
Abstract
Given the increasing literature on forensic assertive community treatment (FACT), we conducted a systematic review and meta-analysis to explore the effectiveness of FACT among justice-involved individuals with severe mental illness. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. Sixteen studies were included in the systematic review, six of which were included in the meta-analyses for a total of 1,246 participants. Mixed results regarding health-related outcomes were found. The pre-post FACT analysis and comparison with control groups did not yield significant results other than increased outpatient service use. Results on forensic outcomes were more compelling. Both the narrative review and the meta-analysis highlighted that FACT programs may improve justice outcomes such as the number of days spent in jail. More high quality and multisite randomized controlled trials are needed to consolidate findings. Further research is needed to examine other psychosocial factors related to FACT program success.
Upon release into the community from forensic and correctional settings, individuals with a severe mental illness (SMI) are at risk of recidivism, including rearrest and reincarceration, as well as at risk of premature mortality and rehospitalization (Angell et al., 2014; Baillargeon et al., 2009; Charette et al., 2015; Fox et al., 2014; Frank et al., 2013; Gagliardi et al., 2004; Skeem et al., 2009) with an increased likelihood when there is a lack of adequate connections to mental health services following release (Osher & Thompson, 2020).
Evidence-based programs to prevent recidivism and enhance community integration are essential given most people convicted of a crime are either currently in the community or will ultimately return to it (DeLuca et al., 2018). In this regard, given the evidence base of assertive community treatment (ACT) teams (Burns, 2010; Dixon, 2000; Mueser et al., 1998; Nelson et al., 2007; Phillips et al., 2001), forensic assertive community treatment (FACT) was developed to help transition justice-involved individuals with SMI into community treatment (DeLuca et al., 2018). FACT programs have been put forth to divert persons with mental illness away from correctional and forensic settings while providing comprehensive team-based services with a small case manager to consumer ratio (Cusack et al., 2010). FACT enhances the ACT model by also targeting criminal justice components and building relationships with the justice system (DeLuca et al., 2018). In addition, distinctive FACT targets individuals with prior arrests, accepts referrals from the justice system, integrates justice providers, and uses court sanctions to encourage participation while making rearrest prevention a goal (Lamberti et al., 2004). FACT programs address both mental health and criminogenic needs, consistent with best practices for justice-involved individuals with SMI as proposed by the risk-need-responsivity (RNR) model (Bonta & Andrews, 2007; Morgan et al., 2010), and thus, FACT is expected to yield better outcomes for these individuals than standard ACT teams that generally failed at reducing criminal justice outcomes (Lamberti et al., 2004).
Although evidence for ACT is well-documented (Burns, 2010; Dixon, 2000; Mueser et al., 1998; Nelson et al., 2007; Phillips et al., 2001), FACT remains relatively underutilized/understudied partly due to its nascency, intervention heterogeneity (Landess & Holoyda, 2017; Marquant et al., 2016; Morrissey, 2013), and the smaller number of teams. FACT effectiveness has been limited by methodological issues (e.g., nonrandomization, limited follow-ups, variability in program structure, different program eligibility criteria; Cuddeback et al., 2009; Lamberti & Weisman, 2010; Morrissey et al., 2007; Osher & Thompson, 2020). Consequently, results from these programs have been variable, with some authors reporting significant reductions in negative outcomes (Cimino & Jennings, 2002; McCoy et al., 2004; Weisman et al., 2004; Wilson et al., 1995) and others failing to observe such significant outcomes or observing the opposite (Cosden et al., 2005; Cusack et al., 2010; Solomon & Draine, 1995). A review by Marquant et al. (2016) concluded that FACT had generally positive effects on forensic outcomes such as convictions, arrests, and days in detention. Additional studies have been published since including an RCT (Lamberti et al., 2017) and a comparative study (Marquant et al., 2018). With the growing FACT literature, there has yet to be a meta-analysis to investigate the effectiveness on justice and health outcomes. We therefore chose to conduct a systematic review and meta-analysis to narratively describe and quantitatively explore the effectiveness of FACT in justice-involved individuals with SMI.
Method
Selection Procedure
Search Strategy
The literature search was conducted through PubMed, PsycINFO, Embase, and Google Scholar to identify all relevant studies reporting the effectiveness of FACT (inception of each database up until February 2020). Librarians helped identify the most appropriate search strategy. Searches used text words and indexing terms (MeSH) with key words that were inclusive for FACT (e.g., ACT), mental illness (e.g., mental disorder, psychiatric), and forensic setting (e.g., forensic psychiatry, prison, jail). No setting, date, or geographical restrictions were applied. Searches were limited to English and French language sources. Additional records were identified through cross-referencing. In addition, authors of the studies included were contacted to obtain any additional manuscripts that may not have been published or found during the initial database search. Throughout the screening procedure, an independent researcher (M.H.G.) supervised two graduate students (L.D. and C.L.D.) who separately assessed articles. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed (Moher et al., 2009). The research protocol has been prospectively registered (PROSPERO #156647).
Study Selection
Studies first underwent full-text eligibility screening for inclusion in the systematic review. Studies were included so long as they met the following criteria:
FACT comprised a hybrid functioning including components of ACT and forensic rehabilitation (i.e., Lamberti et al., 2004; Morrissey et al., 2007),
the sample included justice-involved adults with SMI (i.e., schizophrenia, bipolar disorder, major depression) living in the community,
the study was a retrospective or prospective study or an RCT,
an indicator of forensic and/or health outcome was measured. Forensic outcomes included jail days and number of arrests, incarcerations, bookings, or convictions, whereas health outcomes included number of psychiatric hospitalizations, hospital days, and outpatient service use.
The additional criterion to conduct the meta-analysis consisted of a statistical association that was available or could be calculated using Standardized Mean Differences (SMD). Authors disagreed on the inclusion of 5% of studies that were screened, and disagreements on study inclusion were resolved through group discussions. Studies were excluded if (a) they evaluated regular ACT with no forensic component or did not explicitly explain how forensic rehabilitation was addressed, and (b) the approach comprised in-reach prison care.
Data Extraction
Data extraction was double-checked to ensure consistency. Quality assessment was independently undertaken by L.D. and C.L.D. against a set of criteria based on the GRADE Checklist, and discussions were held with M.H.G. to ensure consensus (Guyatt et al., 2011a, 2011b, 2011c, 2011d). Studies were coded: high, moderate, low, or very low quality.
Analyses
Forensic and health outcomes were first narratively reviewed, and studies that contained methodological inadequacies to compute any effect size could not be included within the meta-analyses. Then, meta-analyses were conducted by a statistician separately for the two main outcome groups (all forensic outcomes, all health outcomes). Globally, the meta-analyses evaluated (a) the pre-post effectiveness of FACT alone and (b) the comparison between FACT with a control group. For the meta-analyses, data were entered into an electronic database and analyzed with a quantitative meta-analytical approach using R version 3.6.2 (R core team) and the metafor package (Viechtbauer, 2010). Effect sizes were reported with 95% confidence intervals (CI). Given some analyses included more than one statistic per study to account for the whole range of outcome subtypes, a multilevel meta-analysis was carried out. This type of analysis allows to account for intraclass variation for statistics from the same paper. We therefore refer to the term “study arms” to describe the number of statistics considered within the meta-analyses that have been provided from the included studies. The following qualitative descriptions of the strength of reported SMDs were used: small (0.2), medium (0.5), and large (≥0.8; Cohen, 1992). Heterogeneity among study point estimates and residuals of the meta-regressions was assessed with Q statistics (Paulson & Bazemore, 2010) and quantified with I2 index (Lipsey & Wilson, 2001). As substantial heterogeneity was observed (see results below), we employed random-effects models (Cooper et al., 2009). Publication bias was examined with funnel plots, Egger’s test (Egger et al., 1997), and the Fail-Safe N method (Orwin, 1983; Rosenthal, 1979). The latter provides an estimate of the number of studies with null findings needed to drop the effect sizes to nonsignificance. Further subanalyses were conducted for the pre-post FACT analyses as studies used different time intervals, that is, the time before and after having entered FACT. We used a dispersion plot of the outcome on the mean timeline as a moderator and examined whether the pre-post timeline made a difference on the levels of the standardized difference; meta-regressions followed to confirm findings (only significant results are reported for this subanalysis). Subanalyses were also conducted on the different subcategories of the main outcomes (i.e., jail days as a criminal outcome, hospital days as a health outcome).
Results
The literature search identified 107 potential papers that were screened for eligibility after removing duplicates; six additional studies were identified by cross-referencing and Google Scholar searches. After excluding papers that did not meet our inclusion criteria, 16 eligible papers remained and were included in the systematic review and six of these were included in the meta-analyses for a total of 1,246 justice-involved adult participants with SMI. Six studies were RCTs (one graded as being of high and five graded as being of moderate quality evidence) and 10 were either retrospective or prospective longitudinal studies (three graded as being of very low, six graded as being of low, and one graded as being of high quality evidence). The PRISMA flowchart for the inclusion of studies is found in Figure 1. The details of the retrieved studies are briefly described in the Supplemental Material (available in the online version of this article).
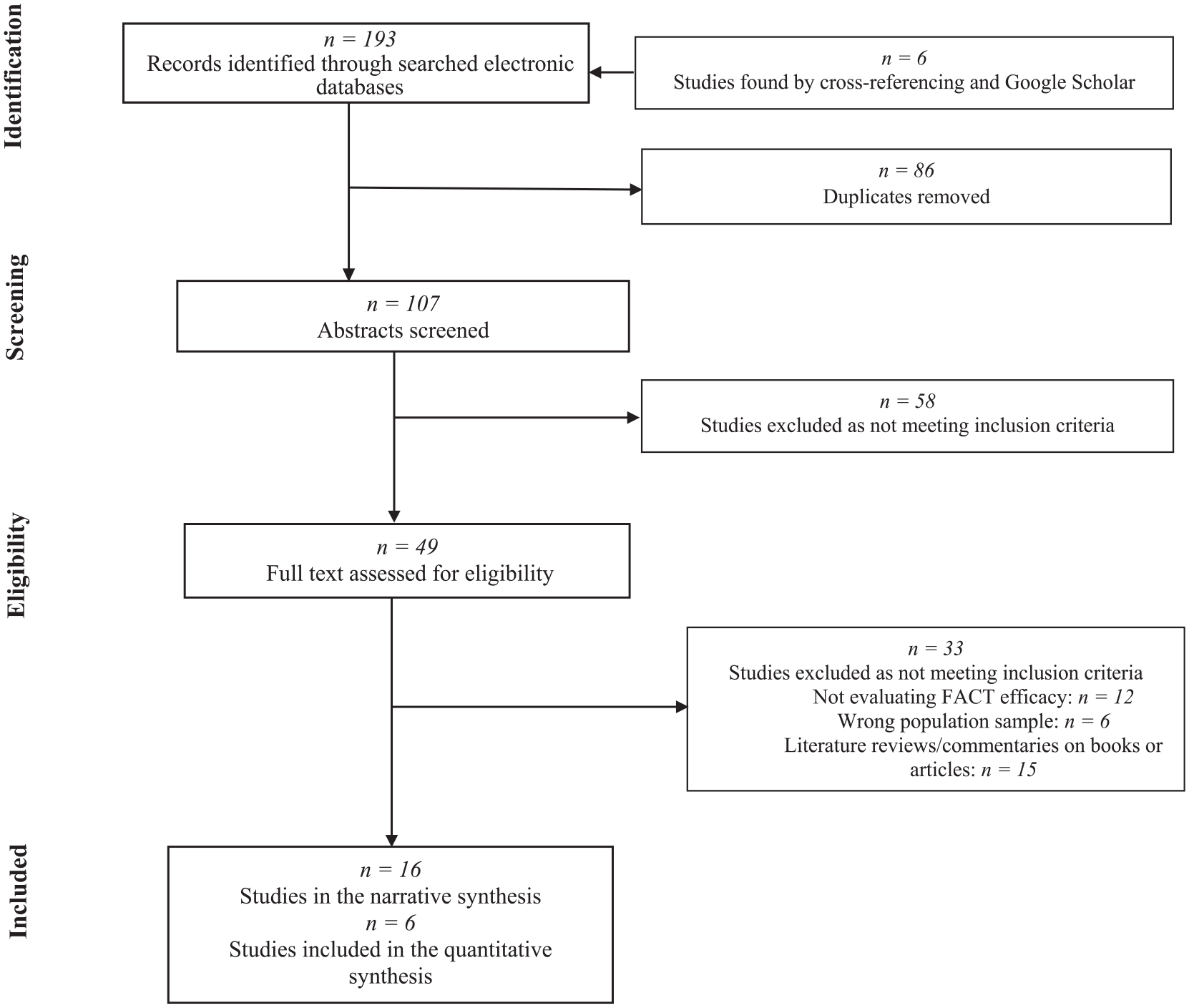
Flowchart Depicting the Search Strategy Employed to Find the 16 Studies Included in the Review
Forensic Outcomes
Systematic Narrative Review
Among the 16 studies identified, nine had no controls, one had a comparison with a control, and six were RCTs. For studies with no controls, the results from the Arkansas Partnership Program by Cimino and Jennings (2002) and Smith et al. (2010) found that 7% of participants were rearrested and 1% was reincarcerated over 7 years. Similarly, in a 7.5-year retrospective study by Simpson et al. (2006), nine patients (18.8%) were re-offended, six patients (12.5%) were reconvicted, and five patients (10.4%) were re-imprisoned of the 48 participants who were discharged from their FACT care. In a 5-year retrospective study, Parker (2004) found an overall rate of 0.02 arrests/participant/year, with none of the arrests resulting in a prison sentence. In a single group pre-post study, individuals who completed 1 year of Project Link (Lamberti et al., 2001; Weisman et al., 2004) had significant reductions in jail days, arrests, and average number of incarcerations. Thresholds State-County Collaborative Jail Linkage Project as well showed 1 year decreases in the number of jail days and arrests by over 90% and 70%, respectively (McCoy et al., 2004). Kelly et al. (2017) followed patients at a 9-month follow-up from Thresholds’ FACT reentry program and found an average 38% reduction in arrests and 21% for incarcerations. Interestingly, Davis et al. (2008) observed that length of the Thresholds Jail Project aftercare and jail days were related; those receiving services for 1 year or less, on average, displayed 76.28 more postservices jail days.
Studies with controls are more helpful in examining the effects of FACT. Marquant et al. (2018) analyzed retrospective data on 70 FACT clients and found significantly better forensic outcomes in comparison with discharged patients receiving general community-based care, including lower arrest (2.8% vs. 16%) and incarceration rates (4.3% vs. 58%) at a 33-month follow-up. Using more rigorous methodologies from RCTs, FACT programs displayed similar trends to treatment-as-usual, but they also appeared to lead to more significant improvements. The earliest RCT conducted by Solomon’s team (1994, 1995) has failed to show any statistically significant differences between groups, although FACT had a higher rearrest rate largely due to technical violations. In the first RCT by Cosden et al. (2003) on 1-year outcomes, a similar proportion of clients in each condition had been booked at least once and spent some time in jail (76% in FACT vs. 72% in treatment-as-usual). However, there were differences in the proportion of clients convicted of a new offense (47% for FACT vs. 60% for treatment-as-usual). In their second study over a 2-year follow-up (Cosden et al., 2005), people convicted of a crime with more jail days in both groups experienced more jail activity after entering treatment, whereas outcomes for the remaining people both showed a greater reduction in jail days relative to treatment-as-usual. At 12 months following enrollment in the study by Cusack et al. (2010), FACT participants had significantly fewer jail bookings than did usual care participants. FACT participants had a higher probability of avoiding jail in the post period, although once jailed, the number of jail days did not differ between groups. At 24 months following enrollment, the results followed a similar pattern. The more recent RCT by Lamberti et al. (2017) found that individuals who received the FACT intervention had fewer convictions for new crimes and fewer days in jail in comparison with treatment-as-usual at 1-year follow-up. No significant between-group differences were observed in number of arrests or incarcerations.
Meta-Analysis
Pre-post FACT
For the pre-post analysis on FACT, six studies with 15 study arms on overall forensic outcomes were available. The pooled effect size of these outcomes indicated fewer forensic outcomes over time for FACT (SMD = −0.48, 95% CI = [−0.69, −0.26], p < .001; Figure 2A). The database was characterized by a high level of heterogeneity (Q = 171.7, p < .001, I2 = 91.08%). When viewing the funnel plot (Figure 3A), five study arms were found to be outside the funnel. The removal of these study arms did not change the significance of results (SMD = −0.47, 95% CI = [−0.60, −0.33], p < .001). However, it did reduce the level of heterogeneity (Q = 24.14, p = .004, I2 = 53.48%). Moreover, while Egger’s asymmetry test showed a statistically significant deviation from symmetry with all study arms (t = −3.33; p = .005), there was no longer any statistically significant deviation upon removal of the five study arms (t = −1.41; p = .20). The Fail-Safe N method indicated that 811 studies would be needed to nullify significant results with all study arms and 434 studies upon removal of the five study arms.
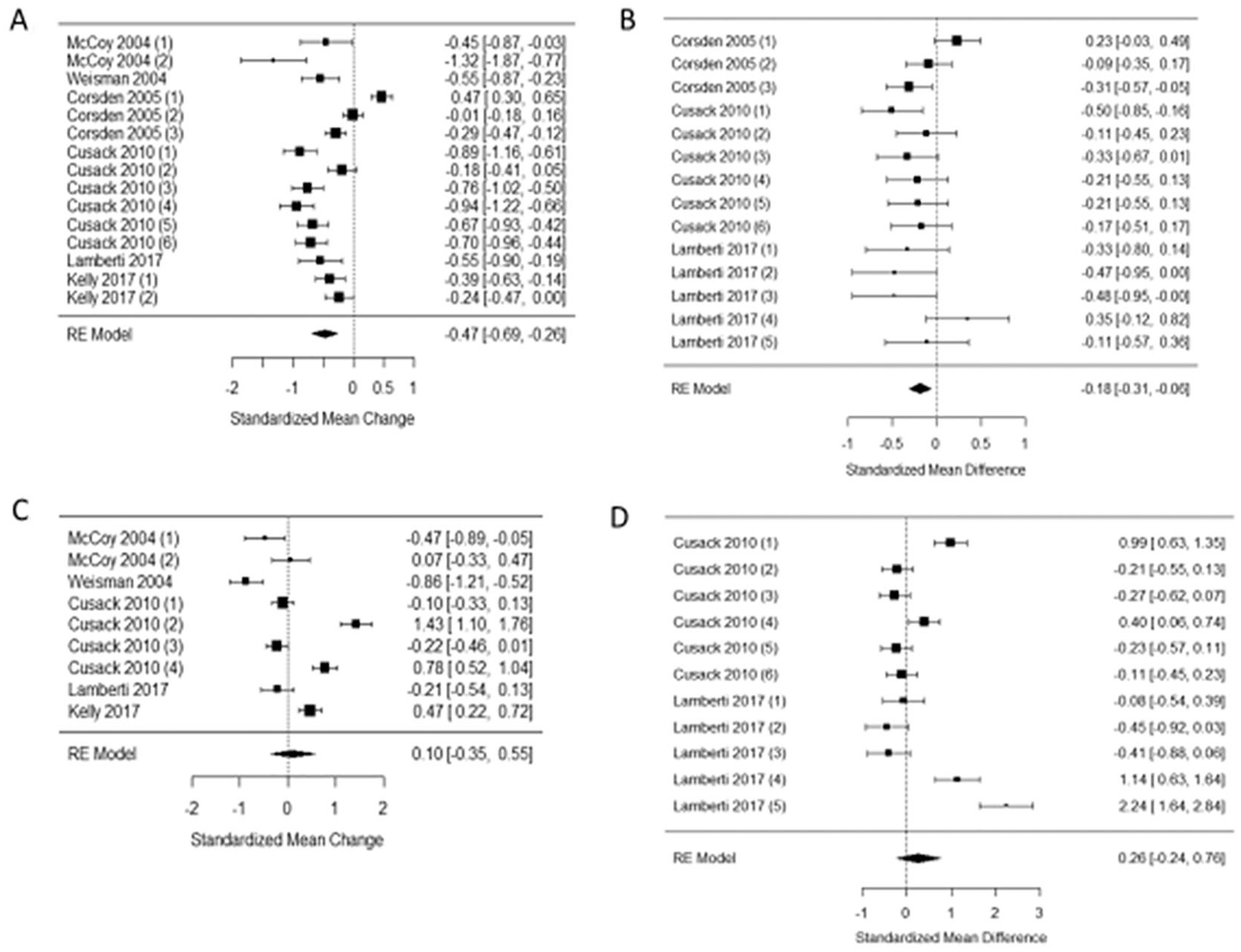
Forest Plot of the Efficacy of FACT on Forensic and Health Outcomes in Justice-Involved Individuals With Severe Mental Disorders
For subanalyses, we first tested if the pre- and post-timeline of all study arms explained some heterogeneity across the studies. There was evidence that pre-FACT timeline made a difference on the levels of standardized difference. This was confirmed via meta-regression. Studies using a prior 12-month timeline had a pre-post SMD of 0.6 lower than the studies using a 24-month timeline. This suggests that studies that had a prior mean 24-month timeline had no pre-post statistically significant result. Consequently, studies with participants who had previously accessed FACT in less than a year had reduction of forensic outcomes from pre- to post-FACT. The post-timeline was not associated with these outcomes.
With the subanalysis distinguishing categories of forensic outcomes, it may be hypothesized that the overall effect detected in previous analyses was mainly driven by the difference in the mean number of jail days. While the heterogeneity in residuals was still high (p < .001) and partly explained by the subtype of criminal outcomes (p = .003), there was no evidence of publication bias. Amid the forensic outcomes observed (jail days, arrests, booking, convictions, and incarceration), jail days was the only measure that was statistically significant (SMD = −0.67, 95% CI = [−1.05, −0.30], p < .001).
FACT versus control
For the comparative analysis, three studies with 14 study arms on overall forensic outcomes were available. The combination of studies indicated significantly fewer forensic outcomes in the FACT group as compared with controls (SMD = −0.18, 95% CI = [−0.31, −0.06], p < .005; Figure 2B). The database was characterized by a moderate level of heterogeneity (Q = 23.75, p = .034, I2 = 44.23%). Funnel plot indicated that two study arms had values outside the funnel (Figure 3B). Removing these two study arms provided a similar effect size (SMD = −0.25, 95% CI = [−0.35, −0.15], p < .001) and reduced the heterogeneity between studies (Q = 7.09, p = .79, I2 < 0.001%). Egger’s test indicated no publication bias with (t = −0.95; p = .36) or without (t = −1.29; p = .23) the two study arms. The Fail-Safe N method indicated that 62 and 102 studies with null findings would be needed to drop the effect sizes to nonsignificance with and without the two outliers, respectively.
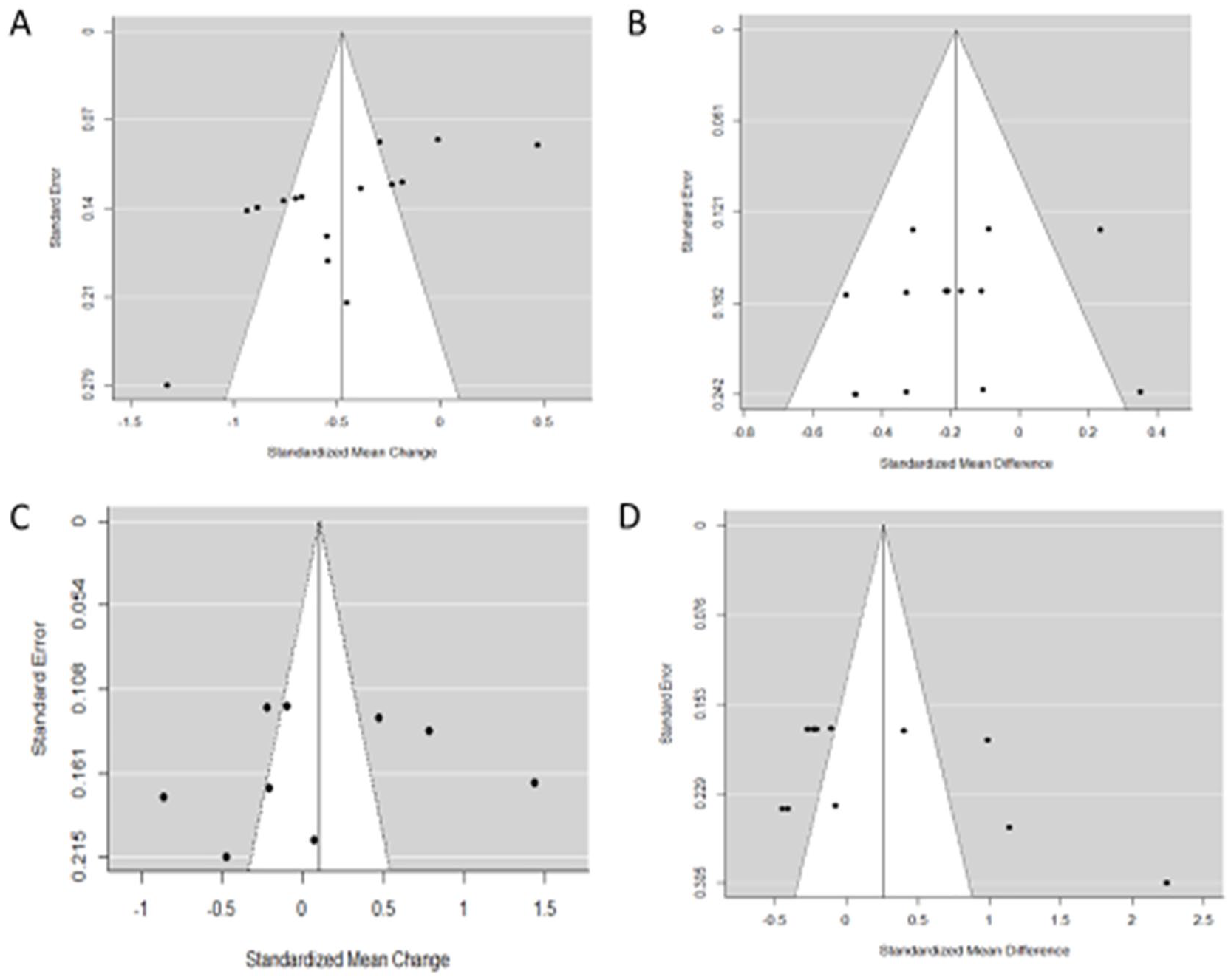
Funnel Plot of the Meta-Analysis
When considering a subanalysis per forensic outcome, the overall effect detected in the previous analyses may have been mainly driven by the difference in the mean number of jail days. The heterogeneity in residuals was no longer statistically significant (p = .06), and it was partly explained by the subtype of criminal outcomes (p = .028). Egger’s test indicated no publication bias (t = −2.08; p = .08). Amid the forensic outcomes observed (jail days, arrests, booking, convictions, and incarceration), jail days was the only measure that was significantly lower than the comparison group (SMD = −0.31, 95% CI = [−0.54, −0.07], p = .01).
Health Outcomes
Systematic Narrative Review
Among the studies reporting health outcomes, nine had no controls, one had a comparison with a control, and three were RCTs. For studies with no controls, Davis et al. (2008) showed that exposure was significantly associated with a reduction in hospital use postservices. Parker (2004) observed that overall hospitalization rate was 0.2 hospitalizations/participant/year. Combining the results by Cimino and Jennings (2002) and Smith et al. (2010), 20% and 9% had a readmission to residential care and hospitals, respectively. In accordance, Simpson et al. (2006) found that 19% were readmitted to a forensic hospital. In the single group pre-post study, individuals who completed 1 year of Project Link (Lamberti et al., 2001; Weisman et al., 2004) had significant reductions in the number of hospitalizations and over 90% reduction in hospital days. McCoy et al. (2004) also observed notable reduction of over 75% in hospitalizations and hospital days after a year of enrollment. However, Kelly et al. (2017) found that 48% of the sample was hospitalized with an increase in number of hospitalizations from a mean of 0.76 two years prior to 1.57 at the 9-month follow-up.
Studies with control groups yielded to less clear-cut results; most found increased hospitalizations and outpatient care, but fewer hospital days. Marquant et al. (2018) found that rehospitalization rates were significantly higher for FACT than treatment-as-usual. The FACT group was over 21 times more likely to have at least one hospital admission during the follow-up compared with patients in the control group. Accordingly, in the RCT by Cosden et al. (2005), more participants in both groups utilized mental health services; however, a higher proportion of FACT than treatment-as-usual patients were engaged in these services at the 6-, 12-, 18-, and 24-month follow-ups. As for amount of treatment use, participants in treatment-as-usual used a similar number of hours of treatment throughout the 24 months, while FACT participants used a greater number of services early in the program and fewer at the 24-month assessment after the enhanced treatment ended. Cusack et al. (2010) found that participants in the FACT group had more than twice the rate of outpatient visits than treatment-as-usual participants, but fewer days of psychiatric hospitalizations in their 1- and 2-year follow-up. A similar pattern was observed in Lamberti et al. (2017), with the FACT program having fewer than 81% reduction of hospital days, but an 80% increase in days spent in outpatient mental health treatment compared with treatment-as-usual at a 1-year follow-up. FACT group participants had significantly less emergency room visits compared with control group participants.
Meta-Analysis
Pre-post FACT
For the pre-post analysis on FACT, five studies with nine study arms on overall health outcomes were available. The pooled effect size of these outcomes indicated no statistically significant effects (SMD = 0.10, 95% CI = [−0.35, 0.55], p = .66; Figure 2C). The funnel plot showed that only a few study arms had values inside the funnel (Figure 3C), which might indicate either the presence of publication bias or that meta-analyses should be considered by subtypes. Egger’s test showed no evidence of publication bias (t = −0.34; p = .74) and the Fail-Safe N method was of 12 studies, although a high level of heterogeneity was observed (Q = 146.7, p < .001, I2 = 95.29%).
Heterogeneity was partly explained by analyzing the subtypes of health outcomes. However, the heterogeneity remained large in the residuals (I2 = 89.30%). Amid the other health outcomes (hospital days, hospitalization, treatment days), only the level of outpatient visits was higher post-FACT in comparison with pre-FACT (SMD = 1.10, 95% CI = [0.47, 1.73], p < .001). All residual values were centered around zero, suggesting that the funnel plot of the main outcome effect may have been odd due to the diverse nature of the different health outcomes, which implies that they must be examined within each subtype.
FACT versus control
For the comparative analysis, two studies with 11 study arms on overall health outcomes were available. The combination of studies indicated no significant differences between FACT and control groups (SMD = 0.26, 95% CI = [−0.24, 0.76], p = .29, Figure 2D). The funnel plot indicated that only two study arms had values inside the funnel (Figure 3D). Egger’s asymmetry test showed no statistically significant deviation from symmetry (t = 1.46; p = .18) and the Fail-Safe N method was of 32 studies, although the database was characterized by a high level of heterogeneity (Q = 114.3, p < .001, I2 = 94.27%).
When considering a subanalysis per subtype of outcome, the level of outpatient visits was higher in the FACT group than in the control group (SMD = 1.15, 95% CI = [0.51, 1.79], p < .001). No significant difference was observed for crisis resources, emergency department, hospital days, hospitalization, and treatment days. Heterogeneity was partly explained by analyzing subtypes of health outcomes. However, the heterogeneity of residuals remained large (I2 = 89.37%). As in the previous section, the residual values were centered around zero.
Discussion
Our systematic review and exploratory meta-analysis aimed to synthesize the literature on the effectiveness of FACT programs on both forensic- and health-related outcomes. Our review provided mixed results regarding health-related outcomes, which was further confirmed in our meta-analytical investigation. The pre-post FACT analysis and comparison with control groups did not yield any significant results apart from an increase in outpatient service use. Considering the characteristics of this population, the other health outcomes, such as hospitalization or the use of emergency services, might need to be reconsidered. Indeed, rehospitalization may not always be negative and may actually be preventive to violence or other criminal behavior when done in a timely manner. To divert this population from the criminal justice stream, these findings are also consistent with those regarding mental health courts that have also observed increased frequency of contact with health providers (Lemieux et al., in press). Moreover, these findings suggest that further attention should be given to other health outcomes to better understand the possible benefits of FACT. For example, Cosden et al. (2005) found an improvement in patients’ global functioning, life satisfaction, psychological distress, and drug and alcohol use.
Results on forensic outcomes were more compelling. Both our narrative review and meta-analysis highlighted that FACT programs in such at-risk populations may be beneficial to improve forensic outcomes. Meta-analytical data from pre-post studies of FACT showed a moderate reduction on overall forensic outcomes, which was mainly driven by the difference in mean jail days. Our results showed significant reductions on overall forensic outcomes in comparison with control groups as well, which was again mostly driven by the significant difference in jail days. Given that the prevention of recidivism is a central goal of FACT (Lamberti et al., 2001), this result is promising.
These findings may be explained by FACT integrating and adjusting their services to accommodate the different client profiles (i.e., addiction problems, antisocial traits). FACT teams consequently ensure and facilitate access to a wide variety of services (e.g., mental health and addictions, vocational, residential) and deliver these services through outreach (DeLuca et al., 2018). However, while the Rochester FACT model specifically integrated forensic rehabilitation aspects by targeting criminogenic risk factors and using legal leverage to engage participants in treatment (Lamberti et al., 2017), other studies included failed to provide specific information on this matter. Given the specificity of FACT is the integration of both mental health services and forensic rehabilitation models, the fact that many programs struggle to integrate the specific needs of justice-involved individuals must be addressed. Models of forensic rehabilitation such as the RNR model (Andrews et al., 1990) could be integrated in FACT programs to ensure that the individual risk factors and needs of each client are considered. The RNR model shows promising relevance for justice-involved individuals with a mental illness, although lacks research data to support it (Skeem et al., 2015); further studies on FACT programs integrating explicitly its principles could not only increase the evidence but also guide clinical practice for FACT team members.
Moreover, collaborative problem-solving could potentially have led to fewer convictions and less jail time among the FACT participants without affecting the actual incidence of new crimes (Lamberti et al., 2017). In the context of community reentry from correctional and forensic settings, the key tasks of intervention are not solely to improve mental health symptomatology but also to engage participants to develop new identities, restore connections to the community, and abstain from committing crimes (Maruna, 2001). Other psychosocial outcomes such as housing, vocational, leisure, and general recovery pathways may be more relevant.
Some limitations should be taken into account when interpreting the current findings. First, our meta-analyses have been conducted on a small number of studies and therefore should be considered as being exploratory in nature. We nevertheless attempted to identify unpublished results or data that may have been missed by contacting the first authors of included studies. Overall, more investigation on the subject is warranted as more studies emerge. Second, the level of heterogeneity between studies was fairly large. This may partly be due to differing FACT across studies approaches. While new programs appeared to maintain similar ingredients (e.g., probation officers and residential components), it has been noted that FACT programs continue to show a significant degree of variability in terms of structure and function, for example, by differing in regard to the length of exposition to the program (DeLuca et al., 2018). Studies have also shown differing standardized admission criteria (e.g., diagnoses and demographics), with some programs having tended to exclude high-risk patients, clients with a primary personality disorder, or violent offenders (Cimino & Jennings, 2002; Cusack et al., 2010; Parker, 2004; Solomon & Draine, 1995; Solomon et al., 1994). This highlights the need to assess the fidelity of the approach by using a standardized fidelity scale, such as the Forensic Assertive Community Treatment Scale (FACTS; Lamberti et al., 2017). Third, caution should be taken considering methodological limitations and differences, including study designs, small sample sizes, lack of long-term follow-ups, lack of adjustment for confounding factors, and lack of outcome data beyond service utilization. These elements in addition to the fact that most studies were conducted in the United States might preclude generalization to many jurisdictions.
Conclusion
Although current research on FACT consists of a few studies with variable programming and methodologies, findings suggest moderate effectiveness of FACT on forensic outcomes for justice-involved persons with SMI. More high quality, multisite, RCTs are needed to consolidate findings and show their reproducibility across diverse communities and jurisdictions. Fidelity scales such as the Rochester Forensic Assertive Community Treatment Scale (RFACTS; Lamberti & Weisman, 2021) should be embedded in the studies, so the key ingredient or combination of ingredients may be identified and may enhance comparability across studies. More research is needed to explore other factors related to FACT program success. Mixed-methods research would also supplement this evidence base by integrating participants’ experiences of FACT.
Supplemental Material
sj-pdf-1-cjb-10.1177_00938548211061489 – Supplemental material for Effectiveness of Forensic Assertive Community Treatment on Forensic and Health Outcomes: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-cjb-10.1177_00938548211061489 for Effectiveness of Forensic Assertive Community Treatment on Forensic and Health Outcomes: A Systematic Review and Meta-Analysis by Marie-Hélène Goulet, Laura Dellazizzo, Clara Lessard-Deschênes, Alain Lesage, Anne G. Crocker and Alexandre Dumais in Criminal Justice and Behavior
Footnotes
Author’s Note
The authors would like to thank Marie Désilets, librarian at the Institut universitaire en santé mentale de Montréal, for her contribution to the search strategy. M.H.G., C.L.D., L.D., A.L., and A.D. designed the review protocol. M.H.G. and C.L.D. conducted the literature review and drafted the manuscript. L.D., C.L.D., and A.D. conducted the meta-analysis. L.D., A.L., A.C., and A.D. provided feedback, contributed to writing, and revised the manuscript. All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors. All authors are in agreement with the manuscript. M.H.G. is backed by a Recruitment and Retention Fund from the Fondation de l’Institut universitaire en santé mentale de Montréal. The authors declare no conflict of interest.
Authors Note
Anne G. Crocker now affilated to Université de Montréal
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.