders incarcerated people from seeking health care treatment and encourages risky substance use that could spread infectious disease and harm the user (Sander et al., 2019). Despite the increased criminalization of substance use, rates of substance use remain stable (UNODC, 2018), indicating a need for the facilitation of policy and law consistent with evidence-based approaches.
PNEPs: Tensions and Benefits
Early Canadian research on PNEP showed a shift in CO thinking, from fear and resentment of harm reduction measures to an acknowledgment that PNEPs represent a necessary addition to a range of harm reduction services in prisons intended to support the health and safety of incarcerated people (Kondro, 2007). These positions were informed by political challenges and opposition to select evidence-informed harm reduction programs correctional systems endured from the Conservative-led Government of Canada (2006–2015; Elliott, 2007; Iafrate, 2015). Research in the United States and Ukraine support how the success of PNEP implementation relies on political context, leadership, and an effective transition from one historical period to another (Bluthenthal, 1998; Dmitrieva et al., 2021; Showalter, 2018).
Beyond the politics of implementing PNEP, concerns remain over the lack of confidentiality the program provides to incarcerated people, especially when compared with service users accessing the program in a community setting (Stöver & Hariga, 2016). PNEPs require stable and sustained funding to operate effectively (de la Fuente et al., 2012), and, depending on the jurisdiction, other legal or programmatic obstacles may be encountered such as strict substance use policy laws and regulations (Bastos & Strathdee, 2005). A major debate fueling barriers to implementation are the questions of whether or not prisons can keep illicit substances out of their facilities, if withholding the program endangers public health, and if PNEP is a violation of incarcerated people’s right to health care (Armstrong-Mensah et al., 2021; Moazen et al., 2020).
Somewhat countering oppositional perspectives to PNEPs is a large body of clinical evidence suggesting the program reduces the spread of infectious disease and does not increase substance use (Bize & Samitca, 2017; Glauser, 2013). Early longitudinal research on PNEPs operating in Switzerland, Germany, Spain, and Moldova found syringe distribution was not followed by an increase in substance use or injection substance use; syringes were not misused; sharing of syringes among substance users reduced; and the disposal of used syringes was uncomplicated (Stöver & Nelles, 2003). A World Health Organization (WHO) review of 55 European PNEPs found no reported increase in substance use and “no negative unintended consequences,” such as needles being used as weapons (Glauser, 2013). A similar study evaluating the effective of PNEPs in Spain revealed that, in 10 years, 15,962 syringes were supplied to 429 users and 11,327 were returned, with the prevalence of HIV infection decreasing from 21% in 1999 to 8.5% in 2009 (Ferrer-Castro et al., 2012). While the majority of needles were documented in this study as being returned, the needles that went missing are still problematic. In penal systems without PNEPs, such as Russia, some evidence indicates injection equipment is routinely shared among incarcerated people and attempts to clean borrowed needles are inadequate (Sarang et al., 2006; see also Van der Meulen, 2017). Scholarship, then, demonstrates how the debate on PNEPs remains conflicted, with some clinical evidence favoring the public health outcomes associated with the program, alongside the valid concerns of correctional staff questioning the implications for institutional safety, security, and recovery-oriented practice.
Current Study
In the current article, we investigate how federal COs (N = 134) with at least 1 year of occupational tenure, some working in institutions with PNEP, understand, experience, and assess harm reduction programs in federal Canadian prisons. Specifically, we asked COs about their view or experience with PNEP. Overall, the feedback from COs was strongly in opposition to PNEP, with very few COs reporting support. As some Canadian and international research has documented, there remains tension in the literature between “encouraging” substance use via exchange and continuing to detect, restrict, and punish illicit substance use—conflict that is rife with complexity and contains no simple solution (Moazen et al., 2020). The current study builds on this literature through an in-depth qualitative examination of CO positioning on PNEPs, which we engage both appreciatively and critically in consideration of ways forward to strengthen the effectiveness of harm reduction programs in prisons. Specifically, we examine some of the reasons for this strong opposition, which are nuanced and reveal a complicated situation that conflicts with COs’ understandings of rehabilitation and is thought to fall short on the objective of reducing the transmission of infectious disease.
Method
Participants
In total, 80 men and 54 women comprise our data set, of whom 71 were between age 25 and 34 (see Table 1 for further demographics).
Correctional Officer Demographics
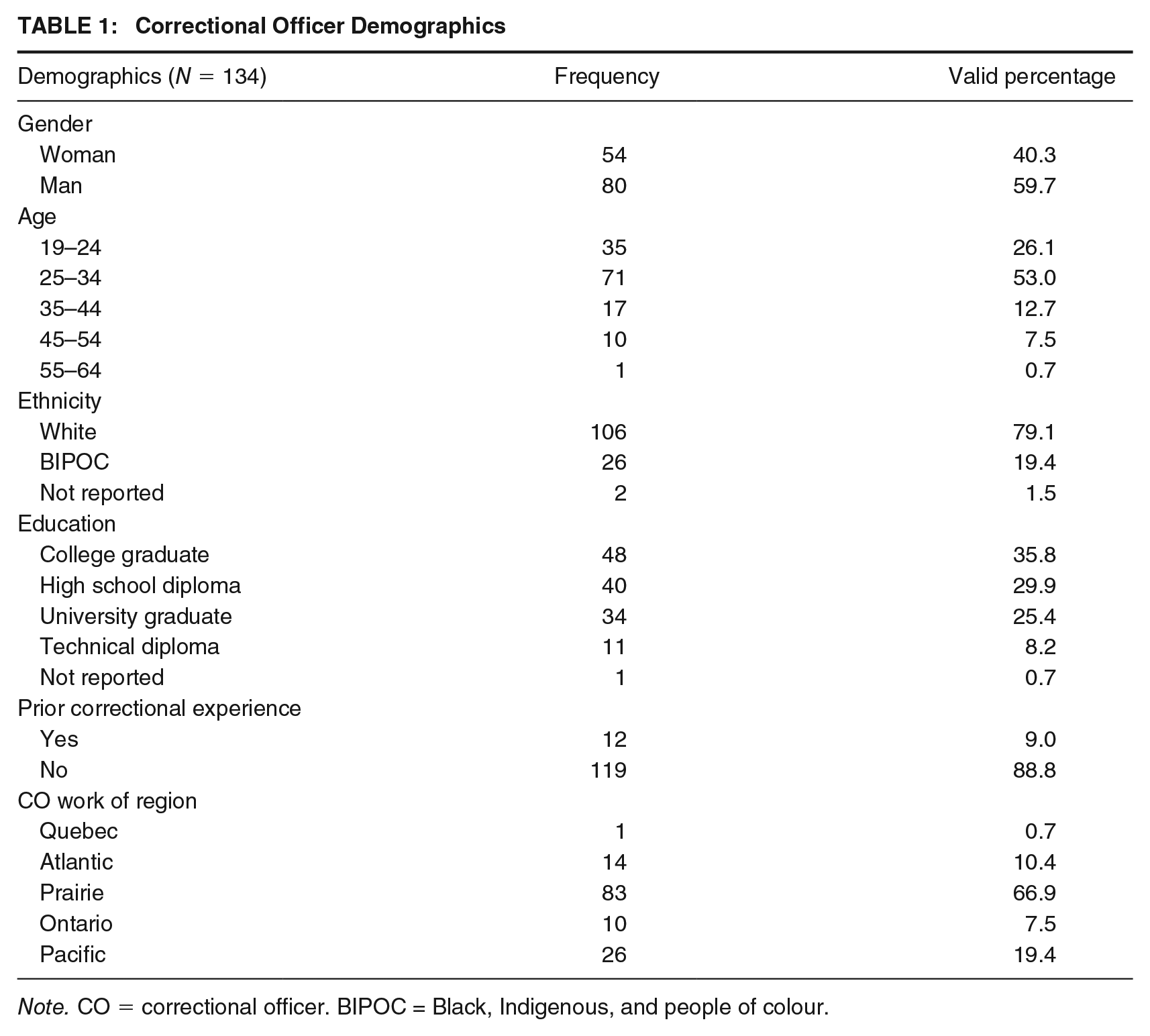
Note. CO = correctional officer. BIPOC = Black, Indigenous, and people of colour.
Measures
In the current study, we analyze data collected from a 10-year longitudinal study (see Ricciardelli et al., 2021, for more details on protocol) of the changing mental health and wellness of COs employed in federal correctional services in Canada. Specifically, we analyzed transcripts from semi-structured interviews with 134 COs, who had at least 1 year of occupational tenure as a CO under the employment of CSC. We asked participants if their institution participated in PNEP, their interpretations of PNEP, and why they held this position. Ethics approval was attained from the Health Research Ethics Board of Memorial University of Newfoundland (File No. 20190481).
CSC has been implementing PNEP into correctional facilities since 2018. In 2020, nine out of 53 of Canada’s federal correctional institutions offered the program (Government of Canada, 2021). CSC mandated numerous steps must occur before an institution can implement PNEP, such as extensive consultations with institutional management and operations, the institutional occupational health and safety committee, the incarcerated people committee, and the community advisory committee (Government of Canada, 2019). CSC has stated they will continue to work with individual sites, taking into account operational considerations, before determining next steps in the rollout of more PNEP.
Procedure
Participant Recruitment
Recruitment of participants for the greater study started in 2018, where the principal investigator (PI) visited each new cohort of recruits at one of CSC’s training academies to introduce the multimethod study. The PI described the study purpose to each cohort of recruits and explained the informed consent process (e.g., data management, confidentiality, funding sources) and created a schedule for participants to sign up for interviews. After baseline interviews, we conduct yearly follow-ups, where we reached out to recruits first by email to determine they want to schedule a follow-up interview outside of work. If they preferred to be interviewed during work hours, which is supported by CSC, we emailed them through their employer to schedule an interview while on shift. Thus, our participants, for this article, were already enrolled in the CCWORK study, and agreed to their first follow-up interview, either onsite at an institution or by phone on their personal time.
Prior to COVID-19, between 80% and 99% of recruits participated in the study when onsite for recruitment. During COVID-19, when the study went online, participation dropped to about approximately 10% to 15% per cohort, and finally, post COVID, with the return to in-person recruitment, the rates of participation have increased to near pre-COVID levels. Few participants drop out of the study once enrolled; however, participants do leave the study for a variety of reasons: inability to complete the training, leave from the institution, resigning from the occupation, and death. Very few participants have otherwise terminated study participation.
Although we have many participants, we maintain the large sample because of the duration of the study and high rates of occupational leaving. Our goal is to have a sample of approximately 200 COs at the 10-year mark of the study in continued participation. Moreover, we are unable to incentivize participation due to restrictions tied to the COs being federal government employees and public servants. The support of CSC was essential for organizing interviews, recruitment, and sustained participation. For some, their follow-up interview was in late 2019, but for others, there was a significant delay because of the COVID-19 pandemic and related public health measures.
Data Collection
In addition, with the introduction of COVID-19, interviews shifted from in-person to phone, as online platforms are of very limited use and access in prisons. Our participants were largely interviewed while on shift in prison, they entered a private room and called the interviewer, who guided the participant through the questions, always following the conversational paths as put forth by the participant. Interviews ranged from 45 to 90 min in length, the average being closer to 90 min. We voice recorded each interview and the recording was transcribed verbatim, although in the quotes presented, we have edited for speech fillers (i.e., umm, you know) and readability. Participant identifying information was removed and names have been replaced with a participant identification number. We refrain from using pseudonyms given we did not find discernible differences based on participant demographics and pseudonyms may inexplicitly suggest race, ethnicity, culture, or gender identity.
Analysis
This study was informed by a realist lens of inquiry, meaning we approached the data—the lived experiences and perspectives of COs—as constituting a reality or truth irrespective of concerns for generalizability or quantifiability, whereby phenomena can be known through words (Bonino et al., 2014). This paradigmatic orientation guided the research team to more fully appreciate the standpoints of participants (Liebling et al., 1999), whose ideas and perspectives on PNEP remain under-studied in Canada. We implemented methodological objectivity-checks (e.g., Are claims a data source or ethnographic knowledge? What contexts are informing findings?), but we acknowledge that we nonetheless remain guided in our analysis by our scholarly and theoretical backgrounds, which are diverse and range from critical criminological forms of inquiry to orientations heavily grounded in the lived experiences of COs and practical realities of correctional work.
We implemented a semi-grounded approach to data analysis, meaning themes emerged from the data but we did not suspend our theoretical knowledge during the analytical process (Ricciardelli et al., 2010). Instead of creating theory, as is the case with many approaches to grounded theory, we tended to apply existing theory to explain the themes (Charmaz, 2014; Glaser & Strauss, 1967). Prior to coding the transcripts for the current study, we constructed a “working” codebook, which we repeatedly revised as we coded more interviews to ensure we captured changes in positioning and maintained comprehensiveness and exhaustive codes. Next, we conducted axial coding for each transcript using QSR NVivo software, following the codebook. We coded parent, child, and grandchild nodes (Kendall, 1999). Frequent codes constituted themes, as they were common experiences or interpretations across participants. Our analysis drew from a parent node for “PNEP” under which we re-coded interviewees’ words tied to discussions of their experience with PNEP or their views on the introduction of PNEP to their institution. Next, we open-coded (Cascio et al., 2019) to further breakdown the data into themes of harm reduction policies, knowledge, challenges, and strategies, which make up the represented data.
Results
We begin the analysis by showing how, generally speaking, participants strongly opposed PNEP, with only a handful supporting PNEP. The few who expressed support for PNEP often praised harm reduction practices more broadly but caveated such support around questions of the effectiveness of PNEPs in a prison setting. As such, we also present themes pertaining to concerns raised by COs regarding the policies and practices governing PNEPs. Our analysis reveals several unintended outcomes of PNEP, such as beliefs from COs that PNEPs are hindering or inconsistent with recovery-oriented practices that could improve incarcerated people’s well-being and better promote rehabilitation; concerns about incarcerated people sharing needles among themselves; fears over being pricked by or assaulted with needles, given their presence in cells; and worries that PNEPs may exacerbate the likelihood of overdoses in prisons.
Expressing (Some) Support of PNEP
A small handful of participants (11.3%) were supportive or somewhat supportive of PNEP. For example, P306, who supports PNEP but has no firsthand experience with the program, favored a harm reduction approach given they recognize people in prison are using substances and “why not give them the resources to make sure they use them in a safe way”? P150, too, describes themselves as “always be[ing] a proponent of harm reduction,” stating I used to volunteer on the downtown east side, so I’m for it. I do respect the safety concerns that other staff have and I think if it’s managed properly and we know exactly which inmate has the needle [it can be managed for safely].
Although they favor the principles of harm reduction based on their lived experience, P150’s challenges and concerns relate to how PNEP is managed. P150 lacks direct experience with the program as it has yet to be implemented in their prison, and with this limitation, they acknowledge their colleagues’ safety concerns with PNEP—but still believe, based on their previous volunteer experience in the community, that those risks can be effectively mitigated through strong management and policy.
P154 believes, with the right people, I would say it does what it needs to do. I personally don’t have a huge, huge opinion on this because I’ve only seen good. I haven’t seen some of the bad like other officers have.
P154 is open to criticisms expressed by their colleagues, but still leans toward supporting PNEP because of the “good” experiences they have witnessed with the program. Other participants, such as P158, note being supportive of PNEP in general but not currently in the prison where they work: “I get the philosophy behind it but I think with the population itself, I don’t think it would be a positive thing. I think it would be more enabling than good. It would cause more harm than good.” This participant recognizes the philosophies behind PNEP but believes the vulnerabilities presented by incarcerated populations present an inherent risk in a prison environment that is supposed to promote and facilitate rehabilitation and recovery, and which, if not achieved, can result in “harm” against incarcerated people.
This position—where people know the harm reduction implications and agree with them but are nonetheless opposed to needle exchange in prison—was more common among participants who expressed some form of support. The sentiment, as summarized by P336, was simply: “As an outsider, I was at one time supportive and now that I’m actually in the job on the frontlines I have become less supportive [laughing].” A theme commonly emerging in the data is pragmatic occupational experiences trumping and complicating the knowledge of harm reduction principles many COs gained before starting their careers, whether through education or community engagement.
COs who expressed some form of support further identified that one of many reasons surrounding their institution’s decision to implement PNEP was to reduce the spread of infectious diseases. Many participants understood and appreciated this sentiment, like P89, who said: “I understand where CSC is coming from. They want to lower the amount of disease transmitted through dirty needles, I get that.” However, central to this theme remains an inherent tension, as P89 continued, I feel like putting a Band-Aid on the problem as in “oh, here’s a clean needle to inject your drugs,” why are we not taking a different avenue to try to find out where these drugs are coming from and stop the drugs themselves.
P89 recognizes the challenge and necessity of preserving public health in a closed institutional setting—especially where substance presence and availability is generally inevitable—but questions if it is still better practice as law enforcers to try to remove contraband from the prison environment.
Likewise, P63 said, “I mean to be honest with you I know the whole theory behind [it] is cutting back on HIV and HEP B but honestly we’re giving them needles to do the drugs that they’re smuggling into the institution.” Thus, some COs, who were aware of the benefits of clean needles for reducing the transmission of infectious disease, did not always express support that the PNEP was the best option for creating rehabilitative/recovery spaces that are substance-free, similar to the philosophies adopted by many addiction recovery centers in the broader community in Canada (e.g., Government of Prince Edward Island, 2023). We found this reality to be in tension with how COs understand PNEP’s role versus the prison’s role and mandate to promote recovery and rehabilitation—a finding we unpack next.
PNEP: Not Rehabilitative
To contextualize the majority attitude toward PNEP, most COs (88.8%) felt PNEP was simply not rehabilitative and, thus, counter to their occupational role, which they felt should be rehabilitative. P10, from an institution yet to implement PNEP, explains that PNEP is “another stupid thing” that again renders prison within a context where “there’s no rehabilitation.” Similarly, P118 describes PNEP as “mind boggling” and P17 clarifies that “We should be making it as hard as possible for them, not easier [laughing].” P17’s words especially identify a synergy between the values of substance abstinence and rehabilitation; illicit substance use, in any form, is thought to inherently hinder rehabilitation from criminal behavior (sometimes precipitated by substance misuse) and encumber health recovery.
Many others echoed the disconnection toward their interpretation of prison being a space for rehabilitation, recognizing that, generally speaking, community rehabilitation/recovery centers in many jurisdictions across Canada do not have needle exchange programs or access to substances. To explain this position, If you come to prison . . . there should be a program to wean you off all of the drugs. To me, rehabilitation is getting you clean, getting you sober, so you go back into society and function and not just feed the habit. (P375) The fact that illegal drugs are illegal drugs in and outside of prison . . . I believe that a needle exchange would be enabling in a lot of ways. Okay, “we know it’s illegal for you to break into that truck but here’s the crowbar. Don’t do it but here’s the crowbar.” That’s not encouraging, that’s not rehabilitation, that’s enabling. (P4) When you come into a prison you’re forced to either sober up or get a debt trying to get your drugs. A lot of people have no other choice but to sober up. People have come in there off the streets, they’re now sober one hundred percent. That’s just ’cause they are forced to do it. (P69) I just don’t think that shooting yourself up with drugs is a good solution to rehabilitation. (P429)
In the first excerpt, P375’s words illustrate how prison should be a space to desist from substance use, which means, in theory, that one of the goals of correctional work should be to provide a substance-free environment. Participants, like P4, believe that providing incarcerated people with safer access to substances is an admittance of failure by the institution to promote and facilitate sobriety. As echoed by P375, substance use may have affected incarcerated people in negative ways in free society and shaped their pathway toward criminalization, which both participants believe can only be positively addressed by COs working to provide an environment where abstinence is possible. In other words, P4 feels that PNEP enables substance misuse rather than supports overcoming substance misuse, which is also evidenced in P69’s words who feels prison should at least provide a space for people who want/or are legally/morally obligated to try to “sober up” to do so without the lure of unsanctioned access to substances. As P429 expresses, participants overwhelming felt providing a venue toward substance use is not “rehabilitation.” Overall, the theme of rehabilitation—and if PNEP was even a source of rehabilitation—was an underlying question participants raised across data and led to an overwhelming lack of support for PNEP. Participants who did not believe PNEP aligned with their occupational mandate of rehabilitation failed to be supportive of the program.
Sharing PNEP Needles
COs, while aware of the role clean needles play in reducing the spread of infectious disease (Ng, 2017), largely do not feel PNEP eliminates the problem of needle sharing in prison locales, specifically. P49 shares the common narrative found in the data: They have needle exchange on the street and that would be something that would be productive. If people would be able to go, change out their needles . . . In prison, it’s different. They’re getting these needles, but the thing is, they’re taking those needles and sharing them throughout the entire unit. It’s supposed to cut down on IV diseases, blood borne diseases, but the thing is, it’s just ramped it up. It’s given them more needles to share with each other more and inject each other more. Another lose-lose situation.
P49 summarizes the general public health concern among participants—that a reduction in the presence and use of dirty needles did not occur following PNEP implementation. The unique and arguably incomparable communities and environments that make up prison living are framed as being incompatible with a needle-sharing program that otherwise can live up more fully to its principles and best standards of practice in a community setting, where access to clean needles and disposable of dirty needles may be more easily controlled and regulated. P49 feels at a loss as they are not able to sanction this problematic and highly risky form of behavior, which in their view is deteriorating the health and well-being of incarcerated people.
P157, in a similar sentiment, reflects on their observation of a PNEP: If one person is on the prison needle exchange, no one is saying that they’re still not sharing that needle with a bunch of other people and then bringing it back. And so at any point, I could be stabbed with something that has been in like up to 5 inmates’ arms and anyone of them could have had a disease or something that I now have to be aware of.
P157’s words illustrate the pronounced reality that is needle sharing and describes how the risk to personal injury increases because the needles coming from the PNEP may be used several times by several different incarcerated people and thus be more likely to be infectious. P103 elaborates on their direct observations of how needles circulate through the PNEP: You see the needles that they give them. The little kits or whatever. They have to show them to you at certain times but I watch them pass it around all the time and use it . . . It doesn’t really eliminate them sharing needles cause they all share those ones so . . . It’s only a clean needle when they first get it so whatever.
What is described here is a “free-for-all” needle-use environment that is not safe nor effectively preventing the spread of infectious disease. The experience is so common that the officer mentions rather passively how incarcerated people share the needles openly, in plain sight, implying the challenges associated with COs trying to stop potentially life-threatening needle-sharing from occurring.
Like P157, P34 feels the needle exchange program impedes on the safety of staff and incarcerated people, given incarcerated people continue to share and circulate needles. The concern over needle sharing and the notion that PNEP was increasing needles in circulation was pronounced among COs with occupational tenure. To further illustrate, There’s a lot of needle sharing that goes on and I can kind of understand where they’re coming from, they don’t want to spread diseases, but at the same time these inmates, it’s like saying “OK, no, here’s some needles,” you brought in some contraband [laughing], be careful. (P30) They can get a new needle however many times they want, and we know they’re just sharing them with each other anyway. (P35)
These participants, echoing others, witness continued needle sharing, despite the program objective being to remedy such a dangerous practice. P30 sees irony in sanctioning incarcerated people for bringing contraband into the prison, while simultaneously providing them with equipment to, in theory more safely but in practice less safely, inject the substance(s). P35, employed in an institution with PNEP and thus with firsthand experience, further explains, I have no idea if it’s been effective in what their goals are, if they’re trying to reduce the end amount of diseases that are being spread. I don’t know if that’s working or not. I know the guys still share their needles, even if it’s new, they still trade them all.
Again, these participants reiterate the needle sharing has not ceased with PNEP, and P35 questions if evidence supports the inference that PNEP reduces the spread of infectious disease in prisons. The challenge for some, like P172, who is supportive of needle exchange programs, remains they are nonetheless conflicted—supporting harm reduction in broader society but less supportive of harm reduction in prisons, given the institution’s harsh and complex realities that perpetuate safety risks and vulnerabilities among staff: “I really believe in harm reduction,” however, PNEP remains “a huge safety concern for me.”
Concerns About Being Pricked
Participants, such as P178, frequently spoke of being concerned about being pricked by a needle while completing occupational responsibilities, like cell searches: There’s a new officer, hired in mid 2019 or 2020, who got poked by a needle and since then he has never come back to work. These inmates, they have so much in their cells, you might not even know where the needle is.
P178’s words highlight the fear some COs have of being put out of work because of a potential workplace injury, which in their eyes, is being exacerbated by the presence of a harm reduction program. P178 also highlights the difficult reality that comprises cell searches, which is an area in a prison that can be quite cumbersome to search given the many possessions that can be scattered throughout the cell, let alone with the potential presence of a dirty needle provided to the incarcerated person by the institution. P228 explains that “[some incarcerated people] have blood borne illnesses, pathogens, HIV, AIDS, HEP, that’s always something in the back of my head. With the drugs well you’re searching . . . you always have to be aware of anything possible.” Against this background and underpinning risk, participants explain the very structure of PNEP leaves them unaware of where needles are located—suggesting that kits are not used as intended—and that more needles are in circulation which increases opportunities to be pricked.
Unpacking the tensions, P228 says “we’re condoning illegal activity by providing them with these needles and it’s confidential.” P228 experiences a form of moral contradiction in that they are obligated to conform to and enforce the laws and rules of their institution and broader society—which still criminalize and sanction many forms of substance use—yet must also provide incarcerated people with (supposed) safer avenues to engage in the denounced activity, all of which are protected through confidentiality and thus leave officers to question which incarcerated people have needles. Moreover, despite needle storage kits being in order during checks, that does not mean needles are not circulated between checks. P104 is concerned about “being stuck with a needle, especially with the new PNEP program,” while other officers explain: Because it’s supposed to be anonymous, they could have their needle hidden somewhere. When I go to search a room and get pricked by it. There’s all those things that are very dangerous to me having that needle in the population. (P157) You got to worry [about] getting pricked by more needles because we give them the resources. (P10) I wouldn’t want to be searching a cell and then having a needle there and then all of a sudden accidentally getting poked by it and it’s just a bad idea. (P30)
The sentiment across the officers’ words is clearly a concern about being pricked by needles, including shared needles, because they have observed more needles in circulation and policy forbids them from being able to clearly delineate who has a needle and when, understandably due to reasons of stigma but nonetheless aggravate officer safety.
Weaponizing PNEP
The concern of sharing needles also underpins concerns about needles being used as weapons, either toward staff or incarcerated people: “You’re now giving inmates needles so you’re giving them a weapon. You don’t know what kind of diseases are on that needle now. They can stab officers” (P114). P77 further unfolds this sentiment: Basically we’re telling inmates like “don’t do drugs in jail but we’re giving you these programs, but then we’re gonna give you needles to do the drugs.” And those needles could also be turned in shanks. Whoever’s gonna have shanks but it’s another weapon.
The concern expressed by both participants is how needles can be used as a means for stabbing officers—needles that, beyond being dangerous because they are sharp, could also be dirty due to needle sharing and consequently transmit infectious diseases.
The weaponization of needles was a perceived challenge because staff fear they will be used against other incarcerated people, for self-harm, or against officers/staff. Even P154, who is supportive of the program, explains, It’s tough too. Can it be a risk? Absolutely. And we’re not entitled to know who’s on it, so we could potentially be exposed to, if you take it to an extreme to being stabbed with a needle at any time. I guarantee the inmates aren’t confidential [if they have needles] . . . Like guaranteed they’re not confidential with other inmates so other inmates really could take that and use it for self-harm, use it against officers. Use it against other inmates.
P154 worries about the victims weaponized needles target and endanger and notes the challenge of the attempted confidentiality of the program, where instead “everyone” knows who has clean needles. Speaking directly to harm between incarcerated people, P62 elaborates: It’s leaving us open to dirty needles and they’re supposed to keep it in a locked box and show us at specific times during the day that everything is there and intact. But what if that inmate decides he has a beef with a certain inmate? Well now, you know they’re opening a box with a weapon in it.
P62, echoing others, feels needles may be used among incarcerated people as weapons when interpersonal challenges inevitably arise. There was a strong sense of distrust of incarcerated people expressed by COs, whose very jobs often require risk-averse thinking and management.
More commonly, participants also voiced concerns about needles being used against officers and recognized that their vest cannot stop the penetration of a syringe or prevent infection. Here, P13 speaks again to how needles can become weapons and spread infectious diseases that could not only harm the officer but their loved ones and close personal contacts as well: You give them weapons in their cells, don’t make them have to steal it, break their lubbers off and sharpen them on the floor late at night . . . you put that needle into a little cocktail straw and he scrubs his hepatitis/HIV cause a lot of them have that here and then he spits that at me and hits me in my neck. I can’t sleep with my girl for 6 months; I’m worried about kissing my children.
Underpinning this passage, again, is lack of trust, likely shaped by officers’ exposure to the realities of prison living and commonality of critical and violent incidents or threats. This lack of trust was not just hypothetical for some officers, but couched in lived experience: Inmates watch each other, we’ve had a couple of times [that] inmates will do drugs with each other and they’ve actually like dropped, they’ll throw cold water to bring him back or whatever before they even, we even know they’ve overdosed. If they can’t bring them back then they come, someone will come tell us like “hey, you need to go check on this guy” and then you go running up there and you find him on the floor. (P10)
Others echoed the sentiment, such as P113, who explains that PNEP is “another huge stressor cause now we’re providing a weapon in many aspects to an inmate cause now they have a needle exchange program but you’re giving them more ways to pass diseases to each other.” P103, where the PNEP program is “in full swing” in their prison, considers needles a potential “weapon,” and P104 expressed: “I could see doing a walk and being stuck with a needle. And again, we don’t know what the inmates have in terms of diseases either right. So there’s a lot of unknown when you give them needles.” P106, who describes themselves as “not really a fan,” although aware of arguments on “both sides,” believes PNEP “just increases the likelihood of somebody getting stuck or having one more tool utilized against us.” Overall, concerns—the stress that is the weaponization of needles—are deeply tied to concerns about infectious disease, needle sharing, and how to best regulate, if at all, the presence of needles in cells.
Needles in Cells and Potential of Overdose
Participants, like P340, discussed incarcerated people’s safety tied to injecting and the potential to overdose, saying “If that’s what it’s for [safely injecting], I don’t feel like it [the needle] should be alone with them in their cell.” Needles in cells was viewed as liability for officers, who are legally responsible to preserve the health and safety of incarcerated people—people, who because of the PNEP, can use their substances in quiet dark corners without the knowledge of staff and, as a lethal consequence, potentially and accidently overdose. P308 explains, You’re not technically supposed to have these things [substances], if you have them, why are we allowing people to take it when again they put us at risk, they put themselves at risk and on top of that we’re responsible for them . . . If I’m on a midnight shift taking a walk and I’m like “oh I think he’s alive” [but he’s overdosed in his cell] and I’m held accountable for this.
P308 problematizes and worries about being accountable for an overdosing incarcerated person despite lacking knowledge or ability to prevent the overdose, and notes the irony—that the needle in which the person injects substances with was provided by the organization. For this reason, comparing an overdose prevention site to PNEP, P81 states: “Safe injection sites, cause if somebody was gonna overdose off something at least they’re visible.” While not against safe injection sites in the community, where people using substances are more visible to on-site health care professionals and not doing the activity covertly, this participant still expresses concern about persons overdosing in cells where officers—who are not medical professionals but must nonetheless intervene to save a life—can only rely on their vision and instincts to detect a possible overdose, which can be especially difficult at night.
Likewise, P152 would prefer “them not hav[ing] access to needles that they can just keep,” as they are concerned about when they will use substances. P158 speaks of the unknown tied to substance use in cells due to PNEP, explaining Is this drug related or is this actual medication related or what is that? We kind of feel in the dark I think about a lot of things. I’m not a fan of this prison needle exchange program. I don’t think that’s a good idea.
P19 feels the same, explaining that “I would prefer the OPS [Overdose Prevention Services] sites just where they don’t have needles in their cells just because, it’s any kind of needle, to get poked with something like that it’s life changing for somebody.” They again voice concern about being poked and encountering dirty needles or needle sharing when incarcerated people are permitted to engage in substance use in their cells and would prefer incarcerated people do that activity in a supervised site where needles and substance use can be more accounted for, monitored, documented, and properly witnessed by all appropriate staff. P340 elaborated further on this potential solution and policy consideration: Ah, [laughter] um, in university I wrote a huge essay about how it’s important and how it should be implemented and all that stuff but it’s so different and it’s so weird to see how your mindset changes once you work in a jail because now, I believe that like, it should be like an on-site problem. Like, if you’re going to use your drugs, and you need safe needles to do that. I feel like there should be nurses present when they’re doing these things. Because telling them that they need to keep it in their cell and then tell us when they like-like just being aware that they have it in their cell, I don’t think it’s enough. Because at the end of the day, like a needle that could be HIV infected is still considered a weapon to me.
In this closing excerpt, the participant recognizes that harm reduction strategies should still be prioritized in prisons, but implemented differently and more carefully managed, to preserve the safety of both incarcerated people and staff. Here, an inner conflict emerged over accepting the research the participant conducted in a university that praised PNEPs versus their practical, firsthand work experience with the program, which raises several questions about the effectiveness of PNEPs’ implementation in Canadian federal prisons.
Discussion
In the current article, we examined COs’ interpretations of PNEP, some with experience with PNEP (i.e., the program was active in their penitentiary) and others who recognized that PNEP would eventually be rolled out in their institution. Relatively few participants supported or were somewhat supportive of PNEP, most of whom felt that harm reduction was a way forward to support the cessation of substance use among incarcerated people (as well as citizens in free society). Here, self-described proponents of harm reduction felt the program was challenged by policy inadequacies but were nonetheless more oriented toward the program’s potential, particularly for reducing the spread of infectious disease, than the recognized or foreseeable challenges documented in other literature (Bastos & Strathdee, 2005; Cassiano et al., 2022; de la Fuente et al., 2012; Stöver & Hariga, 2016). However, even COs supportive of harm reduction often felt PNEP had no place in prisons. Their reasoning tended to align with those of COs who were adamantly opposed to PNEP, believing the program countered the rehabilitation ideal underlying the perceived purpose of prison, that needle sharing continued despite program presence, and the presence of needles in cells was problematic for incarcerated people and all staff—not just COs.
COs felt prisons should strive to provide a substance-free space where incarcerated people can desist from substance use; however, the very presence of PNEP changed the space, appearing in some ways to condone substance use or at least mobilize substance use—albeit more safely. Moreover, COs felt PNEP failed to meet its objectives—to reduce the spread of infectious disease by providing clean needles. Needles, COs expressed, were still shared, sometimes openly. Beyond needle sharing, COs expressed greater concern about being pricked if the needles were not stored correctly or were being circulated. Fear was common here—as found in other studies (Moazen et al., 2019, 2020; Rosalim, 2020)—with COs aware of the ramifications of being pricked, often having witnessed or hearing about the cocktails of medications and other practices that COs endure to prevent illness after accidental exposure to a potentially contaminated needle. Beyond accidental exposure, select few COs voiced concern about intentional exposure to needles—the idea that a needle could be weaponized against another incarcerated person or a CO (or other staff) was pertinent here. Syringes, according to COs, can penetrate a safety vest—thus they lacked protection.
Most concerning was the presence of needles in cells, given the liability if a person incarcerated, known to have needles (and thus substances), was to overdose. COs wanted incarcerated people out of their cells using substances and with support to ensure their safety. They did not desire incarcerated people in corners of their cell using substances without supervision or the officers’ knowledge, nor did they desire encountering an overdosing (or even high) person incarcerated, which can constitute a potentially psychologically traumatic event (Ricciardelli et al., 2022). Officers in this study expressed serious concern about the liability of an overdosing incarcerated person, who they technically knew had substances because of their participation in PNEP. Their occupation is one that inherently requires hypervigilance, sometimes at the expense of mental health and wellness (Johnston et al., 2022), and it is clear in our findings that the presence of needles in cells makes participants feel less safe at work, and more concerned that covert substance use may lead to more critical incidents involving overdose or other substance-related harm.
Permeating these tensions and concerns is the fact federal COs require more health care training and education on harm reduction practices if they are to continue being responsible to manage witnessed or suspected overdoses and oversee some of the PNEP elements in their respective institutions. COs in Canada have raised issue with the burden they must take on to manage the mental health and wellness of incarcerated people (Johnston & Ricciardelli, 2022), as first-responders but not health care professionals. Much literature emphasizes how organizational culture informs correctional workplace relations, experiences, and occupational perceptions, both positive and negative (Arnold et al., 2007; Crichton & Ricciardelli, 2016; Johnston et al., 2021, 2022; Liebling et al., 2010). Empirical research continues to measure the harmful impacts of organizational stress (i.e., structural aspects of the organization) on officer health and wellness, for both correctional service providers employed in the community (i.e., parole/probation officers; Norman & Ricciardelli, 2022) and in institutions (i.e., COs; Ricciardelli & Power, 2020). In this context, data seem to indicate many officers are experiencing stress and positioned at a crossroads in terms of having to promote both institutional security and harm reduction—yet another duty they are expected to fulfill but nonetheless express some discomfort with as well as role ambiguity/conflict, given their points of contention, unease, and tension. Offering education and training to COs may help facilitate destigmatized approaches to substance use that still promote institutional safety and security, which is integral to building trust and support for the program among both staff and incarcerated people.
Further to this point, evidence shows how harm reduction practices become more effective for people who use substances when partnered with other services in a continuum of care, such as substance use detox and treatment services, when appropriate (DC Nex, 2009). PNEPs must regularly and repeatably engage incarcerated people over time to provide ongoing opportunities to link them to services that could improve their health and promote recovery. We emphasize that no single strategy or stand-alone program will effectively meet the needs of diverse incarcerated people or correctional staff who may vary in terms of their social identities, risk behaviors, clinical statuses, and service expectations; as such PNEPs “should be designed to improve integration, cooperation, and focused outreach among an extensive provider network and incorporate early intervention, prevention, counseling and testing, and care services for people who use drugs” (DC Nex, 2009, p. 4). We believe such a multipronged approach to addressing the presence of substances and addiction in prisons will reconcile COs’ persistent objective to meet the rehabilitative objectives of prisons.
Given these findings, we suggest areas for further policy consideration. Explicitly, if PNEP is to continue, there is an unprecedented need to build more support for such programs—beyond training and education, despite both being essential—evidence to support positive outcomes for incarcerated people is perhaps one way of building support. Perhaps, there is a need to recognize the space for PNEP may be best reserved for people living in prison for extended time periods rather than those housed for shorter sentences whose time should be more focused on rehabilitation rather than living. Such considerations may garner more support for PNEP because the rehabilitative orientation of many COs would be better satisfied if PNEP was reserved for individuals with long-term sentences. There is also a need for policy makers to consider measures to further improve the safety of PNEP for officers and residents, including perceptions of safety, which, beyond requiring education, may benefit from having controlled spaces for injecting, using, and having needles. One measure would be to introduce OPS as an alternative to PNEP because the sites would remove needles for cells and circulation, provide more control over the potential for incarcerated people to overdose, and eliminate concerns about weaponization or being pricked.
Conclusion
The PNEP is a harm reduction measure aiming to prevent needle sharing, fatal and nonfatal overdoses, and the spread of infectious diseases among incarcerated people (Government of Canada, 2019). However, despite the seemingly therapeutic and public health benefits of this program, participants in our study generally opposed the practice or implementation of PNEP for a multitude of reasons. Largely entrenched within the staff resistance to PNEP was the concern of officer safety. However, CO support for PNEP is essential and necessary for PNEP to be implemented with success—otherwise, the program will only be met with resistance and create a sense of risk or threat (Viglione et al., 2015). Moreover, without CO support, the program implementation will be hindered, which may negatively affect uptake, making PNEP ineffective. For instance, findings suggest how PNEP bodes a safe supply of sterilized needles among incarcerated people, but staff report that PNEP has little to no impact on the supply of dirty needles within a correctional institution and thus will further deter COs from supporting PNEP. COs report opposition to PNEP as the program inevitably allows incarcerated people to have needles in their cells—a practice which enhances overdose probability as well as the risk of officers being inadvertently pricked by a needle—removing needles from cells is key to CO and resident safety, but is counter to the objectives of PNEP which results in more needles in cells.
Overall, the backdrop of opposition was often characterized by the notion that PNEP undermines effective rehabilitation by increasing substance use and giving incarcerated people another means of substance use, which officers believe may be a risk factor for recidivism or criminal behavior. We emphasize the importance of understanding themes across participant opposition given that staff resistance to PNEP is a leading inhibitor of harm reduction programs being adopted internationally (Stöver & Hariga, 2016). The current study has unpacked CO perspectives on support and opposition for PNEP and the nuances encompassed within this harm reduction inspired program. However, limitations exist. To gain a richer perspective on the nuances of PNEP, including the lived experiences and perspectives of incarcerated people, would enhance the data and allow for this program to be better understood contextually (see Giffin et al., 2023). In addition, a cross-sectional analysis on support and opposition of PNEP from a gender, race, class, and ability perspective could allow for an in-depth understanding of the nuances of PNEP effectiveness for specific populations, who may carry diverse vulnerabilities, allowing for challenges to be better understood and, in due course, resolved.
Footnotes
AUTHORS’ NOTE:
The authors declare no potential conflicts of interests with respect to the authorship and/or publication of this article.