
Abstract
Web-based interventions (WBIs) have become increasingly important in mental health treatment. At the same time, WBIs for individuals who committed sexual offenses against children (ICSOC) are increasingly being developed and implemented. Despite this trend, it is unclear which treatment components make WBIs for ICSOC effective and what needs to be considered for successful implementation. Moreover, only few evaluation studies are available. The goal of this viewpoint paper, that includes a comprehensive literature review, is to provide criteria for the development, evaluation, and implementation of WBIs for ICSOC or for individuals who feel at risk of committing sexual offenses against children. The criteria are drawn from guidelines for WBIs in general psychiatry, in forensic psychiatry, and for ICSOC. For the latter, an overview of current WBIs for ICSOC and for individuals who feel at risk of committing sexual offenses against children will be provided.
Keywords
Along with the increasing digitalization of everyday life, information and communication technologies regarding mental health (eMental Health, eMH) have experienced an upswing (Andersson et al., 2019). At present, there are multiple eMH applications for various mental health concerns available (Andersson et al., 2019), and the effectiveness of many applications has been supported in randomized controlled trials (RCT; Etzelmüller et al., 2020; Köhnen et al., 2021; Reins et al., 2021). Based on these studies in the field of general psychotherapy and counseling, eMH has been developed for forensic psychiatry and psychotherapy since the beginning of the 21st century (Kip et al., 2018). This article focuses on the current state of web-based interventions (WBIs) for individuals who have committed contact or noncontact (e.g., child sexual exploitation material offenses) sexual offenses against children (ICSOC) and their development, evaluation, and implementation. The article also considers individuals who feel at risk of committing sexual offenses against children, for example, because they feel sexually attracted to them. As defined by Barak et al. (2009), WBIs are prescriptive online programs, which operate through a website and are primarily self-guided. There are different types of WBIs (i.e., web-based education interventions, self-guided web-based therapeutic interventions, and human-supported web-based therapeutic interventions) that differ in their program content, multimedia usage, provision of interactive online activities, and provision of human guidance. In addition to WBIs, eMH applications include online counseling, internet-operated therapeutic software (e.g., virtual reality, gaming), and other online activities (e.g., blogs, podcasts, online support groups; Barak et al., 2009). WBIs are one of the most studied (Kip et al., 2018) and used eMH application in the forensic and correctional field (Kirschstein et al., 2021). One reason for this could be that WBIs have similarities to other web-applications we use every day, like apps or websites. Moreover, content from face-to-face (f2f) treatment is relatively easy to transfer into WBIs in comparison to other eMH applications (e.g., virtual reality).
Potential Benefits of WBIs in Forensic Psychiatry and Psychotherapy
WBIs could improve the care of inpatients and outpatients in forensic psychiatry and psychotherapy. Section 2 of the German Prison Act (StVollzG, 1976) defines the objective of prison placement as preparation for a life without crime. To fulfill this legal mandate of tertiary prevention, effective treatment must be offered to persons who have been convicted of a crime. However, the fulfillment thereof is restricted by limited monetary and human resources for staff training and treatment services (Chaple et al., 2014). WBIs could at least become a partial solution by providing a time- and cost-effective complement to f2f treatment (Chaple et al., 2014; Cunningham et al., 2009; Levesque et al., 2008, 2012; Walters et al., 2014). In WBIs, staff costs are potentially low because clients largely teach themselves the content and there is only relatively brief or no interaction with staff (Levesque et al., 2012). Hence, there could be an increase in treatment capacity and potentially more individuals receiving treatment (Chaple et al., 2014). However, so far these assumptions are hypothetical, as no systematic analysis of cost-effectiveness in forensic psychiatry or psychotherapy has been performed. In addition, staff turnover and high client caseloads could threaten treatment fidelity for inpatients. WBIs, however, are highly structured and standardized (Levesque et al., 2008, 2012), so that all participants can receive treatment as intended (Chaple et al., 2014; Cunningham et al., 2009).
Just as the inpatient sector, the outpatient sector of forensic clients is a fast-growing field. For example, in the Netherlands, the number of forensic outpatients easily exceeds the number of forensic inpatients (Drieschner & Boomsma, 2008). In the United States, nearly 40% of new prison intakes result from probation failures (Guerino et al., 2011), highlighting the importance of adequate support and follow-up care after release. Yet, in the outpatient sector, patients can face difficulties in accessing care. People who live in rural areas often have poor access to existing care structures (Gaebel et al., 2009). Other difficulties in participating in f2f treatment may include unusual work schedules (e.g., shift work), mobility limitations, and medical conditions (Barnett, 2005). Forensic outpatients experiencing these difficulties could benefit from the flexibility and accessibility of WBIs, as sessions can be scheduled flexibly in terms of time and place (Chaple et al., 2014; Cunningham et al., 2009; Elison et al., 2016).
Especially ICSOC and individuals who feel at risk of committing sexual offenses against children face barriers while searching for treatment options. Stiels-Glenn (2010) questioned psychotherapists working in a large German city about their willingness to work with individuals who committed sexual offenses. Of the psychotherapists who responded, 13% were willing to work with individuals who committed sexual offenses, but only 4% were willing to work with ICSOC, and 5% were willing to work with people who feel sexually attracted to children. Psychotherapists cited the potential risk of reoffending or the lack of experience or knowledge in treatment of these clients as reasons (Stiels-Glenn, 2010). WBIs could provide an additional option to existing f2f treatments, especially for individuals who have difficulties finding a psychotherapist. Furthermore, WBIs could provide a higher degree of privacy and a reduced level of stigmatization (Chaple et al., 2014; Tait & Lenton, 2015). In WBIs, patients can work self-guided, with little (e.g., in written form) or no contact with another person. WBIs may, therefore, reach more ICSOC who have not been convicted and who are, therefore, reluctant to take part in a f2f treatment. In addition, WBIs could provide a low threshold treatment option for people who do not seek f2f treatment because of shame or guilt, such as people who feel sexually attracted to children (Levenson et al., 2017).
In summary, WBIs could be used as a low threshold, time- and cost-effective add-on to other treatments for forensic patients and ICSOC, helping to increase the amount of treatment on offer. WBIs seem to offer the greatest potential in the outpatient treatment, as access to the internet in prisons or forensic psychiatric hospitals may be restricted. Nevertheless, WBIs could also provide new treatment opportunities in the inpatient sector.
Goal of the Present Paper
As WBIs are increasingly being developed for ICSOC (Fromberger et al., 2021), a clear overview thereof is needed to draw on experience already gained, make the results more readily available, and allow similarities or differences between different types of WBIs to be identified. To guide further development, evaluation, and implementation of WBIs for ICSOC, criteria from f2f forensic psychiatry and psychotherapy as well as from WBIs for other target groups should be considered. In the f2f context, treatment that is developed according to evidence-based criteria shows the largest effectiveness (Hanson et al., 2009). Nonetheless, adherence to criteria does not preclude negative effects for a given treatment (Banse et al., 2021; Mews et al., 2017). In addition, especially with a new technology, such as WBIs, there needs to be a focus on how implementation can succeed (Kip, Sieverink et al., 2020). The use of assessed and evaluated criteria could improve the efficacy and effectiveness of WBIs and prevent the dissemination of harmful WBIs by more rigorous evaluations thereof. Furthermore, the use of these criteria could increase the acceptability of WBIs and adherence to them, leading to a higher standard of care. For this purpose, the present viewpoint paper, that includes a comprehensive literature review, provides (a) an overview of current WBIs for ICSOC and individuals who feel at risk of committing sexual offenses against children, (b) criteria for developing, (c) evaluating, and (d) implementing WBIs.
WBI for ICSOC
The first goal of this article is to provide an overview of current WBIs for ICSOC and individuals who feel at risk of committing sexual offenses against children. The overview is based on Wild et al. (2019) and the authors’ experiences. One of the first WBI developed is the Lucy Faithfull Foundation’s (LFF) Get Help website. The target group comprises people who are consuming child sexual exploitation material or have sexual online conversations with children. Similarly, LFF launched the Get Support website targeting people who are troubled by their sexual thoughts or have committed an offense against a child (Bailey et al., 2018). These self-guided web-based therapeutic interventions consist of cognitive behavioral online modules with psychoeducation about online behavior as well as management strategies and worksheets. Both websites are closely connected to the Stop It Now! Helpline, which offers a free and anonymous telephone as well as chat support.
Another offer for individuals with sexual interest in children is the self-guided WBI Troubled Desire (Beier, 2018; Schuler et al., 2021). On the Troubled Desire website, users can complete a self-assessment questionnaire and receive feedback on their sexual preferences and problematic sexual behavior. After that, users can access the WBI or/and seek for further help (e.g., contact a therapist). The WBI consists of 16 modules with cognitive-behavioral psychoeducation and worksheets. Similar to Troubled Desire, the self-guided website Help Wanted was recently developed for individuals with sexual interest in children. In interactive videos, users can learn about coping with sexual attraction to children and building a positive self-image (Moore Center for the Prevention of Child Sexual Abuse, 2020).
In addition to the self-guided WBIs, there exist the two human-supported WBIs, Prevent It and @myTabu. Prevent It targets individuals who use child sexual exploitation material with the treatment goal of reducing consumption. The WBI consists of eight cognitive-behavioral sessions in video or text format that provide exercises to work on in between the sessions. Participants get individual feedback from a therapist for each session via online chat or email (Parks et al., 2020). Fromberger et al. (2021) developed @myTabu for ICSOC who are under community supervision. The treatment goal of @myTabu is to reduce the risk of recidivism. The WBI consists of 24 cognitive-behavioral sessions, incorporating videos, texts, and exercises. Participants get written feedback on exercises by an online coach, which they can further contact via in-app messages (Bauer et al., 2021). Since Prevent It and @myTabu are currently being evaluated, access is only available through study participation.
To our knowledge, six WBIs for ICSOC and individuals who feel at risk of committing sexual offenses against children have been published so far. The WBIs differ especially in guidance, access options, and target group. Similarities and differences between the WBIs presented can be found in Table 1.
Characteristics of WBIs for ICSOC and Individuals who Feel at Risk of Committing Sexual Offenses Against Children
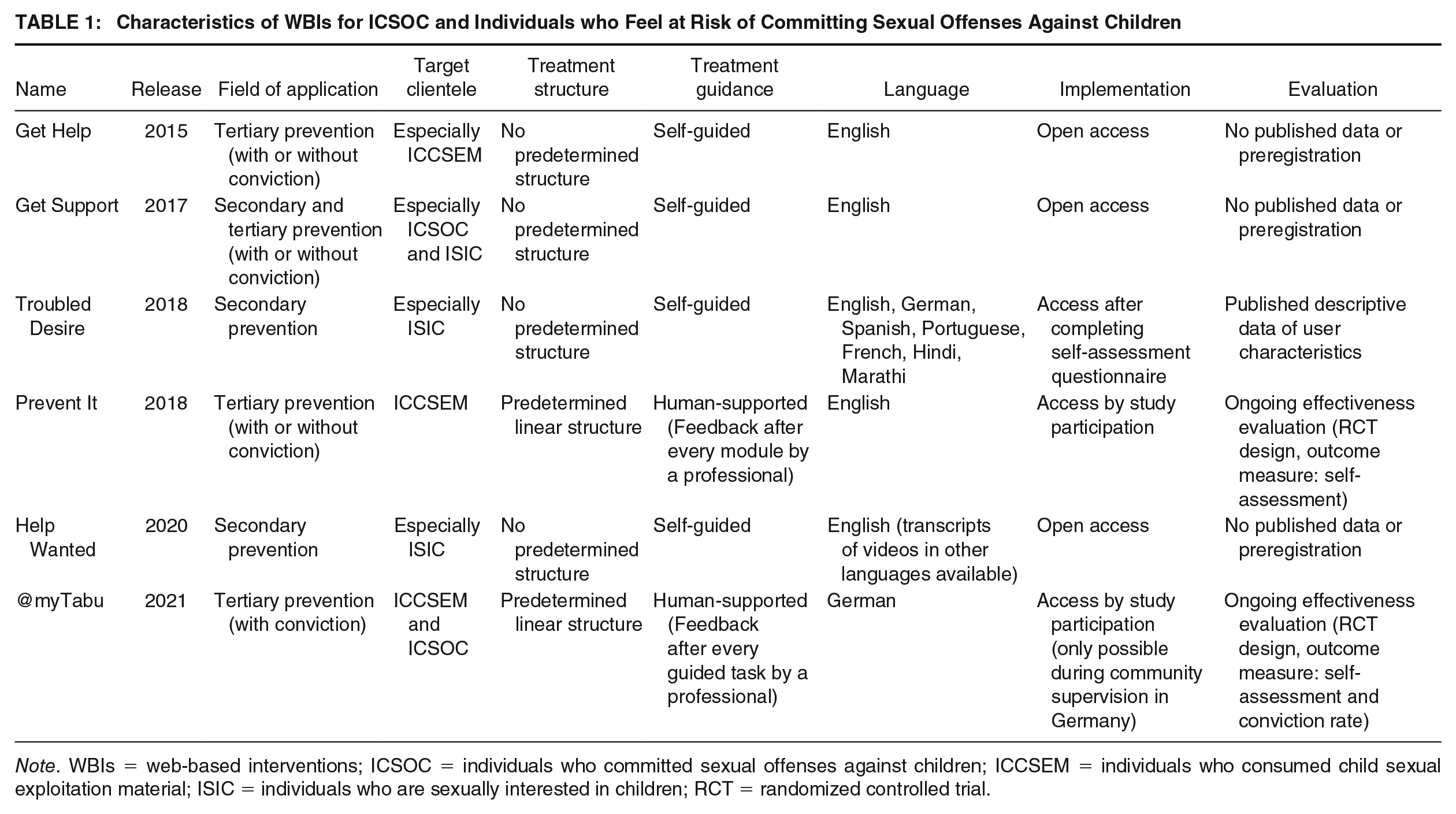
Note. WBIs = web-based interventions; ICSOC = individuals who committed sexual offenses against children; ICCSEM = individuals who consumed child sexual exploitation material; ISIC = individuals who are sexually interested in children; RCT = randomized controlled trial.
Development of WBIs for ICSOC
We recommend that criteria for the development of a WBI for ICSOC should be based on different sources. In general psychiatry, where WBIs have shown to be effective in reducing symptoms of disorders (Etzelmüller et al., 2020; Köhnen et al., 2021; Reins et al., 2021), key factors for the effectiveness of WBI could be identified (Knaevelsrud et al., 2016). This enables the identification of criteria that are relevant for the effectiveness of a WBI for ICSOC. Furthermore, there are criteria that are relevant for the treatment of individuals who have committed offenses, especially sexual offenses, which should also be considered when developing a WBI.
Criteria for the Development of WBIs for ICSOC
Research on WBIs in general psychiatry has shown the importance of therapeutic guidance. Therapeutic guidance in WBIs is a form of contact with a health professional, which can be synchronous (“real-time”) or asynchronous (“time-delayed”). In many cases, human-supported WBIs have achieved better results than self-guided WBIs, which do not provide further contact with a professional (Andersson & Cuijpers, 2009; Spek et al., 2007). Besides that, meta-analytic results did not reveal any differences in the efficiency of synchronous or asynchronous therapeutic contact (Richards & Richardson, 2012). Therefore, it is recommended that a WBI for ICSOC should provide the guidance of a mental health professional (Wild et al., 2019).
Findings in general psychiatry suggest that the amount of structuring and the length of WBIs have an impact on their effectiveness. Dölemeyer et al. (2013) found that WBIs that did not follow a structured treatment program were less efficient in reducing symptoms than structured treatment programs. Shorter programs were found to be more effective than programs with a larger number of sessions (Richards & Richardson, 2012), although it is unclear whether this is influenced by the severity of the disorder (Knaevelsrud et al., 2016). We, therefore, recommend development of structured WBIs with as few sessions as possible.
Research on WBIs in general psychiatry suggests that usability is important for WBIs to work as intended (Petersen et al., 2019). As people with intellectual disabilities are overrepresented among individuals who have sexually offended (Callahan et al., 2022; Cantor et al., 2005), intellectual and learning disabilities could limit the understanding of the content of a WBI and therefore its effectiveness (Knaevelsrud et al., 2016). Also, language-based WBIs require reading skills and motivation, which can be a barrier for forensic clients with low education and low motivation (Drieschner & Boomsma, 2008). Four criteria for WBIs for ICSOC can be derived from these considerations. First, usability should be ensured, for example by highlighting the more important sections of the WBI and presenting information simply (Petersen et al., 2019). Second, language appropriate for the target group should be used. Third, it should be possible to address different cognitive abilities with adaptations of the WBI, such as additional content that can be unlocked for clients in need (Wild et al., 2019). Finally, low motivation should be targeted by using motivational interviewing techniques to enhance treatment adherence (Wild et al., 2019).
The application of WBIs in general psychiatry as well as in the forensic context has identified physical incapability and a lack of knowledge regarding the use of specific technologies as barriers for using a WBI (Kip et al., 2018; Titzler et al., 2020). Issues regarding physical incapability should be considered during the technical development of a WBI through barrier-free programming (e.g., for clients with visual impairment). To ensure that clients with little computer experience can participate too, instructions on how to navigate the WBI have to be available (Wild et al., 2019). Furthermore, to enhance accessibility, WBIs should be optimized for different hardware, like desktop computers, tablets, and smartphones (Wild et al., 2019). A WBI for ICSOC should, therefore, follow the criteria of barrier-free programming, providing a user tutorial and responsiveness to different hardware.
The Risk–Need–Responsivity (RNR) model is of special importance (Bonta & Andrews, 2007) when looking at the treatment of individuals who have offended. The “risk” principle considers that treatment should be adapted to the individual’s likelihood of re-offending. The “need” principle entails identifying and addressing criminogenic needs (i.e., factors that are related to re-offending). Wild et al. (2019) propose that dynamic (i.e., changeable) risk factors, which have been shown to be related to re-offending (e.g., Mann et al., 2010), should be the primary focus of WBIs for ICSOC. The “responsivity” principle is divided into general and specific responsivity. General responsivity promotes the use of cognitive social learning methods to influence behavior. From this Wild et al. (2019) deduce that principles of cognitive behavioral therapy should be applied in WBIs. Meta-analytic results suggest that this is one of the most effective treatment approaches for individuals who have committed sexual offenses (Schmucker & Lösel, 2015). The specific responsibility includes the adjustment of treatment to the individual’s skills, learning style, personality (Bonta & Andrews, 2007). Giving the importance of the RNR principles in treatment of offending individuals, Wild et al. (2019) suggest that a criterion for WBIs for ICSOC is adherence to RNR-principles and therefore consideration of dynamic risk factors with principles of cognitive behavioral therapy.
A negative aspect of WBIs in forensic psychiatry and psychotherapy is related to the confidentiality of the data collected by eMH (Kip et al., 2018). Clients could fear a violation of privacy by insecurely stored data. In the context of ICSOC treatment this could have particularly negative consequences, because of the sensitivity of the data. A WBI for ICSOC should, therefore, ensure data security and data protection, furthermore, participants should give informed consent (Wild et al., 2019). This includes that all communication should be encrypted and databases should be secured not only by software but also by hardware solutions. A summary of all development criteria for a WBI for ICSOC can be found in the first column of Table 2.
Criteria for Development, Evaluation, and Implementation of WBIs for ICSOC
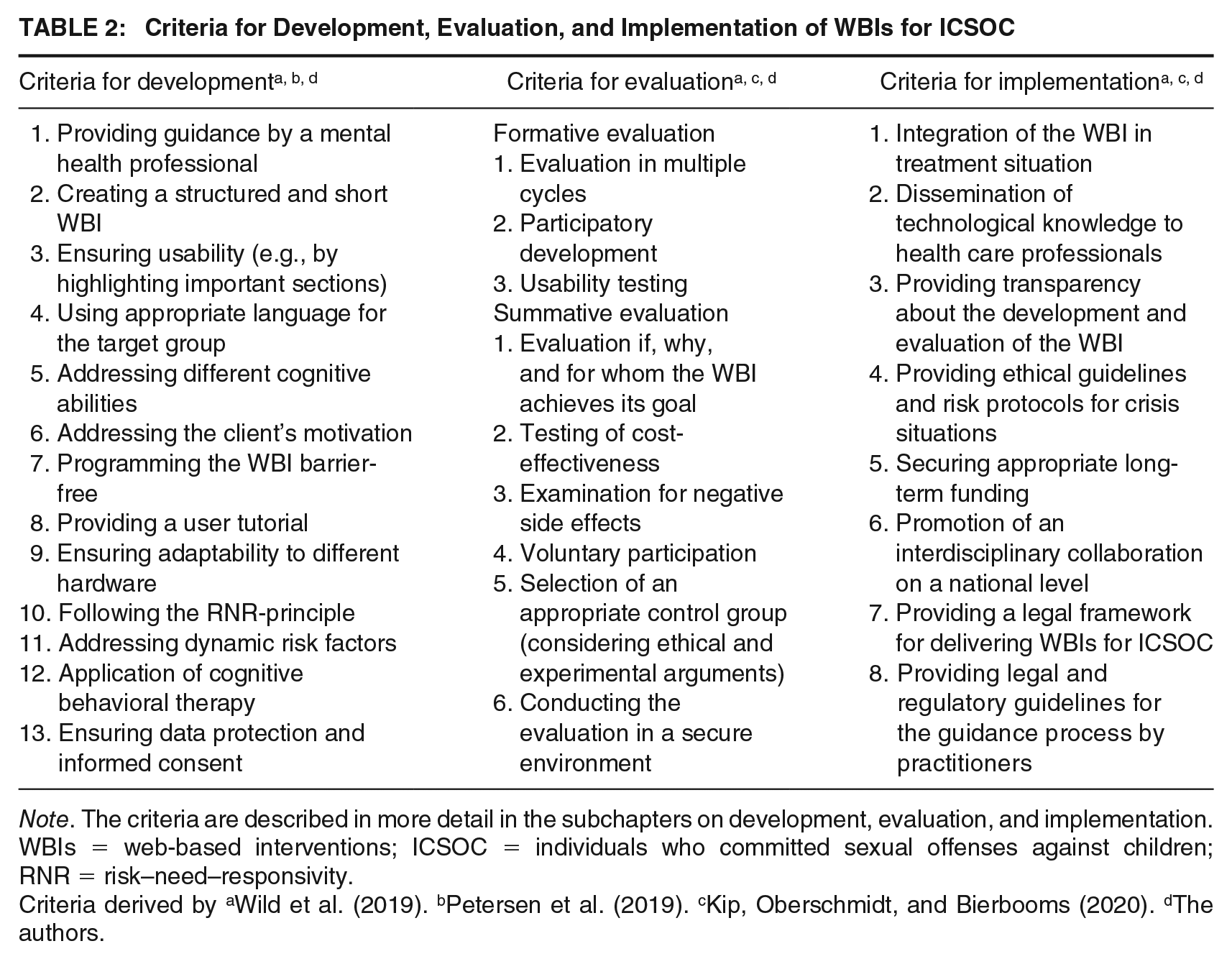
Note. The criteria are described in more detail in the subchapters on development, evaluation, and implementation. WBIs = web-based interventions; ICSOC = individuals who committed sexual offenses against children; RNR = risk–need–responsivity.
Criteria derived by aWild et al. (2019). bPetersen et al. (2019). cKip, Oberschmidt, and Bierbooms (2020). dThe authors.
Development Criteria in Practice
The criteria for the development of WBIs in general psychiatry and for ICSOC can be used as a starting point for the development of new WBIs. However, if and how these criteria influence the effectiveness of WBIs is still unclear, as current research in this area lags behind the desire for fast implementation. Because of that, some of the criteria, like ensuring usability, provide little concrete guidance on how an WBI should be designed. Furthermore, this makes it difficult to evaluate existing WBIs because it is not clear when the criterion is met. Not all of the criteria might have equal weight. Data security and data protection as well as informed consent seem to be fundamental and highly mandatory. In contrast, the criterion on a tutorial about how to navigate the website could be abandoned under certain circumstances, for example if the WBI has a very simple design. Some criteria even might not be suitable for every kind of WBI. Some WBIs could have the goal of providing low threshold support that reaches as many individuals of the target population as possible. It could be that this goal is better achieved without therapeutic guidance.
Evaluation of WBIs for ICSOC
The evaluation criteria for WBIs for ICSOC are described using the Stage Model of Behavioral Therapies Research (Onken et al., 1997). According to this model, the evaluation process can be divided into three successive stages. In formative evaluation (stage I), researchers assess the intervention’s target criterion and the needs of the target population to determine the design and content of an intervention. In the summative evaluation stages, researchers can then determine whether the intervention can achieve its effects under ideal conditions (Stage II, efficacy research) and under more naturalistic conditions (Stage III, effectiveness research; Danaher & Seeley, 2009; Onken et al., 1997).
Criteria for Formative Evaluation of WBIs for ICSOC
To date, few studies have addressed formative evaluation of WBIs in forensic psychiatry or psychotherapy. For this reason, this section also considers criteria for other eMH applications. According to professionals, patients, and eMH experts in forensic psychiatry or psychotherapy, it is important during the development of eMH to have multiple formative evaluation cycles (Kip, Oberschmidt, & Bierbooms, 2020). Within the evaluation cycles, participatory development methods should be used, like methods with active involvement of stakeholders. This can increase the fit of the eMH application to the needs, characteristics, and contexts of patients and therapists. Other methods that can be used in this evaluation stage include mixed-methods approaches and qualitative methods like semi-structured interviews or questionnaires (Kip, Oberschmidt, & Bierbooms, 2020). Furthermore, usability testing is an important step in this stage of evaluation to enhance the accessibility of WBIs (Petersen et al., 2019; Wild et al., 2019).
Kip, Oberschmidt, and Bierbooms (2020) mention that the evaluation process has to be optimized for the forensic context. Kip et al. (2019) conducted a formative evaluation for virtual reality in forensic psychiatry and psychotherapy and concluded that when working with forensic patients, specific examples should be used, data collection should be kept as brief as possible, inquiry should be perceived as personally relevant or rewarding, and different methods and perspectives should be combined. Some of these findings, such as that it is helpful to provide examples of possible uses of virtual reality, may be less relevant for WBIs, since the similarity to apps and websites might make the application more intuitive. In addition to these points, other issues may be relevant when evaluating a WBI for ICSOC, such as that participants may wish to remain anonymous and that there may be inhibitions about addressing shame-related issues in focus groups.
Criteria for Summative Evaluation of WBIs for ICSOC
In the next phase, efficacy evaluation (Stage II) and effectiveness evaluation (Stage III) can determine whether the WBI achieves its intended effects. According to the participants in the study by Kip, Oberschmidt, and Bierbooms (2020), it is important to answer the questions if, why, and for whom eMH applications accomplish their goal. Furthermore, the cost-effectiveness of WBIs needs to be considered (Kip, Oberschmidt, & Bierbooms, 2020). Thorough evaluation can prevent the dissemination of WBIs that are ineffective or have negative side effects, like danger to the general public or to the clients (Wild et al., 2019). In this regard, it is important in forensic psychiatry and psychotherapy that individuals do not feel coerced into participating in a study which would occur for example by linking the evaluation study to mandatory treatment (Fromberger et al., 2021).
Along with a traditional RCT, suitable approaches in summative evaluation include factorial design and analysis of log data (Kip, Oberschmidt, & Bierbooms, 2020). Factorial design is recommended in f2f forensic psychiatry and psychotherapy (Banse et al., 2021) as well as in eMH for general psychiatry (Collins et al., 2007) to investigate the effectiveness of treatments. In a factorial design, researchers can determine which components are most promising for development of an effective treatment. As a first step, the most effective components for a treatment should be identified and then the effect of the treatment comprising those selected components should be evaluated. Log data such as number and duration of webpage visits provide an objective assessment of the participant usage of a WBI (Danaher & Seeley, 2009). They are especially informative for WBIs, in which the users are not forced to work on the content in a specific order.
ICSOC represent a heterogeneous group and sample sizes in trials are often small so that participants in the experimental and control group should be matched (Lösel et al., 2020). Moreover, when conducting RCTs, the selection of the control condition is of particular importance and must be guided by ethical (e.g., exclusion of clients from potentially effective treatment, Marshall & Marshall, 2010) and experimental considerations. To evaluate WBIs which are adjunct to f2f treatment (i.e., blended approach), the WBI would take place in addition to the usual care for the experimental group (Danaher & Seeley, 2009). In the case of stand-alone WBIs, the control groups could receive the usual care, another WBI, or a placebo—depending on the research question and application area (Lavori, 2000). Especially in placebo-controlled trials conducting the trial in a secure environment (e.g., through regular risk assessment; Wild et al., 2019) could help to address ethical concerns. A summary of the criteria for formative and summative evaluation is given in the second column of Table 2.
Evaluation Criteria in Practice
The current evaluation status of WBIs for ICSOC and individuals who feel at risk of committing sexual offenses against children is shown in Table 1. For WBIs with the goal of delivering anonymous, self-guided support, descriptive data related to user characteristics and user satisfaction are available (Bailey et al., 2018; Schuler et al., 2021). In the evaluation of Get Help and Get Support by Bailey et al. (2018), it is unclear how the results were achieved. For Troubled Desire, Schuler et al. (2021) examined user characteristics based on the self-assessments that must be completed before accessing the WBI. However, as mentioned by the authors, as a result of this anonymous approach, it is unclear whether the statements are robust (e.g., unbiased by multiple or casual logins).
The WBIs above were implemented prior to their evaluation. Given that evaluation is necessary because WBIs might be ineffective or have negative side effects (Wild et al., 2019), this has to be regarded as critical from an ethical point of view. Conducting an evaluation according to the above criteria seems to be difficult for already implemented, anonymous, self-guided WBIs. For currently implemented WBIs, analyses of log data could be used to assess which part of the WBI is used the most. To evaluate effectiveness, questionnaires correlated with meaningful risk factors could be used to measure change. Furthermore, participants could be asked to provide personal data for research purposes to collect other outcome measures, such as criminal offenses. To perform RCTs, a control condition must be implemented and considerations must be made to enable informed consent. Furthermore, if the WBI is accessible without a user account, tracking techniques have to be used to make the users traceable and distinguishable from each other. However, to prevent the dissemination of WBIs which have negative side-effects, we recommend hosting only evaluated WBIs.
For Prevent It and @myTabu, effectiveness evaluations are currently being conducted. These guided WBIs are both preregistered for an RCT with a placebo control group (Fromberger et al., 2021; Parks et al., 2020). Up to now, no results from these trials have been published. For human-supported WBIs that are more closely linked to an institution, a thorough effectiveness evaluation appears more feasible than for self-guided WBIs.
In summary, there is a difference in evaluation of WBIs with and without guidance. WBIs without guidance focus on descriptive data that help identify the individuals who are most interested in a WBI. Human-supported WBIs focus on effectiveness evaluation using RCT designs. However, to answer the questions if, why, and for whom WBIs achieve their goal, more formative and summative research with different study designs is needed. Furthermore, it is important to determine (theoretically and practically) which evaluation design is appropriate and feasible for different types of WBIs.
Implementation of WBI for ICSOC
The aim of developing and evaluating WBIs is their implementation in standard care. How challenging this aim is, has been shown by Kip, Sieverink et al. (2020) who examined the implementation of a WBI in a forensic mental health care institution in the Netherlands. Their log data analysis for clients as well as for therapists showed a disappointing implementation outcome. For example, a relatively large group of therapists did not use the WBI at all. The authors concluded that the match between needs of clients, therapists, organization, and the technology was suboptimal. At present, there are too few studies regarding the implementation of WBIs in forensic psychiatry or psychotherapy, especially for ICSOC.
Implementation Barriers for WBIs
Research on the barriers to implementing WBIs in general psychiatry supports the findings of Kip, Sieverink et al. (2020), who identified barriers for health care professionals, clients, and organization. Furthermore, we identified legal and regulatory barriers which arise especially in the use of WBIs for ICSOC. For health care professionals, little knowledge about WBIs and low self-efficacy beliefs in dealing with the new technology appear to hinder the use of WBIs (Titzler et al., 2020; Walthouwer et al., 2017). Uncertainty about how to integrate WBIs into care and the large number of available technologies slow down implementation because most health care professionals feel obligated to be an expert in the technology before using it (Feijt et al., 2018). Another concern is that increased accessibility leads to an increased perceived responsibility, especially in crisis situations. The lack of ethical guidelines and instructions makes this situation difficult and is a source of stress for health care professionals (Feijt et al., 2018). Some implementation barriers on the side of the clients, like negative attitudes toward eMH, reservations regarding data safety, and the limitation of personal contact have already been addressed in the section on criteria for the development of WBIs for ICSOC. In addition, people who have been incarcerated are affected by a higher unemployment rate than the rest of society (Couloute & Kopf, 2018) which leads to limited financial access to electronic devices and an internet connection.
At the organizational level, barriers are related to the organizational capacities, such as knowledge gaps about cyber security and limited knowledge of available services (Wozney et al., 2017). Maximizing profits and integrating WBIs into the organization were considered important facilitating factors for implementation (Walthouwer et al., 2017). In forensic psychiatry and psychotherapy, there are specific problems in the implementation of WBIs. Especially in inpatient treatment, lack of access to the internet or computers is a challenge (Chaple et al., 2014; Elison et al., 2016). This is related to security issues as the internet could be used for criminal activities, like continuation of criminal enterprises, access to child sexual exploitation material, and intimidating individuals affected by the offense. Furthermore, there are a number of practical considerations including cost of equipment, training of staff, and risk management (Champion & Edgar, 2013).
Legal barriers may exist in probation or parole conditions that restrict the use of the internet for ICSOC, especially for those, who consumed child sexual exploitation material (Renberg & Sbano, 2021). In addition, it is unclear whether WBIs can fulfill court-ordered treatment and how risk monitoring of these patients will be conducted. Furthermore, legal and regulatory issues regarding provider compensation of human-supported therapeutic WBIs could arise. The COVID-19 pandemic showed that there is a need for fee codes and billing schedules for providers of telehealth (Basu et al., 2021). If human-supported WBIs for ICSOC are implemented in standard care, practitioners would need some sort of client records to bill for their services. This could threaten the implementation of anonymous WBIs. Furthermore, clarification to the question which practitioners are qualified to treat which clients is required, including, for example provision of therapeutic guidance across country borders.
Criteria for the Implementation of WBIs for ICSOC
To overcome barriers to the implementation of WBIs in forensic psychiatry and psychotherapy, Kip, Sieverink et al. (2020) propose a holistic approach which may include changes in the organization, attitude changes in therapists, and adaptability of the technology. On the level of health care professionals, Kip, Oberschmidt, and Bierbooms (2020) propose that eMH should be integrated in the existing treatment and that technological skills should be disseminated to health care professionals via courses, team meetings, or eMH ambassadors. Of the above-mentioned barriers regarding attitudes, beliefs, and acceptance, we identify the importance of creating acceptance among health care professionals. This could be achieved through clarifying the possible advantages of WBIs and providing transparency in their development and evaluation. Furthermore, ethical guidelines on how to deal with crisis situations should be developed as well as risk protocols especially in the context of new offenses or self-harm. Most of the client-related barriers should be targeted in the developmental stage. In the section criteria for the development of WBIs for ICSOC we have given an overview of how this could be achieved.
On the organizational level, appropriate long-term funding should be secured (Kip, Oberschmidt, & Bierbooms, 2020). In this way, sufficient resources can be guaranteed to provide staff, technical requirements, and technical training. Furthermore, Kip, Oberschmidt, and Bierbooms (2020) propose that an interdisciplinary collaboration on a national level between different types of stakeholders should take place. This allows an exchange of different experiences and strategies. Lack of access to the internet in prisons or forensic security wards could be overcome by providing WBIs on locally secure set-ups such as described by Chaple et al. (2014), who networked their intervention on a stand-alone server with restricted access to other websites. Furthermore, many countries, like Norway and Finland, are increasing the digitization development of prisons and allowing incarcerated person access to the internet (Järveläinen & Rantanen, 2021). Thus, a positive perspective for the use of WBIs in prisons is apparent.
Regarding the legal and regulatory issues, there is a need of clear guidelines and a legal framework for delivering WBIs for individuals who offended. Restrictions regarding the internet use of ICSOC would need to be modified to allow access to WBIs. Furthermore, the legislator should clarify if WBIs are appropriate for court-ordered patients and how the risk-monitoring of these patients is conducted when using a WBI. Legal and regulatory guidelines should clarify the guidance process by licensed practitioners. However, these criteria lie in the field of responsibility of the legislator and the health care provider and therefore depend on the respective country. The implementation criteria are summarized in the third column of Table 2.
Implementation Criteria in Practice
The WBIs for ICSOC that can be considered already implemented are all self-help WBIs without guidance. Looking at these WBIs, it becomes clear that not all implementation criteria are relevant for every type of WBI. For example, the criterion to integrate a WBI in an existing treatment situation may not be feasible for a self-help WBI. In addition, without a link to a treatment facility or health care professionals, it is not possible to offer individuals further support. However, WBIs without guidance should also meet the criteria of fulfilling technological prerequisites or securing appropriate long-term funding. This indicates that to find the best way for implementing a WBI, an individual assessment that considers the goal of the WBI and the target group, is necessary. The implementation status of all WBIs mentioned in this article can be found in Table 1.
Conclusion
Studies on eMH in general and forensic psychiatry and psychotherapy identify the potential benefits of WBIs for ICSOC. We found six published WBIs that differ primarily in terms of the guidance, access options, and target group. Up to now, however, it is unclear, which effects these WBIs have (e.g., reducing dynamic risk factors or preventing recidivism). It is unclear which components could cause the effect (e.g., program content, multimedia usage, provision of interactive online activities, or provision of guidance). It is further unclear for whom they are effective (e.g., individuals who consumed child sexual exploitation material, individuals who committed sexual offenses against children, or individuals who are sexually interested in children). Finally, it is unclear if they are cost-effective. The WBIs @myTabu and Prevent It are both preregistered for a clinical trial and could be a first step in answering some of these questions.
Criteria for the development, evaluation, and implementation of WBIs for ICSOC were derived from previous research. The criteria found could be relevant for WBIs for other forensic target groups as well, for example the criterion on following the RNR principle. Future research should investigate possible differences and similarities regarding the development, evaluation, and implementation. When looking at the small but heterogeneous spectrum of WBIs for ICSOC, it becomes clear that there cannot be universally valid criteria for every form of WBI. Depending on the goal, target group, and application field (e.g., secondary or tertiary prevention) the criteria for development, evaluation, and implementation are to be rated differently in terms of their importance and feasibility. Future research should examine in depth which criteria should be met by which type of WBI. Nonetheless, the criteria provided in this work are important guidelines for researchers and health care professionals who want to develop a WBI for ICSOC.
Footnotes
Authors’ Note:
The authors have no conflict of interest to disclose. Our work was funded by the German Federal Ministry of Education and Research (BMBF, Funding number:748 01KR1807A). The publication was created as part of the @myTabu research—consortium. Sonja Schröder and Louisa Bauer contributed equally to this work and share first authorship.