
Abstract
Supportive communication can benefit people coping with the stigma that often accompanies mental or emotional distress; however, people might be reluctant to seek support effectively, if at all, for these types of stressors. Guided by the paradox of support seeking, this study expands understanding of how and why people seek support by examining multiple dimensions of stigma, exploring factors that hinder or facilitate people’s decision to seek support, and investigating nuanced support seeking behaviors in the context of mental or emotional distress. Results (N = 406) revealed that internalization and visibility of stigma differentially impacted strategies people chose to seek support. Whereas visibility corresponded with direct seeking and more emotional content, internalized stigma was associated with avoidance. Perceived costs served as barriers to seeking support, and efficacy buffered against the negative consequences of stigma by encouraging direct seeking and allowing for greater depth and emotional content when seeking support.
Seeking and subsequently receiving support benefits people experiencing stressful situations, and ample research demonstrates the positive impact of supportive communication on mental health (e.g., High & Dillard, 2012; Smith et al., 2008). Specifically, effective support may ease emotional distress (Cutrona & Suhr, 1994), increase self-efficacy (High & Scharp, 2015), and motivate positive health behaviors (Pauley & Hesse, 2009). Reaping the benefits of quality supportive communication often requires that support be sought; support rarely materializes without people seeking it (High & Scharp, 2015). In fact, some scholars have labeled seeking support as the first act in the process of supportive communication, with subsequent behaviors often hinging on how people seek support (Barbee & Cunningham, 1995).
The majority of research on supportive communication has focused on how people provide and process, rather than seek, support. Scholars (Barbee & Cunningham, 1995) have explored seeking support in terms of direct and indirect strategies, but less research has examined other ways in which seeking support varies or the cognitive processes guiding whether and how people seek support. Seeking support often occurs across messages and interactions, and people may use a variety of strategies to communicate their need for support (Goldsmith, 1995). Further examination of the factors that shape supportive communication is valuable because identifying predictors of different strategies allows for a more in-depth explanation of what facilitates and hinders seeking support. Despite the benefits of support for reducing feelings of isolation (Smith, 2007), it can be challenging to seek support when coping with potentially stigmatizing experiences, such as mental or emotional distress (Corrigan et al., 2014).
Mental or emotional distress is a common stressor (National Institute of Mental Health [NIMH], 2022), and seeking support within this context is likely impacted by the presence of stigma (Corrigan, 1998). When people feel stigmatized, they may employ different strategies to seek support than people who feel less stigma (Goffman, 1963; Smith, 2007). Guided by the paradox of support seeking (Williams & Mickelson, 2008), the current study extends previous work on stigma and seeking support in three main ways. First, we examine the multidimensionality of stigma by exploring how the visibility and internalization of stigma related to mental or emotional distress shape decisions regarding whether and how to seek support for that distress. Visible and internalized stigma elicit different perceptions and outcomes (Flanagan & Davidson, 2009; Herek & Glunt, 1995), and examining both components of stigma enables researchers to draw conclusions about the relation between specific attributes of stigma and how individuals seek support. Second, we identify and test barriers and buffering factors that explain the relation between stigma and seeking support. Feelings of stigma often inhibit communication (Smith et al., 2016), yet factors protecting against its deleterious effects exist (Smith & Bishop, 2019). This study advances scholarship by investigating barriers and buffers associated with stigma on people’s impressions of how they seek support when experiencing mental or emotional distress (Chaudoir & Fisher, 2010; Goldsmith & Parks, 1990). Finally, variations in the strategies people use to seek support are examined to provide a more complete understanding of how people facing stigma regarding mental or emotional distress seek support pertaining to that distress. Many studies focus on direct and indirect support seeking, which obscures other dimensions on which supportive behaviors vary and deemphasizes the idea that people might avoid seeking support.
Mental or Emotional Distress
Experiences of mental or emotional distress 1 exert significant personal, emotional, and relational consequences. Young adults have the highest rates of mental or emotional distress in the United States, but the lowest rates of received treatment (NIMH, 2022). Seeking support for mental or emotional distress could be valuable; however, mental health-related stigma may serve as a barrier to effectively seeking treatment and/or social support (Johnstone, 2001). Formal support is sometimes inaccessible or too costly (Corrigan et al., 2014), leading many people to turn to their social networks for support (Oliver et al., 2005), but even these informal forms of assistance can be difficult to access when coping with stigma (Rickwood et al., 2007).
Stigma based on mental or emotional distress hinders both communication and health promotion (Smith et al., 2016). It often reduces self-esteem and self-efficacy (Corrigan et al., 2006), whereas quality supportive communication, such as esteem support, may bolster people’s sense of self (Holmstrom, 2012). In light of the prevalence of mental or emotional distress that people encounter and the often deleterious effects of any corresponding stigma, examining the processes underlying how and why people seek support for mental or emotional distress is an opportunity for scholars to understand the cognitive considerations that lead people to seek support in different ways or even avoid seeking support altogether. Mental or emotional distress is felt when facing a variety of acute and everyday stressors, and that distress is often accompanied by feelings of stigma (e.g., Corrigan et al., 2010). Although stigma has been conceptualized in a variety of ways, including focused on a particular stressor (Miller & Kaiser, 2001) or as a chronic component of someone’s identity (Goffman, 1963), stigma is rooted in the perceptions of a communicator (Meisenbach, 2010). Because perceptions of stigma often shape how people communicate and request assistance (Smith, 2007), we endeavor to examine the associations of that stigma on whether, how, and why people seek support for those stressors.
Supportive Communication
Although the provision and processing of support have received extensive study, the factors shaping how people seek support have received considerably less research attention. Of the limited scholarship on seeking support, many studies focus on the likelihood of seeking support (Ray et al., 2020) and the specific types of support that are desired and sought in certain circumstances (High & Crowley, 2018). Less scholarship explores the factors that influence whether and how people seek support, or variation in strategies used to seek support (Buehler et al., 2019; Goldsmith & Parks, 1990; MacGeorge et al., 2011).
Also referred to as support elicitation (Cutrona et al., 1990) or activation (Barbee et al., 1993), seeking support is defined as an “intentional communicative activity with the aim of eliciting supportive actions from others” (MacGeorge et al., 2011, p. 330). Seeking support is consequential and complex because how people seek support shapes the outcomes of an interaction (Conn & Peterson, 1989), and there are a variety of factors that influence whether and how people seek support. We draw on sensitive interaction systems theory (SIST; Barbee & Cunningham, 1995), which considers internal and external factors that may determine how people seek support and save face when doing so (Floyd & Ray, 2017; Goldsmith, 1994).
According to SIST, support seeking varies along dimensions of direct/indirect and verbal/nonverbal (Barbee & Cunningham, 1995). Although SIST theorizes how people seek support, it has been criticized for its inability to fully capture the range of communicative behaviors that may be used to elicit support (e.g., Goldsmith, 1995). An alternative approach emphasizes the microdynamics of communication to understand how people seek support (Goldsmith, 1995). Along these lines, Goldsmith (1995) identified approach and avoidance behaviors as the main dimensions regarding how people seek support. Because there are many ways that people may approach seeking support, and to further identify common microdynamics, we draw on theories of disclosure (e.g., T. D. Afifi & Steuber, 2009; Chaudoir & Fisher, 2010) to expand the conceptualization of seeking support to include the depth and emotional content used when seeking support, along with directness and avoidance. Doing so adds nuance to describing how individuals seek support, thereby allowing for a more precise understanding of how people communicate their need for support and the factors that can predict variations in these behaviors.
When people seek support, they have to decide what information they wish to disclose and how they will share that information (Barbee & Cunningham, 1995). For example, people may choose to directly disclose information about a stressor (Goldsmith, 1995). Direct strategies of eliciting support often result in the best responses from providers, and they consist of verbal messages that explicitly ask for help, reassurance, and suggestions for how to mitigate the problem (Barbee & Cunningham, 1995). Despite the benefits of directly seeking support, some people might seek support indirectly by providing insufficient information, avoiding discussions of their emotions or details of the situation, or indirectly hinting at a problem without explicitly seeking support (Barbee & Cunningham, 1995; Goldsmith, 1995). Other people might avoid seeking support altogether if they perceive seeking support to be too costly (T. D. Afifi & Steuber, 2009).
Beyond directness, strategies of seeking support might also mimic qualities of disclosure by varying in depth and the emotions people reveal (Barbee & Cunningham, 1995; Chaudoir & Fisher, 2010). For example, people may vary the level of intimacy of personal information when seeking support, and the depth of disclosure positively corresponds with the degree of person-centeredness in the support they receive in reply (Pan et al., 2020). Support seekers may also vary the emotional content they share, which pertains to the level of affect they express (Kring et al., 1994). The present study extends research on seeking support by considering new and understudied strategies people use when seeking support.
Paradox of Support Seeking When Coping With Stigma
The paradox of support seeking (Williams & Mickelson, 2008) asserts that people who perceive stigma often avoid seeking support or communicate their desire for support indirectly as a protective measure, but these attempts often lead to unsupportive responses that reinforce the experience of stigma and result in the very rejection initially feared. Seekers’ expectations for interactions, including the likelihood of rejection and perceived quality of the support provided, shape behaviors pertaining to whether and how support is sought (Rains et al., 2020; Williams & Mickelson, 2008). Feelings of stigma also tend to decrease people’s ability and likelihood of seeking support, especially in the context of mental or emotional distress (Corrigan et al., 2006; Smith, 2007).
The paradox of support seeking is predicated on the assumption that stigma negatively affects the process of seeking support. Feelings of stigma can bias cognitions and influence how people manage a stressor, including how they balance the benefits of receiving support with the risks of revealing a shortcoming to a potential support provider (Goldsmith & Parks, 1990). People often weigh the pros and cons of seeking support for a stigmatized stressor (Williams & Mickelson, 2008). When coping with mental or emotional distress, people’s level of uncertainty (Kuang & Wang, 2022) and expectations for an interaction (Rains et al., 2020) often shape the strategies they choose when seeking support. This calculation of risk and subsequent strategy selection for coping with distress is in line with Williams and Mickelson’s (2008) assertion that, “perceived stigma impacts individuals’ decisions about seeking support from close network members” (p. 495). Because it is not a unidimensional concept, a more nuanced understanding of the role of stigma in Williams and Mickelson’s (2008) model could advance our knowledge of the factors people consider when deciding whether and how to seek support.
Stigma is an inescapable part of human existence that occurs when people are reduced from whole beings to discounted ones (Goffman, 1963). A widely recognized definition of stigma follows Goffman’s (1963) conceptualization of stigma as a discrediting mark that is socially constructed in nature; stigma “spoils [a] social identity” (p. 19) and may prohibit people from being fully accepted by their peers. People perceive varying levels of stigma for a variety of personal attributes, including sexual orientation (Herek et al., 2009), physical illness or disability (Goffman, 1963), and mental illness (Corrigan et al., 2014), as well as everyday distressing experiences that people perceive to be stigmatized (Goffman, 1963). Stigma based on mental or emotional distress impacts people’s well-being (Corrigan et al., 2010; Goffman, 1963) and hinders communication and health promotion (Smith et al., 2016). Consistent with communication scholarship on stigma (e.g., Meisenbach, 2010), we approach stigma as a multifaceted construct. Specifically, this study examines two dimensions of stigma in the context of mental health: visibility and internalization. Researchers can gain a better understanding of the paradox of support seeking by studying how different attributes of stigma influence people’s decisions to seek support.
The visibility of a stigma pertains to whether the causes of stigma are able to be concealed, hidden, and controlled, or whether they are readily apparent to observers or potential support providers (Jones et al., 1984). There is considerable variation in the concealability of the symptoms and experiences that elicit feelings of mental or emotional distress (Day et al., 2007). Many visible indicators of mental or emotional distress stem from unexpected or nonnormative communicative behaviors and appearance (Flanagan & Davidson, 2009). Although some indicators of distress are overtly manifest, others are concealable, and the person passes as someone who is unaffected and unimpaired, thereby preserving positive self-presentation (Flanagan & Davidson, 2009; Jones et al., 1984). Visibility is a subjective assessment of stigma that governs decisions to seek or avoid seeking support.
In their initial test of the paradox of support seeking, Williams and Mickelson (2008) predicted that “visibility should not change the paradox of indirect seeking. All individuals with stigmas are mindful of what others might think during social interactions” (p. 497). Reversing course, however, the authors later identified the visibility of stigma as playing a more crucial role than initially predicted. They stated, “[p]erhaps the stigmatized seek support directly from those to whom the stigma is visible” (p. 507). There is arguably less risk involved in seeking support directly for a concern that is already apparent. This notion has been examined in “coming out proud” interventions (e.g., Corrigan et al., 2010), whereby people experiencing mental or emotional distress embrace who they are and their social situation, thereby reducing self-stigma and enhancing perceptions of personal empowerment. Furthermore, scholarship has indicated that those with visible stigmatized attributes do not face the same level of distress pertaining to disclosure as those with easily concealable attributes (Bos et al., 2013). Because stigma is a multidimensional construct and extant scholarship has demonstrated the ways visibility, especially in the context of mental health, shapes disclosure, we advance our first hypothesis:
H1: The degree of stigma visibility associated with mental or emotional distress is (a) positively associated with the directness, emotional content, and depth of seeking support for that issue and (b) negatively associated with avoidance.
Another dimension on which perceptions of stigma vary is internalization, a subjective assessment of the extent to which people align with a devalued social group and self-label as deviant or shameful (Ritsher et al., 2003). High degrees of internalized stigma occur when people align with something that is perceived as inherently negative and accept that stigma as part of their personal belief system, whether temporary or long-lasting (Herek et al., 2009). People who internalize feelings of stigma tend to isolate and avoid interaction as a means of limiting communication and reducing stigmatizing encounters (Meisenbach, 2010; Smith, 2007).
Internalization of stigma often contributes to psychological harm based on its associated sense of shame and devaluation (Corrigan, 1998). People who internalize stigma adjust their self-perceptions to be in line with society’s response to the stigma (Herek et al., 2009). High degrees of internalized stigma often result in a lack of disclosure and withdrawal from social interaction (Corrigan, 1998; Meisenbach, 2010), both of which affect the process of seeking support. Williams and Mickelson (2008) proposed that fear of rejection is positively associated with indirectly seeking support. Because feelings of internalized stigma often result in shame, avoidance, and limited social interaction (Corrigan, 1998; Smith, 2007), internalized stigma related to mental or emotional distress should hinder effective support seeking. We predict:
H2: The degree of stigma internalization associated with mental or emotional distress is (a) positively associated with avoidance, and (b) negatively associated with the directness, emotional content, and depth of seeking support for that issue.
Buffers and Barriers of Seeking Support
Disclosure and seeking support carry both risks and rewards (Goldsmith & Parks, 1990). When faced with a decision to disclose personal information, people cognitively assess the risks involved in disclosure and make a decision about their willingness and ability to share (T. D. Afifi & Steuber, 2009). Feelings of stigma often lead to perceived barriers to seeking support (Williams & Mickelson, 2008); however, such feelings are not always a barrier. There are buffering factors that promote resistance to stigma (Smith & Bishop, 2019). To appreciate the communicative consequences of stigma pertaining to mental or emotional distress, we examine barriers (i.e., costs) and buffers (i.e., efficacy) that shape whether, why, and how people seek support. Doing so positions assessments of costs and efficacy as explanatory mechanisms for why perceptions of stigma associated with a stressor shape how people seek support for that issue.
When people perceive that others will respond negatively to their disclosure, they are unlikely to disclose as a means of self-protection (T. D. Afifi et al., 2005). Extant research has identified personal costs, such as guilt (Smith & Bishop, 2019) and shame (Landau & York, 2004), that motivate people to avoid seeking support. Other costs, such as believing that seeking support places a burden on the potential support provider, exist at the interpersonal level and lead people to seek support ineffectively (Smith et al., 2008). Perceived relational consequences from revealing stigmatized information, including rejection (Williams & Mickelson, 2008), anger, or withdrawal (Cloven & Roloff, 1993), may also lead people to engage in avoidance or seek support ineffectively. When there is a high degree of cost involved with disclosure, seeking support is often avoided based on fears that it could harm the support seeker, potential support provider, or their relationship (W. A. Afifi & Afifi, 2009). Based on costs related to seeking support, we predict:
H3: Higher perceived costs to the self and others are (a) positively associated with avoidance, and (b) negatively associated with directness, emotional content, and depth when seeking support for mental or emotional distress.
The paradox of support seeking focuses solely on barriers to seeking support (Williams & Mickelson, 2008); however, buffering factors may shield people from the negative aspects of stigma and encourage them to communicate directly. Although there are presumably many factors that buffer the negative effects of stigma, this study focuses on efficacy because of its central role in decision-making regarding disclosure and information management (T. D. Afifi & Steuber, 2009; W. A. Afifi & Weiner, 2004). People who perceive greater efficacy are generally more likely to disclose potentially costly personal information and seek support more effectively (T. D. Afifi & Steuber, 2009).
Similar to how perceived costs exist at multiple levels, efficacy assessments exist at personal (i.e., self-efficacy) and relational (i.e., target efficacy) levels (W. A. Afifi & Weiner, 2004; Sheffield et al., 2004). Self-efficacy plays a key role in seeking support because being capable of disclosing and seeking support is positively associated with the willingness to do so (T. D. Afifi & Steuber, 2009). In other words, when people are able to communicate their wishes for support and cope with a support provider’s response, they are more likely to disclose their distress and seek support in direct ways (W. A. Afifi & Weiner, 2004; High & Scharp, 2015).
Perceived target efficacy also plays a role in deciding whether and how to seek support. When people perceive that a potential provider (i.e., target) has the ability to honestly offer the type and amount of support desired, they are more likely to seek support (W. A. Afifi & Weiner, 2004). Likewise, a support seeker’s perception of a potential support provider’s efficacy is positively associated with directly seeking support and negatively related to indirect seeking or avoidance (Sheffield et al., 2004). Although efficacy is often studied in relation to disclosure and information management, we extend that research to offer the following hypothesis:
H4: Higher perceived self and target efficacy is (a) positively associated with directness, emotional content, and depth when seeking support in the context of mental or emotional distress, and (b) negatively associated with avoidance.
Stigma pertaining to feelings of mental or emotional distress, perceived barriers, and perceived buffers impact the process of seeking support. This study extends research on the stigma associated with feelings of mental or emotional distress (e.g., Corrigan, 1998; Johnstone, 2001) by examining whether and how that stigma shapes how people seek support by biasing their perceptions and behavior. Specifically, H1 and H2 predict that higher levels of visibility and lower levels of internalization are positively associated with strategies of directness, emotional content, and depth, whereas lower levels of visibility and higher levels of internalization are positively associated with avoidance when seeking support. We also predict in H3 and H4 that lower perceived costs and higher efficacy assessments are positively associated with the directness, emotional content, and depth when seeking support. Consequently, higher perceived costs and lower efficacy assessments are positively associated with avoidance. Synthesizing these predictions and extending the logic of the paradox of support seeking, which generally claims that stigma shapes how people seek support because it biases coping (Williams & Mickelson, 2008), we advance hypotheses that identify perceived costs and assessments of efficacy as explanatory mechanisms guiding the relation between attributes of stigma and variation in behaviors used to seek support. This logic implies a layering of increasingly specific perceptions as people’s general perceptions of stigma shape their understanding of barriers and buffers related to seeking support, which in turn shape their decisions regarding how to seek support for their feelings of mental or emotional distress.
Support seekers who possess higher degrees of internalized stigma likely perceive that seeking support is costly because it could lead to rejection (Williams & Mickelson, 2008), shame (Corrigan, 1998; Ritsher et al., 2003), and damage to their self-concept (Herek et al., 2009).
Additionally, internalized stigma is associated with lower levels of self-efficacy and self-esteem (Corrigan et al., 2006). When someone perceives they are less able to communicate their desire for support effectively, they often seek support indirectly or avoid doing so altogether (e.g., High & Scharp, 2015). They may also perceive that the support provider is not efficacious in providing quality support (e.g., Sheffield et al., 2004). In other words, internalization heightens perceived costs to the self and others while decreasing assessments of self- and target (i.e., provider) efficacy, which in turn influences assessments of communication. Put formally:
H5: Greater costs and lower efficacy mediate (a) the positive association between internalization and avoidance, and (b) the negative association between internalization and the directness, emotional content, and depth of support seeking in the context of mental or emotional distress.
Support seekers who perceive higher degrees of visibility are often more comfortable discussing the causes and feelings associated with stigma (Thompson, 1982), and there might be fewer costs involved with seeking support because the stigma is already apparent. Furthermore, connecting with others through direct strategies of seeking support is typically associated with self-efficacy and the ease with which stigmatized individuals engage in interactions (Corrigan et al., 2010; Thompson, 1982). Because higher levels of stigma visibility are expected to correspond with lower perceived costs to the self and others and higher assessments of self- and target efficacy, we predict:
H6: Lower costs and greater efficacy mediate (a) the positive association between visibility and the directness, emotional content, and depth of support seeking, and (b) the negative association between visibility and avoidance in the context of mental or emotional distress.
Methods
Sample and Procedures
Young adults aged 18 to 25 have the highest prevalence of mental health concerns among all adults in the United States (NIMH, 2022), so we identified this age range as our first eligibility criterion. To capture the experiences of people who both sought and avoided seeking support, participants must have considered seeking support for mentally or emotionally distressing experience(s) within the past month. Rather than employing a clinical sample, we recruited individuals across the U.S. with a range of everyday experiences of mental or emotional distress. Doing so increased the generalizability with which we are able to discuss how stigma shapes seeking support and established a means for identifying a stigma that people actually felt, without the researchers ascribing stigma to participants’ experiences. To capture a range of experiences that elicit mental or emotional distress, participants answered screening questions measuring depressive-and anxiety-type symptoms (e.g., feeling down, worrying) taken from the Generalized Anxiety Disorder scale (Spitzer et al., 2006) and Patient Health Questionnaire (Kroenke & Spitzer, 2002). Respondents were required to have had at least three of the six experiences in the past month to ensure that eligible participants had been feeling at least half of the common indicators of mental or emotional distress. We were less interested in the particular stressors people identified, as long as they aroused some level of mental or emotional distress. We were more interested in their accompanying feelings of stigma. Specifically, participants were instructed, “Please think back to a time in the past month where you considered seeking support for any mentally and emotionally distressing experience you may have encountered.”
People coping with mental or emotional distress seek support from a range of formal and informal support providers (Oliver et al., 2005), and there are different perceived costs and benefits of seeking support from formal (e.g., healthcare professional) and informal (e.g., family member, friend) providers (Rickwood et al., 2007). Consequently, we asked participants to identify the main person from whom they sought or considered seeking support for their mental or emotional distress. Eligible participants were asked to describe their mental or emotional distress (i.e., stressor), including the everyday impact of the stressor, from whom they sought support (or considered seeking support if they avoided an interaction), and how long ago they sought (or considered seeking) support for the stressor they identified. Participants identified stressors pertaining to grief and loss (e.g., death of a loved one), friendship struggles, family dysfunction (e.g., fights, abuse), romantic relationship turbulence or dissolution (e.g., breakup with a partner), and bullying. Another type of stressor frequently identified by participants pertained to health concerns, spanning mental health (e.g., PTSD, anxiety, depression, eating disorder, OCD, loneliness), physical health (e.g., cancer, pregnancy, miscarriage, abortion, exhaustion), and addiction. The remaining stressors were more situational, including academic and employment concerns (e.g., school performance, laid off from job), financial difficulties (e.g., struggling to pay bills), legal issues, and general feelings of being overwhelmed by life changes.
Participants (N = 406) were a sample of young adults living in the United States who were recruited using Qualtrics survey software in December 2019. The mean age of our sample was 21.19 years (Robs = 18–25, SD = 2.37). Our sample was predominantly female (84.4%) and heterosexual (69.1%) and also included individuals identifying as bisexual (18.2%), lesbian or gay (6.5%), or a different sexual orientation (3.6%). The majority of the sample identified as White (78.7%), with participants also identifying as Black (15.6%), Asian (6.9%), American Indian or Alaska native (1.2%), Native Hawaiian or Pacific Islander (0.5%), or a race not listed (e.g., Middle Eastern, several races; 4.1%). Additionally, 19.7% of the participants were Spanish, Hispanic, or Latinx. Participants were employed (53.3%), currently looking for work (22.0%), students (12.9%), stay at home parents/homemakers (4.5%), or not working (2.9%). Participants were asked to identify the support provider from whom they most considered seeking support, with family members (34.0%), friends (25.4%), healthcare providers (18.4%), and partners (16.3%) representing the majority of support providers identified. Participants were instructed to answer survey items with the specific stressor and support provider they identified in mind.
Measures
All variables were measured using self-report scales that employed Likert-type scaling with responses ranging from 1 (strongly disagree) to 7 (strongly agree).
Everyday Impact of Mental or Emotional Distress
The everyday impact of mental or emotional distress was assessed using a single item in which participants were asked to indicate their level of (dis)agreement with the statement, “My experiences with mental and emotional distress over the past month have impacted my everyday life (e.g., school, work, home, relationships).” The conceptualization of everyday impact is akin to quality of life measures, which are often used in health contexts to assess how distress affects functioning and coping on a regular basis. On average, participants agreed that their experience(s) impacted their everyday lives (M = 5.42, SD = 1.55, Robs = 1.00–7.00). To account for variance in responses, the everyday impact of mental or emotional distress was controlled for in later analyses.
Attributes of Stigma
Stigma Internalization
The internalization of stigma was measured using the Internalized Stigma of Mental Illness (ISMI) scale (Ritsher et al., 2003). We included six items from the alienation subscale of the ISMI scale (e.g., “People without mentally and emotionally distressing experiences like mine could not possibly understand me”) to capture participants’ personal, internal assessment of stigma. Two additional items (e.g., “I feel uncomfortable about who I am. . .”) were added to this scale to capture pertinent emotional and cognitive experiences that constitute internalization. A composite variable was created by averaging all items, such that higher scores signify greater internalization of stigma (M = 4.55, SD = 1.54, Robs = 1.00–7.00, McDonald’s ω = .93).
Stigma Visibility
The visibility of stigma was measured using the visibility items from the Mental Illness Stigma Scale (Day et al., 2007). This “Visibility” subscale consists of four items (e.g., “It was easy for others to recognize my experience with mental and emotional distress”). A composite variable was created by averaging all items, such that higher scores signify greater visibility of stigma (M = 3.87, SD = 1.45, Robs = 1.00–7.00, ω = .82).
Aspects of Seeking Support
Direct Strategies
Direct verbal strategies of seeking support were assessed using Barbee and Cunningham’s (1995) typology of support-seeking strategies (adapted by Derlega et al., 2003). This study used the four-item “Ask” subscale to measure direct strategies of seeking support (e.g., “I asked how I could best manage the mentally and emotionally distressing experience”). A composite variable was created by averaging all items, such that higher scores signify greater use of direct verbal strategies (M = 5.23, SD = 1.20, Robs = 1.75–7.00, ω = .75).
Emotional Content
The degree of emotional content included when seeking support was assessed using 16 items from Kring et al.’s (1994) Emotional Expression Scale. Items were adapted to fit the context of the present study (e.g., “Others would see my support seeking as very emotional”). A composite variable was created by averaging all items, such that higher scores signify more emotional content (M = 4.45, SD = 1.13, Robs = 1.87–7.00, ω = .92).
Depth
The depth of seeking support was measured with Bazarova’s (2012) semantic-differential scale consisting of five items, each with two anchors (e.g., impersonal—personal, shallow—deep). A composite variable was created by averaging all items, such that higher scores signify greater perceived depth (M = 5.11, SD = 1.40, Robs = 1.00–7.00, ω = .86).
Avoidance
Avoidance of seeking support was assessed using W. A. Afifi and Afifi’s (2009) seven-item Avoidance scale and Barbee and Cunningham’s (1995) four-item indirect seeking (i.e., Hint) subscale. These scales were highly correlated (r = .82). Confirmatory factor analysis2 revealed that the indirect seeking and avoidance items loaded onto one latent variable of avoidance (e.g., “I avoided talking about my mentally and emotionally distressing experience”). After correlating four error terms, the model fit the data well, χ2(31) = 137.75, p < .05, SRMR = .03, CFI = .97, RMSEA = .09. A composite variable was created by averaging all items, with higher scores signifying greater avoidance (M = 4.38, SD = 1.48, Robs = 1.00–7.00, ω = .93).
Barriers and Buffers Related to Seeking Support
Barriers to seeking support were operationalized as costs relating to self-perceptions (i.e., intrapersonal costs) and costs relating to the others’ perceptions (i.e., interpersonal costs). Items were drawn from Lim et al.’s (2013) measure of psychological costs of seeking support. For intrapersonal costs, participants were presented with the stem, “When considering whether and how to seek support for this experience, I worried that I would:” and answered six items assessing intrapersonal costs (e.g., “view myself as being unable to cope with stress”). For interpersonal costs, participants were presented with a similar stem focusing on other people and answered eight items assessing interpersonal costs (e.g., “judge me negatively”). Composite variables were created by averaging all items, such that higher scores signify greater intrapersonal (M = 4.68, SD = 1.60, Robs = 1.00–7.00, ω = .93) and interpersonal costs (M = 4.18, SD = 1.80, Robs = 1.00–7.00, ω = .97).
Buffering factors were operationalized as self- and target (i.e., provider) efficacy.
Consistent with previous research, scale items were derived from two measures of self-efficacy and two measures of target efficacy (W. A. Afifi & Afifi, 2009; W. A. Afifi et al., 2006). Self-efficacy was assessed with three items that measure communication efficacy (e.g., “I felt like I was able to approach the person. . .to talk about my experience with mental and emotional distress”) and four items that measure coping efficacy (e.g., “I felt confident that I could cope with whatever this person said. . .”). Target efficacy included three items that assess target ability (e.g., “This person had the skills necessary to provide support for my experience. . .”) and four items that measure target honesty (e.g., “This person would have been completely honest when providing support for my experience. . .”). Consistent with prior research (e.g., W. A. Afifi et al., 2006), composite variables were created by averaging all items, such that higher scores signify greater self-efficacy (M = 5.25, SD = 1.08, Robs = 1.00–7.00, ω = .75) and target efficacy (M = 5.31, SD = 1.02, Robs = 1.86–7.00, ω = .82).
Results
Preliminary Analyses
We began by conducting a confirmatory factor analysis for the overall measurement model. Individual items loaded on the ten variables in the model, which were allowed to correlate. The initial model did not achieve acceptable fit, χ2(2429) = 4,816.38, p < .05, SRMR = .08, CFI = .89, RMSEA = .05. Modification indices recommended correlating three pairs of within-factor error terms. An omnibus test of the revised measurement model revealed adequate fit (Hu & Bentler, 1999) and demonstrated both unidimensionality of the variables and a lack of cross loading, χ2(2426) = 4,654.07, p < .05, SRMR = .08, CFI = .90, RMSEA = .05. Correlations among the variables in the model are provided in Table 1.
Correlation Matrix for All Variables in the Model.
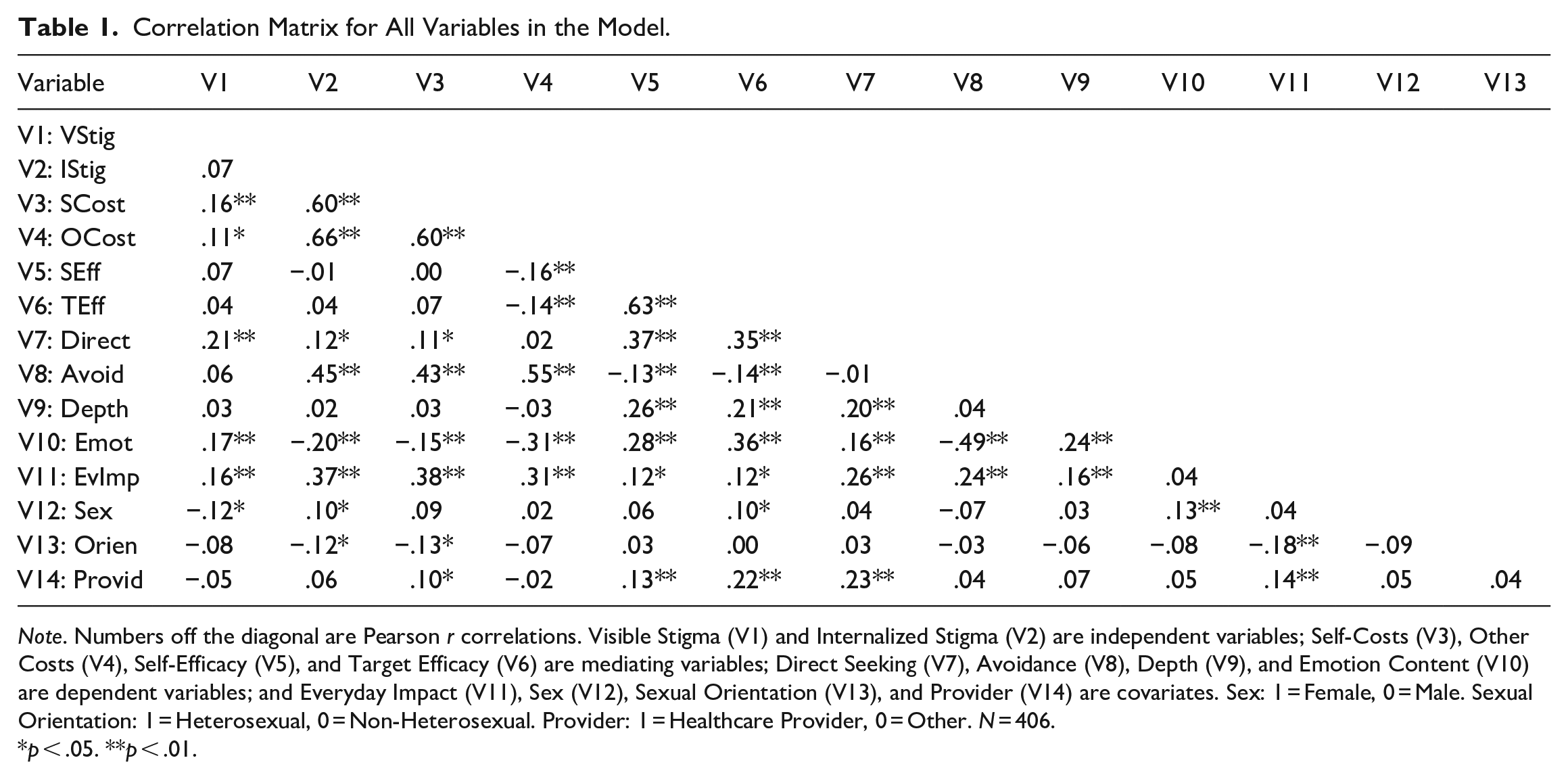
Note. Numbers off the diagonal are Pearson r correlations. Visible Stigma (V1) and Internalized Stigma (V2) are independent variables; Self-Costs (V3), Other Costs (V4), Self-Efficacy (V5), and Target Efficacy (V6) are mediating variables; Direct Seeking (V7), Avoidance (V8), Depth (V9), and Emotion Content (V10) are dependent variables; and Everyday Impact (V11), Sex (V12), Sexual Orientation (V13), and Provider (V14) are covariates. Sex: 1 = Female, 0 = Male. Sexual Orientation: 1 = Heterosexual, 0 = Non-Heterosexual. Provider: 1 = Healthcare Provider, 0 = Other. N = 406.
p < .05. **p < .01.
The hypotheses were tested using the MEDIATE macro for SPSS (Hayes, 2014) because it allowed us to model the direct and mediated effects of both of our predictors (i.e., visibility and internalization of stigma) in the model concurrently. Four models were analyzed, one for each of the dependent variables (i.e., direct seeking, emotional content, depth, and avoidance), with all predictors and mediators included in each model. We included four covariates when testing each of the models: everyday impact of the mental or emotional distress, sex of the support seeker, sexual orientation, and type of support provider (i.e., professional vs. informal support provider). The everyday impact of a stressor has been shown to influence help-seeking behaviors (e.g., Fox et al., 2018). Sex and sexual orientation often shape people’s willingness to seek support and their actual engagement in support elicitation behaviors (e.g., Barbee et al., 1993). The type of provider has implications for whether and how support is sought (Rickwood et al., 2007; Sheffield et al., 2004). All scores were standardized before conducting analyses, and 10,000 bootstrapped samples were utilized for the estimation of indirect effects.
Tests of Hypotheses
Hypothesis 1 predicted that the degree of stigma visibility for mental or emotional distress would be (a) positively associated with strategies of directness, emotional content, and depth, and (b) negatively associated with avoidance pertaining to that stressor. Consistent with predictions, stigma visibility was positively and significantly associated with directly seeking support, β = .17, SE = 0.04, p < .01, and the emotional content used when seeking support, β = .28, SE = 0.06, p < .01. There were no significant effects of visibility on depth (β = −.00, SE = 0.05, p = .99) or avoidance (β = −.03, SE = 0.04, p = .50). These results largely support H1a, but do not support H1b.
Hypothesis 2 predicted that the degree of stigma internalization would be (a) positively associated with avoidance, and (b) negatively associated with strategies of directness, emotional content, and depth. There was a significant direct effect of internalization on avoidance, β = .12, SE = 0.06, p < .05. There were no significant effects of internalization on directness (β = .05, SE = 0.06, p = .37), emotional content (β = −.13, SE = 0.09, p = .14), or depth (β = −.02, SE = 0.07, p = .72). Thus, H2a is supported, but H2b is not supported.
Hypothesis 3 predicted that higher perceived costs to the self and others would be (a) positively associated with avoidance, and (b) negatively associated with directness, emotional content, and depth when seeking support for mental or emotional distress. In line with our predictions, intrapersonal, β = .12, SE = 0.05, p < .05, and interpersonal, β = .34, SE = 0.05, p < .01, costs were positively associated with avoidance. Interpersonal costs were negatively associated with emotional content, β = −.28, SE = 0.08, p < .01. There were no significant effects of intrapersonal costs on directness (β = −.03, SE = 0.05, p = .60), depth (β = −.02, SE = 0.06, p = .76), or emotional content (β = −.08, SE = 0.08, p = .31), and no significant effects of interpersonal costs on directness (β = −.01, SE = 0.05, p = .89) or depth (β = −.00, SE = 0.06, p = .94). These results support H3a and partially support H3b.
Hypothesis 4 predicted that higher perceived efficacy of the self and target would be (a) positively associated with directness, emotional content, and depth, and (b) negatively associated with avoidance. Perceived self-efficacy was positively associated with directness, β = .22, SE = 0.06, p < .01, and the depth of disclosure used when seeking support, β = .20, SE = 0.07, p < .01, but not with emotional content (β = .08, SE = 0.08, p = .33). Target efficacy was positively associated with the directness, β = .18, SE = 0.06, p < .01, and emotional content conveyed when seeking support, β = .42, SE = 0.09, p < .01, but not with depth (β = .07, SE = 0.07, p = .31). Self-efficacy (β = −.03, SE = 0.06, p = .58) and target efficacy (β = −.08, SE = .06, p = .21) were not associated with avoidance. H4a was largely supported, but H4b was not supported.
Hypothesis 5 examined the indirect effects of internalized stigma on strategies used to elicit support through perceived costs and efficacy. We found significant positive indirect associations between the degree of stigma internalization and avoidance through both intrapersonal, β = .07, SE = 0.03, 95% CI [0.00, 0.14], and interpersonal, β = .23, SE = 0.05, 95% CI [0.14, 0.33], costs. In other words, people who internalized the stigma pertaining to their mental or emotional distress were more likely to avoid seeking support about that stressor because they worried about concerns related to themselves and potential support providers. We also observed a significant negative indirect association between the degree of stigma internalization and emotional content through interpersonal costs, β = −.19, SE = 0.07, 95% CI [−0.33, −0.07]. People who internalized stigma were less likely to be emotionally expressive when seeking support because of the interpersonal costs they perceived. All other indirect effects, including all paths via self and target efficacy and on directness and depth of seeking, failed to attain statistical significance. These findings provide partial support for H5a and H5b.
Hypothesis 6 examined the indirect effects of stigma visibility on support seeking through perceived costs and efficacy. Contrary to H6, we found a positive indirect association between the degree of stigma visibility pertaining to mental or emotional distress and avoidance of support for that stressor through intrapersonal costs, β = .01, SE = 0.01, 95% CI [0.00, 0.04]. People who perceived their stigma to be highly visible to others were more likely to avoid seeking support because of the personal costs associated with disclosing their stigmatized experience. All remaining paths failed to attain statistical significance. H6 was not supported. The full results for H1 to H6 are presented in Tables 2 and 3.
Results of Hypothesis Testing: Direct Seeking and Avoidance (Using Standardized Coefficients).
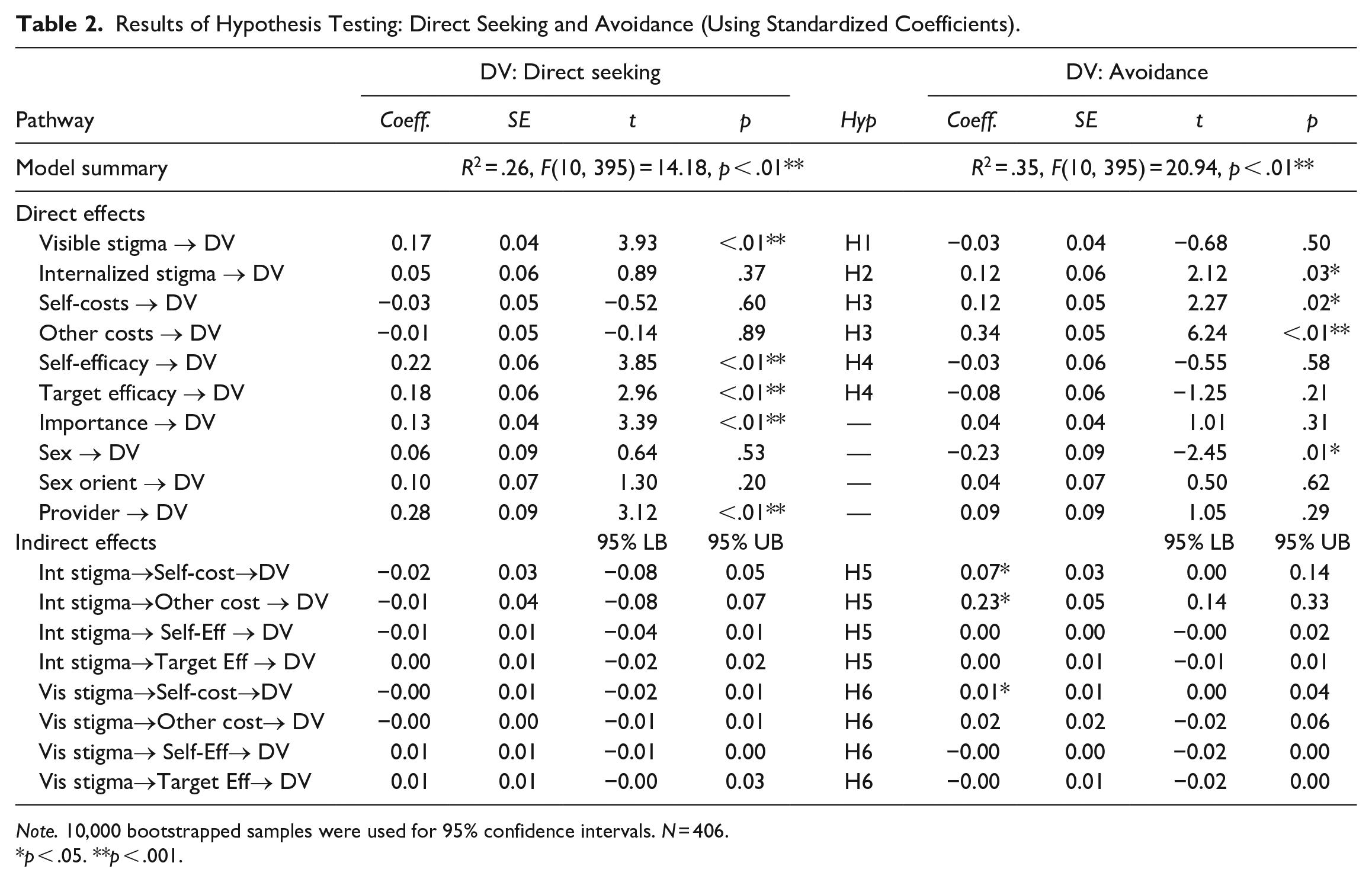
Note. 10,000 bootstrapped samples were used for 95% confidence intervals. N = 406.
p < .05. **p < .001.
Results of Hypothesis Testing: Depth and Emotional Content (Using Standardized Coefficients).
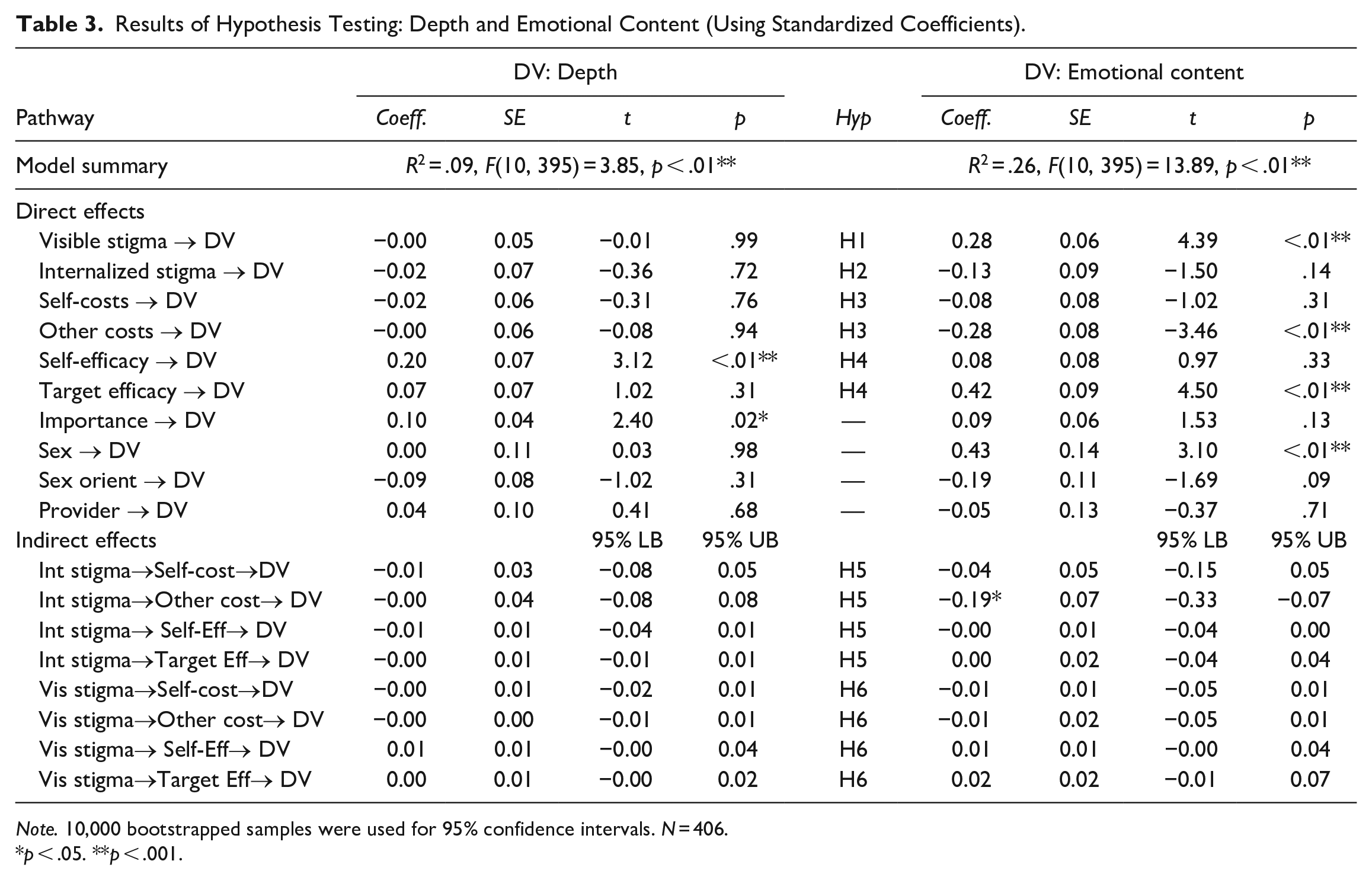
Note. 10,000 bootstrapped samples were used for 95% confidence intervals. N = 406.
p < .05. **p < .001.
Discussion
We set out to accomplish three main goals in this study. First, we wanted to examine the multidimensional nature of stigma. We found positive associations between the visibility of stigma and both the directness and emotional content of support seeking. The internalization of stigma was directly associated with avoidance, and indirectly associated with avoidance and emotional content when considering the perceived costs to the self and support provider, highlighting the complex nature of stigma. Second, we sought to better understand the process of seeking support for people who felt stigma as a result of experiencing mental or emotional distress, which we accomplished by studying the mediating role of barriers and buffers to seeking support for those issues. We found that higher levels of intra- and interpersonal costs were positively associated with avoidance, and higher levels of interpersonal costs were negatively associated with the emotional content of support seeking. In other words, when people experienced barriers related to seeking support for their mental or emotional distress, they were more likely to avoid seeking support for it. In contrast, people who felt they were able to communicate their need for support and cope with the support they received were more likely to directly seek support and use greater depth. Additionally, participants who perceived their support provider to be efficacious were more likely to directly seek support and include a greater degree of emotional content when doing so. Finally, we were interested in expanding the dimensions used to describe how people seek support, so we analyzed the degree of directness, emotional content, and depth used when seeking support, in addition to avoiding supportive interactions altogether.
Examination of indirect effects through our explanatory mechanisms of perceived costs and efficacy revealed a negative association between the degree of internalized stigma on the emotional content of support seeking through interpersonal costs, and a positive association between the degree of internalized stigma and avoidance through both intra- and interpersonal costs. In other words, those who had higher levels of internalized stigma typically revealed less emotional content or avoided seeking support altogether because of the perceived costs of seeking support. Visibility, however, did not predict variation in support eliciting behaviors in the hypothesized manner. Instead, the only significant indirect effect involving visibility was its positive indirect association with avoidance through intrapersonal costs.
Theoretical and Practical Implications
The results from this study suggest an extension to the paradox of support seeking (Williams & Mickelson, 2008) and bolster the need for a more nuanced understanding of the ways in which people seek support. In the paradox of support seeking, stigma is considered a unidimensional construct. In reality, stigma is multidimensional and should be studied as such, which is consistent with Williams and Mickelson’s (2008) later thinking. The paradox of support seeking can be further extended by exploring the multidimensionality of stigma beyond visibility and internalization. For instance, experienced stigma, or instances of discrimination based on one’s stigmatized identity (Van Brakel, 2006), is another dimension that might impact how people seek support. The study of support seeking would be further enhanced by examining the ways that stigmas are communicated and experienced. This can be done by integrating theories of stigma, such as the model of stigma communication (MSC; Smith, 2007), which focuses on stigmatized identities and contends that people make choices about the strategies they use to communicate stigma to others. In considering multiple dimensions on which stigmas and support seeking behaviors vary, we found evidence that the processes guiding whether and how people seek support are complex and dynamic, with different perceptions of stigma associated with different support seeking behaviors.
Smith (2007) discussed the concept of a mark, or a physically and socially recognizable cue communicating one’s membership in a stigmatized group, which is similar to people’s perceptions of visibility in the current study. Depending on the degree of visibility, marks may be concealed to minimize social recognition and response (Smith, 2007). This conceptualization of marks could help explain why we found a positive direct effect of visibility on the directness and emotional content included when seeking support, but a positive indirect effect of visibility on avoidance when considering intrapersonal costs. The perception of the visibility of stigma alone might not encourage avoidance unless the visibility of a mark evokes negative cognitive and affective responses, such as shame, perceived threat, and intrapersonal costs (Smith, 2007). Another relevant factor in the theory of MSC is responsibility, which is the degree to which a stigmatized person is perceived to choose and control their stigma (Smith, 2007). When people believe that they are responsible for a stigma, they might internalize stigma and regard their experiences as inherently deviant and/or shameful, thereby hindering their support seeking (Herek et al., 2009; Ritsher et al., 2003).
SIST (Barbee & Cunningham, 1995) considers a range of behaviors used to elicit support, but these behaviors are often reduced to direct and indirect strategies. The need for a more comprehensive way of studying and characterizing support seeking has been articulated for decades (e.g., Goldsmith, 1995), with some recent work being done to push the boundaries of what constitutes variation in support seeking in technologically mediated contexts (e.g., Buehler, 2018; Youngvorst & High, 2018). There is still, however, ample room for expansion pertaining to how researchers conceptualize and measure variation in support seeking behaviors. We drew upon research on disclosure to help explain people’s decisions pertaining to whether and how to seek support in the context of stigma. Seeking support and self-disclosure are similar processes, with disclosure often serving as a component of seeking support (e.g., Barbee & Cunningham, 1995; Barbee et al., 1993; Youngvorst & High, 2018). Drawing on the disclosure process model (Chaudoir & Fisher, 2010) could further advance scholarship by considering a range of strategies used to elicit support, including the breadth of experiences shared and the duration of supportive interactions. Having more nuance to describe variation in how people seek support not only provides a more precise understanding of the process of supportive communication, but also identifies variables that might predict the success of these interactions.
We can also turn to the revelation risk model (RRM; T. D. Afifi & Steuber, 2009) to examine the ways in which costs may contribute to variation in how people seek support. The RRM posits that people cognitively assess the risks involved in disclosing personal information and make calculated decisions regarding whether they are willing and able to disclose. Self-protection (T. D. Afifi et al., 2005) is especially salient in the context of stigma because disclosing one’s mental or emotional distress may be seen as a taboo disclosure (Vangelisti, 1994), and avoiding disclosure may reduce judgment, rejection, or disapproval (Williams & Mickelson, 2008). Information that is inconsistent with one’s desired image might be concealed when seeking support because face concerns of the seeker and provider are especially salient (Floyd & Ray, 2017; Goffman, 1959).
The level of disclosure involved in seeking support might be so risky that people think it is safer to avoid seeking support altogether, especially if they have previously experienced damaging reactions following the disclosure of a stigmatized experience or identity (Rickwood et al., 2007). Although visibility was a significant positive predictor of directly seeking support, when costs were included in the model, participants were more likely to avoid seeking support, which could indicate an elevated desire for self-protection. It would be interesting to further explore the ways in which costs impact strategies of seeking support, thereby providing further insight into the explanatory mechanisms that drive whether and how people seek support.
Future Research Directions
In light of the theoretical implications outlined above, it is useful to also consider the practical implications of this research. For example, interpersonal costs directly and indirectly explained variation in strategies used to seek support and did so with greater frequency than intrapersonal costs. This indicates that the risks of confronting others might be more consequential than personal risks when seeking support. Seeking support places a demand on a potential support provider, which could be anticipated as a burden by the support seeker (Smith et al., 2008; Williams & Mickelson, 2008). There could also be a fear of stigma and the associated judgment and discrimination being placed on the support provider by way of courtesy stigma, which occurs when broader social networks extend stigma from a stigmatized individual to those with whom that person interacts (Smith et al., 2016).
Participants in this study based their decision to seek support on assessments of their own efficacy and the efficacy of a potential support provider. Research on mental health-related stigma has revealed that internalized stigma is typically associated with worsened self-esteem and self-efficacy (Corrigan et al., 2006). Future research can examine how efforts to enhance support seekers and providers’ efficacy when asking for and offering support for stigmatized stressors may promote adaptive coping. Increasing empathy and perspective taking (Trobst et al., 1994) may also be especially useful in building safety and rapport between support seekers and providers. Taken together, these directions for future research might reduce perceived costs and enhance perceived efficacy, which the current results indicate can buffer against the often deleterious effects of stigma in the context of seeking support for mental or emotional distress. We explained between 9% and 35% of the variance in the dependent variables in our model, and including these motivational, relational, and contextual factors could help to better explain how and why stigma shapes how people seek support.
Limitations
This study provided insights into the process of seeking support in light of feelings of stigma surrounding mental or emotional distress, and the ways assessments of costs and efficacy influence these processes; however, this study is not without its limitations. First, the study design and relative homogeneity of our sample (i.e., predominantly White and female) warrant further investigation. The cross-sectional survey design allowed us to make inferences about the relationships among variables and explore explanatory mechanisms but not test causality. Although our model was based on past empirical research (e.g., Williams & Mickelson, 2008), a more diverse sample should be employed and a longitudinal design could be utilized to assess temporal relations.
Another limitation pertains to the measurement of our variables. We asked about participants’ relationship with a support provider, but not the sex of the provider. Although sex differences are often modest (High & Solomon, 2014), future work could assess whether provider sex shapes strategies used to seek support in the context of mental or emotional distress. We also utilized self-report measures to capture participants’ perceptions of seeking support, which might differ from the actual messages communicated. Self-report measures, however, are useful for examining perception and decision-making processes and are in line with previous tests of the paradox of support seeking (Williams & Mickelson, 2008). Future research would benefit from combining subjective and objective assessments of support seeking to further explore interactive coping and the degree to which people’s perceptions align with their communication. For example, researchers could code actual messages used to seek support (Buehler et al., 2019) and/or reasons why people chose not to seek support (Floyd & Ray, 2017).
A final limitation is our choice to study a broad conceptualization of mental or emotional distress, rather than examining specific mental illnesses, which could impact the conclusions we are able to draw from this research. For instance, we cannot connect specific diagnoses to clinical recommendations for therapeutically beneficial supportive interactions. Using a broad definition also combined chronic diagnoses, acute difficulties, and emotional upset as factors that can produce feelings of stigma. Stigma is applicable beyond a formal diagnosis, and we were interested in the perception of stigma following distress rather than a specific context, stressor, or identity. Future research can test the boundary conditions of our work by testing it across a variety of specific circumstances. The “mental or emotional distress” terminology, however, was intentionally selected to be more inclusive of the breadth of experiences that may arise in the context of mental health-related stigmas, without further stigmatizing and ascribing labels to those who experience mental or emotional distress (Mental Health Foundation [MHF], 2022). This terminology also appreciates the varied ways that distress is experienced across persons and situations and allows for a more nuanced understanding of cognitive, behavioral, and affective processes that might impact people’s lives (Johnstone, 2001).
Conclusion
This study sheds light on the multidimensional nature of stigma along with barriers and buffering factors that impact whether and how people seek support. People who feel stigma do not have to seek support ineffectively, as suggested by the paradox of support seeking. Instead, this study provides insight into reasons why people seek support, while also expanding the descriptors used to illustrate variation in how people seek support. People facing distress and stigma do not have to suffer alone. This study demonstrates that people can and do seek support when experiencing stigma and that they can find their voice and draw on their own and others’ efficacy in the face of adversity.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health Award Number TL1TR002016. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.